
Abstract

The Case
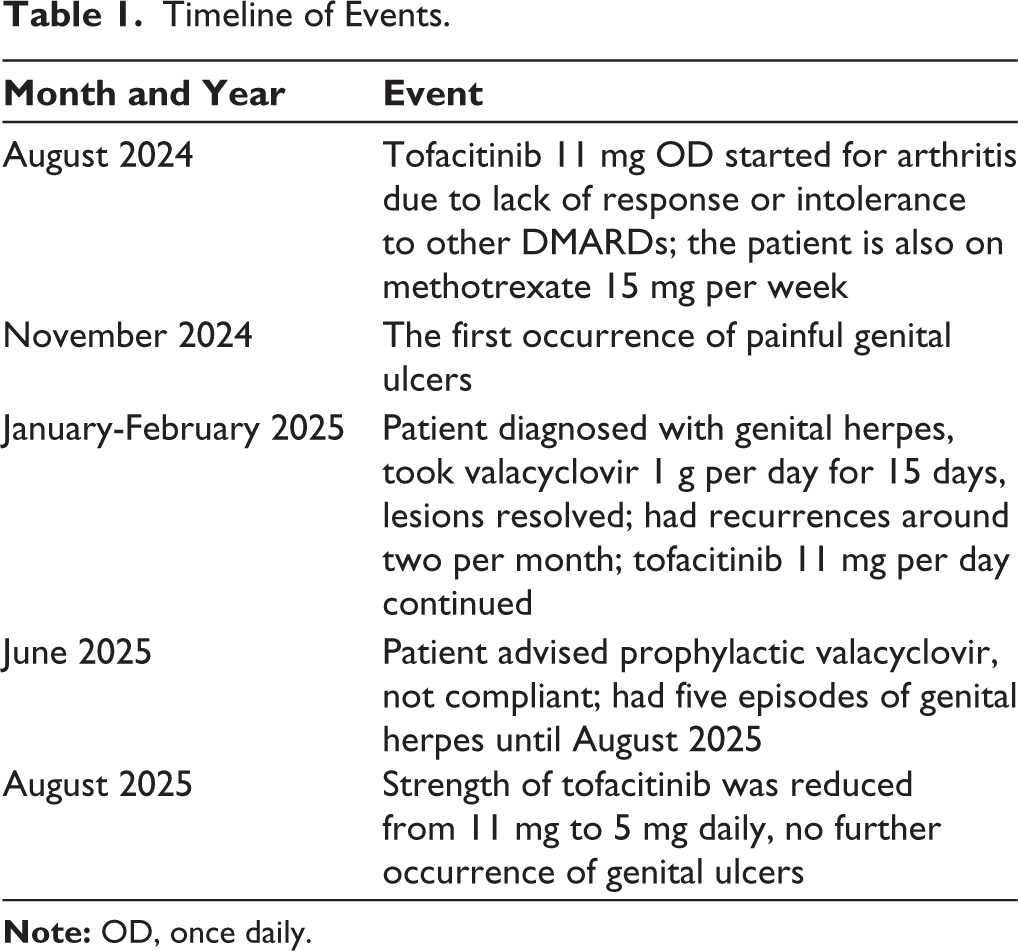
A 55-year-old lady was under our treatment for rhupus for over 25 years. She had seropositive inflammatory arthritis with mucocutaneous features of lupus. Because of inadequate response or adverse effects of other disease-modifying anti-rheumatic drugs (DMARDs), she was started on tofacitinib 11 mg once daily for the arthritis. She was also on oral methotrexate 15 mg once a week. She was not receiving glucocorticoids.
After approximately three months of receiving tofacitinib 11 mg daily, she developed painful, itchy vulvovaginal ulcers. The lesions were eventually diagnosed a few months later as genital herpes by a qualified dermatologist. Other causes such as syphilis, HIV and cervical neoplasm were excluded.
She had no prior history of herpes and was not vaccinated. She initially took oral valacyclovir 1 g once daily for 15 days, during which the lesions resolved. However, she had recurrences at an average frequency of two per month, for which she took valacyclovir once daily for 3–7 days. She continued to take tofacitinib. She was advised prophylactic valacyclovir 500 mg once daily in June 2025 by the dermatologist. However, she was non-compliant with the same. She had five episodes of genital herpes from June to August 2025, each one prompting her to take a three-day course of valacyclovir 1 g daily (Table 1). During her routine follow-up in August 2025, we reduced the dose of tofacitinib from 11 mg to 5 mg daily, after which she had no further episodes of genital herpes to date. She also had no flare-up of the arthritis.
Timeline of Events.
Discussion
Infection risk is an established concern with Janus kinase (JAK) inhibitors. The inhibition of the JAK/signal transducer and activator of transcription (STAT) pathway impairs interferon-mediated antiviral immunity and reduces T-cell/natural killer (NK) cell surveillance, allowing reactivation of the dormant virus. 1 An increased incidence of herpes zoster infection is well recognised, but evidence for herpes simplex virus (HSV) infection remains limited and less conclusive.2,3 Risk factors that can affect herpes zoster and herpes simplex infections for patients receiving JAK inhibitors include age, glucocorticoid exposure, other combined therapy, and underlying immunologic dysregulation. 3 While isolated cases of HSV reactivation have been reported with JAK inhibitors,4,5 to the best of our knowledge, recurrent genital herpes has not been previously described. As per a meta-analysis of infection risk with JAK inhibitors in dermatoses, there was no overall increased risk of herpes simplex infections (OR: 1.43, 95% CI: 0.93-2.23, P = .102) compared to placebo, with no significant difference based on the mechanism (P = .77), or class of the JAK inhibitor. 6
This case highlights the need for clinician awareness regarding the risk of HSV reactivation in patients on JAK inhibitors. Prompt recognition and antiviral therapy are essential. In cases of recurrent HSV infection, dose reduction or temporary discontinuation of the JAK inhibitor may be considered, balancing infection risk with disease control.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from the patient for the publication of this case report.