
Abstract
Peripheral spondyloarthritis (pSpA) includes many cases of PsA, ReA, IBD-SpA, and a subset without features of psoriasis, IBD and preceding infection, referred to as ‘pure’ pSpA. It is well documented that peripheral manifestations contribute considerably to the morbidity of SpA. However, despite a lot of advances in the treatment of axSpA with the introduction of newer biological agents targeting IL-17, IL-23, and JAK pathways, pSpA (excluding psoriatic arthritis) remains an area devoid of much research, with only a few clinical trials. In this narrative review, we tried to look into this entity of pSpA, excluding psoriatic arthritis (non-psoriatic pSpA). Future studies should focus on genetics, the development of specific biomarkers, exclusive classification criteria, specific outcome measures, imaging modalities and randomised control trials in pSpA.
Introduction
Spondyloarthritis (SpA) is a group of inflammatory rheumatic disorders having specific clinical features, genetic predispositions, and pathophysiology. It is an umbrella term comprising of a various subtypes, which includes ankylosing spondylitis (AS), psoriatic arthritis (PsA), reactive arthritis (ReA), inflammatory bowel disease-related SpA (IBD-SpA) and undifferentiated SpA.1,2 SpA involves both the axial and peripheral joints; axial manifestations include neck/back pain and stiffness resulting from involvement of spine, facet joints, costovertebral joints and sacroiliac joints; whereas peripheral manifestations comprise arthritis, enthesitis and dactylitis. Accordingly, the classification system by the Assessment of SpA International Society (ASAS) has also divided SpA into axial SpA (axSpA) and peripheral SpA (pSpA). 3
pSpA is a heterogeneous group that includes the entities of PsA, ReA, and IBD-SpA. 4 Pure pSpA is another subset of pSpA (fulfilling the classification criteria of ASAS 2011) with no evidence of IBD, preceding infection, psoriasis (present or past) or family history of psoriasis in a first-degree relative. It is well documented that peripheral manifestations contribute considerably to the morbidity of SpA. 5 However, despite a lot of advances in the treatment of axSpA with the introduction of newer biological agents targeting IL-17, IL-23, and Janus kinase (JAK) pathways, pSpA (excluding PsA) remains an area devoid of much research, with only a few clinical trials. 2 In this narrative review, we tried to look into this entity of pSpA excluding PsA (non-psoriatic pSpA).
Terminology and Classification Criteria
Prior to the ASAS classification criteria, one of the useful and popular composite classification criteria was the European Spondylarthropathy Study Group (ESSG) criteria, which had entry criteria of either inflammatory low back pain or peripheral arthritis (asymmetric oligoarthritis). Once classified as SpA, patients were subsequently classified into AS (if they fulfilled 1984 modified New York criteria), PsA (if they had psoriasis), ReA (if preceded by infection) and IBD arthritis. The remaining patients were bundled into the umbrella term of ‘undifferentiated SpA’.6,7 This comprised both non-radiographic axSpA and pSpA.
ASAS proposed a new classification criterion to separate SpA patients into axSpA in 2009 and pSpA in 2011, respectively. 3 They possibly intended to differentiate SpA into two subsets with no overlap, and proposed that patients should initially be evaluated for fulfilling axSpA criteria, and only then, pSpA criteria could be applied. In other words, patients with severe florid lower limb arthritis with only mild inflammatory back pain would be classified as axSpA rather than pSpA despite the major source of morbidity.
As per ASAS, the criteria for pSpA were to be applied to patients with only peripheral manifestations and no ongoing inflammatory low backache (although past inflammatory low backache was allowed). This was not in keeping with the usual practice of applying labels based on the most prominent clinical manifestation to direct therapy. In the example above, if the patient had severe arthritis, with mild inflammatory back pain, most clinicians would like to apply the label of pSpA, as it captures the current problem and thus directs therapy towards the most prominent issue.
Indeed, many studies and commentators apply the criteria based on predominant involvement. This is apparent in studies like the Clinical Remission in Early peripheral SpA trial (CRESPA), where 35% of pSpA patients had sacroiliitis on magnetic resonance imaging (MRI), and 11.6% had inflammatory backache. 8 Similarly, in the ABILITY-2 trial on adalimumab in non-psoriatic pSpA, the inclusion criteria were based on ongoing arthritis, with exclusion restricted to AS but not those with axial symptoms. 9 Also, the largest study on peripheral manifestations of SpA, the ASAS-PerSpA study, also recruited patients based on ‘best fit’ as determined by a clinician, rather than using a rigid first axial then peripheral approach. 10 They found 55% patients classified as pSpA had axial involvement. Indeed, pSpA classification allows sacroiliitis on imaging, a cardinal feature of axial involvement.
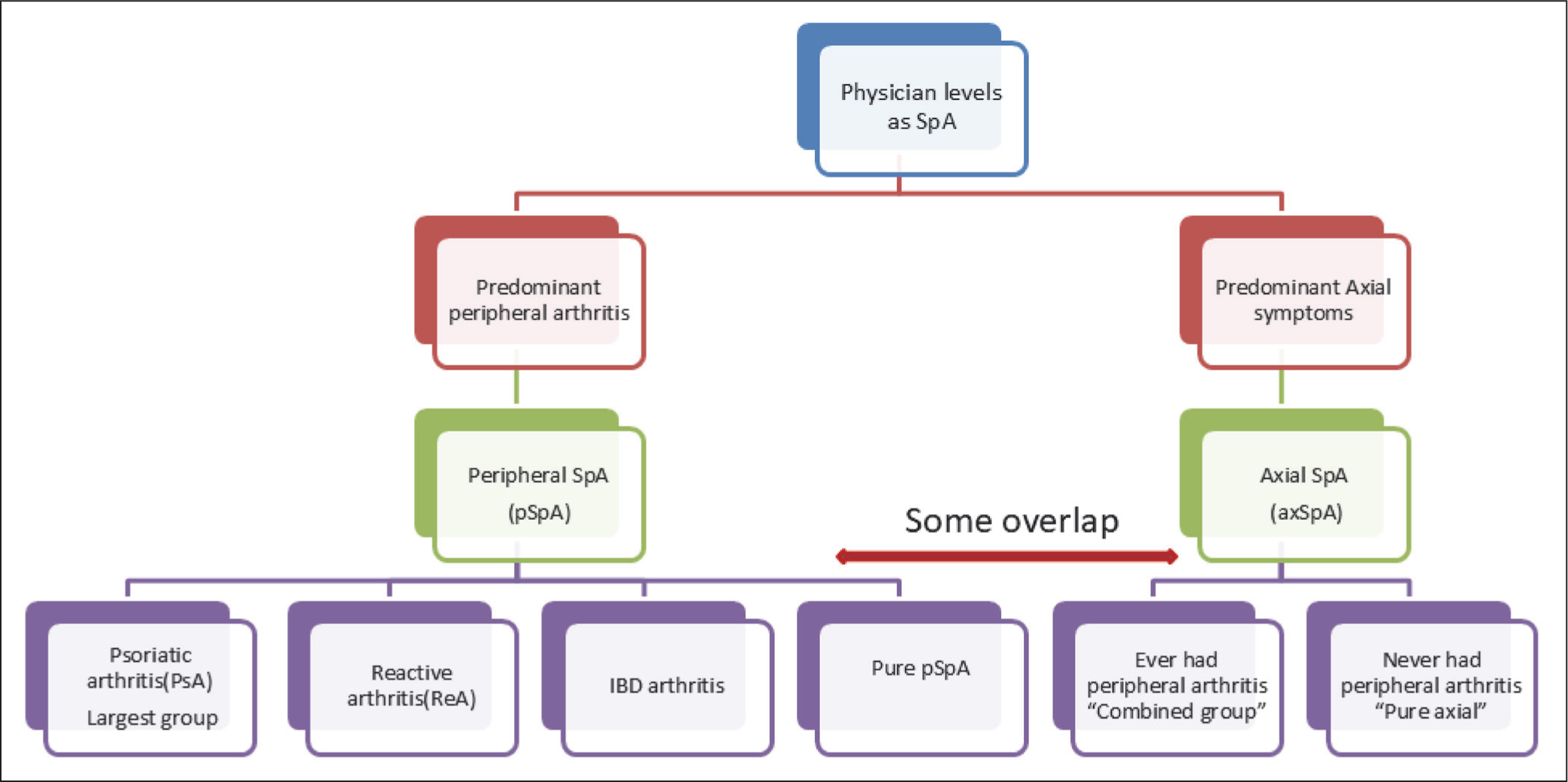
Even in the clinic, most rheumatologists would follow a ‘predominant manifestation’ based terminology, dividing SpA into axial and peripheral, and then, if there is further classification possible, into AS, PsA, ReA or IBD-SpA. Subsequently, this would leave patients who were not further classifiable into a‘pure’ pSpA and ‘pure’axSpA (Figure 1). An important issue is how to classify patients with both ongoing peripheral and axial clinical manifestations. Some authors have labelled this as the ‘combined axial and peripheral group’.
Finally, it must be emphasised that predominant manifestations change with time, and thus labels are temporary (i.e., axial or pSpA). For example, a ‘pure’ pSpA may fall into the category of ‘sine psoriase’ (‘PsA sine psoriasis’) and later can evolve into PsA. Also, there may be a change from axial to peripheral or vice versa. It is difficult to differentiate between PsA sine psoriasis and pure pSpA. PsA sine psoriasis shows higher dactylitis, HLA -Cw6 positivity and DIP joint involvement. Pure pSpA is associated with male predominance, higher HLA B27, more enthesitis and lower limb predominant arthritis. 11
Magnitude of the pSpA
SpA has a general prevalence of 0.9%–1.7% with variation across different studies. 12 In a systematic review and meta-regression analysis on the global prevalence of SpA by Carmen et al., the prevalence is 0.2%–1.61% across various geographical areas. For the subgroups, ReA ranges from 0% to 0.2%, SpA related to IBD ranges from 0 to 0.1% and undifferentiated SpA from 0% to 0.7%. 13
The prevalence of peripheral arthritis in SpA depends on the initial ASAS classification of patients. Among patients classified as pSpA, arthritis occurs in 96%–98%. 8 In patients classified as axSpA, peripheral arthritis lies between 22% and 30%. 14 This is based on data from three major cohorts: the Spanish Esperanza cohort (22.8%), Dutch SpA cohort (26.8%) and the Belgian Be-Giant cohort (28.5%).11,15 There have been some cross-sectional studies as well; De Winter et al., in their cross-sectional study of 314 patients, reported that 230 and 84 fulfilled axial and pSpA criteria. Among axSpA, 51% had combined disease, that is, had peripheral manifestations. 14
The ASAS-PerSpA is the largest study to assess the occurrence of peripheral manifestations in SpA. This cross-sectional study included 4465 patients diagnosed by rheumatologists across 26 centres as axSpA, pSpA or PsA. It found 78% of patients had peripheral manifestations (ever) and 57% had peripheral arthritis (ever). Among the various subgroups, axSpA, pSpA and PsA had peripheral arthritis in 36%, 95% and 91%, respectively. The prevalence of monoarticular, oligoarticular, and polyarticular involvement was 12%, 44% and 44%, respectively. Interestingly, the classic ‘lower limb large joint arthritis’ was only present in 39% of total peripheral arthritis patients. In PsA, polyarticular involvement was most common (60%), whereas oligoarticular disease was common in ReA and IBD-SpA (68%). The data on the epidemiology of peripheral arthritis in IBD is limited, but estimated to be approximately 12%–13%.16,17
In the above study, enthesitis occurred in 44% of all SpA patients overall, with a notably high prevalence in the pSpA subgroup. Enthesitis ranged from 41% in axSpA to 65% in juvenile SpA. Heel enthesitis was seen in 69% of the patients, with 17% confirmed on imaging and 18% active enthesitis by the Maastricht Enthesitis Index. Dactylitis occurred in 15% of all patients, with higher occurrence in PsA. Fingers were affected more than toes (62% vs. 59%) with an overlap in 21% of the cases. A meta-analysis found pooled prevalence rates of arthritis, enthesitis and dactylitis of 22.9%, 13.6% and 5.6%, respectively. 18
Acute anterior uveitis is the most common extra-articular manifestation, with an estimated prevalence of 15%–25%. 19 Prevalence is less in pSpA, as compared to axSpA, with a prevalence of about 17%. 10 Less prevalence is observed in PsA and IBD subtypes of pSpA. HLA B27 positivity strongly correlates with the risk of acute anterior uveitis, with a stronger association with pSpA. In the ASAS Per-SpA cohort, 146 (4.6%) had IBD, as confirmed by endoscopy, though prevalence in pSpA is not reported.
Genetics of pSpA
It must be re-emphasised that pSpA is a heterogeneous group of diseases which vary from PsA, IBD arthritis, ReA to pure pSpA. Thus, it is not surprising that the prevalence of human leucocyte antigen (HLA)-B27 in pSpA is lower and ranges from 27% to 47%,15,18 unlike AS and axSpA, where it is 90%–95%. Interestingly, a large cohort of pSpA patients, including PsA, found that HLA-B27 positivity was associated with root joint involvement, polyarticular joint pattern and tarsitis. 20 HLA B27 positive patients were associated with male predominance, had earlier disease onset and a shorter diagnostic delay. They had a higher frequency of axial involvement, radiographic sacroiliitis, enthesitis and uveitis.
Looking at association with other HLA-B genes, one study from Colombia with a relatively small sample size found that HLA-B15 is associated with peripheral arthritis predominant SpA. 21 However, this has not been replicated in larger multiethnic cohorts.
The genetics of PsA is out of the scope of this review, but briefly, HLAC*0602 has a strong association with psoriasis per se (rather than PsA). HLAB*38 and 39 have been found to be associated with psoriatic pSpA in some studies. Among non-HLA genes, IL23R, IL12B, TYK2, TRAF3IP2 and STAT3 have strong signals in GWAS of PsA. Again, there are GWAS on IBD, but they specifically lack any stratification for IBD arthritis.
To reiterate, apart from PsA, there is no large GWAS or study which has looked at the genetic association of pSpA as a group. 22
Interplay of Cytokines
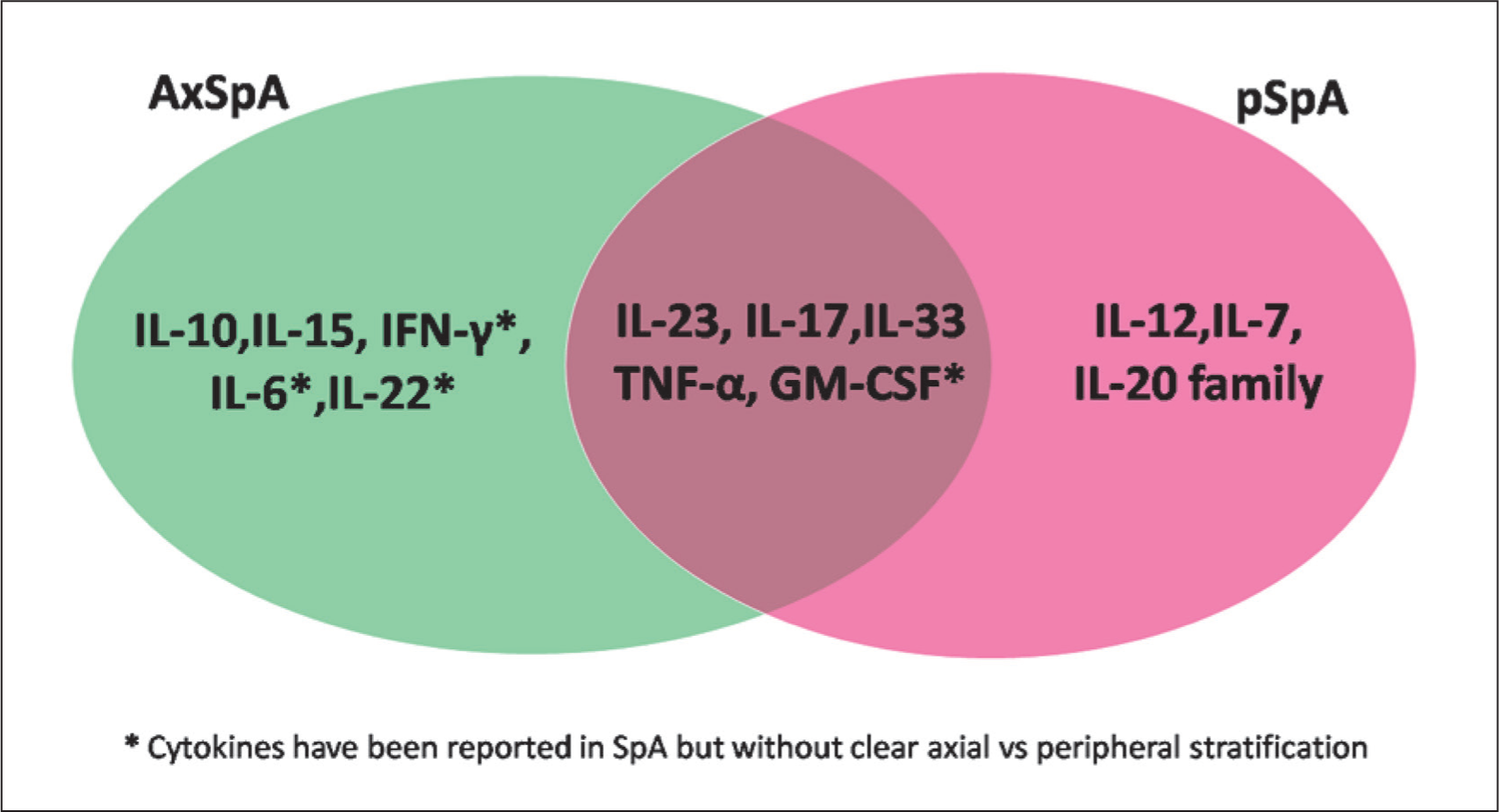
Cytokine interactions are central to the pathogenesis of axial and pSpA. Major pro-inflammatory mediators—including TNF-α, IL-7, IL-10, IL-12, IL-15, IL-17, members of the IL-20 family, and IL-23—contribute to the differentiation of axial and peripheral phenotypes by activating distinct yet overlapping inflammatory pathways. However, the roles of certain cytokines remain incompletely defined; in particular, IL-6, IL-22, and IFN-γ in axial disease, as well as IL-33 and GM-CSF in both axial and peripheral forms, continue to be subjects of ongoing investigation23–27 (Figure 2).
Schematic Representation of Cytokine Interactions Contributing to Inflammation in Axial and Peripheral Spondyloarthritis.23–27
NSAIDS
It has been suggested that the initial therapy of peripheral arthritis be monotherapy with Nonsteroidal anti-inflammatory drugs (NSAIDs) (similar to the initial strategy for axial symptoms). However, most clinicians would consider a trial of NSAIDs monotherapy only in patients with limited disease, that is, only mild peripheral oligoarticular involvement.2,28 In the cases with severe or extensive arthritis, most rheumatologists would probably go for other therapies as an anchor (like those detailed later) with additional NSAIDs to relieve pain and stiffness and improve mobility. In case of enthesitis and dactylitis, NSAIDs continue to be the first-line therapy, although this would depend on the severity and morbidity.
Glucocorticoids (Systemic and Intraarticular)
Low-dose oral steroids are often used in the management of peripheral arthritis of SpA in resource-limited settings in the presence of morbidity like persisting pain not fully responding to NSAIDs, difficulty in walking or performing activities of daily living. 29 This is akin to the strategy for patients of florid active rheumatoid arthritis to ‘bridge’ for a few weeks till the action of disease-modifying antirheumatic drugs (DMARDs) sets in.
To bridge the evidence gap of this strategy in peripheral arthritis of SpA, we conducted a pilot randomised controlled trial (RCT) on the efficacy of oral steroids on non-psoriatic pSpA over 24 weeks. The study included 94 patients, but failed to achieve its primary or secondary endpoints. However, it showed a trend of benefit to oral steroids, with numerically higher ACR50 at both 12 and 24 weeks in the steroid group (by 10%–12%) and numerically lower need for rescue therapy in the steroid group. It is pertinent to mention that this study used a higher dose of glucocorticoids upfront (starting dose at 30 mg), which was tapered to maintenance (or low dose) by 6 weeks (of 5 mg prednisolone) and continued for the remainder of the trial. An important finding in that study was the significant adverse effects of glucocorticoids even in young pSpA, namely hyperglycaemia and hypertension. 30
Intra-articular injections of glucocorticoids are often used in clinical practice, especially for monoarthritis and oligoarthritis as a standard of care. A systematic review on the role of glucocorticoids found four studies that reported on the efficacy of intra-articular steroids in SpA and concluded these to be effective. 31
Conventional Synthetic DMARDs
Among the csDMARDs, sulfasalazine has the strongest evidence for treatment of peripheral arthritis in SpA. However, this evidence is from studies on PsA. In one study of psoriatic SpA, sulfasalazine had a beneficial effect on patients’ and physicians’ overall assessments, pain, morning stiffness and number of inflamed joints. 32 In another study, patients with persistent peripheral arthritis responded well to sulfasalazine. 33 Evidence for other csDMARDs like methotrexate and leflunomide is also from the treatment of peripheral arthritis in psoriatic SpA. 28
The 2019 update of ACR recommends treatment with sulfasalazine or methotrexate, stressing that there is more evidence in favour of sulfasalazine for peripheral arthritis. 34 EULAR guidelines 2022 also recommend csDMARDs for peripheral arthritis in SpA, with sulfasalazine being the preferred option. 35 A review article suggests that either methotrexate, sulfasalazine or leflunomide can be tried for peripheral arthritis in SpA. 2 Methotrexate may have some efficacy in enthesitis and dactylitis based on indirect evidence from SEAM -PsA study and other RCTs for PsA.36,37
Biological DMARDs
In comparison to csDMARDs, biological DMARDs have robust evidence in the management of peripheral arthritis in SpA.
There is evidence with regard to both Tumour necrosis factor inhibitors (TNFi) and Interleukin-7 inhibitors (IL-17i) in non-psoriatic pSpA. In an RCT in 40 SpA patients with peripheral arthritis, adalimumab led to significant improvement in swollen joint counts (SJC) compared to placebo. 38 Another RCT, ‘Ability 2’ included 183 patients with non-psoriatic pSpA and found that adalimumab significantly improved physical function and higher PSpARC40 response compared to placebo (39% vs. 20%; P = .006). 9 The CRESPA trial also found golimumab to be efficacious (compared to placebo) in peripheral manifestations. 8 Almost 50% of patients had drug-free remission in this trial.
However, there are no studies on IL-17 inhibitors in non-psoriatic peripheral arthritis in SpA, and most of the efficacy data on peripheral manifestations comes from studies in PsA (and AS).39–41 A note of caution is warranted as IL-17 inhibitors may lead to exacerbation of IBD and are not recommended in peripheral arthritis in this disease. 42
Targeted Synthetic DMARDs
JAK inhibitors have found great success in the treatment of axSpA and PsA. Two JAK inhibitors, tofacitinib and upadacitinib, are already FDA approved for the treatment of radiographic SpA 39 and PsA, but not in non-psoriatic SpA.
There are no specific studies of JAK inhibitors in peripheral arthritis in SpA. In a Phase 2 RCT dose-ranging study of tofacitinib in AS by Vander Heijde et al., in the subset of peripheral arthritis, there was no significant change in mean swollen joints at 12 weeks compared to baseline. 43 Even in the landmark Phase 3 trial, which led to its approval in axSpA, there was no significant difference noted in SJC between the tofacitinib and placebo group at week 16 and in the open-label extension phase. 44 However, it is difficult to draw conclusions as these trials were clearly not powered to assess a statistically significant difference, and clearly larger studies are needed in this area. So, evidence for JAK inhibitors is based on RCTs in PsA. 45 Summary of current evidence of various therapies for other peripheral manifestations of pSpA is summarised in Table 1.
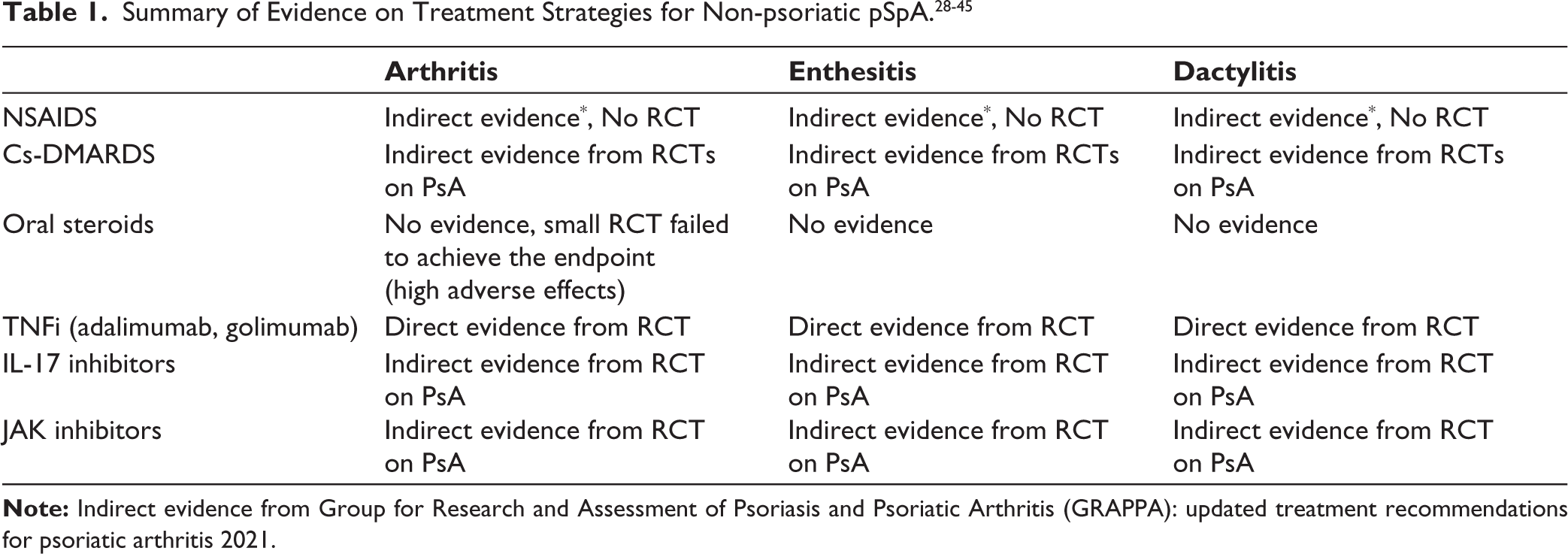
A summary of the current status of evidence of various therapies in peripheral manifestations of SpA is presented in Table 1.
Challenges and Unmet Needs
Imaging in pSpA
Although a lot of advances have been made in imaging in axSpA with various scoring systems, the role of imaging in pSpA is poorly understood. Musculoskeletal ultrasound remains widely used as a non-invasive imaging to detect synovitis, tenosynovitis and enthesitis. Though a few scoring systems are validated for PsA, their utility in non-psoriatic SpA is questionable. 46 MRI may help in better assessment of the extent of inflammation and soft tissue involvement, and AI-based deep learning algorithms based on MRI are also emerging as a potentially useful tool. 47
Lack of Composite Outcome Measures
While there are numerous outcome measures for PsA, these are lacking in non-psoriatic SpA. Outcomes measures for axial SpA, like Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Ankylosing Spondylitis Disease Activity Score (ASDAS), have notable limitations in pSpA by underweighting peripheral joint, enthesitis, and dactylitis. In PsA, both of these outcome measures fail to discriminate pure pSpA activity. 48 Various outcome measures used as per data from two major RCTs were continuous outcome measures, including patients’ global assessment (PGA)/physician’s global assessment of disease (PhGA), C-reactive protein (CRP), tender joint counts (TJC)/SJC, BASDAI and ASDAS. Dichotomous response criteria included Peripheral SpondyloArthritis Response Criteria (PSpARC), American College of Rheumatology (ACR), ASDAS and BASDAI response criteria. 49
pSpA 40% Response Criterion’ (PSpARC40) was the first composite outcome measure introduced for SpA, used in ABILITY 2 trial. It is defined as ≥40% improvement from baseline (≥20 mm absolute improvement), respectively, in the Visual Analogue Scale (VAS) scores for PGA of disease activity and PGA of pain on a 100 mm VAS and ≥40% improvement in at least one of the following scores-76 SJC and 78 TJC; total enthesitis count or dactylitis count. 9 PGA was used as an outcome measure in the TIPES trial. A study by Maureen C Turina et al. tried to find out the discriminatory capacity of these outcome measures. Among the status measures evaluated for disease activity, ASDAS-CRP, BASDAI, PGA, patient global pain, and PhGA consistently had both the highest sensitivity to change from baseline and the highest level of discriminatory ability. Regarding the response criteria, in both trials, ACR20 and PSpARC50/70 performed best in terms of discrimination.49,50 In a post hoc analysis of the CRESPA trial by Lopez -Medina et al., composite and global outcome measurement instruments performed well in pSpA. Composite scores like the Disease Activity Index for Psoriatic Arthritis (DAPSA), ASDAS and BASDAI showed better construct validity. The clinical remission definition (absence of arthritis, enthesitis and dactylitis) was the most discriminatory response criterion. 51 However, the lack of good outcome measures is still a hindrance to future RCTs and further research in this domain.
Need for a New Classification Criterion
Already, a newer classification criterion for axSpA with more specificity is underway to take care of the high burden of back pain. The global Classification in Axial Spondyloarthritis Inception Cohort (CLASSIC) study recruited 1,015 patients under 45 with chronic back pain from 61 centres across 27 countries to validate the 2009 criteria with the aim of increasing the specificity. The cohort was divided into training and validation sets. Diagnostic criteria were applied at five stages. Revised criteria were refined through statistical modelling methods like least absolute shrinkage and selection operator (LASSO), multivariable logistic regression (MLR), expert consensus, voting by ASAS and SPARTAN members. The new classification criteria propose a point-based system with more weightage for imaging (MRI indicative of axSpA-8 points, radiographic sacroiliitis as modified New York criteria-7 points), HLA B27 positivity (4 points) and inflammatory low back ache (3 points) and less reliance on broader SpA features (1 point each). Among SpA features, dactylitis was replaced by increased CRP. A cut-off ≥11 points is required to classify a patient with axSpA. The proposed new classification criteria achieved 79.5% sensitivity and 90.4% specificity. While the new classification criteria have high specificity, enhance homogeneity in research studies, the limitation is a small decrease in sensitivity, missing a few non-radiographic early SpA cases. Similar exclusive classification criteria for pSpA are an unmet need. 52
Future Directions
While a lot of advances have been made in axSpA and PsA, peripheral manifestations in SpA remain relatively neglected. Although the pathophysiology and genetics of PsA are extensively studied, there are no studies in pure pSpA. There are no biomarkers or specific imaging to diagnose or distinguish this entity from psoriatic SpA. Furthermore, the lack of exclusive classification/diagnostic criteria for pSpA leads to underestimation of the true prevalence of the disease. Apart from PSpARC, no composite outcome measures have been developed so far, and it is, in turn, a hindrance to randomised control trials in this area. There are only a few RCTs on biological treatments in pSpA (only on adalimumab and golimumab). There is a pressing requirement for more RCTs on treatment strategies. Hence, future studies should focus on genetics, development of specific biomarkers, exclusive classification criteria, specific outcome measures, imaging modalities and randomised control trials in pSpA.
Footnotes
Authors’ Contribution
The first authors, SJ and VD, are the first authors of the manuscript. Concept design and manuscript drafting: VD and SJ. Review and revision: SJ, VD, CBP, BL.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval was not required for this study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Not applicable.