
Abstract
Background:
The intraoperative frozen section (IFS) diagnosis is a reliable diagnostic tool to rapidly diagnose ovarian neoplasms, thereby preventing debulking surgeries in benign cases.
Objective:
We aim to correlate and identify the concordance in intraoperative diagnosis with the permanent histopathology diagnosis.
Materials and Methods:
A retrospective study of concordance in FS diagnosis of 484 cases of ovarian neoplasms compared with the final diagnosis from January 2014 to December 2023 in the Department of Histopathology.
Results:
The study included 484 cases of ovarian neoplasms, of which 471 (97.3%) were concordant and 13 (2.7%) were discordant. In 13 discordant cases, 4 were overdiagnosed in the FS and proceeded with extensive surgery. The remaining discordant cases did not receive undertreatment or overtreatment. The sensitivity of FS diagnosis in benign, borderline, and malignant tumours was 91.2%, 91.3% and 87%, respectively.
Conclusion:
The FS diagnosis is a reliable method for intraoperative diagnosis of ovarian neoplasms. The detailed evaluation of the patient’s clinical history, imaging findings, and active intraoperative consultation with the surgeon will help in reducing the rate of discordance.
Introduction
Ovarian cancer is a devastating disease as it is often diagnosed late, hence related to poor diagnosis and survival.[1] Ovarian tumours are diagnosed in all age groups. In patients of reproductive age, benign and borderline ovarian tumours will be treated with fertility-sparing surgery. They will not perform major procedures on some malignancies because they are chemosensitive, such as germ cell tumours. Currently, ovarian cancers are diagnosed using imaging modalities such as CT, USG, and MRI, as well as serum tumour markers like CA125. However, none of these techniques can reliably predict the malignant behaviour of ovarian tumours. The patient may be over-diagnosed or under-diagnosed, which could lead to overtreatment or undertreatment, increasing preventable morbidity or requiring a second operation.[2] To prevent extensive debulking surgery and proceed with fertility-sparing surgery in the case of benign tumours, as well as to avoid incomplete surgery and staging in the case of borderline and malignant tumours, a correct frozen section (FS) diagnosis is essential. FSs can typically discriminate between benign and malignant tumours with an accuracy of 90%, but they are substantially less effective in identifying borderline tumours.[3] This study assesses the concordance of the intraoperative FS (IFS) diagnosis and final histopathological diagnosis. Also, analyse the possible causes of discordance to reduce the risk of under- or over-treatment.
Materials and Methods
After institutional ethics committee approval was obtained, we collected the data of all patients with ovarian neoplasms who underwent IFS diagnosis followed by histopathological examination in our department from 2014 to 2023.
The aim of this study was to correlate and identify the concordance in intraoperative diagnosis with the permanent histopathology diagnosis.
Patients who did not have an FS analysis of pathologic specimens were excluded. The pathology reports of all patients were extracted from the hospital medical record database. Pathology reports were used to determine histologic subtype, patient age, type of surgery undergone, tumour stage, and tumour size. The intraoperative specimens were sent to the histopathology department after a prior discussion with the pathologist about the patient’s details and history with the operating surgeon. The pathologist takes representative sections from the tumour after the complete gross examination. The sections were frozen in the Leica Cryostat CM3050s and sectioned at -23°C. The FS report was mostly given within 20 minutes of receiving the specimen. The Haematoxylin and eosin-stained slides of concordant and discordant cases were reviewed.
Statistical Analysis
Descriptive statistics were presented with frequency (percentage). McNemar’s Bowker test was used to determine the significant difference in the proportion between Frozen and final visits. A P value < .05 is considered statistically significant. All the statistical analyses were carried out using SPSS (IBM, 28.0).
Results
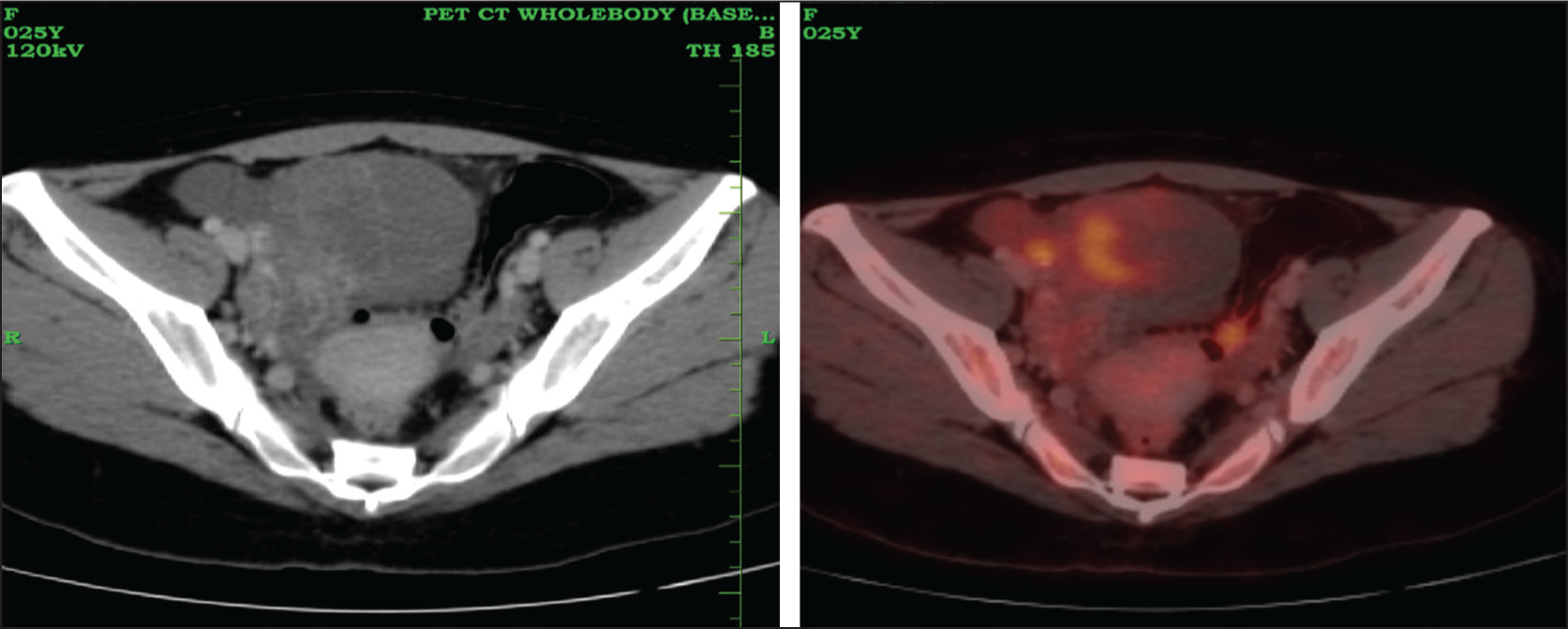
A total of 484 cases were included, with both IFS and final histopathological diagnoses. Table 1 summarises the clinical and demographic details of all cases. The patients diagnosed with ovarian neoplasm were mainly in the 41–60-year-old age group. As per the clinical data available in 108 cases, 71 cases had elevated serum tumour markers (65.7%), 20 patients were known cases of carcinoma on sites other than the ovary (18.5%), and 10 were known cases of ovarian neoplasm (9.3%). Figures 1 and 2 show PET CT images of patients with ovarian neoplasm. There was no significant difference in the laterality of ovarian tumour occurrence. The patients with bilateral ovarian neoplasm were 56/484 (11.5%). Most tumours were smaller than 10cm (39.8%) and were diagnosed in stage 1 (64.4%).
Clinical and demographic details

PET CT shows a large, relatively well-defined lobulated multiloculated complex mass with cystic and ill-defined FDG avid enhancing solid components noted in the right adnexal region measuring 5.8 × 8.4 × 10.2 cm (SUV max 4.1)
PET CT shows an FDG-avid large complex solid cystic mass with internal septations and loculations noted in the midline pelvis, measures ~9.5 (AP) × 11.5 (T) × 12.6 (CC) cm. There is heterogeneous enhancement noted within the solid component and internal septations
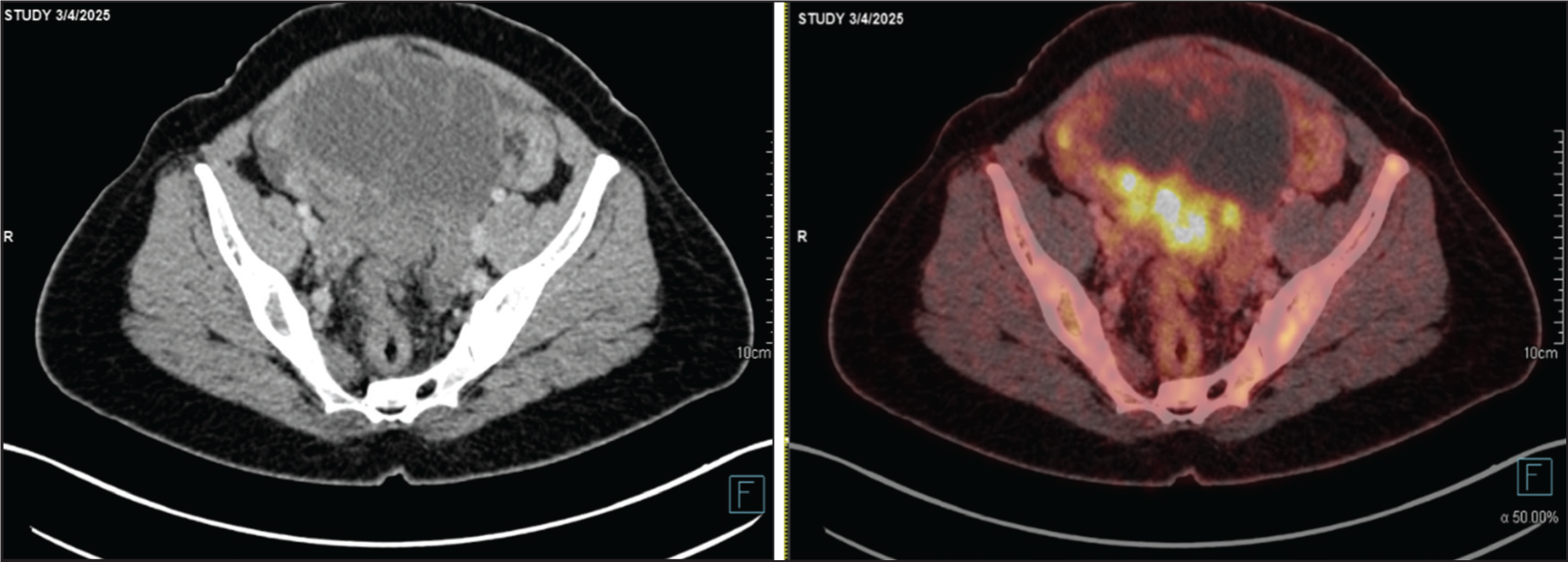
Table 2 shows a comparative analysis of FS diagnosis with that of permanent paraffin section diagnosis of all the ovarian tumours. In the FS diagnosis, malignant epithelial tumours constituted 157 (32.4%), borderline epithelial 89 (18.3%), benign epithelial 125 (25.8%) followed by sex cord-stromal 32 (6.6%), germ cell tumours 31 (6.4%), other benign tumours 51 (10.5%), other malignant cases 3 (0.6%), and metastasis 8 (1.6%).
Frozen and final
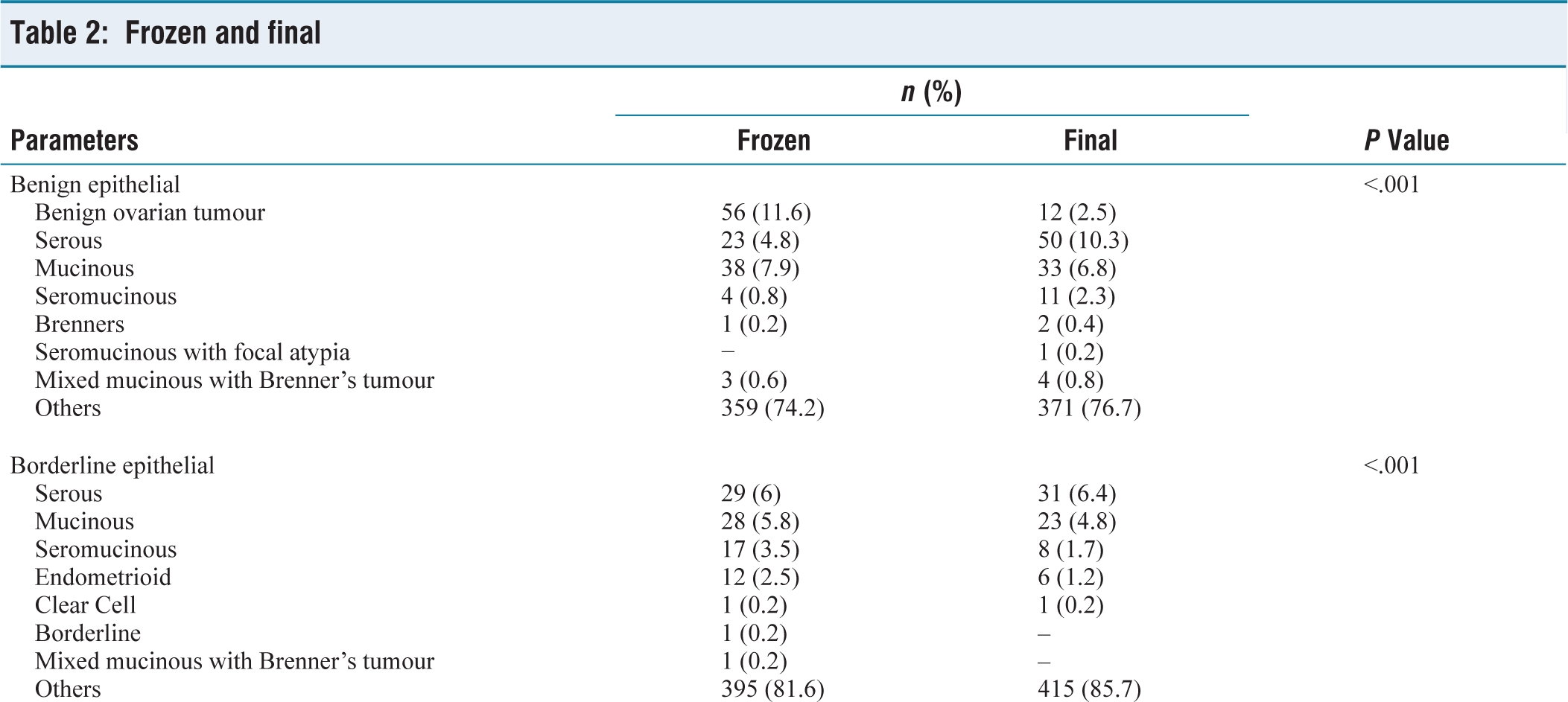

In the permanent sections, 169/484 (35%) cases had malignant epithelial tumours, with the highest tumour type being high-grade serous carcinoma. All tumour categories have at least one discordant case, except in other malignant cases; two leiomyosarcomas and one myeloid sarcoma remained the same. The majority of discordant cases were in benign epithelial and borderline epithelial tumour types.
Table 3 shows the positive predictive value (PPV), negative predictive value (NPV), sensitivity, and specificity values of epithelial tumours of the ovary. In diagnosing malignant epithelial tumours, the IFS had a sensitivity and specificity of 87% and 96.8%, whereas in borderline tumours, it is 91.3% and 93.7%. IFS has a sensitivity of 91.2% and a specificity of 94.1% in diagnosing benign epithelial tumours.
Diagnostic value of frozen section diagnosis of epithelial tumours according to malignancy status in terms of sensitivity, specificity, PPV and NPV

Of 484 cases, 471 (97.3%) were concordant and 13 (2.7%) were discordant. In 13 discordant cases, 4/13 cases were over-diagnosed in the FS and underwent extensive surgery. The remaining discordant cases did not receive undertreatment or overtreatment.
Discussion
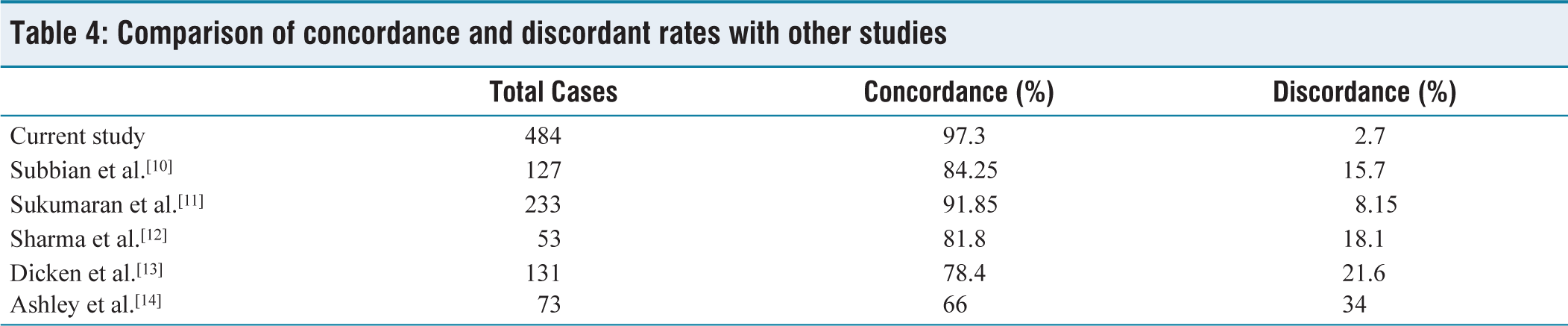
Our study analysed 484 cases of ovarian lesions, including primary ovarian neoplasms, metastatic tumours and non-neoplastic lesions. The results showed that primary ovarian tumours and ovarian metastasis from other sites can be misinterpreted during IFS diagnosis. The overall concordance rate of IFS diagnosis was 471 (97.3%). The IFS diagnosis has a high sensitivity for borderline epithelial tumours and a high specificity for malignant epithelial tumours. There were no false-positive malignant cases in this study. A relatively high incidence was noted in serous tumours, especially high-grade serous tumours. The discordance rate was high in interpreting mucinous and seromucinous neoplasms. The concordance and discordance of this study and other studies are shown in Table 4.
Comparison of concordance and discordant rates with other studies
Other studies show that ovarian metastasis of colorectal cancer mimics primary endometrioid carcinoma.[4] In these situations, squamous differentiation favours endometrioid carcinoma and the presence of goblet cells and intraluminal dirty necrosis favours colorectal cancer.[4] Shih et al. study states that to note micropapillary features in a serous borderline tumour, which has a high chance of getting reclassified as invasive cancer in permanent sections.[5] Also, discordance in endometrioid and intestinal mucinous tumours occurs due to sampling errors. These tumours often present as large masses with small invasive foci in a background of predominantly borderline tumours.[5]
Yoshita et al. study had a concordance rate of 93.8%, underdiagnosed and overdiagnosed cases represented 47 and 3 cases out of 802 cases.[4] In their study, diagnostic sensitivity was highest for benign (99.6%) and lowest for borderline (85.6%) epithelial tumours, but in our study, it was highest for both benign and borderline tumours. The PPV for borderline tumours was 79%, which is similar to our analysis (70.8%). The discordance rate was higher in the borderline epithelial tumour category, which was either called carcinoma or benign cystadenoma. Both cases resulted in under-treatment and over-treatment of the patients. A study by Decker et al. suggested a full surgical staging at initial surgery itself for a borderline serous tumour, as it has a high rate of upgradation into carcinoma during permanent sections.[6]
As per Madhusmitha et al.’s study, the factors that affect the FSs are sampling errors, technical errors, and interpretation errors.[7] The term ‘at least borderline’ can be used as a reasonable FS opinion, which indicates that the final diagnosis may change, but the surgeon can proceed with the staging laparotomy.[7] The incidence of over-diagnosis is rare, with some examples showing tangential cutting leading to a false impression of invasion.[7] Most of the discordant cases in our study were under-treated, and three cases were over-treated. According to the Kennedy et al. study, the rate of over-treated patients was 5.9%, who were exposed to surgical risk and related medicolegal issues.[2] The under-treated patients will have treatment failure and need subsequent corrective measures like chemotherapy or a second surgery. Morton et al. suggested that additional tests, such as diffusion-weighted MRI, may be helpful if a borderline tumour is suspected.[8]
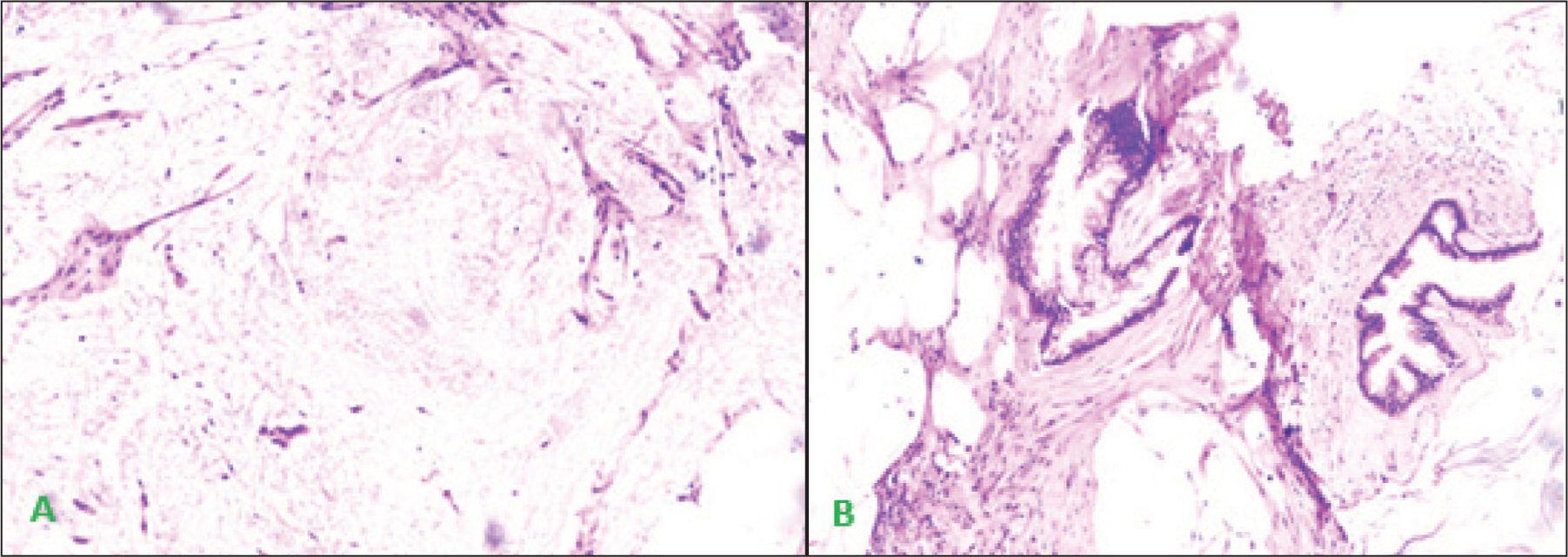
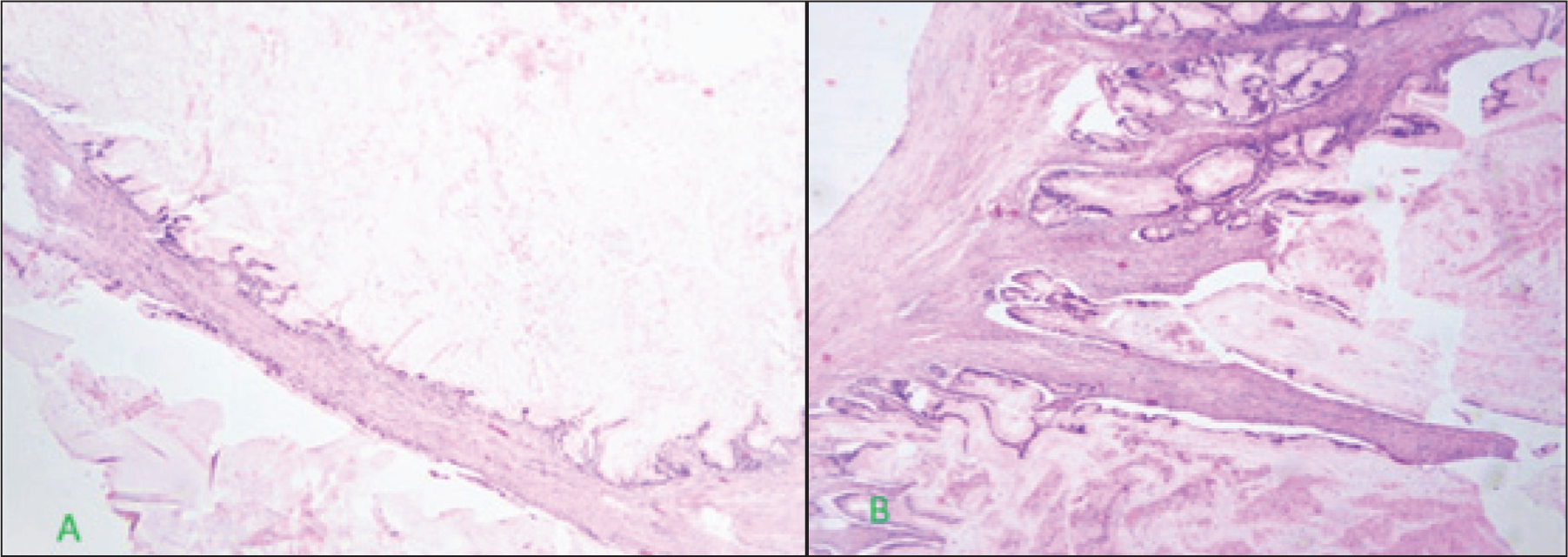
For metastatic carcinomas to the ovaries, gynaecological staging surgery is unnecessary.[9] In this study, the most common metastatic tumour was adenocarcinoma from the gastrointestinal tract primary. Microscopic findings like tubular and cystic glands may raise suspicion for endometrioid carcinoma and Sertoli Leydig cell tumours. However, the presence of signet ring cells, single cell infiltration, bilaterality, and intraoperative discussion with the surgeon about any peritoneal nodules or other lesions will be able to differentiate metastasis from primary ovarian tumours. The other diagnostic challenge is to differentiate primary mucinous neoplasm from metastatic mucinous adenocarcinoma and LAMN. Morphologically, LAMN presents like a mucinous cystadenoma and a mucinous borderline tumour. Ovarian metastasis of LAMN does not exhibit the usual features of metastasis, like bilaterality and multi-nodularity, causing frequent misinterpretation.[4] Without the evaluation of the appendix, it is impossible to differentiate it from primary ovarian origin. Figures 3 and 4 show FSs and permanent sections of a mucinous neoplasm of the ovary.
Sections from ovarian mass, (A) Mucinous neoplasm on frozen section. (B) The diagnosis on permanent sections was pseudomyxoma peritonei
(A) Borderline mucinous neoplasm on frozen section of ovarian mass. (B) Permanent section shows expansile growth suggestive of mucinous adenocarcinoma of ovary
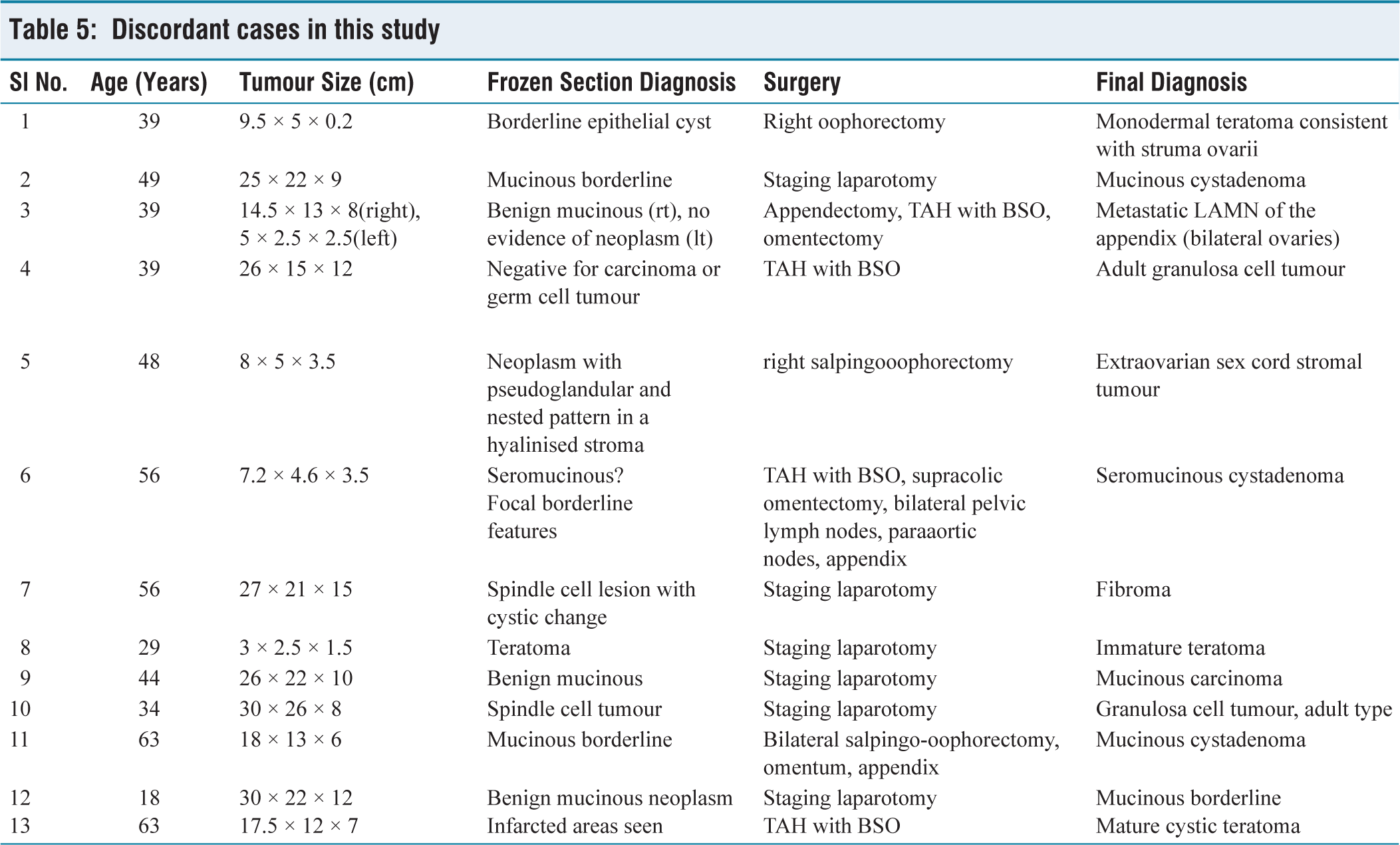
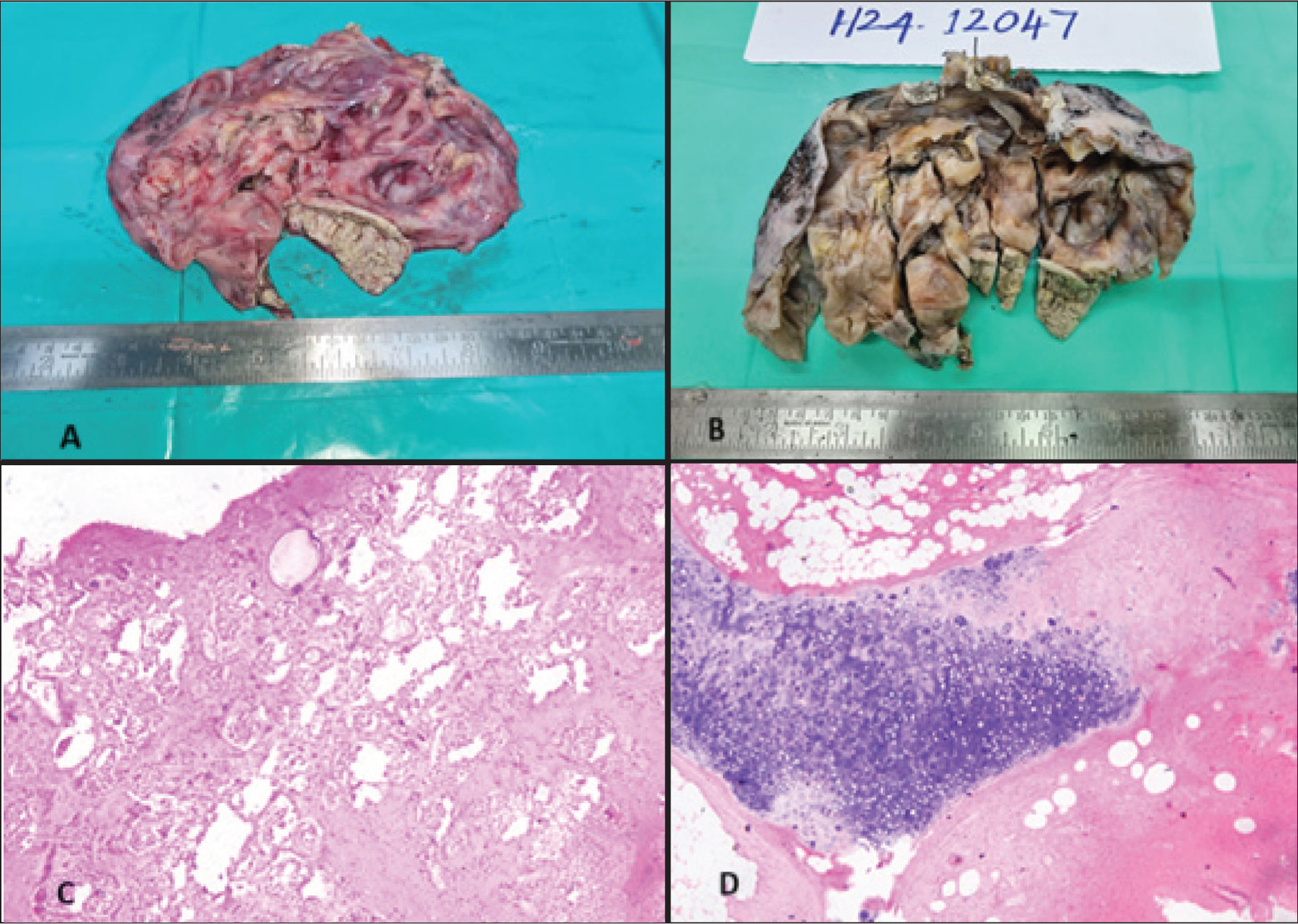
Irrespective of the tumour affecting the FS diagnosis, frozen artefacts, necrosis and haemorrhage may cause difficulty in interpretation, thereby deciding the surgical treatment. Table 5 shows the discordant cases in this study. Arshad et al. study shows that in cases of teratoma, torsion-related changes will mask the foci of immature components, which will be seen in extensive sampling during permanent sections.[15] Figure 5 shows the gross and microscopic features of mature teratoma.
The limitation of the study is that, because of its retrospective nature, the possible communication errors that occurred between the pathologist and surgeons during surgery were not available. The study has cases diagnosed based on the latest WHO classification of ovarian tumours in 2020 and the previous WHO classification of ovarian tumours in 2014. Despite these limitations, our study was able to demonstrate high concordance in reporting FS and to discuss possible errors in discordant cases.
Discordant cases in this study
(A & B) Gross appearance of a case of mature teratoma of the ovary in the frozen section (A) and permanent section (B). (C & D) The microscopic views of frozen section sampling (C) and permanent sections (D) of mature teratoma of the ovary
Conclusion
The FS diagnosis is a reliable method for intraoperative diagnosis of ovarian neoplasms. It helped to decide the need for extensive surgeries, especially in reproductive-age women. Intraoperative diagnosis was able to minimise undertreated and overtreated cases. The detailed evaluation of the patient’s clinical history, imaging findings, and active intraoperative consultation with the surgeon will help in reducing the rate of discordance.
Footnotes
Acknowledgements
To all technicians and non-technical staff in the Histopathology Department, Dr Shivashankari (research assistant) and Mr Logesh (Biostatistician, Research Department).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
AMH-C-S-086/10–23: Institutional ethical committee approval has been obtained on 26th October 2023. Approval for publication (AMH-C-S-048/04–25) obtained on 29th April 2025.
Informed consent
Informed consent has been obtained from all the patients who met the eligibility criteria.
Credit author statement
CR participated in data acquisition, literature search, investigations, data analysis, and manuscript preparation.
SLN participated in conceptualisation, investigation, supervision, data analysis, and manuscript editing.
All the authors have reviewed and approved the manuscript.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author upon request.
Use of artificial intelligence
No use of artificial intelligence.