
Abstract
Background and Aims:
Chronic suppurative otitis media (CSOM), a prevalent middle ear inflammation, presents challenges in the post-coronavirus disease era due to increased patient loads, stringent infection control and irrational antibiotic use. Understanding the evolving bacterial growth and antimicrobial sensitivity patterns of CSOM is vital for effective management and treatment in this changing healthcare landscape.
Objectives:
This study aims to identify prevalent bacteria in CSOM patients attending an ENT outpatient department (OPD) in the tertiary care hospital and determine their antibiotic sensitivity patterns, contributing to an antibiotic stewardship policy.
Materials and Methods:
This cross-sectional study, conducted over five months, investigated the bacterial aetiology and antibiotic susceptibility patterns in CSOM patients attending the tertiary care hospital’s ENT OPD. The sample of 100 patients was selected using convenience sampling. Aural swabs were collected and sent for culture and sensitivity tests. Data were analysed using the chi-square test and one-way analysis of variance.
Results:
The study investigated bacterial prevalence in 100 otitis media patients. Pseudomonas aeruginosa (34%) and Staphylococcus aureus (25%) were the most prevalent organisms. Ciprofloxacin and amikacin showed the highest overall sensitivity. No significant association was found between gender and pathogen (P = .22316) or between mean ages across different pathogens (P = .416).
Conclusion:
The study identified P. aeruginosa and S. aureus as the most prevalent bacteria in CSOM. Ciprofloxacin and amikacin were highly effective against all identified bacteria. Although these antibiotics can be used as empirical therapy in remote areas without antibiotic susceptibility testing facilities, we suggest initiating culture-directed antibiotics to prevent antibiotic resistance and ensure optimal treatment outcomes.
Introduction
Otitis media is an inflammation of the mucoperiosteal lining of the middle ear, which can either present as an acute attack or chronic inflammation with subsequent complications. Chronic suppurative otitis media (CSOM) is defined as a chronic inflammation of the mucoperiosteal lining of the middle ear cleft, which presents with recurrent ear discharge or otorrhoea through a tympanic perforation. It has been classified into tubotympanic or mucosal (safe) and atticoantral or squamosal (unsafe) types.[1]
It has been a common health issue affecting a large number of individuals worldwide. The incidence of CSOM cases is estimated at more than 20 million people worldwide. Of these, approximately five million patients suffer from chronic otitis media with cholesteatoma. The prevalence of CSOM worldwide is around 65–330 million people with complaints of discharging ears. Sixty per cent of them (39–200 million) are found to suffer from significant hearing loss. The incidence of chronic otitis media with cholesteatoma is 3 in 100,000 in children and 9.2 in 100,000 adults.[2] India is one of the countries with highest CSOM prevalence (>6%).[3] In the post-coronavirus disease 2019 (COVID-19) era, tertiary care hospitals are facing many challenges, which include increased patient loads and adoption of stringent antibiotic policies. Moreover, there prevails an unregulated antibiotic intake among the general population. Previous studies have attempted to determine the etiology of otitis media and their antimicrobial sensitivity patterns in various populations.[4–6] However, the COVID-19 pandemic has resulted in significant changes in the healthcare landscape and possibly altered the epidemiology of infections. In such a scenario, understanding the bacteriology of otitis media in this context is important for effective management of patients.
This cross-sectional study aims to determine the various pathogens causing CSOM and their antibiotic sensitivity patterns in patients attending a tertiary care hospital. The antibiotic sensitivity of these bacteria will be analysed for better management of CSOM.
This would help in making evidence-based clinical decisions regarding empirical treatment for future cases. The findings of this study will contribute to the existing body of knowledge, helping to make informed decisions on the treatment of otitis media and guiding public health initiatives to help the community.
Aim and Objectives
To determine the common bacteria and their prevalence in patients with otitis media attending an ENT outpatient department (OPD) in a tertiary care hospital.
The objectives of the current study are as follows:
To identify the common organisms in culture-positive cases in the post-COVID era. To determine the antibiotic sensitivity pattern, thereby helping in the establishment of an antibiotic stewardship policy.
Methodology
Study Design
A cross-sectional study was conducted to investigate the bacteriology and antibiotic susceptibility patterns of CSOM in patients attending a tertiary care hospital.
Study Period
The study was carried out over a five-month period, from August 2022 to December 2022.
Study Centre
The research was conducted at the Department of Otorhinolaryngology, Government Medical College and Hospital, Omandurar Government Estate, Chennai.
Sample Population
The sample population consisted of patients attending the ENT OPD in the tertiary care hospital.
Inclusion Criteria
Participants were included in the study if they met the following criteria:
Patients diagnosed with chronic otitis media—mucosal type, presenting with painless, non-foul-smelling, non-blood-stained ear discharge for a duration of more than six weeks. Patients who had not received antibiotic treatment within the past 10 days.
Exclusion Criteria
The study excluded the following patients:
Patients who had previously undergone otologic surgeries. Patients diagnosed with otitis externa, traumatic perforations, or other granulomatous conditions causing ear discharge. Immunosuppressed patients.
Sample Size
Based on the study by Agarwal et al.,[7] the prevalence (p) was determined to be 0.376. The sample size was calculated using the formula:
where q is the complementary probability (1 − p) and L is the allowable error. The calculated sample size was determined to be 100.
Sampling Method
A convenience sampling method was employed to select participants for the study. This non-probability sampling technique was chosen due to its ease of use and the accessibility of the sample population within the study centre’s ENT OPD.
Procedure
In preparation for the collection, the patient was informed about the procedure and consent was obtained, while maintaining a comfortable seated position with their head slightly tilted away from the targeted ear. To maintain a sterile environment and prevent cross-contamination, the investigator donned appropriate personal protective equipment, such as disposable gloves. The external ear was cleansed using a sterile saline solution or an alcohol swab, particularly if visible dirt was present. An aural speculum of appropriate size was used. By employing a circular motion, the outer part of the ear, including the auricle or pinna, was gently wiped. Subsequently, the sterile swab, obtained from its packaging without contacting the swab tip, was carefully inserted into the ear canal. Once appropriately positioned, the swab was gently rotated in a circular motion within the ear canal for a brief duration, enabling the collection of any potential discharge. Upon completion, the swab was gradually withdrawn from the ear canal, ensuring that it did not come into contact with external surfaces. To maintain the integrity of the collected specimen, the swab was promptly transferred to a sterile transport tube. To facilitate proper identification and traceability, the transport tube housing the swab was clearly labelled with the patient’s relevant information, including name, sex and age. Additionally, the date and time of collection were recorded. The collected sample was sent to the microbiology laboratory for performing culture and sensitivity tests. The sensitivity tests were performed using the Kirby–Bauer disk diffusion method. The data from the culture and sensitivity reports were analysed.
Statistical Analysis
Comparison of the prevalence of various bacteria and their antibiotic sensitivity patterns was conducted. The collected data were analysed using chi-square test and one-way analysis of variance (ANOVA) to determine the association of age and sex with specific bacterial pathogens.
Results
The present study investigated the prevalence of various pathogens in a sample of 100 participants. Table 1 summarises the results in terms of the count and percentage of each organism identified in the sample. The most prevalent organism in the sample was Pseudomonas aeruginosa, which was found in 34 participants, accounting for 34% of the total sample. This was followed by Staphylococcus aureus, which was identified in 25 participants, comprising 25% of the sample. The no-growth group, indicating the absence of any detectable organisms, comprised 17 participants, representing 17% of the total sample. Klebsiella pneumoniae was found in eight participants, accounting for 8% of the sample, while Klebsiella oxytoca was present in seven participants, representing 7% of the sample. Proteus species and coagulase-negative Staphylococcus (CoNS) were both identified in three participants each, constituting 3% of the sample for each organism. Acinetobacter was present in two participants, accounting for 2% of the sample, and Non-albicans Candida was the least prevalent organism, found in only one participant, representing 1% of the total sample. The same is illustrated in Figure 1.
Culture sensitivity reports of aural swabs of patients with CSOM

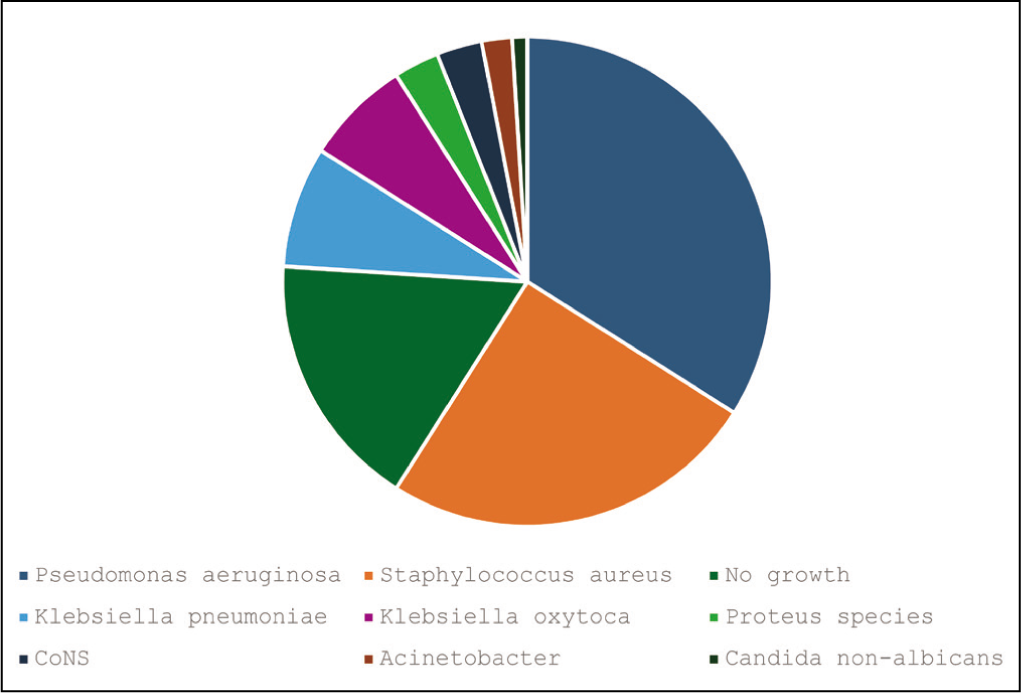
Table 2 and Figure 2 describe the antibiotic susceptibility patterns of seven bacterial species, including Acinetobacter, CoNS, K. oxytoca, K. pneumoniae, Proteus species, P. aeruginosa and S. aureus. The antibiotic profiles of these bacterial isolates were determined against 13 different antibiotics, namely gentamicin, erythromycin, amikacin, cefalexin, imipenem, ceftazidime, cotrimoxazole, piperacillin + tazobactam, ciprofloxacin, cefotaxime, vancomycin, penicillin G and cefoperazone.
Antibiotic sensitivity profile across selected bacterial strains: percentage of isolates susceptible to various antibiotics

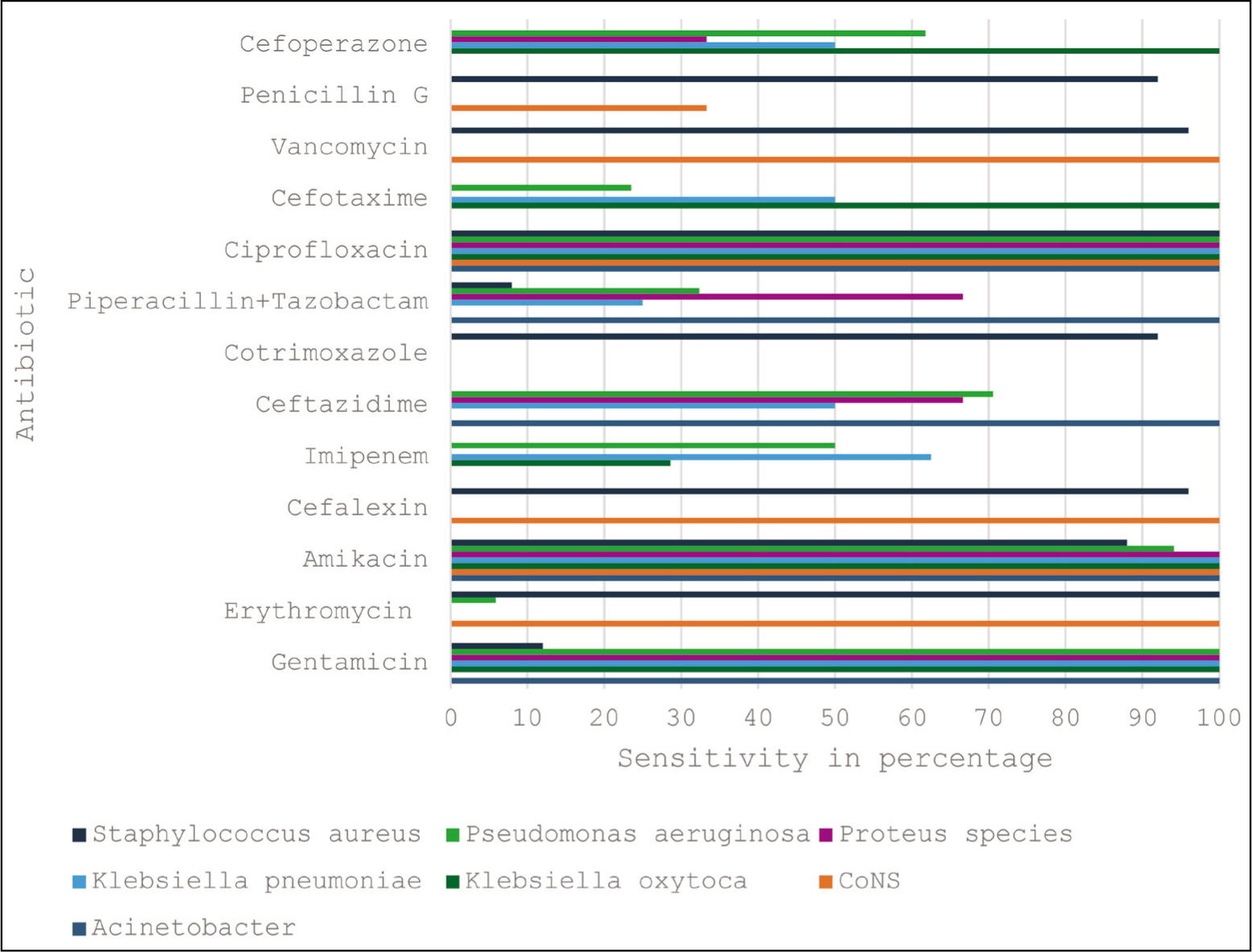
Acinetobacter isolates exhibited susceptibility to gentamicin, amikacin, ceftazidime, piperacillin + tazobactam and ciprofloxacin (100%).
CoNS isolates demonstrated susceptibility to erythromycin, amikacin, vancomycin, cefalexin and ciprofloxacin (100%). Low susceptibility was observed to penicillin G (33.33%).
K. oxytoca isolates showed susceptibility to gentamicin, amikacin, cefotaxime, cefoperazone and ciprofloxacin (100%). Susceptibility to imipenem was observed in 28.57% of the isolates.
K. pneumoniae isolates exhibited susceptibility to gentamicin, amikacin and ciprofloxacin (100%). The isolates showed 62.5% susceptibility to imipenem, 50% susceptibility to ceftazidime, cefoperazone and cefotaxime, and 25% susceptibility to piperacillin + tazobactam.
Proteus species isolates displayed susceptibility to gentamicin, amikacin and ciprofloxacin (100%). Susceptibility to ceftazidime and piperacillin + tazobactam was observed in 66.66% of the isolates. The isolates showed 33.33% susceptibility to cefoperazone.
P. aeruginosa isolates showed susceptibility to gentamicin (100%), erythromycin (5.88%), amikacin (94.12%), imipenem (50%), ceftazidime (70.58%), cefoperazone (61.76%), piperacillin + tazobactam (32.35%) and ciprofloxacin (100%). Susceptibility to cefotaxime was observed in 23.53% of the isolates.
S. aureus isolates demonstrated susceptibility to erythromycin (100%), amikacin (88%), cefalexin (96%), cotrimoxazole (92%), ciprofloxacin (100%), vancomycin (96%), piperacillin + tazobactam (8%) and penicillin G (92%). Susceptibility to gentamicin was observed in 12% of the isolates.
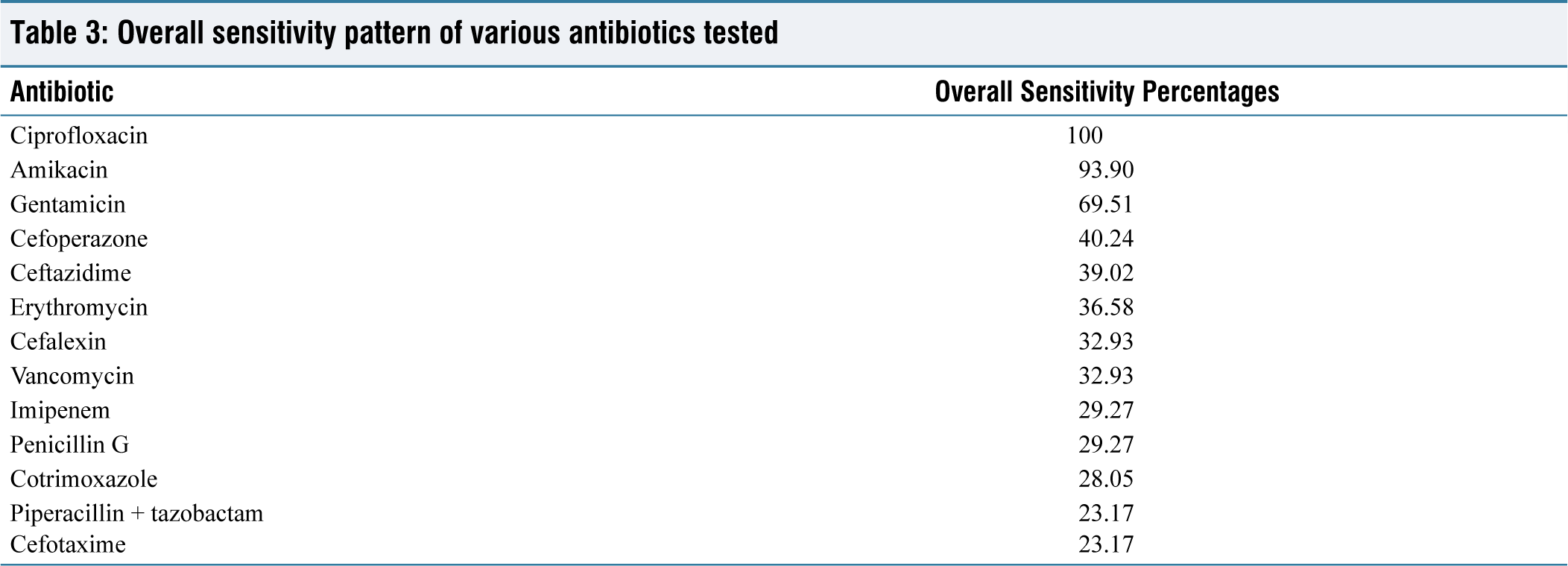
The results summarised in Table 3 and Figure 3 revealed that the highest overall sensitivity percentage was observed for ciprofloxacin (100%), indicating that it was effective against all bacterial species tested. Amikacin demonstrated a high overall sensitivity percentage of 93.90%, suggesting its broad-spectrum effectiveness against most tested bacterial species.
Overall sensitivity pattern of various antibiotics tested
Overall sensitivity pattern of various antibiotics tested
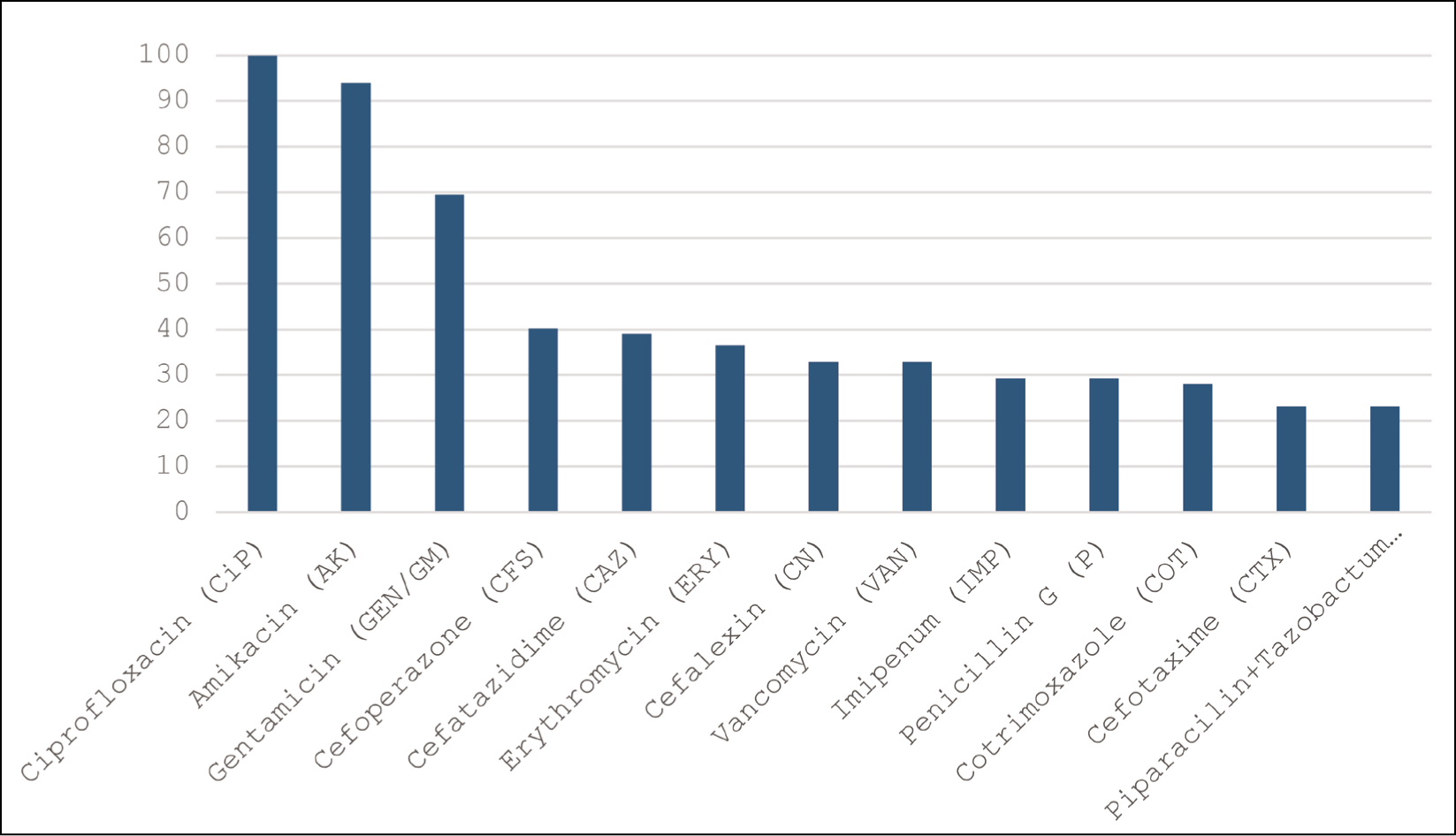
Gentamicin exhibited a moderate overall sensitivity percentage of 69.51%. Other antibiotics, such as erythromycin (36.58%), cefalexin (32.93%), imipenem (29.27%), ceftazidime (39.02%), cotrimoxazole (28.05%), piperacillin + tazobactam (23.17%), cefotaxime (23.17%), vancomycin (32.93%), penicillin G (29.27%) and cefoperazone (40.24%), displayed relatively lower overall sensitivity percentages.
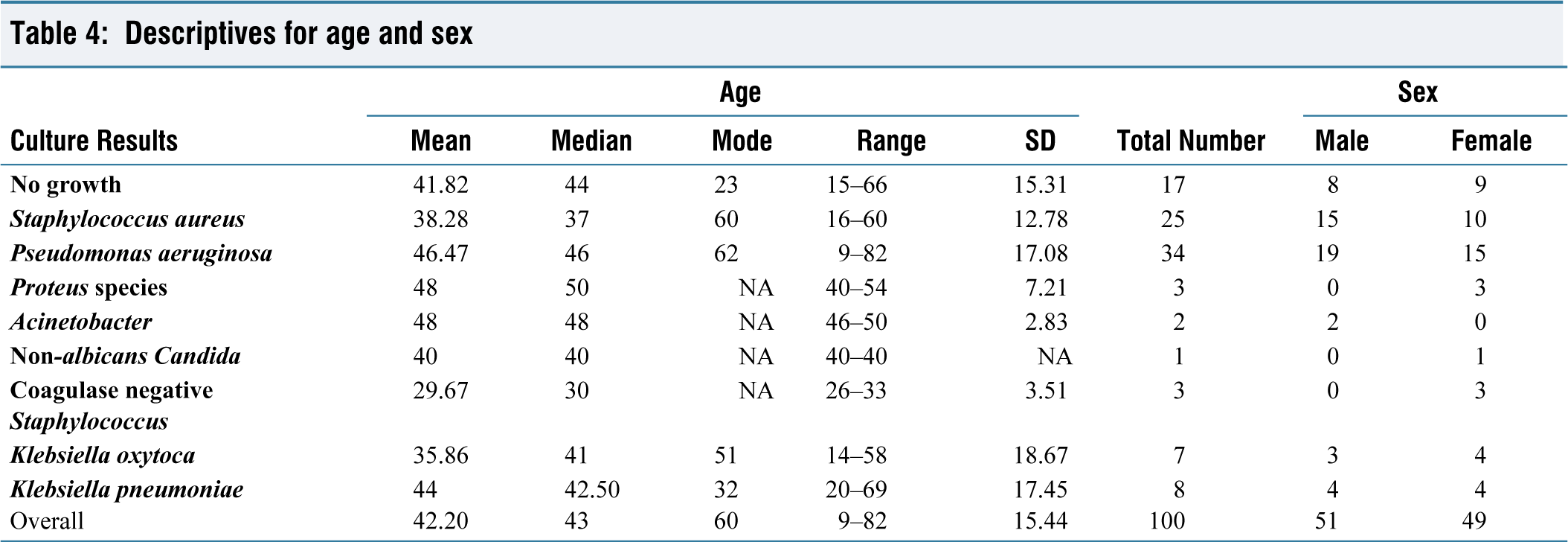
The study analysed aural swab culture results from 100 participants, with an equal sex distribution of 51 males and 49 females, and ages ranging from 9 to 82 years. The groups were categorised as follows: ‘no growth’ (17 participants, mean age 41.82 years), S. aureus (25 participants, mean age 38.28 years), P. aeruginosa (34 participants, mean age 46.47 years), Proteus species (3 females, mean age 48 years), ‘Acinetobacter’ (2 males, mean age 48 years), Non-albicans Candida (1 female, 40 years), ‘CoNS’ (3 females, mean age 29.67 years), K. oxytoca (7 participants, mean age 35.86 years) and K. pneumoniae (8 participants, mean age 44 years). Overall, the mean age was 42.20 years. These results are summarised in Table 4.
Descriptives for age and sex
The results from the chi-square analysis [Table 5] indicate a chi-square statistic of 10.64 and a P value of .22316. With 8 degrees of freedom, the P value is greater than the commonly used significance level of .05. This means that we fail to reject the null hypothesis, suggesting that there is no significant association between gender and the type of infection in this data.
Comparison of expected and observed culture results for various microbial agents by gender: chi-square analysis
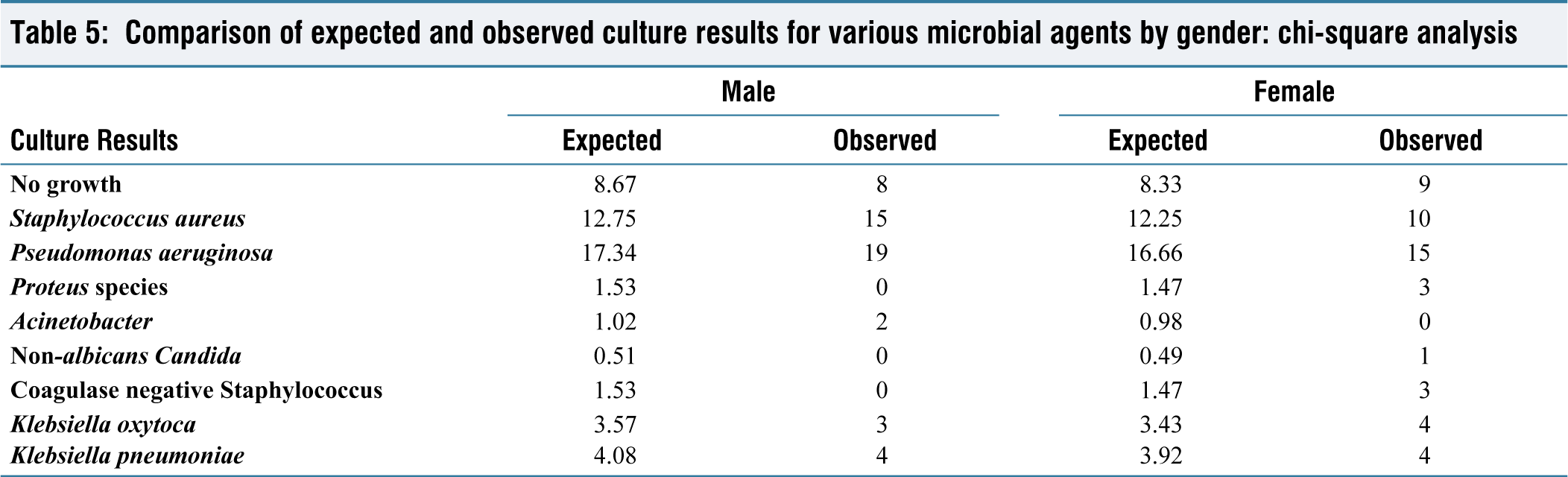
The one-way ANOVA test produced an F-statistic of 1.04 and a P value of .416. In this case, the P value of .416 is greater than the significance level of .05. Therefore, there is no significant difference in the mean ages across the different infection types.
Discussion
Otitis media, an inflammation of the middle ear, is a common disease affecting our population. This study aimed to identify the common organisms causing CSOM and their antimicrobial susceptibility patterns to improve the clinical outcomes. Our study analysed 100 samples, with an average age of 42.20 years and an age range of 9–82 years. The gender distribution is almost equal, with 51 males and 49 females. The average age varies among the categories, with CoNS having the lowest average age (29.67 years) and P. aeruginosa having the highest average age (46.47 years). The age range also varies significantly among the categories, with P. aeruginosa covering the widest range (9–82 years) and Non-albicans Candida having the smallest range (only 1 case of 40 years). Some categories show a more balanced gender distribution, such as K. pneumoniae (4 males and 4 females) and no growth (8 males and 9 females). The standard deviation values indicate variability in age distribution for each category. K. oxytoca shows the highest variability (SD = 18.67), while Acinetobacter has the least variability (SD = 2.83). This suggests that the age distribution for K. oxytoca is more widespread, while Acinetobacter has a more concentrated age distribution around the average age. Considering the overall data, it is evident that different types of infections affect various age groups and that there is a diverse gender distribution across the categories. Further research could explore the reasons behind these differences, such as underlying risk factors, environmental influences, or genetic predispositions. Statistical analysis reveals that there is no significant association between age, sex and the bacteria causing the infection.
P. aeruginosa emerged as the most prevalent organism in our sample, accounting for 34% of the cases, followed by S. aureus (25%), and the no growth group (17%). In line with our findings, Alam et al., in Northern India, Shwetha et al., Sandhu et al. and Mahajan et al., found that P. aeruginosa was found to be the most common, followed by S. aureus. However, the antibiotic susceptibility differs from ours, with Alam et al. reporting that piperacillin–tazobactam was found to be most effective.[8–11] Prakash et al. conducted a study in Chennai in 2013 and found that S. aureus was most common, followed by P. aeruginosa. However, ciprofloxacin was found to be less sensitive.[12]
Our study also assessed the antibiotic susceptibility patterns of the identified bacterial species. The highest overall sensitivity percentage was observed for ciprofloxacin (100%), suggesting its efficacy as a therapeutic option for infections caused by the tested bacterial species. Amikacin also demonstrated high overall sensitivity (93.90%), indicating its potential as a broad-spectrum antibiotic for treating CSOM cases. Gentamicin exhibited moderate overall sensitivity (69.51%), while other antibiotics showed relatively lower sensitivity percentages. These findings align with the studies by Poorey and Iyer and Mofatteh et al., which reported ciprofloxacin and amikacin as the most effective antibiotics.[13,14] However, our results differ from the study conducted by Gupta and Kumbhat, which reported varied antibiotic susceptibility patterns, with piperacillin–tazobactam, meropenem, vancomycin and linezolid as the most sensitive antibiotics.[15]
In contrast, Alam et al. found that the most common bacterium causing CSOM was S. aureus, followed by P. aeruginosa and Proteus, with vancomycin and piperacillin + tazobactam identified as the most effective antibiotics.[16] Another study by Agrawal et al. in 2012 reported S. aureus as the most common, followed by P. aeruginosa. They also identified Escherichia coli and Streptococcus, which were not found in this study. Additionally, they found imipenem to be the most effective antibiotic.[7] Similarly, studies conducted by Shrestha et al. in 2010 and Sah et al. in 2020 from Nepal found that S. aureus was the most prevalent, followed by P. aeruginosa, with ofloxacin exhibiting the highest efficacy.[17,18] A study conducted by Mofatteh et al. in Iran in 2018 found that S. aureus and Klebsiella were the most common, followed by P. aeruginosa.[14] Another interesting finding by Sandhu et al. was that piperacillin and vancomycin were found to be the most sensitive antibiotics.[11] Similarly, Sharma et al. in 2021 found that S. aureus was the most common, followed by P. aeruginosa.[19] Madana et al., from JIPMER, Pondicherry, reported that P. aeruginosa, Proteus and Staphylococcus were most common, while ceftazidime and vancomycin were found to be most susceptible antibiotics.[20]
This reveals a varying pattern in the antibiotic sensitivity profiles across varying geographical areas and time periods, emphasising the need for appropriate antimicrobial sensitivity testing before initiating treatment. This approach would also help reduce the development of antibiotic resistance, which is on the rise, by promoting judicious use of antibiotics. The findings of this research can be used in the empirical management of patients in high-volume, low-resource settings where antibiotic susceptibility testing may not be feasible. It is also evident that continued research in this context is essential to determine the constantly varying patterns of pathogens and their antimicrobial sensitivity to ensure the best possible care for patients.
Conclusion
Based on this study, the most prevalent bacterium causing CSOM was found to be P. aeruginosa, followed by S. aureus. Proteus, Klebsiella and Acinetobacter were also identified in other cultures. Ciprofloxacin was found to be effective against all bacteria identified, followed by amikacin. Based on these findings, it is suggested that ciprofloxacin or amikacin can be used as empirical therapy for the management of CSOM in remote areas where antibiotic susceptibility testing facilities are not available. However, it is important to exercise caution and avoid indiscriminate use of these antibiotics to prevent the development of antibiotic resistance. This approach will ensure the most effective treatment for patients with CSOM, thereby improving clinical outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical Committee approval was obtained before starting the study (IEC No.: 75/IEC/GOMC/2022).
Informed consent
The patient was informed about the procedure and consent was obtained.
Credit author statement
Conceptualisation: Swaminathan Ramasubramanian, Sonali Dhanaseelan, Shamuga Ashok.
Methodology: Swaminathan Ramasubramanian, Sonali Dhanaseelan, Aishwarya Prateep, Shamuga Ashok.
Formal Analysis and Investigation: Swaminathan Ramasubramanian, Sonali Dhanaseelan, Aishwarya Prateep.
Writing—original draft preparation: Swaminathan Ramasubramanian, Sonali Dhanaseelan.
Writing—review and editing: Swaminathan Ramasubramanian, Sonali Dhanaseelan, Aishwarya Prateep.
Supervision: Aishwarya Prateep, Shamuga Ashok.
Data availability
All data is contained within the manuscript.
Use of artificial intelligence
No AI tools were used in this manuscript.