
Abstract
Background and Aims:
Undiagnosed exudative pleural effusions were defined as pleural effusions in which an aetiological diagnosis could not be ascertained by initial pleural fluid analysis. Between 25% and 30% of pleural effusions may remain undiagnosed despite a combination of pleural fluid analysis and closed pleural biopsy. Medical thoracoscopy may assist physicians in diagnosing such cases.
Aims and Objectives:
This study aims to study the diagnostic utility of medical thoracoscopy in undiagnosed pleural effusions.
Materials and Methods:
This is an observational prospective, hospital-based study conducted on 40 patients at the Government Hospital for Chest and Communicable Diseases, Department of Pulmonary Medicine, Andhra Medical College, Visakhapatnam, from January 2024 to December 2024. The study was carried out after obtaining institutional ethics clearance and informed written consent from the participants.
Results:
Thoracoscopy was performed in 40 patients, of whom 29 were male and 11 were female. The indication for thoracoscopy in all these patients was inconclusive initial pleural fluid analysis. Of the 40 cases, 17 were diagnosed as malignant and 23 as non-malignant. Of the 23 non-malignant cases, 15 were diagnosed as tuberculosis.
Conclusion:
Based on our results, we conclude that, given its high diagnostic yield and acceptable safety profile, rigid thoracoscopy should be considered in the evaluation of exudative pleural effusion when pleural fluid analysis is inconclusive.
Keywords
Introduction
Pleural effusion, defined as the pathological accumulation of fluid within the pleural cavity, is a common clinical issue encountered in respiratory medicine. More than 60 different causes have been identified, encompassing primary pleural conditions, lung-related diseases, systemic organ dysfunction and drug-related effects. The most frequent causes are congestive heart failure, infectious pleural conditions, such as pneumonia and tuberculosis, and malignancies.[1]
The fluid build-up arises due to either increased production or decreased absorption. In healthy individuals, pleural fluid is produced at a rate of approximately 0.26 mL/kg/h, while clearance—mainly through the lymphatic stomata of the parietal pleura—occurs at a slightly lower rate of about 0.20 mL/kg/h.[2]
In India, exudative pleural effusions are most often attributed to tuberculosis, cancer, parapneumonic infection and pulmonary embolism. Malignancies, particularly those originating in the lungs and breasts, account for a significant proportion. Other, less common, malignancies affecting the pleura include lymphomas and cancers of the ovaries, uterus, kidneys, stomach and colon. Notably, nearly 15% of lung cancer cases present with pleural effusion at the time of diagnosis. Among malignancies, adenocarcinoma is most frequently associated with such effusions, whereas small cell lung cancer rarely causes them.
When initial investigations—including cytology, cell block studies and adenosine deaminase (ADA) levels—fail to determine the aetiology of an effusion, and pulmonary embolism has been excluded, thoracoscopy becomes a critical diagnostic step.[1] This procedure can be performed using either rigid or flexible thoracoscopes, each with its respective benefits. Rigid thoracoscopy generally offers a superior diagnostic yield due to its ability to obtain larger tissue samples, although it may cause more patient discomfort. Medical thoracoscopy enhances diagnostic accuracy by allowing direct visual inspection and targeted sampling from the costal, diaphragmatic and mediastinal pleura. Additionally, it plays a key role in staging thoracic cancers such as mesothelioma and lung cancer, and in excluding conditions like Mycobacterium tuberculosis and malignancy with high reliability.
Methods
Study Setting
This study was conducted in the Department of Pulmonary Medicine at the Government Hospital for Chest and Communicable Diseases, affiliated with Andhra Medical College, Visakhapatnam.
Study Duration
The research was carried out over a 1-year period, from January 2024 to December 2024.
Study Design
A prospective, observational, tertiary care hospital-based study was undertaken using a consecutive sampling technique.
Statistical Analysis
Data analysis for this study was performed using SPSS software, Version 20.0.
Inclusion Criteria
Patients with pleural effusion for whom a definitive aetiological diagnosis could not be established through initial pleural fluid analysis.
Cases that were diagnosed as exudative pleural effusion according to Light’s criteria.
Exclusion Criteria
Patients who are newly diagnosed with smear-positive tuberculosis.
Cases of smear-positive retreatment tuberculosis.
Individuals with respiratory failure.
Patients unwilling to provide informed consent.
Those deemed unfit for thoracoscopy.
Patients receiving anticoagulant therapy.
Individuals with known coagulation disorders.
Cases with empyema.
Patients with a recent myocardial infarction or a history of cardiac arrhythmias.
Individuals with thrombocytopenia (platelet count <60,000/mm3).
Patients unable to maintain a lateral decubitus position.
Method of Study
Patients presenting with moderate to large pleural effusions identified on imaging underwent initial diagnostic work-up with thoracentesis. The aspirated fluid was subjected to analysis for cytological examination, total and differential leucocyte counts, protein and glucose levels and ADA activity. If a conclusive diagnosis could not be reached using these parameters, and the patient was deemed medically fit for the procedure, medical thoracoscopy was considered for further evaluation.
Preoperative Assessment
Each patient underwent a comprehensive clinical evaluation, including a detailed medical history and thorough physical examination.
Laboratory Work-up
The following blood tests were performed as part of the pre-thoracoscopy preparation:
Complete blood count: To identify anaemia, infection or low platelet counts. Coagulation profile: Including bleeding time, clotting time, prothrombin time with international normalised ratio and activated partial thromboplastin time, particularly relevant for patients on anticoagulants. Renal function tests: Blood urea and serum creatinine, to assess bleeding risk in the context of renal dysfunction. Liver function tests: Evaluated using alanine transaminase, aspartate transaminase) and bilirubin levels. Electrolytes: Serum sodium, potassium and related parameters. Blood grouping and typing, in case transfusion is required. Viral screening: All patients were tested for HIV, hepatitis B surface antigen and hepatitis C virus.
Pulmonary Evaluation
Pulmonary status was assessed using arterial blood gas analysis and spirometry. Spirometric measurements included forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and the FEV1/FVC ratio to assess pulmonary reserve and baseline function.
Cardiac Assessment
Electrocardiography (ECG) and transthoracic echocardiography were performed to determine cardiac suitability for the procedure.
Imaging
Chest radiography (posteroanterior and lateral views), along with lateral decubitus imaging, was routinely performed. In selected cases, ultrasonography or CT thorax (computed tomography of the chest) was used to further evaluate pleural abnormalities, such as thickening, loculations and underlying lung pathology.
Procedure
Pre-procedure Preparation
Patients were instructed to fast from solids for at least 6 h and from clear fluids for a minimum of 2 h prior to the thoracoscopy procedure.
Premedication
Midazolam (0.05–0.15 mg/kg intravenously (IV)) was administered for anxiolysis, and glycopyrrolate (0.005–0.01 mg/kg IV) was used to reduce salivary and airway secretions.
Positioning
Patients were placed in the lateral decubitus position, with the unaffected side downwards. The dependent side was padded for comfort, and the arm and forearm were supported with armrests beneath. Additional supports were also used to stabilise the pelvis.
Sedation and Monitoring
The procedure was performed under local anaesthesia with conscious sedation. Midazolam (0.5–1 mg IV, titrated as required) and fentanyl (4-20 µg IV) were used for sedation and pain control. Continuous monitoring included ECG, non-invasive blood pressure, pulse oximetry and capnography to promptly detect hypoventilation.
Entry Site Selection
In cases with large or loculated effusions, ultrasonography was used to identify the safest entry point, targeting areas with at least 5 cm of fluid depth. For minimal effusions, the standard entry site was the fifth intercostal space along the mid-axillary line.
Local Anaesthesia
Lidocaine 1% was used for infiltration in a graded fashion, with a maximum dose of 3 mg/kg (not exceeding 250 mg or 25 mL). The anaesthetic was administered from the skin down to the parietal pleura, with special attention to the intercostal nerve and periosteum. Aspiration was routinely performed before each injection to avoid accidental intravascular administration.
Thoracoscope Insertion
A vertical skin incision of approximately 10 mm was made, aligned parallel to the intercostal space. A trocar was inserted using controlled corkscrew movements until the pleural space was entered, confirmed by a loss of resistance. The depth was regulated using the index finger. Once the pleural space was accessed, the trocar was removed, leaving the cannula in place, secured 1–3 cm within the cavity by an assistant.
The thoracoscope was then introduced through the cannula. If pleural fluid was present, it was aspirated through the working channel. Full visual exploration of the pleural cavity was performed using a video-assisted system, including evaluation of the parietal pleura, diaphragmatic surface and costophrenic angles. Suspicious areas were sampled using optical biopsy forceps, typically obtaining five to seven specimens with a shearing technique from the parietal pleura.
Post-procedure Care
An intercostal chest drain (24–28 Fr) was inserted and connected to an underwater seal drainage set-up. Biopsy specimens were sent for histopathological evaluation. The chest tube was removed once the daily fluid output dropped below 50 mL.
Results
A total of 40 patients underwent thoracoscopy between January 2024 and December 2024. Of these, 29 were male and 11 were female. All patients had exudative pleural effusion of unknown aetiology, as the initial pleural fluid analyses were inconclusive. Thoracoscopy was performed in each case, and targeted biopsies of the parietal pleura were obtained under direct visualisation.
The mean age of the study population was 43 ± 14.9 years, with the youngest patient aged 18 years and the oldest aged 71 years.
Regarding the extent of effusion, 23 patients presented with massive pleural effusion, while 17 had moderate effusion.
The laterality of the effusion was evenly distributed: 20 patients (50%) had left-sided pleural effusion, and the remaining 20 (50%) had right-sided effusion. No cases of bilateral pleural effusion were observed in this cohort.
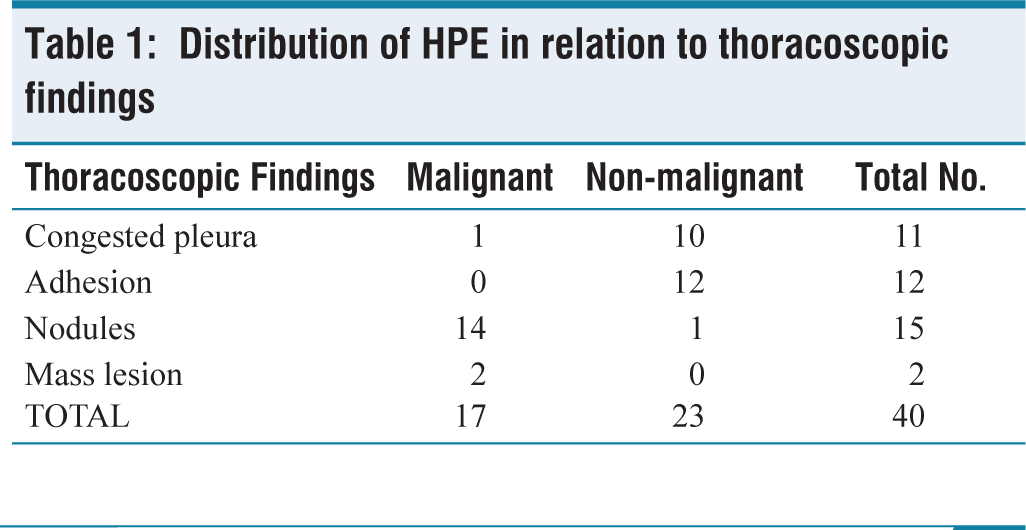
Thoracoscopic findings revealed pleural adhesions in 12 cases and mass lesions in 2 patients, both of which were confirmed to be malignant on histopathological examination. Congested pleura was observed in 11 patients; of these, 10 were non-malignant and one was malignant. Pleural nodules were noted in 15 cases, 14 of which were diagnosed as malignant and 1 as non-malignant [Table 1].
Distribution of HPE in relation to thoracoscopic findings
In our study, 24 cases presented with straw coloured pleural effusion, of which 22 were non-malignant and two were malignant. Sixteen cases had haemorrhagic effusion, of which 15 were malignant and 1 was non-malignant [Table 2].
Histopathology with colour of pleural fluid

Out of 40 cases, 17 were malignant and 23 were non-malignant. Of the 23 non-malignant cases, 15 were diagnosed as tuberculosis, while the remaining 8 cases were diagnosed as chronic pleural fibrosis, acute inflammatory process and chronic non-specific inflammation [Table 3].
Broad classification of etiologies

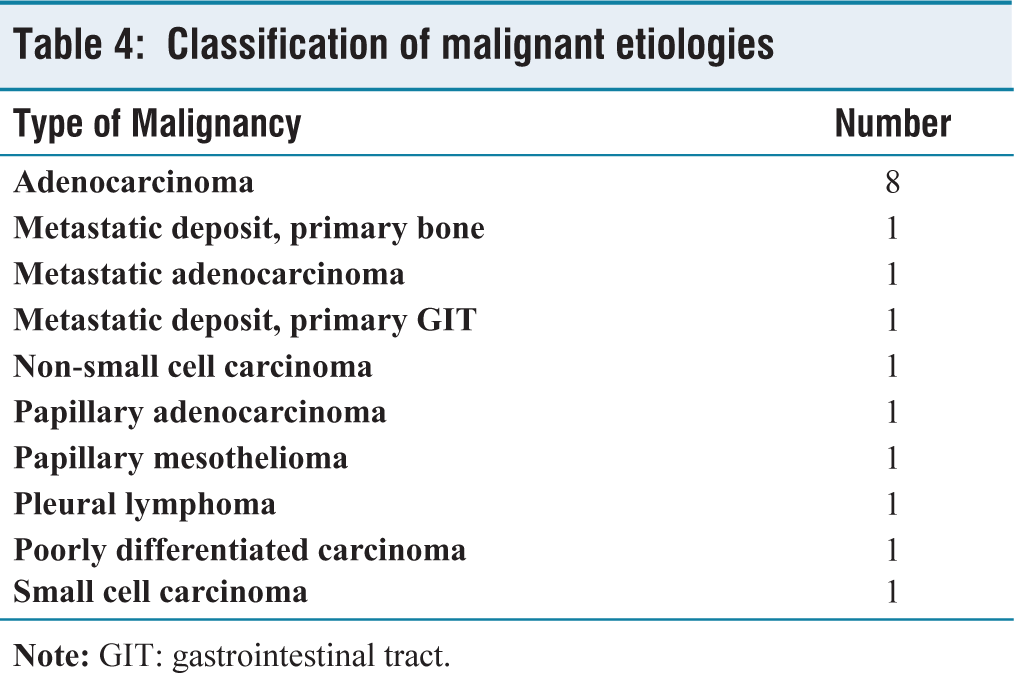
Among the 17 malignant cases, the majority were adenocarcinoma. There were 8 cases of adenocarcinoma, 1 metastatic carcinoma with primary bone, 1 case of metastatic deposits with primary gastrointestinal tract, 1 metastatic adenocarcinoma, 1 non-small cell carcinoma,1 papillary adenocarcinoma,1 papillary mesothelioma, 1 pleural lymphoma, 1 poorly differentiated carcinoma of the lung and 1 small cell carcinoma [Table 4].
Classification of malignant etiologies
Discussion
Thoracoscopic pleural biopsy continues to be the most definitive diagnostic approach for identifying malignant and tuberculous pleural effusions. Reported diagnostic accuracies reach up to 95% for malignancies and 99% for tuberculosis, significantly exceeding the sensitivity levels achieved by closed pleural biopsies or pleural fluid analyses.[3]
In this study, thoracoscopy was conducted on 40 individuals presenting with exudative pleural effusions of unclear origin following inconclusive initial fluid assessments. The overall diagnostic success rate achieved through thoracoscopic pleural biopsy was 80%. This is consistent with previously reported figures: Sobha et al.[4] documented an 87.8% yield, Augustine et al.[5] and Shrestha et al.[6] both reported a perfect 100%, Kuwal et al.[7] noted 83.64% and Abd El Rehim Yousef et al.[8] observed 80.6%.
Among the malignant effusions identified in our series, metastatic lung cancer emerged as the most common aetiology, with adenocarcinoma accounting for 50% of these cases. These results are in agreement with those of Malik and Mir,[9] who found adenocarcinoma in 67% of cases, and Kuwal et al.[6] who reported a frequency of 45.16%. The second most frequent cause of malignant effusion was metastatic disease originating from non-pulmonary sites, such as the skeletal system.
Of the 23 patients with non-malignant effusions, 65.2% were diagnosed with tuberculosis. This figure closely mirrors the findings of Krishnaraj et al.[10] (62%) and Augustine et al.[5] (56%). Conversely, Malik and Mir[9] reported a lower incidence of 31%. The high rate of tuberculosis in our sample likely reflects the institution’s function as a specialised referral centre for tuberculosis-related conditions. The other benign diagnoses included chronic fibrotic changes, acute pleural inflammation and nonspecific chronic inflammatory findings.
The visual thoracoscopic findings showed strong correlation with the final diagnoses. All individuals presenting with pleural adhesions were ultimately diagnosed with non-malignant diseases. Conversely, 93.3% of patients who had pleural nodules and all those with pleural masses were found to have malignant pathology (P = .001). Haemorrhagic pleural effusion was also significantly linked with malignancy—15 out of 16 cases (93.75%) were cancer-related. In contrast, among 24 patients who had straw-coloured effusions, only 2 were malignant, while 58.3% were diagnosed with tuberculosis (P = .001).
The thoracoscopic procedure was well tolerated across the cohort, with no recorded complications such as subcutaneous emphysema, prolonged air leakage or empyema. These findings further affirm the safety and reliability of thoracoscopy as a diagnostic modality.
Conclusions
The findings of this study affirm that rigid thoracoscopy is a highly effective and safe tool for diagnosing cases of exudative pleural effusion that remain unexplained after initial fluid evaluation. Its diagnostic accuracy in detecting both malignant and tuberculous causes makes it a valuable second-line investigation when non-invasive tests are inconclusive. The common practice of starting empirical anti-tuberculosis treatment in undiagnosed effusions—especially in settings with limited resources—should be reconsidered and ideally reserved for cases with histopathological confirmation. In addition to its diagnostic utility, thoracoscopy also serves important functions in cancer staging, diagnosing mesothelioma and enabling therapeutic interventions like pleurodesis and the release of adhesions. Although the outcomes of this study are encouraging, further large-scale research is needed to substantiate and generalise these observations.
Limitations
Small Sample Size
The study included only 40 patients, which limits the ability to generalise findings to a broader population.
Single-centre Study
The study was conducted at a single tertiary care institution, potentially introducing selection bias and limiting external applicability.
Supplemental material
Supplemental material for this article is available online.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
IEC No.: 286/IEC AMC/DEC 2023.
Informed consent
Written informed consent was obtained from all participants prior to inclusion in the study.
Credit author statement
D.V. Pratapa Reddy: Conceptualisation, methodology, investigation and writing.
V. Vijayakumari: Validation and supervision.
Neha Tarannum: Data curation, writing and visualization.
Raghumanda Sunil Kumar: Supervision and project administration.
CH.R.N. Bhushana Rao: Supervision and project administration.
Siddavali Chagalamarri: Validation and supervision.
Data availability
Non-digital data were curated at the Department of Pulmonary Medicine, Andhra Medical College, Visakhapatnam.
Use of artificial intelligence
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.