
Abstract

Nailfold capillaroscopy (NFC) is gradually emerging as a pivotal, non-invasive imaging tool for evaluating microvascular involvement in inflammatory conditions, moving beyond its traditional role in systemic sclerosis to become an essential diagnostic and prognostic asset in rheumatic diseases. Additionally, its role in non-rheumatic diseases, including diabetes, is also being explored. 1
Historically, NFC was used almost exclusively to identify the scleroderma pattern in systemic sclerosis and Raynaud’s phenomenon. However, its role has expanded considerably from a simple clinical observation to a broader tool that aids in diagnostic differentiation, assessment of disease severity, prediction of disease progression and internal organ involvement, evaluation of treatment response, and biological correlation reflecting systemic cytokine activity.2,3 It may serve as a preclinical biomarker predicting change in disease phenotype and assessing systemic microvascular involvement.
The study by Abd-Allah et al. 4 highlights differences in NFC findings between psoriasis (PsO) and psoriatic arthritis (PsA), suggesting that features such as capillary density and bushy capillaries/neoangiogenesis may serve as early warning indicators, potentially enabling early treatment before clinically evident disease and structural damage develop. However, the findings should be interpreted cautiously as the study is based on a small case–control cohort of 20 PsO patients, 20 PsA patients, and 20 controls, includes patients already receiving treatment rather than treatment-naïve individuals, relies on single-reader NFC acquisition, and applies exploratory statistical analyses without correction for multiple comparisons. Similar observations have been reported by Fukasawa et al., who also demonstrated that nailfold bleeding and enlarged capillaries can predict the development of PsA (HR = 2.75, 95% CI = 1.38–5.47 and HR = 4.49, 95% CI = 2.25–8.96, respectively). 2 Similar findings were reported by Prioteasă et al. in their systematic review, where they showed that disorganised and tortuous capillaries, along with a notable reduction in capillary density, were more common in PsA when compared to PsO. 5 These findings also suggest that articular involvement may correspond with more advanced microvascular disorganisation. However, larger prospective studies across diverse PsA phenotypes and ethnic populations are required to validate the role of NFC as a predictive tool before joint damage ensues.
The study also contributes to the growing recognition of psoriatic disease as a systemic microvascular disorder rather than a condition limited to the skin and joints. The demonstration of reduced capillary density, increased rarefaction and avascular areas, greater tortuosity, enlarged apical diameter, and a higher prevalence of bushy capillaries in both PsO and PsA supports the concept that microangiopathy accompanies the inflammatory process across the psoriatic spectrum. However, these findings need to be interpreted in the context of nail disease, which was present in 70% of patients in both groups. Within each group, nail involvement was associated with greater avascularity, larger apical diameter, and increased tortuosity, suggesting that nail pathology itself may significantly influence nailfold capillaroscopic patterns. As the main between-group comparisons do not appear to be adjusted for the severity of nail involvement, the observed microvascular differences may partly reflect the impact of nail disease rather than differences intrinsic to PsO versus PsA, representing an important limitation of the study.
Over the last decade, PsO has been reframed within the paradigm of the ‘psoriatic march’, linking chronic inflammation to endothelial dysfunction, metabolic syndrome, and cardiovascular morbidity. The current study aligns with this vascular narrative. The observed rarefaction and avascular areas may represent microvascular dropout secondary to sustained inflammatory and angiogenic signalling (VEGF, TNF-α, IL-17), while tortuosity and neoangiogenesis likely reflect pathological remodelling rather than physiological repair.
In the original study, correlation analysis demonstrated a moderately positive association between PASI score and capillary tortuosity severity in PsO patients (Spearman r = 0.597, P = .005), while the relationship between DAPSA score and capillaroscopic parameters in PsA was weaker, with a correlation between DAPSA and capillary tortuosity of r = 0.403 (P = .078). The reported correlation, although modest, raises the possibility that NFC may serve as a dynamic surrogate of inflammatory burden. If validated longitudinally, NFC could evolve from a descriptive imaging technique into a functional disease-activity adjunct. Abd-Allah et al. also observed significantly less severe avascularity in biologic-treated PsA patients. This finding supports the broader concept that effective systemic therapy may partially reverse microvascular abnormalities and underscores the role of inflammatory cytokines in mediating microvascular damage, indicating therapeutic benefits extending beyond joints and skin. These observations highlight the potential utility of NFC as a tool for monitoring treatment response besides assessing systemic vascular involvement. This observation requires longitudinal follow-up studies.
However, despite its strengths, several limitations remain that warrant further exploration in larger cohorts and across different disease phenotypes. The cross-sectional design of the study also limits the ability to define the temporal sequence of microvascular changes. PsA is a heterogeneous condition that may present as pure axial disease, enthesitis, oligoarthritis, polyarthritis, DIP arthritis, or in its most severe form as arthritis mutilans. Elmesiry et al. have shown that PsA patients with different clinical domains have lower capillary density and larger capillary dimensions as compared to PsO. 6 Another important limitation is the absence of a graded assessment of nail disease severity, which restricts the ability to determine whether progressive nail involvement parallels progressive microvascular damage. In addition, nail involvement itself can mechanically and structurally alter the periungual region, potentially influencing capillaroscopic visualisation and interpretation. Future studies should therefore incorporate validated nail severity scores (e.g., Nail PsO Severity Index) and analyse their relationship with capillaroscopic parameters. This would help clarify whether microvascular abnormalities track with the severity of nail disease or simply with its presence, and whether NFC abnormalities could serve as a surrogate marker of entheso-nail unit inflammation in psoriatic disease.
The influence of factors such as gender, ethnicity, age, disease duration, and diagnostic delay requires further evaluation. In addition, patients with PsA frequently have metabolic syndrome, and the impact of these metabolic factors on microvascular abnormalities needs to be clarified, including their relationship with cardiovascular risk indices. Without adjusted analyses, attribution of findings can be weak. The application of standardised NFC scoring systems 7 may help reduce inter- and intra-observer variability and allow more meaningful utilisation of the numerous capillaroscopic parameters assessed, while appropriate statistical correction for multiple comparisons would help minimise the risk of Type I error.
Where Do We Go from Here?
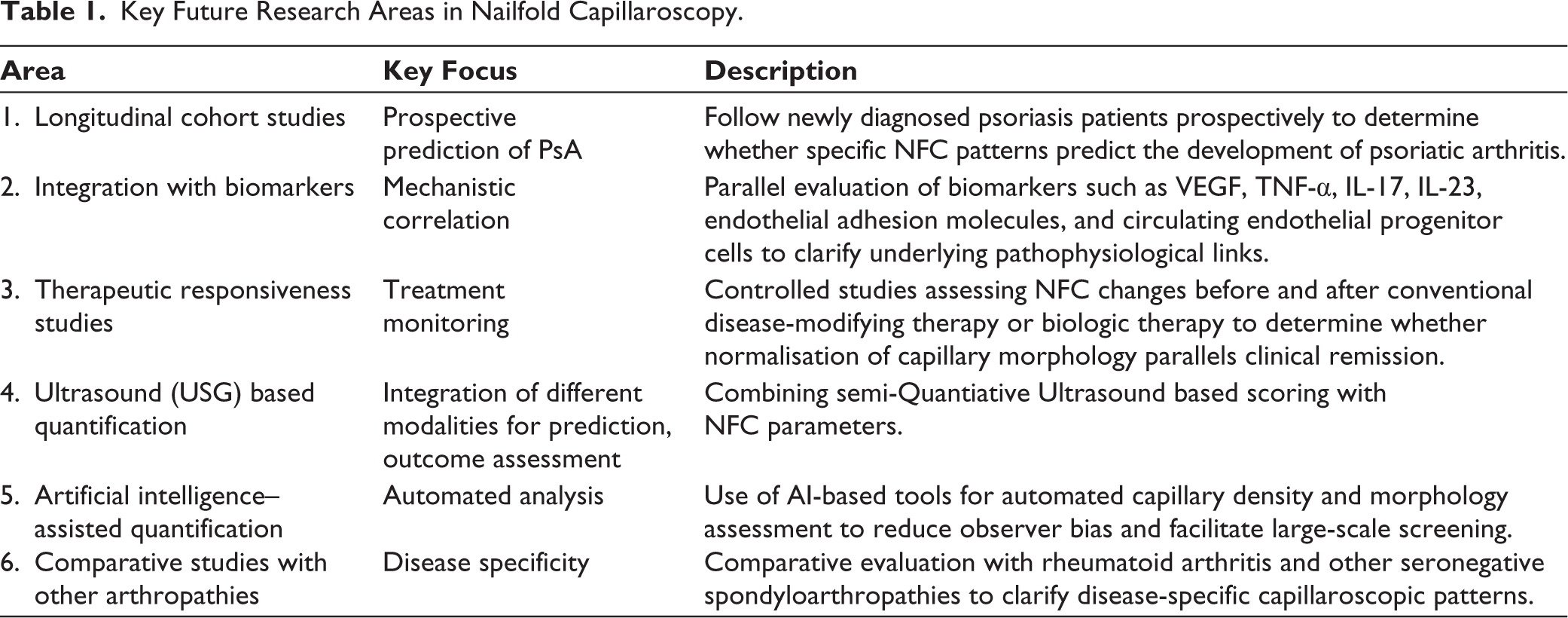
To move NFC from exploratory observation to a clinically actionable tool, future research should prioritise the following (Table 1).
Key Future Research Areas in Nailfold Capillaroscopy.
Conclusion
Abd-Allah et al. contribute meaningful evidence that NFC captures measurable microvascular abnormalities in psoriatic disease. Their findings reinforce the concept of PsO and PsA as systemic inflammatory vasculopathies. However, NFC remains, at present, a promising investigational modality rather than a validated monitoring tool.
The challenge ahead is to determine whether these vascular signatures are epiphenomena of inflammation or predictive biomarkers of disease trajectory. Only longitudinal, mechanistically integrated studies will resolve whether NFC is merely a mirror reflecting inflammation—or a marker capable of guiding precision care (Figure 1).
Timeline of Progression and Utility of Nailfold Capilloscopy (NFC) in Psoriasis (PsO) and Psoriatic Arthritis (PsA).

Footnotes
Declaration of Conflicting Interests
Avinash Jain is an Associate Editor in the journal. Aradhana Singh is a member of the National Editorial Board of the journal. None of them were involved in the decision making process related to this manuscript.