
Abstract
Access to adequate sanitation facilities is a basic human right and fundamental to good health. Inadequate and unhygienic sanitation practices have severe consequences for public health and socio-economic development. This study examines the levels and trends in access to latrine facilities, spatial variations and the associated socio-economic factors in India. Data drawn from the National Sample Survey Organization’s (NSSO) 69th (2012) and 76th rounds (2018) were used in this study. Moran’s ‘I’ statistic and Local Indicators of Spatial Association (LISA) were applied to assess the spatial variations in access to latrine facilities. Bivariate and multivariate logistic regressions were employed to examine the factors associated with latrine use. The findings revealed that access to sanitation facilities is unsatisfactory, and there is a huge rural–urban gap in latrine use. Unequal access among socio-economic groups is also very prominent. The study found substantial geographical variations in latrine use across the country; open defecation is highly prevalent in eastern and central regions of the country, while the north and north-eastern regions have better access to latrine facilities. Factors like education, occupation, socio-religious affiliation, water availability, and economic status are significant determinants of accessibility to latrine. It is recommended that targeted interventions for the socio-economically disadvantaged groups, spreading awareness about the importance of latrine use and hygienic practices, and proper assistance for construction and maintenance of toilets could be helpful to combat the harmful practice of open defecation and ensure adequate and equitable sanitation for all.
Introduction
Access to adequate sanitation is fundamental to good health (Esrey et al., 1991). United Nations General Assembly recognises access to sanitation as a basic human right and entitles ‘everyone, without discrimination, to have physical and affordable access to sanitation, in all spheres of life, that is safe, hygienic, secure, socially and culturally acceptable and that provides privacy and ensures dignity’ (UN, 2016). Improved sanitation facility is essential for the public health, livelihood, and dignity of the households and the entire community (Shukla, 2018). Not only does it play a crucial role in public health and hygiene, but it also contributes to a clean and improved environment and social development and generates significant economic benefits (Bartram et al., 2005; Esrey et al., 1991; Mishra & Shukla, 2015).
Inadequate and unhygienic sanitation practices have severe consequences for public health and human capital development. It causes transmission of infectious diseases, such as cholera, diarrhoea, dysentery, hepatitis A, typhoid and polio that can affect survival, physical growth, cognitive development and adult economic productivity (Esrey et al., 1991). It is alarming to note that every year around 432,000 deaths occur due to preventable water and sanitation-related diarrheal diseases. In addition, poor sanitation is also a major factor for several neglected tropical diseases (WHO, 2019).
The Sustainable Development Goal target 6.2 calls for ‘adequate and equitable sanitation’ for all and aims to end open defecation by 2030. However, the recent WHO/UNICEF Joint Monitoring Programme (2017) reported that only 39% of the global population had access to safely managed sanitation services in 2015, whereas 2.3 billion constituting 30% of the total population still lack basic sanitation services across the world. Moreover, 892 million people worldwide practice open defecation. While open defecation has consistently decreased worldwide, it remains exceptionally prevalent in India as over 524 million people, that is, 58% of those who defecate in open spaces reside in this county alone (WHO & UNICEF, 2017).
Given its paramount importance to public health, sanitation has been given focus by the government of India through various schemes and programmes since the 1980s. Central Rural Sanitation Programme was launched in 1986 to provide sanitation facilities in rural areas. This ‘supply driven, highly subsidy and infrastructure-oriented programme’ was later replaced with the Total Sanitation Campaign in 1999 and again subsumed with Nirmal Bharat Abhiyan in 2012 (Irigoyen, 2017). However, these schemes could not yield a sustained impact on sanitation behaviours. The government of India recently launched Swachh Bharat Mission in 2014 to achieve universal sanitation coverage and make India ‘open-defecation free’ by 2019 (Yogananth & Bhatnagar, 2018). Despite several policies and programme interventions, the accessibility to adequate sanitation facilities remains a major concern in India, and a significant portion of the population still defecates in open spaces. Therefore, there is a need for a comprehensive study on access to sanitation facilities to make more efficient policy interventions for promoting sanitation coverage. To address the inadequate access to sanitation facilities, it is therefore necessary to study the inequity in latrine facilities across regions, states and districts in the country. Nevertheless, the geographical patterns of latrine use and its associated factors have been poorly understood in India. In this context, this study examines the levels and trends in access to latrine facilities in India, spatial variations, and the associated socio-economic factors, using the recent large-scale data from the National Sample Survey Organization’s (NSSO) 69th round (2012) and 76th round (2018) surveys.
Data and Methods
Data Source
This study used data from the National Sample Survey Organization’s 69th (2012) and 76th (2018) rounds, known as ‘Drinking Water, Sanitation, Hygiene, and Housing Condition’ survey. These rounds provide a wide range of latest information on the condition and structure of dwelling units and the facilities with respect to drinking water, sanitation, drainage and garbage disposal. The surveys covered almost the entire country, except for some villages in Andaman and Nicobar Islands, which were difficult to access. As high as 106,838 households (63,736 in rural areas and 43,102 in urban areas) and 95,548 households (53,393 in rural areas and 42,155 in urban areas) were surveyed in 76th round and 69th round, respectively.
Indicators
This study focuses on the accessibility to sanitation facilities, particularly latrine use in India. Access to an improved latrine is considered as the outcome variable in this study. World Health Organization (WHO) defines an improved latrine as the safe removal of human excreta (WHO & UNICEF, 2014). Access to improved latrine was dichotomised into binary groups: the households having flush or pour flush latrine, ventilated improved pit latrine, pit latrine with slab or composting latrine were considered as safe (1), and other traditional types of latrine or no latrine facility as unsafe (0).
A wide range of variables, including socio-economic, demographic and geographic characteristics, were included to assess the factors associated with access to latrine facilities, based on several previous studies conducted in India and other countries (Abubakar, 2018; Adams et al., 2016; Dickinson & Pattanayak, 2009; Gilman et al., 1993; Saroj et al., 2020; Vyas & Spears, 2018; Yogananth & Bhatnagar, 2018). These variables include age (≤30 years, 30–50 years, and >50 years), sex (male and female), educational level (illiterate or no formal education, primary, secondary, and higher) and occupation of household head (primary, secondary and tertiary sector), social group (Scheduled Tribe [ST], Scheduled Caste [SC], Other Backward Classes [OBC] and General), religion (Hindu, Muslims and others), economic status (poorest, poorer, middle, richer and richest), place of residence (urban and rural), housing condition (katcha, semi-pucca and pucca), water availability (within dwelling unit, within premises and outside premises) and region. Economic status of the household was estimated by the monthly per capita consumption expenditure (MPCE) and categorised into five quintile groups: poorest, poorer, middle, richer and richest. Depending on the materials of the wall, roof and floor of the houses, the housing condition was categorised into three groups as katcha, semi-pucca and pucca. Similarly, water availability was examined by the location of the primary water source: within dwelling unit, within premises and outside premises. Based on geographical contiguity and cultural settings, the states and union territories were grouped into six regions to study the regional variations in latrine use. These regions are north, central, eastern, north-eastern, western and southern.
Analytical Strategies
The study assessed the levels and trends of latrine facilities by socio-economic groups, place of residence and states. The geographical variations in access to latrine facilities were discussed across the states and districts of India. Furthermore, Moran’s ‘I’ statistic was estimated and Local Indicators of Spatial Association (LISA) was prepared to understand the spatial clustering of open defecation across the districts in India. Moran’s ‘I’, a commonly used indicator of spatial autocorrelation, ranges from −1 to 1. The value of ‘1’ indicates perfect positive spatial autocorrelation when similar values cluster together and ‘−1’ shows perfect negative spatial autocorrelation with dissimilar values cluster together (Anselin et al., 2006). LISA map represents spatial clusters of high value with similar neighbours (high-high) or hot spots and clusters of low value with similar neighbours (low-low) or cold spots. NSSO 76th Round (2018) provides data for 682 districts in this country; however, four districts have sample size of less than 30. Therefore, the spatial analysis was applied in 678 districts with sample size of at least 30 (Delice, 2010; Springate, 2012). Spatial analyses were carried out using Arc-GIS version 10.2.2 and GeoDa version 1.14.
The study estimated the access to latrine facility by various socio-economic and geographic factors, and the differences were tested using Pearson’s chi-square test. The sample weight was used for the estimation of percentage distribution. Finally, bivariate and multivariate logistic regression models were employed to examine the factors associated with access to latrine facilities. The results of regression analyses are presented by unadjusted and adjusted odds ratios (ORs) with 95% confidence intervals (CIs). All statistical analyses were carried out using STATA version 14 (StataCorp LP, College Station, TX, USA).
Results
Levels and Trends in Access to Latrine Facilities
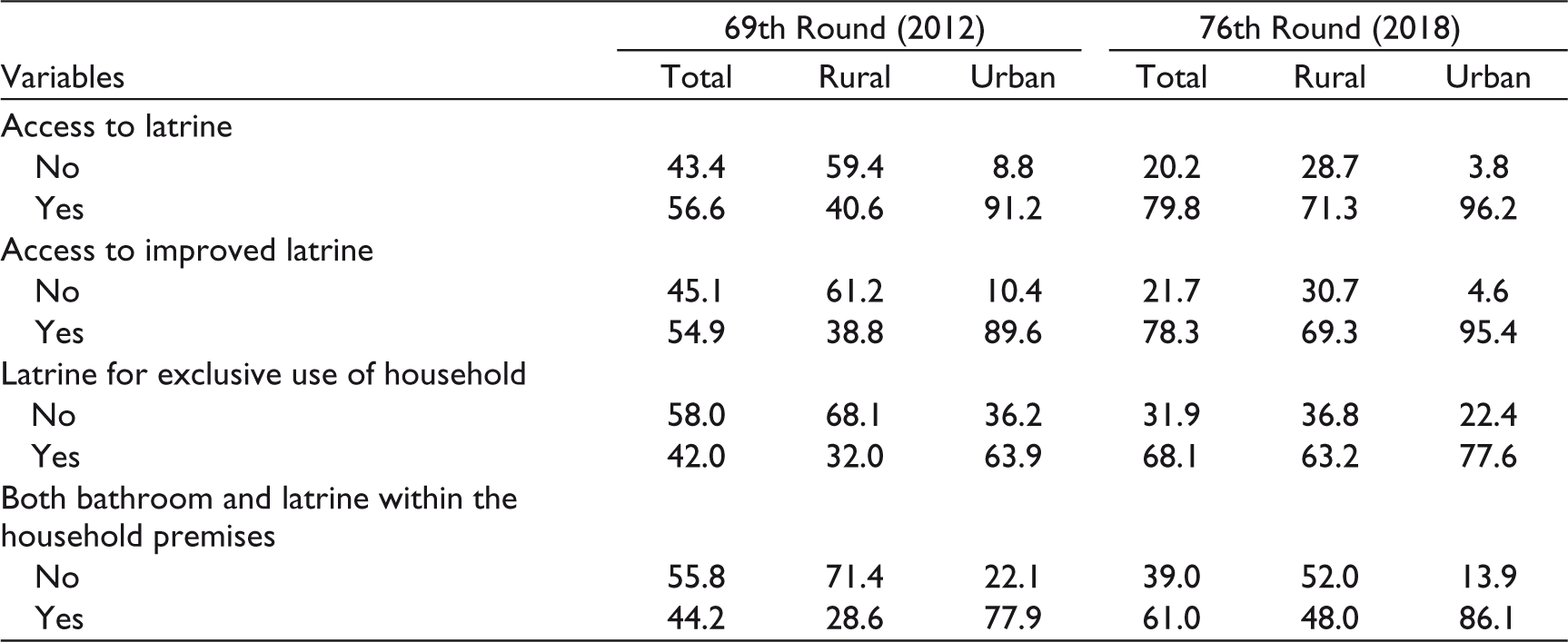
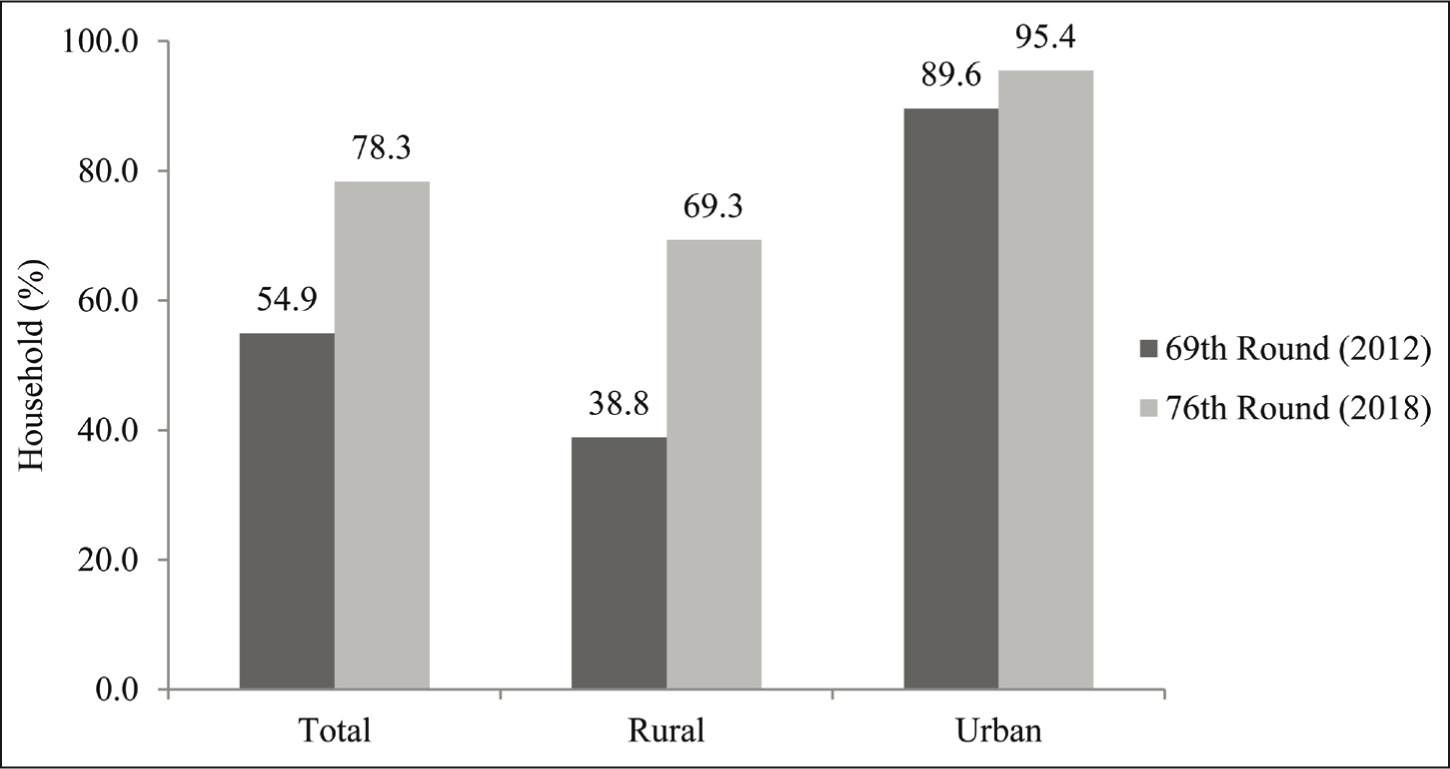
Levels and trends in access to sanitation facilities, particularly latrine facilities, in India are presented in Table 1. It is observed that the sanitation facilities have improved significantly over the period. Around 43.4% of households had no access to any latrine in 2012. There was a significant improvement in the next few years as the figure went down to 20.2% in 2018. Similarly, access to improved latrines has also increased from 54.9% to 78.3% over the same period (Figure 1). Access to latrines for exclusive use of household reported a steady increase to 68.1%, while the figures of shared latrines with other households and public or community latrines showed a declining trend from the previous round (Figure 2). Likewise, almost two-thirds of households reported access to both latrine and bathroom within household premises in 2018.
Percentage of Access to Sanitation Facilities in India.

Unequal Access to Latrine Facilities Among Socio-Economic Groups
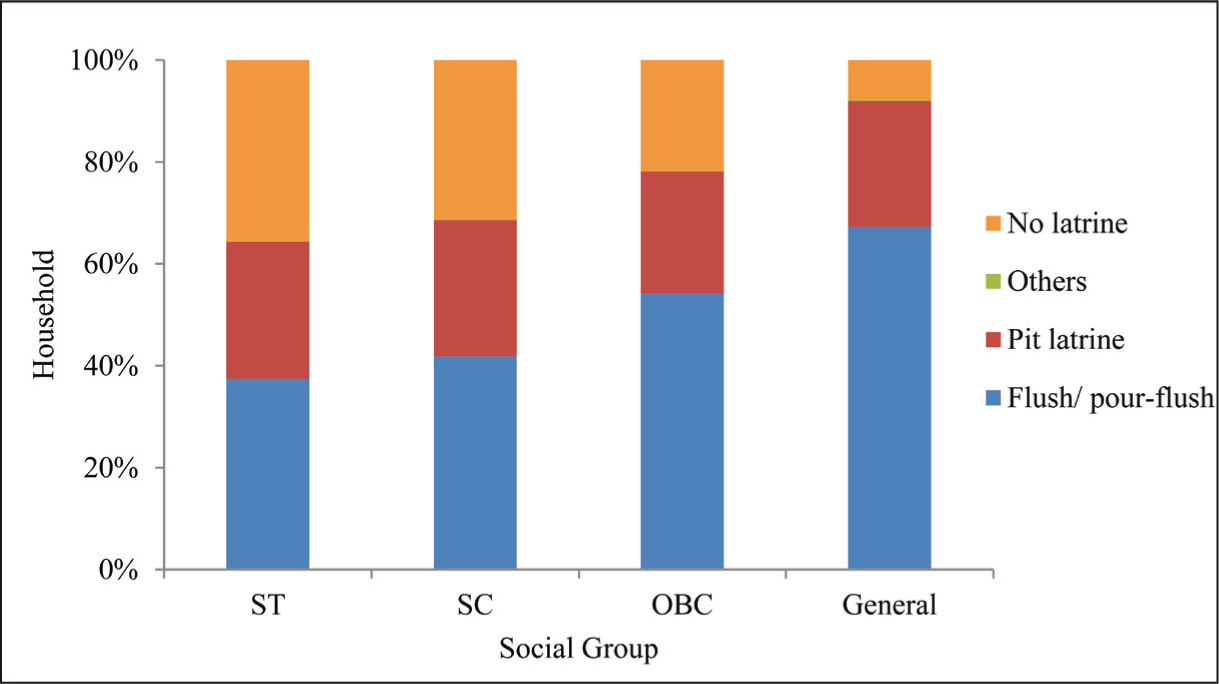
It is observed that there are huge deficits in sanitation facilities at the household levels. As per the latest estimate of the NSSO, 79.8% of households have access to latrine, out of which 53.9% of households use improved flush or pour-flush latrine connected to piped sewer system or septic tank, and 25% use pit latrines (NSSO, 2018). However, there are marked differences among the socio-religious and economic groups in the country (Table 2). Lack of access to improved sanitation facilities poses severe challenges for the socio-economically weaker sections of society. As indicated in Figure 3, more than 67.3% of households in General category had access to improved flush latrine facilities, while the corresponding shares were consistently reduced for OBC (54.2%), SC (41.9%) and ST (37.5%) categories. Contrastingly, the proportion of households without latrine facilities increased from a mere 7.7% in General category to more than 32% among socially weaker sections. It is alarming that around 35.5% of ST households did not have any latrine and practice open defecation. Similarly, access to latrine facilities differs significantly among religious groups. Around 86.9% of Muslim households reported using latrines, whereas 78.1% of households among Hindus used such facilities. With respect to prevalence of open defecation, the differences are more striking as 22.8% of Hindu households defecate in open spaces compared to only 13.5% of Muslims. The differences among different socio-religious groups are not only limited to types of latrines used but also considerable disparities in the location of latrine. When 76% of General households have both latrine and bathroom within premises, the corresponding figures for STs and SCs are only 39.1% and 48.6%, respectively.
Distribution of Latrine Use by Various Socio-Economic Factors in India, 2018.


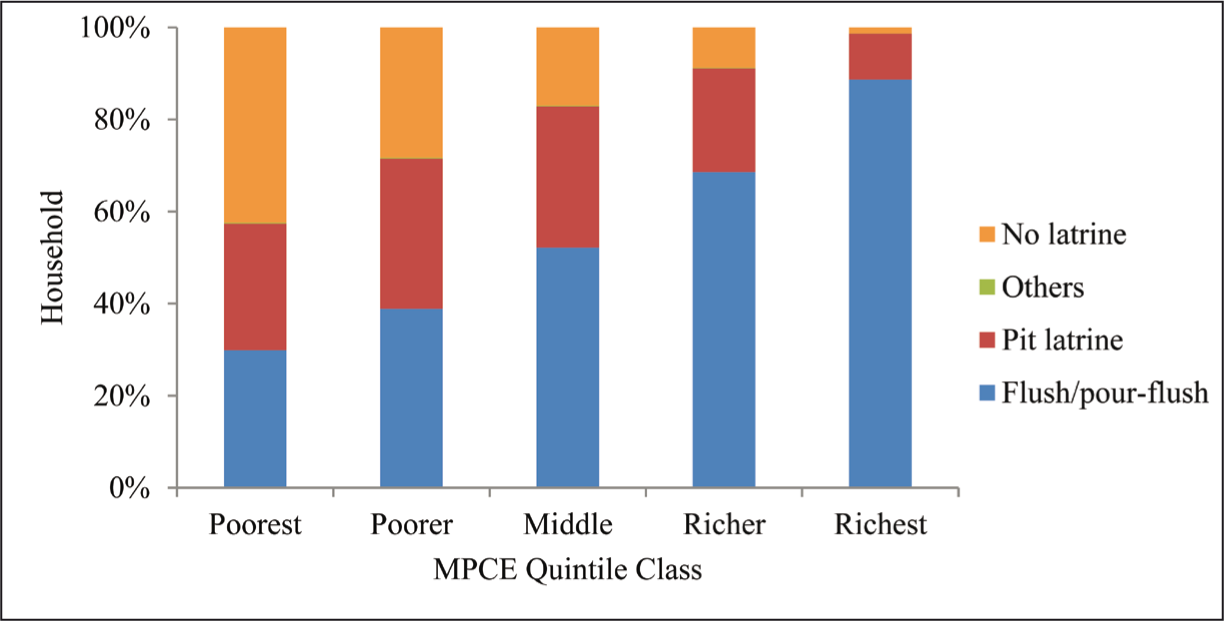
The economic condition of households also plays an important role in access to safe sanitation facilities. Only 59.4% of households from the poorest MPCE quintile group reported using latrines, while as high as 98.8% of households in the richest group had access to latrine facilities. There are huge variations with regard to types of latrines used by different economic groups. Most of the households in the richest group (88.9%) used improved flush or pour-flush latrines, but the corresponding figure reduced consistently with decreasing economic status of the households. Only 29.9% of poorest and 38.9% of poorer households had access to improved flush latrines, while a significant proportion of households of these two groups (27.8% and 32.7%) were found to use unsafe pit latrines (Figure 4). As far as accessibility is concerned, a major chunk of poor households (14.6%) lacked access to household latrines and used shared latrines in the community.
Geographical Variations in Latrine Usage Across States
Figure 5 presents the prevalence of open defecation across the states in India from 2012 to 2018. There are striking regional disparities in access to latrine facilities in this country. The coverage of latrine facilities is relatively higher in the north-eastern region and lower in the central and eastern states of the country (Figure 6). More than 91% of the households for both rural and urban areas in the north-east region had access to improved latrine facilities. The central and eastern regions had relatively lower coverage, and the rural areas were even in worst condition with 59.3% and 64.9% coverage, respectively. The southern and northern parts of the country show a moderate coverage of latrine facilities. In 2018, the north-eastern states, like Nagaland, Sikkim, Mizoram, Manipur reported 100% coverage of latrine facilities within household premises. In contrast, the practice of open defecation is highly prevalent in central and eastern states. Jharkhand reported around 73.9% of households, the highest among the states, defecated openly in 2018, followed by Odisha (71.9%), Bihar (67.4%), Chhattisgarh (65.7%), Madhya Pradesh (60.6%), Uttar Pradesh (60.2%) and Rajasthan (57%). The southern states show a moderate share of households without latrine facilities ranging from 20% to 37%.
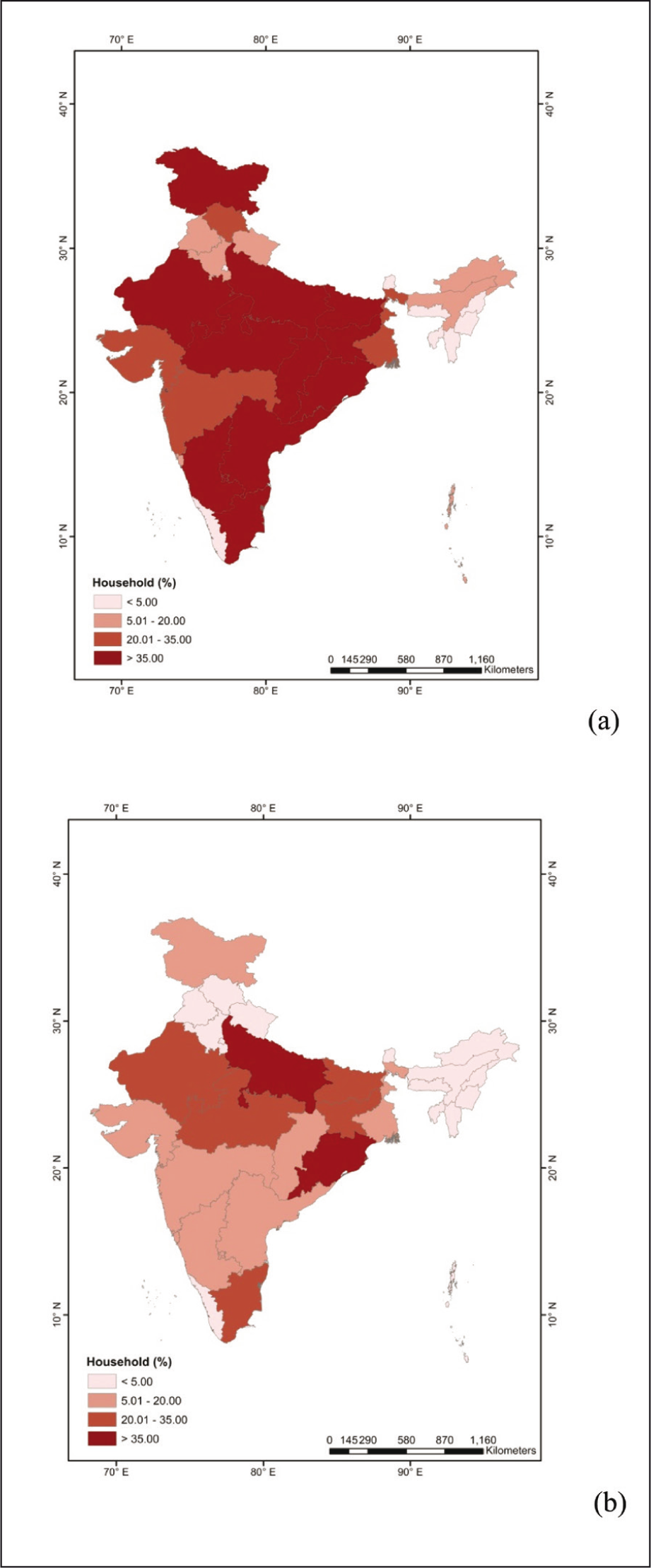
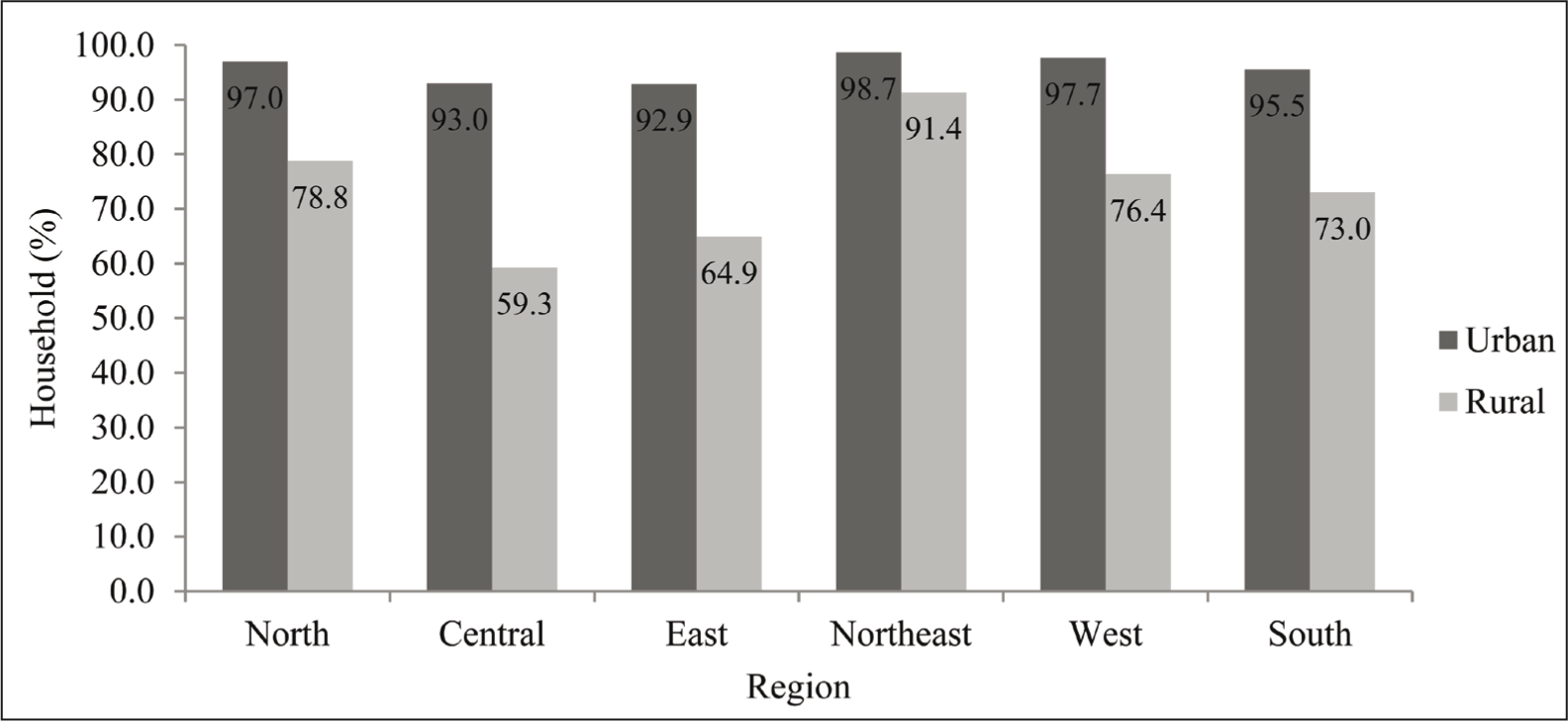
Figure 5 also represents the changes in practice of open defecation over the years between 2012 and 2018. India has witnessed significant improvement in access to latrine facilities over this period; the prevalence of open defecation reduced from 43.8% in 2012 to 20.1% in 2018. However, there are regional disparities among the states. The improvement made by Chhattisgarh was highest in the country over this period with a 58.3% reduction in prevalence of open defecation, followed by Jharkhand, Madhya Pradesh, Bihar and Rajasthan at 40.3%, 38.2%, 34.6% and 30.1%, respectively. Although a considerable improvement was noticed in states like Odisha, Uttar Pradesh, Jharkhand and Bihar, a large chunk of households (more than 30%) was still practicing open defecation.
Spatial Clustering of Open Defecation
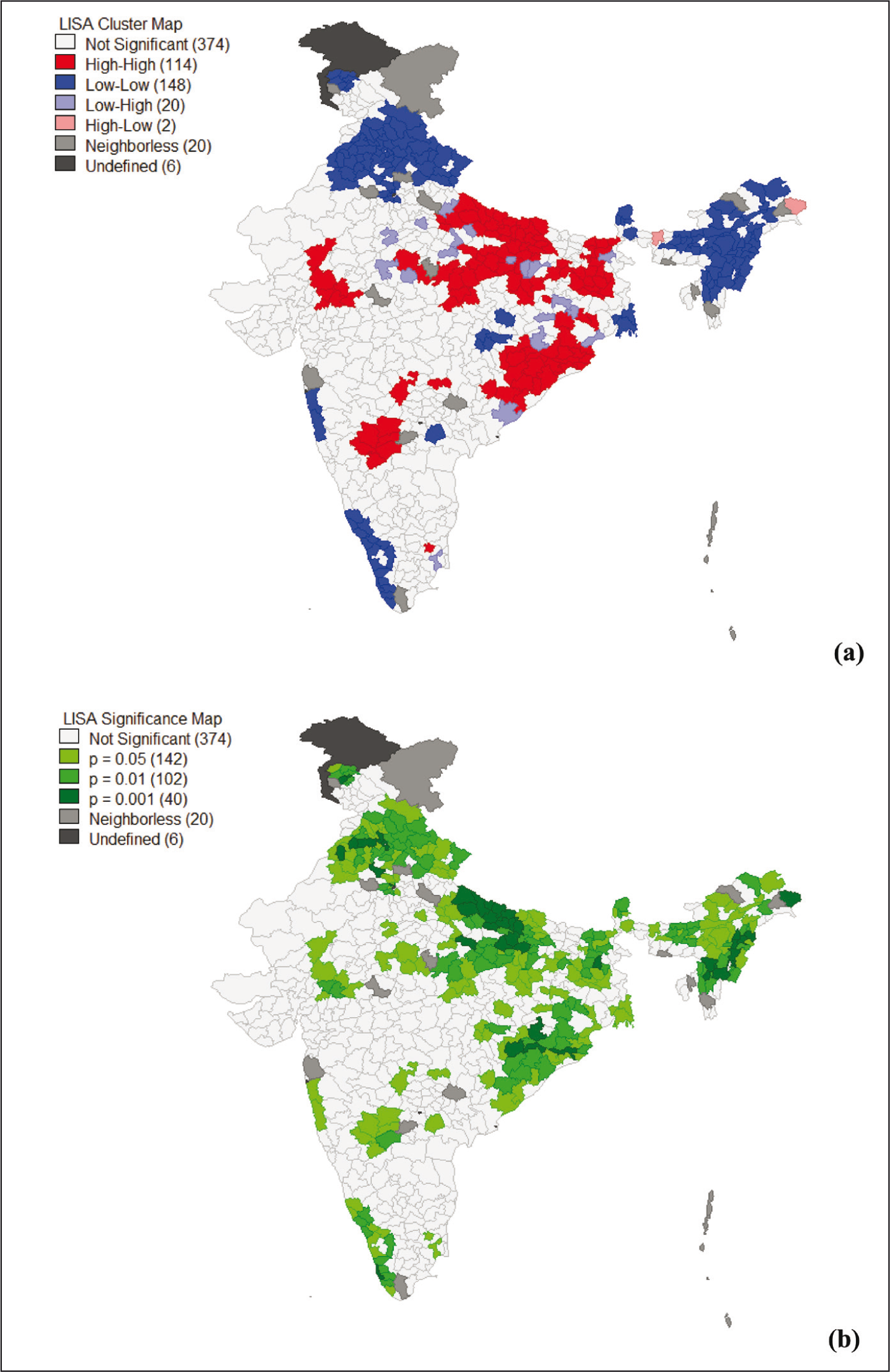
The spatial autocorrelation analysis reveals clustering patterns of open defecation at the district level. The Moran’s ‘I’ value of 0.579 indicates a strong spatial clustering in open defecation across the districts in this country. LISA cluster map, presented in Figure 7, reveals that out of 678 districts, there were 114 hot spots indicating districts with high prevalence of open defecation surrounded by other high-prevalence districts and 148 cold spots, that is, districts with low prevalence of open defecation surrounded by other low-prevalence districts. On the other hand, 374 districts were observed to have insignificant autocorrelation with the neighbouring districts. The clusters with a higher prevalence of open defecation are mostly located in eastern and central regions of the country, comprising the states of Uttar Pradesh, Odisha, Bihar, Jharkhand and Madhya Pradesh. The cold spots with low clusters were found in Himachal Pradesh, Uttarakhand, Punjab and Haryana in the north region and Nagaland, Manipur, Assam and Arunachal Pradesh in north-eastern region of India.
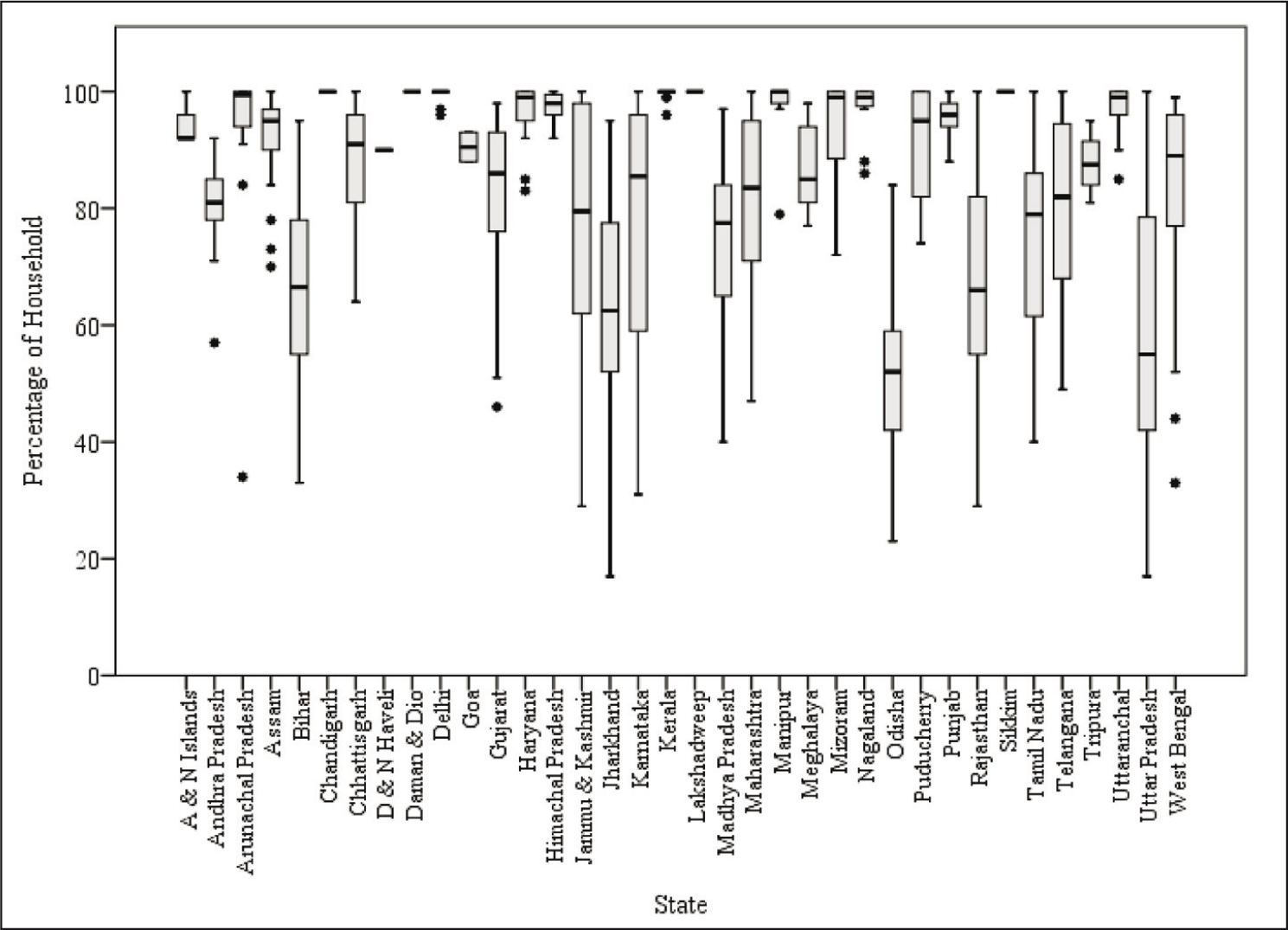
In Figure 8, box plots have been used to further illustrate the marked variations of latrine coverage among the districts in each state of India. They provide an overview of the inter- and intrastate disparities among the districts in access to improved latrines. It is observed that the north, north-eastern and some southern states (i.e., Kerala, Goa) had higher coverage of improved latrine facilities at the district level in 2018. The intra-state variation was also significantly less in these states. On the other hand, the states like Uttar Pradesh, Odisha, Jharkhand, Rajasthan, Bihar and Madhya Pradesh reported low coverage of latrine use. Not only was the average access to safe latrines lesser in these states, but there were also substantial intra-state district level variations. One could figure out some outlier districts in some states in the box plots. The presence of outlier or extreme values in better-performing states of Arunachal Pradesh, Assam, Kerala, Manipur, Nagaland and Mizoram indicates that these two-three districts (i.e., outliers) were lagging from the average coverage in terms of latrine facility.
Factors Associated with Access to Improved Latrines
The results of binary logistic regression model examining the association of various socio-economic and geographical factors with accessibility to latrine facilities are presented in Table 3. Demographic characteristics, socio-religious affiliation, occupation, education, economic status, place of residence, housing condition, water availability and region were considered as important factors in this study. It is observed that the household heads of older ages were more likely to have better sanitation coverage than those below 30 years. The gender of household head was found to be a significant determinant. Compared to the female-headed households, the male-headed households were 13% more likely to use improved latrine facilities (AOR: 0.87, 95% CI: 0.80–0.94). Education is a vital factor in determining the sanitation facility. In comparison to household heads who were illiterate or had no formal education, the household heads with primary (AOR: 1.53, 95% CI 1.47–1.60), higher secondary (AOR: 2.27, 95% CI 2.13–2.41) and graduation or above (AOR: 3.84, 95% CI 3.39–4.37) education had a greater likelihood of using safe latrine. Occupation is observed to be a significant determining factor. Compared to the household heads engaged in primary activities, those who were involved in tertiary activities had more chances of having latrine facilities at house.
Regression Results Showing the Socio-economic and Geographic Factors Associated with Access to Improved Latrine Facilities in India, 2018.
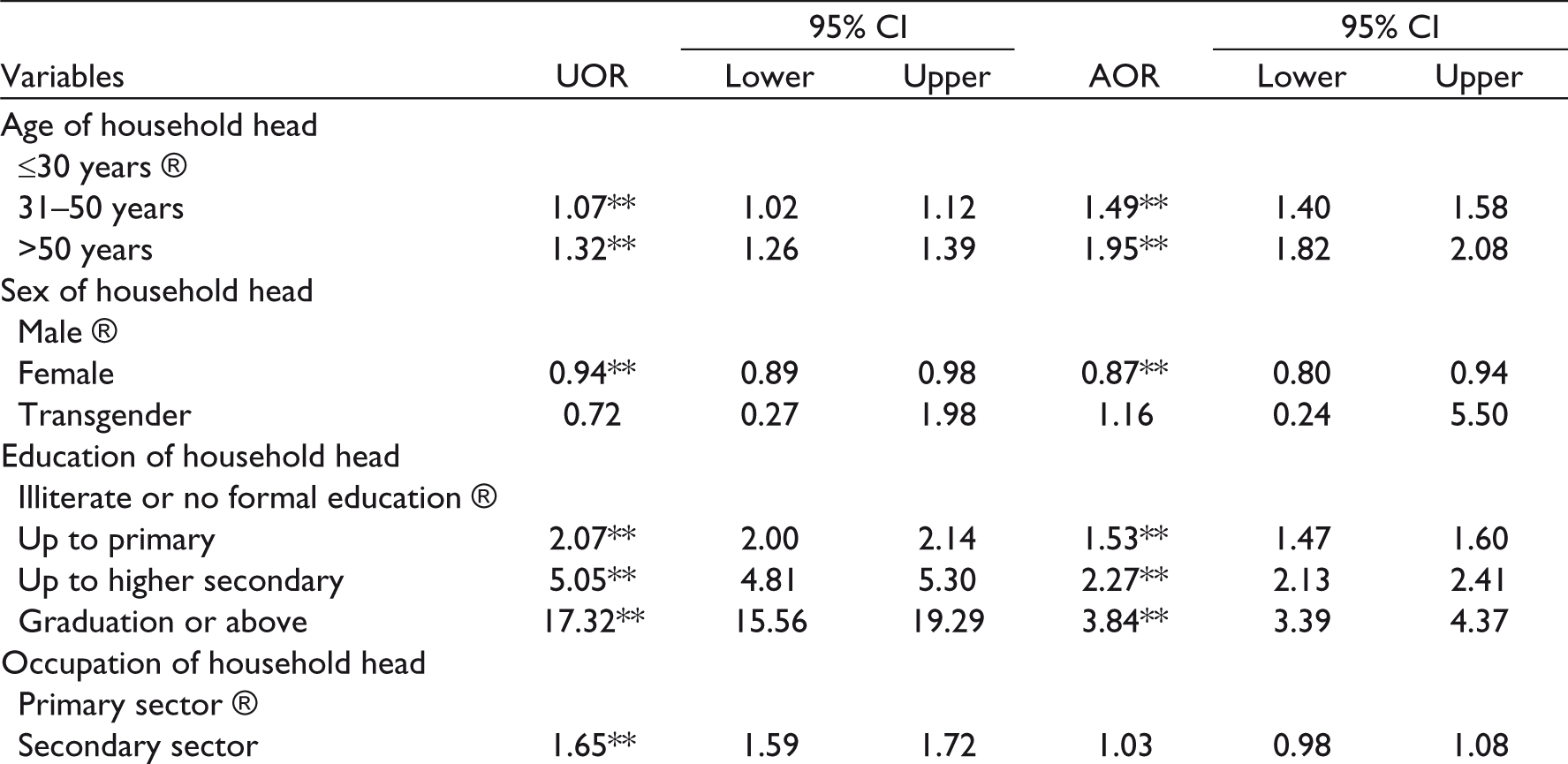

** p < 0.01, * p < 0.05.
Socio-religious affiliation appeared to be a significant factor in determining accessibility. Compared to the ST communities, the households that belonged to General categories were associated with 73% greater likelihood (AOR: 1.73, 95% CI 1.61–1.87) and SCs with 15% lower likelihood (AOR: 0.85, 95% CI 0.80–0.91) in having sanitation facility. Similarly, Muslims and other religious groups had higher odds of using latrine facilities than those who believe in Hinduism. Place of residence was significantly correlated with sanitation use. The households living in urban areas (AOR: 2.37, 95% CI 2.23–2.52) had more than twofold greater likelihood of accessing better sanitation facilities than those in rural areas. Economic status of the household is one of the most dominant factors in determining the utilization of sanitation. The accessibility to sanitation significantly increased from the poorest to the richest MPCE group of households. Compared to the households that belonged to the poorest quintile group, the households in richer (AOR: 2.97, 95% CI 2.76–3.19) and richest quintile (AOR: 5.51, 95% CI 4.87–6.22) were more than three and five times as likely to use improved latrine facilities. Housing condition was found to be positively associated with the use of sanitation. The coverage of sanitation was significantly higher in semi-pucca and pucca households as compared to households living in katcha houses. Similarly, water availability plays a vital role in determining latrine use. In comparison with households having water supply within dwelling unit, those who had water availability within premises (AOR: 0.74, 95% CI 0.70–0.78) and outside premises (AOR: 0.48, 95% CI 0.45–0.50) had 26% and 52% less livelihood of using latrine at home. The results suggest that there is a significant regional variation in overall sanitation performance. Compared to the northern region, the households in north-east (AOR: 4.21, 95% CI 3.79–4.69) and west (AOR: 1.11, 95% CI 1.02–1.20) regions were more likely, and the households in central (AOR: 0.93, 95% CI 0.86–1.00) regions were less likely to have sanitation use.
Discussion
Access to basic sanitation facilities is crucial for decent and healthy living. Although India has witnessed a substantial improvement in access to basic sanitation facilities over the past decades, the present condition of sanitation is still unsatisfactory, especially in rural areas. As per the 2011 Census of India, around 49.8% of all households in this country did not have access to toilet facilities and practiced open defecation. Moreover, this proportion is as high as 67.3% of households in rural India (Government of India 2012). This study has investigated the levels and trends in access to latrine facilities, geographical variations and the associated socio-economic factors using the recent large-scale data from the National Sample Survey Organization.
After a detailed analysis of levels and trends in latrine use, this study found that the coverage of sanitation facilities improved significantly in India between 2012 and 2018. The prevalence of open defecation went down to 20.2% in 2018, while access to improved latrines increased to 78.3%. Similarly, the study observed a declining trend of shared latrines, reflecting people’s willingness to use individual household latrines. The possible reason stems from the concerns of cleanliness and accessibility. The shared latrines are not as hygienic as individual household facilities and may not be easily accessible at night, particularly for women and children (Heijnen et al., 2014; WHO & UNICEF, 2017). Moreover, the health concerns of using shared facilities are also disturbing; it is evident that shared latrines may be a risk factor for diarrhoea among children (Fuller et al., 2014).
There are wide disparities between urban and rural households in access to latrine facilities. It is observed that one in every three households in rural India defecates in open spaces. These results are in agreement with several studies conducted earlier (O’Reilly et al., 2017; Shukla, 2018). Defecation practices depend on people’s habits, cultural practices, sanitary preferences and availability of resources (Coffey et al., 2014; Routray et al., 2015). The higher prevalence of open defecation in rural India is attributed to the traditional behaviour and lack of awareness among rural people (Ghosh & Cairncross, 2014; Yogananth & Bhatnagar, 2018). A study by Routray et al. (2015), using exploratory qualitative field methods, observed that ‘even where people had an option to use a household latrine, many were reluctant to adopt latrine use habits and instead chose to continue their traditional behaviours to defecate under the open sky’. In the same line, the preference for open defecation among rural households has also been documented in five north Indian states (Coffey et al., 2014). Similarly, Ngwu (2017), in a study of Nigeria, found that the practice of open defecation is deeply tied to culture and tradition. Because of behavioural preference, most of the rural dwellers in this country defecate openly in bushes, rivers and open spaces outside the designated toilets.
The results of this study show huge geographical variations in access to latrine facilities in India. The access to latrine facilities is higher in north-eastern and northern parts of the country, while the central and eastern regions have very low coverage. The spatial analysis (LISA) reveals that the clusters with high prevalence of open defecation are mostly located in eastern and central regions of the country, while the north and north-eastern regions have clusters with low prevalence of open defecation. Some north-eastern states, such as Nagaland, Sikkim, Mizoram and Manipur, have achieved 100% coverage of latrine use within household premises and become open defecation free. In contrast, the practice of open defecation is highly rampant in central and eastern states of Uttar Pradesh, Odisha, Bihar, Jharkhand, Madhya Pradesh and Rajasthan. Such regional pattern has also been documented in previous studies (Banerjee et al., 2017; Coffey et al., 2014). These states come from the group of BIMARU 1 states as coined by Ashish Bose in the early 1980s. Historically, the BIMARU states are the backward states in India with regards to demographic, social and economic indicators (Bose, 1988, 1996). Sharma (2015) pointed out that although these states have made some individual progress over the years, as a group, BIMARU states have not converged with the national average, and none of the states have been able to depart from the grouping; however, the states of Rajasthan, Uttar Pradesh and Madhya Pradesh have achieved a greater degree of improvement than Bihar. Few studies revealed that all the BIMARU states also perform very poorly in basic human needs, such as latrine facilities, safe drinking water and electricity (Shukla, 2018). In a recent study, Vani and Madheswaran (2018) observed that most BIMARU states have low access to basic services, including sanitation facilities, while the states of Punjab, Kerala and Uttarakhand have relatively higher accessibility. These findings are consistent with the results of this present study.
The multivariate analysis of this study found that various socio-economic, demographic and geographic factors are significantly associated with access to latrine facilities. In line with other studies (Abubakar, 2018; Kuberan et al., 2015; Vani & Madheswaran, 2018), the results show that the level of education of the household head is associated with better accessibility to sanitation facilities. Education makes people aware of the importance of hygiene and sanitation and their implications on health. There is also a link between occupational status and latrine use, as those households engaged in high-paid tertiary jobs are more likely to have better access to sanitation facilities. It might be because occupation status is often correlated with high educational and economic status.
Socio-religious affiliation of a household also affects the access to sanitation facilities considerably. It is observed that the probability of using latrines was greater among the households of General categories than that of socially disadvantaged SC and ST categories. In consistent with the previous studies (Banerjee et al., 2017; Bonu & Kim, 2009; Vyas & Spears 2018), the results of the present study found that Muslims have 34% greater likelihood of access to latrine facilities than Hindus. Coffey et al. (2017) observed that certain societal norms about purity and pollution in Hinduism intersect with deep-rooted caste dynamics to influence everyday sanitation practices. It is argued that the historical associations between low-caste groups and latrine pit emptying work, which continues to annoy certain caste communities even today, make the simple pit latrines that require frequent emptying unattractive to rural Indians (Dyalchand et al., 2011). The stigma and discrimination associated with handling faeces largely contribute to a collective norm that latrines should have large, expensive septic tanks (Gatade, 2015). The poor families who cannot afford expensive latrines simply go for open defecation but do not use inexpensive pit latrines in rural India. The practices of purity and pollution in Hinduism strictly discourage having latrines in close proximity to their homes (Coffey et al., 2017). In India, Spears and Thorat (2015) found that households are more likely to defecate in open spaces where a greater fraction of their neighbours practice untouchability, meaning where norms of purity and pollution are more enforced. Similarly, Hathi et al. (2016) explored that open defecation is more prevalent in rural areas of this country, where caste-based social conflicts are frequent.
Economic condition has always been an important factor for sanitation facilities. In agreement with other studies (De, 2018; Dickinson & Pattanayak, 2009; Halder & Kabir, 2008), the findings of this present study showed that the households with higher economic status and good housing condition have better access to latrine use. Banerjee et al. (2017) reported that affluent households with a pucca house are more likely to have toilets within dwelling units. Dickinson and Pattanayak (2009) also observed a similar positive association between housing characteristics, such as type of walls and ownership of toilets. Affordability always plays a major role in determining the accessibility to hygienic sanitation facilities (Giné-Garriga et al., 2017; Novotný et al., 2018; Wasonga & Bukania, 2015). One of the major reasons for higher prevalence of open defecation in this country is the huge initial investment required for the construction of toilets that poor households cannot afford. The present study observed that a significant proportion of poor households use shared or public toilets constructed for common use. In the same line, few previous studies also found that the users of shared sanitation are poorer and less educated than those using individual household latrines (Heijnen et al., 2014, 2015). Water unavailability is a generally significant barrier to toilet adoption in India. Consistent with previous studies (Exum et al., 2020; Gilman et al., 1993), the present study found that the households having water availability within dwelling units are more likely to use latrine facilities than those households that have to collect water from outside premises. Gilman et al. (1993) argued that water shortage plays a crucial role in reducing accessibility to sanitation and hygienic practices. Without adequate in-house water supply, providing increased hygiene information will probably not result in better sanitation practices.
Adequate and hygienic sanitation facilities and safe water supply are fundamental to good health and social and economic development. Unhygienic sanitation practice is the leading cause of infectious excreta-related diseases, such as diarrhoea, hepatitis and typhoid fever and soil transmitted diseases, like ascariasis and hookworm, thereby creating huge health burden including anaemia, stunting growth and premature death especially among children (Gertler et al., 2015; Mara, 2017). The practice of open defecation also contaminates local environment with human faeces and pollutes the air with foul odour (Abubakar, 2018). Sustainable Development Goal 6 focuses on ensuring availability and sustainable management of water and sanitation for all. To achieve the target of accessibility to adequate and equitable sanitation and hygiene for all and end open defecation by 2030, India needs to focus more on the hot spot clusters and rural areas that are far behind the anticipated targets.
Recently launched Swachh Bharat Mission to achieve universal sanitation coverage and ‘open-defecation free’ India has great potential to improve sanitation services in this country. Under this scheme, many household toilets have been constructed since its start in 2014. However, it has some hindrances in its structure. The reimbursement model of this scheme, where the households are expected to build the toilets from their own funds and then apply for the subsidy, fails to cover the poor households as they lack the initial fund for the construction (Kumar, 2019). There are also reports of defunct and unusable toilets due to poorly built and lack of water (Chauhan, 2017; Dutta, 2017). It is worth noting that the issue of open defecation in India is very complex; building toilets alone cannot resolve this, it also requires a change in people’s attitude at the individual and contextual level. Coffey et al. (2014) explored that over 40% of households with a working latrine have at least one member who defecates in the open. In cases where government toilets are constructed, most people yet prefer open defecation. There are misperceptions that open defecation is healthier than using a latrine. Increasing accessibility alone cannot be the main solution. Therefore, what needs to be changed is the behaviour towards latrine use.
Strengths and Limitations
The main strength of this study is that it utilised large-scale nationally representative sample survey data. It provides the most recent evidence for understanding the access to sanitation facilities in India. In addition, this study examined spatial variations in latrine use which would help the stakeholders to understand the problem of sanitation coverage at a spatial scale. However, the study has a few limitations. The spatial analysis (LISA) has been done using data from NSSO 76th round; therefore, sample bias might have been introduced due to low sample size in some districts. It should be noted that the spatial analysis was applied in the districts with a sample size of at least 30. Another limitation of this study is the cross-sectional research design, thus cause–effect relationship between latrine uses and its predictor variables cannot be assumed from this study.
Conclusion
The study has highlighted the progress, geographical variations and associated socio-economic factors in access to latrine facilities in India. Access to sanitation facilities is still unsatisfactory, and a huge rural–urban gap exists in latrine use. Open defecation is still prevalent in this country, especially in rural areas. Unequal access among socio-economic groups is also very prominent. The findings of this study reveal that there are apparent geographical variations in access to latrine facilities across the country; the clusters with high prevalence of open defecation are mostly located in eastern and central regions of the country, while the north and north-eastern regions have better access to basic sanitation facilities. Factors like education, occupation, socio-religious affiliation, water availability and economic status are significant determinants of accessibility to latrine facilities. It is recommended that targeted interventions for the socio-economically disadvantaged groups, spreading awareness about the importance of latrine use and hygienic practices, and proper assistance for construction and maintenance of toilets could be helpful to combat the harmful practice of open defecation and ensure adequate and equitable sanitation for all.
Footnotes
Note
Declaration of Conflict of Interest
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.