
Abstract
Background
Simulation-based education (SBE) has become an emerging teaching strategy in which faculty play a central role in implementing SBE within nursing curricula; hence, to understand how simulation is integrated into teaching practices, this study aimed to explore nursing faculty perspectives and implementation experiences of SBE in nursing institutes across Northern India.
Methods
A qualitative phenomenological design was adopted to collect data through in-depth interviews with 19 nursing faculty members, purposively sampled from selected institutes in Northern India, who had completed training in SBE at least 6 months prior. Audio-recorded interviews were transcribed and analyzed thematically until data saturation.
Results
Four themes reflected faculty perspectives: perceived educational value of SBE, safe and supportive learning environment, enhancing competence and patient safety, and accessibility and adaptability of SBE. Three themes captured their implementation experiences: comfort and confidence in using SBE, scope and barriers to simulation usage, and enabling factors influencing implementation. Faculty perceived SBE as a realistic and interactive pedagogy that enhances competence and patient safety. Implementation experiences were influenced by prior training, infrastructure, and administrative support.
Conclusion
Nursing faculty in Northern India expressed positive perspectives and meaningful engagement with SBE. Faculty training, resource optimization, and institutional support are vital for strengthening simulation-based nursing education.
Introduction
Simulation-based education (SBE) is an emerging and innovative educational methodology that bridges the gap between theory and practice. It engages learners in realistic scenarios, enabling them to reflect on their actions and develop essential technical and nontechnical skills before entering actual clinical environments.¹ A landmark National Simulation Study conducted by the National Council of State Boards of Nursing (NCSBN) revealed that high-quality simulation can substitute up to 50% of traditional clinical hours across the nursing curriculum.²
In India, the recent shift toward competency-based curriculum reform has further emphasized the integration of simulation into nursing education. In alignment with this shift, the Indian Nursing Council incorporated SBE into the revised BSc Nursing curriculum (2021). Additionally, the establishment of a state-of-the-art national simulation facility in 2018 aimed to strengthen faculty competencies and promote the wider adoption of SBE across the country.
Simulation sessions typically occur in well-equipped laboratories where students participate in structured activities designed to meet specific learning objectives. The success of such experiences depends on meticulous planning, the faculty’s understanding of simulation principles, and adequate preparation of learners in cognitive, psychomotor, and decision-making domains. 1
Faculty play a pivotal role in the effective implementation of simulation pedagogy, and their attitudes and readiness significantly influence its adoption and integration within curricula. Several international studies have reported generally positive faculty perceptions toward SBE, recognizing its effectiveness in enhancing student engagement, realism, and clinical preparedness. Educators often acknowledge simulation as a valuable alternative to traditional clinical exposure, especially in contexts with limited patient availability or safety concerns.3–5
In the Indian context, simulation remains an evolving concept. Previous studies highlight that while nursing faculty generally hold positive perceptions and favorable attitudes toward SBE, its actual implementation within curricula is influenced by multiple interrelated factors.6, 7 Multiple international studies have revealed that successful and sustained use of simulation depends on institutional support, workload management, scheduling, resource availability, infrastructure readiness, continued faculty development, and student-related and operational factors. A lack or inadequacy of these factors can lead to insufficient curricular integration.8–14
Despite the growing global evidence on faculty perceptions and implementation of SBE, limited qualitative research has been undertaken in the Indian context to explore faculty experiences in depth. Existing studies primarily focus on student learning outcomes or quantitative evaluations of perception and attitude.6, 7 Very few have examined how nursing faculty, after receiving formal training in SBE, actually perceive and use simulation in their teaching–learning practices.
Northern India represents a diverse educational landscape, with institutions differing markedly in infrastructure, faculty preparedness, and curricular integration. This variation underscores the need for region-specific qualitative evidence to understand how trained faculty perceive, utilize, and experience the implementation of SBE within their institutional settings. Such insights can provide valuable evidence to guide future faculty development programs (FDPs), strengthen simulation infrastructure, and promote sustainable integration of SBE into nursing curricula.
This study forms part of a broader doctoral research project on the implementation of SBE across India. The present article specifically focuses on qualitative findings from nursing faculty based in Northern India, exploring their perspectives and implementation experiences of SBE in their respective institutions.
Objectives
To explore nursing faculty perspectives about SBE in nursing education.
To describe faculty experiences in implementing SBE within their teaching–learning practices.
To identify the perceived enabling factors and barriers encountered by nursing faculty during the implementation of SBE.
Materials and Methods
A qualitative approach with a descriptive phenomenological design was used. The study was conducted across selected nursing institutions in Northern India. Participants included nursing faculty who had completed a six-day Training of Trainers (ToTs) program in SBE at a national simulation center at least 6 months before data collection. This criterion ensured that participants had sufficient time to apply SBE in their teaching–learning practices, enabling richer experiential reflection. A total of 19 nursing faculty were enrolled in this study using purposive sampling from September 2024 to March 2025, and the sample size was determined by data saturation. Data saturation was achieved when no new information or insights emerged across successive interviews. Maximum variation (in terms of designation, teaching experience, and institutional type) was attempted to capture diverse perspectives.
A semi-structured interview guide was developed based on the literature and inputs from nine experts in the field of nursing and simulation. It contained four main questions and seven probing questions related to participants’ background, opinions regarding simulation, whether and how they were using simulation, its feasibility, their comfort level in utilizing SBE, associated enabling factors, and perceived barriers in the implementation of SBE. Two pilot interviews were conducted to refine the guide. Data were collected using the interview guide through in-depth face-to-face interviews. Interviews lasted 20–25 min, were audio-recorded with consent, and were conducted by the principal investigator, who was a PhD scholar and had prior training and experience in qualitative interviewing. Reflexivity was maintained throughout the research process through journaling. Confidentiality, anonymity, and voluntary participation were ensured. Ethical approval was obtained from the Institutional Ethics Committee of the university. The rigor of the study was maintained as follows:
Strategies Adopted to Ensure Rigor and Trustworthiness of the Present Study.

Data analysis was done using Colaizzi’s seven-step model of phenomenological analysis. Each transcript was read and reread to obtain a general impression of the whole content. Significant statements were identified, and formulated meanings were developed. All coding was done manually using structured note-taking, annotation, and iterative categorization. Codes were grouped into subthemes and themes through constant comparison. A total of 104 codes, 19 subthemes, and 7 themes emerged. Intercoder agreement was established through peer review of selected transcripts to enhance dependability. Rigor was ensured following Lincoln and Guba’s criteria, represented in Figure 1.
Credibility: Pilot testing of interviews, audio recordings, and member checking. Dependability: Intercoder agreement and data collected until data saturation. Transferability: Purposive sampling and thick description of data. Confirmability: Reflexive journaling and data triangulation.
Results
A total of 19 nursing faculty members were interviewed, comprising 16 females (84.2%) and 3 males (15.8%). In terms of educational qualifications, 5 participants (26.3%) were Doctors of Philosophy (PhD), while the remaining 14 (73.7%) held a Master of Science in Nursing (MSc) as their highest qualification. With regard to professional experience, the majority of participants, 9 (47.4%), had 10–15 years of experience, followed by 5 (26.3%) who had 15–20 years of teaching experience. In relation to designation, 5 participants (26.3%) were principals or vice principals, 5 (26.3%) were tutors, and 9 (47.4%) were working as associate professors, assistant professors, or lecturers. Institutional affiliation was almost evenly distributed, with 9 (47.4%) participants representing government institutions and 10 (52.6%) from private institutions.
Geographically, the participants were taken from Delhi (8; 42.1%), Haryana (3; 15.8%), Uttar Pradesh (2; 10.5%), Punjab (1; 5.3%), Gujarat (3; 15.8%), and Rajasthan (2; 10.5%). Regarding simulation infrastructure, one participant (5.3%) reported having access to a fully functional simulation center dedicated to nursing education, three participants (15.8%) had an institutional simulation lab that was used by students of other departments, apart from nursing, while the remaining 15 participants (78.9%) reported having only traditional skill laboratories in their institutions as per Indian Nursing Council (INC) norms.
Section 1: Thematic analysis describing the major themes and subthemes identified regarding nursing faculty perspectives for SBE
Major Themes and Subthemes Regarding Nursing Faculty Perspectives for Simulation-based Education (SBE).
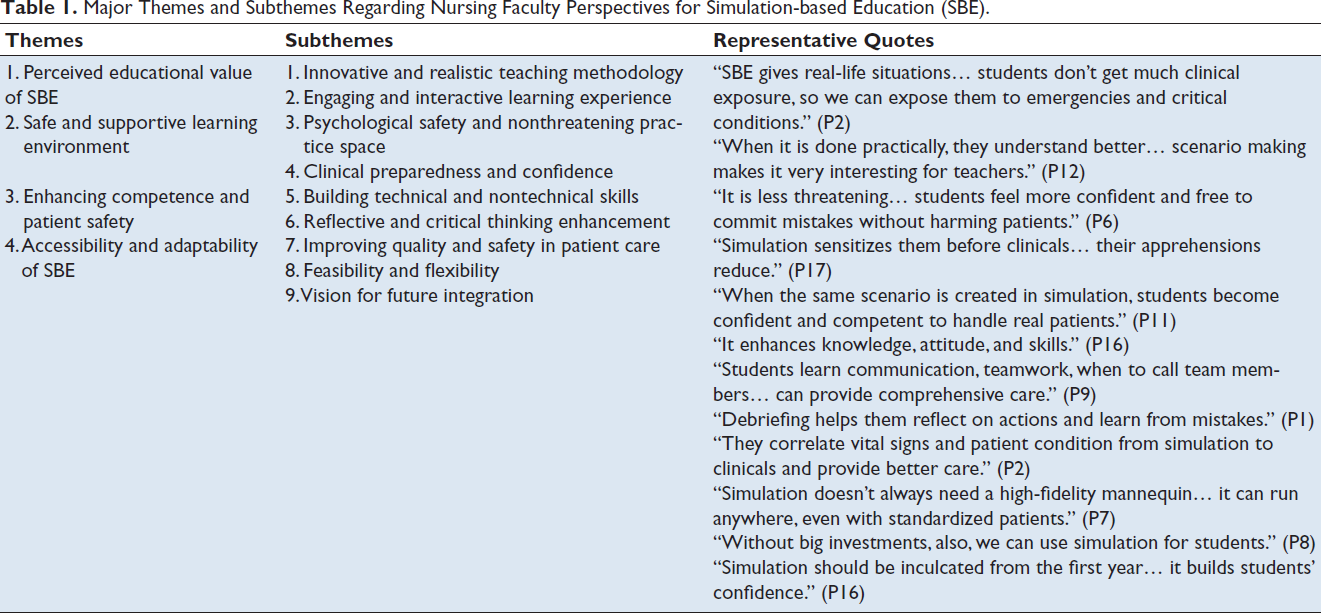
Major themes and subthemes regarding nursing faculty perspectives for simulation-based education (SBE) illustrated in Table 1 are described as follows:
Theme 1: Perceived Educational Value of Simulation-based Education
Subtheme 1.1: Innovative and Realistic Teaching Methodology
Faculty members consistently described SBE as a modern, effective, realistic, and innovative teaching approach. Many considered it a “good concept” and “the best method for teaching students,” highlighting its realism and ability to replicate clinical conditions. Faculty emphasized that SBE provides a more authentic and engaging learning experience compared to traditional demonstrations, and can even substitute certain clinical experiences when real exposure is limited.
It is a good methodology that can be used with students to give real life situation as we know that students don’t get that much clinical exposure and they won’t be able to see that much of critical cases in the clinical area as well, so by this SBE we can actually try to expose them to emergency and various critical condition that they are not able to encounter in their clinical but they may encounter when they will be actually working in clinicals, so it is a good substitution for that. (P2)
Subtheme 1.2: Engaging and Interactive Learning Experience
Participants viewed SBE as an interactive and stimulating learning process that keeps both students and teachers actively engaged. They noted that simulations make learning “interesting,” “easy,” and “immersive,” leading to deeper learning and better knowledge retention. Faculty shared that designing scenarios and facilitating sessions stimulated creativity, making the teaching–learning process more enjoyable and impactful for both educators and learners.
Every time we take a traditional way of teaching, it becomes a lot boring at times, and it becomes difficult for them (students) to understand. But when it is being done practically, they understand even more better. And for teachers, also, it is a break from the traditional classroom teaching, and they also inculcate new ideas. The scenario making also requires a lot of ideas, and then we also do a lot of work in this. So, it makes it very interesting. It is a form of interesting form of teaching. (P12)
Theme 2: Safe and Supportive Learning Environment
Subtheme 2.1: Psychological Safety and Nonthreatening Practice Space
Faculty emphasized that simulation offers a safe and nonthreatening learning environment where students can practice skills without fear of harming real patients. It allows students to make and correct mistakes freely.
I find it (simulation) is less threatening. It is not associated to the harmful outcome of the patients, that’s why those students feel more confident in performing, they are free to commit mistakes. (P6)
Some contrasted this with their own training, recalling the “inhuman” practice of performing procedures on peers.
Students can have practice on the manikins and on the simulators. And it is safe…I remember, when we were giving injections, we were giving on one another, we were giving IM injections, Intradermal injection, everything we were doing on our classmates, that was very painful…something inhuman. So, now, it is very good that we can teach the students and they can practice in a safe environment. (P2)
This psychological safety promotes confidence and encourages risk-taking necessary for learning clinical skills effectively.
Subtheme 2.2: Clinical Preparedness and Confidence
SBE was viewed as a valuable preclinical readiness tool, helping students overcome anxiety before entering clinical placements. Faculty shared that simulation “sensitizes students,” reduces hesitation, and helps them rehearse clinical judgment before managing real patients.
Simulation-based education is good because it is just sensitizing them. So, before putting them or exposing them into the clinical, so they are be ready with that things and whatever apprehensions are there, those have been sorted out. (P17)
It acts as a bridge between theory and clinical practice, improving student confidence and preparedness. Exposure to realistic scenarios helps them become capable of adapting to various clinical environments.
When in the simulation lab, the same kind of scenario is created, which the student will face in the clinical…So the student is already exposed to that…kind of situation…So the student will be competent and confident enough in handling…the real patient in the clinicals. (P11)
Major themes and subthemes regarding implementation experiences of nursing faculty for simulation-based education (SBE) illustrated in Table 2 are described as follows:
Theme 3: Enhancing Competence and Patient Safety
Subtheme 3.1: Building Technical and Nontechnical Skills
A strong consensus emerged that SBE builds knowledge, psychomotor skills, and attitudes of students, leading to overall improvement in their competence, due to which they can manage complex situations effectively.
It enhances the knowledge and attitude. And it enhances the skills also. (P16)
Not only does it build technical skills like assessment and performing procedures to manage the patient, but it also builds nontechnical skills such as communication, leadership, and team dynamics.
We can give the students the actual experience, which all hurdles they will go through while performing the particular skills, the communication skills needed in there…so we can provide comprehensive care also the teamwork in the scenario. Like, when to call the other team members…. (P9)
Subtheme 3.2: Reflective and Critical Thinking Enhancement
Faculty acknowledged simulation as a powerful medium for reflective learning. Through structured debriefing, students are able to analyze their actions, identify mistakes, and learn corrective strategies in a safe environment.
Debriefing helps them to reflect on their actions, and they learn from their actions. (P1)
This process fosters accountability, prevents repetition of errors in real clinical settings, and supports a deeper understanding of patient care.
Definitely it (errors) will be there doing in a simulated case, the chances of error when they go to the real this thing (clinicals)… that time, the error will also be less in comparison with the directly putting them into the clinical. (P15)
Simulation was recognized for enhancing analytical thinking and clinical reasoning. Faculty observed improved student ability to assess situations, prioritize interventions, and make sound decisions under pressure. The process cultivates critical thinking—a core attribute for competent and independent nursing practice.
It’s a good method to develop their competencies and critical thinking and improve quality of nursing care. (P1)
Subtheme 3.3: Improving Quality and Safety in Patient Care
Participants agreed that simulation contributes to better-quality nursing care and safer clinical outcomes. It allows students to rehearse high-risk procedures and make decisions in controlled settings, thereby minimizing potential harm to patients and strengthening safety culture within nursing education.
First they will see the demonstration, then they will do the re-demonstration…then after the particular simulation scenario…they have the skill of assessment and decision making, apart from performing skills (interventions). (P9) In simulation, the whole scenario is there in front of them, regarding the vital signs of the patients, the conscious level of the patient…all these aspects, they can correlate this thing (learnings from simulation) in the clinicals as well, and they can do better for the patient. (P2)
Theme 4: Accessibility and Adaptability of Simulation-based Education
Subtheme 4.1: Feasibility and Flexibility
While some initially expressed skepticism about simulation’s practicality, most reported a shift in perspective after witnessing its effectiveness. Several faculties appreciated the flexibility of simulation methods, noting that effective learning can occur even without high-fidelity manikins or elaborate setups. Many realized that simulation “doesn’t always need a mannequin” and can be implemented in low-resource settings using creative approaches.
Initially, I was skeptical about it (Simulation) as will it work or not? There were few things which I got to learn that simulation doesn’t always need a mannequin or a high-fidelity manikin but you can have simulation run anywhere, in-situ or on standardized patient. So, coming to know about those things, definitely made me believe that simulation definitely will help in teaching students. (P7)
This adaptability increases the feasibility of SBE across diverse institutional contexts. Faculty realized that proper training enables meaningful learning experiences without dependence on high-end equipment.
When I started that simulation programme (TOT on SBE), so my query was that if I don’t have this kind of big setup, I cannot teach my students like that. But after third or fourth day, I came to know that without any setup or big investment also, we can use this to our students. (P8)
This transformation underscored the importance of continuous refresher training for sustainability.
Only the important thing is that facilitator should understand their role properly…People who are actually going to execute this thing (simulation) should be well trained. (P7)
Subtheme 4.2: Vision for Future Integration
Participants described SBE as the “need of the hour” in modern nursing education. They emphasized its relevance in the changing academic structure, such as the semester system, and advocated for making simulation-based teaching mandatory from the first year onward.
I think that this should be inculcated right from the BSc first year, because it gives the confidence also, to the person who is doing the simulation and to students, as well. (P16)
Faculty viewed SBE as essential for bridging the gap between classroom theory and real-world nursing practice.
So, simulation-based teaching is a bridge, that will connect and ease the pass towards the clinical experience. (P15)
Section 2: Thematic analysis describing major themes and subthemes identified regarding implementation experiences of nursing faculty for SBE.
Major Themes and Subthemes Regarding Implementation Experiences of Nursing Faculty Perspectives for Simulation-based education (SBE).
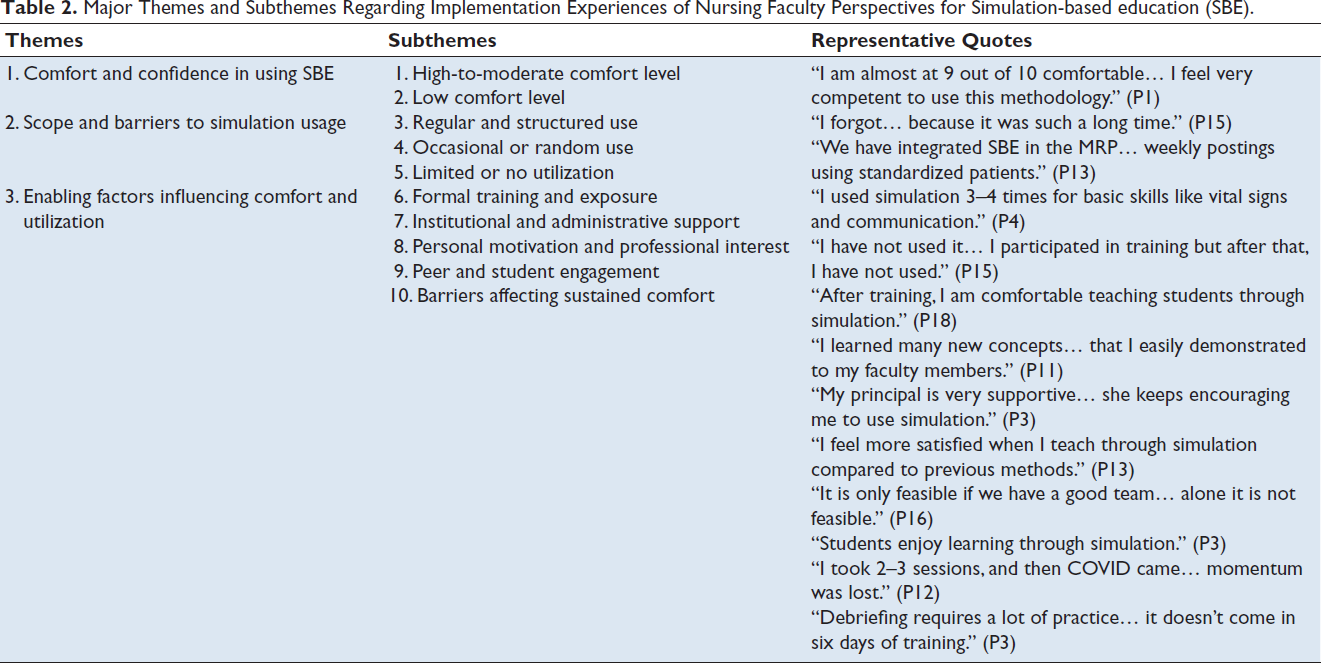
Theme 1: Comfort and Confidence in Using Simulation-based Education
Subtheme 1.1: High-to-moderate Comfort Level
Faculty who had undergone the ToTs program at the simulation center and had regular exposure to simulation reported higher confidence levels (8–9 out of 10). These participants described themselves as “competent,” “confident,” and “comfortable” in using simulation methods, often integrating them into their teaching plans. Continuous engagement, supportive management, and prior training were key contributors to their comfort.
I am almost at 9 out of 10 comfortable. Because I have been trained in simulation and I am involved in simulation since 2019, so, I feel very competent to use this methodology. (P1) I have done this simulation training and AHA training also. So, I can say that I was bit more confident; 8 or 8+ confident in performing simulation. (P6)
Many faculty members expressed a moderate level of comfort with SBE, typically rating themselves between 6 and 7 out of 10. This group included faculty who had limited exposure or used simulation sporadically for specific topics such as basic life support (BLS), injection techniques, or vital signs. While they understood the concept and valued its usefulness, their confidence was limited by irregular practice, lack of structured integration, or time constraints.
7 out of 10 comfortable because I enjoy and we can improve ourself as well as the students. (P3)
Subtheme 1.2: Low Comfort Level
Only one faculty member admitted to low confidence in using SBE. This was attributed to a long gap since training, lack of practice, or insufficient clinical exposure through their affiliated hospitals. Some had forgotten the methodology or felt simulation was not yet essential in their context.
I forgot…because it was such a long time. (P15)
Theme 2: Scope and Barriers to Simulation Usage
Subtheme 2.1: Regular and Structured Use
Faculty reporting consistent simulation usage described well-planned, structured implementation—including weekly postings, integration into the master rotation plan (MRP), and subject-specific scenarios. They utilized standardized patients, manikins, and low-fidelity setups for teaching critical procedures like code blue and code pink, PPH, APH, newborn resuscitation, and communication skills.
We are using simulation, like in the different subject like paediatric, mental health nursing, medical- surgical and fundamentals (of nursing). So, from the basic with the first semester students, we start working on that. We have integrated in MRP from last year, weekly posting, using standardized patients. (P13)
One participant who had a state-of-the-art simulation center dedicated to the nursing department reported 20%–25% replacement of clinical hours with simulation and students posted routinely in the lab.
We have a simulation lab in our institute and it is a well-equipped lab, so we used to post our students every year…like based on 20-25% of their clinical postings is being replicated by simulation and they are posted in simulation by rotation basis. (P1)
Subtheme 2.2: Occasional or Random Use
Several faculty members indicated sporadic or unstructured usage of simulation, conducted “randomly” during skill lab hours. These sessions were often used for specific topics such as BLS, injections, or basic communication, but were not formally documented in academic schedules or integrated into their master rotation plans.
Last semester, I have used with B.Sc. 1st sem for 3–4 times for basic skills like vital signs and communication. They wanted it to be more but because of their semester system, it was not possible that more than three times. (P4) I am using simulation for teaching but it is not integrated in master rotation plan… We have advanced skill hours. In my hours, I am using this method. (P9) Randomly we have done with skill lab hours. 40 hours were there, so we have managed 4-6 hours only for simulation. (P18)
Participants who were from mental health or community health nursing reported the use of standardized patients and replacing some of the clinical hours randomly with simulation hours.
We have practical hours, like two hours or three hours (for simulation) in community, which was already mentioned in the timetable. So, during those hours only, we plan simulations. (P10)
Subtheme 2.3: Limited or No Utilization
Some participants reported doing only one to two simulations for training their co-faculty but then could not implement them with students due to various barriers, such as time constraint, bigger batch size, and difficulty in scenario designing or debriefing.
It’s difficult to arrange all the articles and then to write the script…because if you are doing the skill, procedure already written in the book, but simulation script is not written in the book…Moreover shortage of time, faculty and manikins is a major problem. (P14)
Some participants had not yet integrated simulation into their teaching.
I have not used and not using also. I just participated in that training program and after that, I have not used. (P15)
Reasons included availability of parent hospital, faculty attitude and interest, lack of institutional resources, absence of formal planning, or faculty workload. However, many expressed interest in implementing SBE in future batches.
We are not using but we have already planned…in future we will definitely teach them through the simulation. (P5) We have got skill lab- 200 hours only. We have planned it, exclusively some hours for the simulations. So, we will schedule this time (next academic year). (P19)
Theme 3: Enabling Factors Influencing Comfort and Utilization
Subtheme 3.1: Formal Training and Exposure
Almost all participants identified the ToTs program at the simulation center as a major enabler of confidence and usage. Faculty emphasized that exposure during training enhanced their conceptual understanding, technical skills, and motivation to use SBE.
I was confident enough because I got training, exclusive training. And the thing was that I learned many new concepts in deeply which I was easily able to demonstrate to all of my faculty members. (P11)
Many credited training for transforming their teaching approach and reducing apprehension about simulation.
Firstly, we are thinking this for simulation, we need only the equipped lab, but after taking the training, I am comfortable to teach students through simulation. (P18)
Subtheme 3.2: Institutional and Administrative Support
Comfort and frequency of use were significantly influenced by support from institutional leadership, including access to manikins, simulation rooms, and management encouragement. Faculty who worked in supportive environments or had simulation infrastructure reported greater motivation and smoother integration of SBE in teaching.
My management, my principal is very supportive. She keeps on saying, do this, do this. (P3) It is much feasible for us because we have facilities…And there’s the central simulation lab is also there…support from the institute also…If you think, like tomorrow, I have to run this kind of simulation scenario, so, there are the facilities and resources are also there. (P17)
Subtheme 3.3: Personal Motivation and Professional Interest
Self-motivation, curiosity, and enthusiasm also played a key role in adoption. Faculty who viewed simulation as a professional development opportunity or a means to improve student outcomes were more proactive in utilizing it, even when institutional setups were limited.
One thing, I want my students to learn more. Second, psychiatry, they have only 1 month posting, they are going to psychiatric clinical area which is not having that acute patients…and if there are acute patients, my students are not allowed to go to them. So, to make them learn acute disorders, I feel it is my responsibility to teach them. So, that’s why I use simulation there. (P3) I feel more satisfied when I teach my student with the simulation method as compared to the previous method, which I have done in my learning. (P13)
Subtheme 3.4: Peer and Student Engagement
The enthusiasm of students and cooperation from co-faculty also acted as enabling factors.
It is only feasible if we have a good team. Alone, it is not feasible. (P16) I had to train my colleagues for that and then we, as a team we conduct simulation scenario. (P9)
Faculty noted that student engagement during simulations enhanced their own comfort and confidence to use SBE regularly.
Students are comfortable with me; they enjoy learning through simulation. (P3)
Subtheme 3.5: Barriers Affecting Sustained Comfort
Despite initial enthusiasm, some faculty mentioned loss of momentum post-training due to lack of continuity, especially during COVID-19 disruptions.
In the beginning I was very enthusiastic…When I came back, I have trained all my teachers…So, I took 2-3 sessions for simulation and then COVID came…Others faced challenges due to insufficient practice opportunities or lack of refresher training. (P3)
P12 expressed:
I feel that debriefing requires a lot of practice. Yeah, it doesn’t come in six days training. It was a learning experience for me. It’s about the entire process of simulation, starting from everything, how to set up and then how to conduct and debrief, and all those things…I forgot because such a long time ago… (P15)
Discussion
The present study revealed that nursing faculty in Northern India perceive SBE as an innovative, realistic, and transformative andragogical approach that enhances learner engagement, critical thinking, and confidence. These findings are consistent with global evidence recognizing simulation as a key strategy for integrating theoretical knowledge with clinical practice and developing competent nursing graduates.2, 3, 15
Faculty in this study appreciated that simulation offers an active, hands-on mode of learning that encourages reflection and experiential understanding, aligning with Jeffries’ framework 16 and the INACSL standards 17 that advocate participatory learning designs.
Faculty emphasized that simulation fosters a psychologically secure environment where students can practice procedures and learn from errors without posing risks to patients. Similar observations were reported in studies from Ethiopia 4 and Pakistan, 5 where educators valued the method for supporting ethical and safe practice. Respondents also observed noticeable improvement in students’ teamwork, communication, and clinical decision-making skills, echoing Baayd et al., 18 who identified simulation as an effective tool for developing professional competence across different educational contexts.
Educators who had completed structured training expressed greater confidence, motivation, and willingness to integrate simulation regularly, findings that parallel the work of Grover et al. 6 and Park et al. 10 Institutional encouragement and peer collaboration were further recognized as catalysts for successful adoption.8, 9
Despite the generally positive perceptions and growing confidence among faculty, implementation remains context-dependent. Some participants acknowledged persistent barriers such as inadequate infrastructure, limited faculty availability, and time constraints within existing curricula, challenges similarly highlighted in previous studies across Asia and Africa.4, 5, 9, 18
Overall, the study highlights growing faculty confidence and institutional willingness to adopt SBE. With sustained support, training, and infrastructure, simulation can be fully integrated into nursing curricula to enrich learning quality and promote patient-safe practice.
Implications for Nursing Education and Practice
The findings of this study underscore that successful integration of SBE requires more than faculty enthusiasm; it demands sustained institutional and policy-level support. To enhance implementation:
Faculty capacity building should be prioritized through regular simulation workshops, refresher training, and Continuing Nursing Education programs that focus on evolving simulation modalities and debriefing techniques. Structured FDPs should guide educators in designing, conducting, and evaluating simulation sessions, and in developing institution-specific implementation plans. Policy makers and accrediting bodies should address infrastructural gaps by investing in regional simulation centers and promoting inter-institutional collaboration to share resources, expertise, and best practices. Inclusion of simulation-based teaching as a quality criterion during institutional accreditation and inspection processes could further encourage systematic adoption across nursing programs.
Future Research
Future research could include nationwide exploratory or mixed-method studies assessing faculty knowledge, attitudes, practices, long-term utilization, challenges, strategies, and outcomes of simulation implementation across diverse institutional contexts.
Studies examining student learning outcomes, cost-effectiveness, and sustainability models of simulation integration would provide valuable insights for large-scale curricular reforms.
Evaluating the impact of continuous FDPs on teaching competence and learner outcomes could strengthen evidence for investment in ongoing simulation training.
Conclusion
The study highlights that nursing faculty in Northern India hold strong, positive perceptions of SBE, recognizing its value in enhancing realism, clinical preparedness, and learner engagement. Participants expressed varying levels of comfort and confidence in using simulation, largely attributed to their structured training at the simulation center, institutional encouragement, and personal motivation. To scale SBE nationally, the INC should reinforce national guidelines for simulation integration, establish standardized competency benchmarks for faculty, and promote periodic refresher programs. Strengthening faculty networks, incorporating structured simulation hours into the MRP, and fostering a supportive academic culture by institutions will further consolidate simulation as a cornerstone of high-quality nursing education in India.
Footnotes
Acknowledgments
The authors would like to thank the management of NRSC, SGT University, Haryana; Dr. T. Dileep Kumar, President, Indian Nursing Council (INC); and all participants who contributed to the study.
Data Availability Statement
The authors ensure the availability of data to the editor, keeping the names of the participants confidential due to ethical reasons (including audio recordings and transcripts).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval has been obtained from the Institutional Ethics Committee for the PhD study. As this manuscript is based on part of the work done for the PhD study, separate ethical approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed written consent has been obtained from the participants of the study to participate in the study, audio-recording, and publishing the research findings for widespread dissemination. Moreover, verbal consent was also taken during the audio recording of the interviews.