
Abstract
Background:
Acne vulgaris, a prevalent dermatological condition, affects adolescents and adults, leading to physical and psychological burdens. Isotretinoin, a potent oral retinoid, has revolutionised the treatment of severe acne but is associated with adverse effects, such as hepatotoxicity, hyperlipidaemia, and teratogenicity, necessitating cautious use.
Objectives:
This study evaluates isotretinoin’s therapeutic efficacy, safety profile, and impact on the quality of life (QoL) in patients with moderate to severe acne vulgaris. The primary objectives are to analyse drug utilisation patterns and assess QoL changes using the Cardiff Acne Disability Index (CADI).
Methods:
A prospective follow-up study was conducted on patients with moderate to severe acne attending a tertiary hospital. Data on demographics, prescriptions, lipid profiles, liver enzymes, and CADI scores were collected at baseline and after three months. Statistical analysis was performed using paired t-tests to assess changes.
Results:
Seventy patients participated, with a mean age of 20.63 ± 3.91 years. Isotretinoin (20 mg/day) was prescribed in 60% of cases. Significant increases in cholesterol (146.57–177.36 mg/dL, P < .05) and triglycerides (88.05–109.24 mg/dL, P < .05) were observed in the isotretinoin group, along with elevated liver enzymes. CADI scores improved significantly in this group (11.62–3.21, P < .001) compared to non-isotretinoin-treated patients.
Conclusions:
Isotretinoin effectively reduces acne severity and improves QoL but is associated with metabolic and hepatic side effects. Close monitoring of lipid and liver parameters is recommended. This study underscores isotretinoin’s efficacy while highlighting the need for safety vigilance in acne management.
Keywords
Introduction
Acne vulgaris is a widespread skin disorder seen in both teenagers and adults, marked by the presence of both inflammatory and non-inflammatory skin eruptions. It arises from a combination of factors, including increased sebum production, follicular hyperkeratinisation, Cutibacterium acnes colonisation, and inflammation. While the condition is typically self-limiting, it often results in psychological distress and scarring, prompting individuals to seek medical treatment. A variety of treatment modalities are available, including topical therapies (benzoyl peroxide, retinoids, and antibiotics) and systemic agents (oral antibiotics, hormonal therapies, and retinoids). Among these, oral retinoids, particularly osotretinoin, represent one of the most potent and effective treatment options for severe or recalcitrant acne. However, despite their efficacy, oral retinoids are not without risks, making their use a double-edged sword in acne management.
Oral retinoids, particularly isotretinoin, have significantly transformed the management of severe acne vulgaris. They work by decreasing sebum production, regulating follicular keratinisation, and providing anti-inflammatory effects, which collectively result in notable improvement of acne symptoms. Studies have consistently shown that isotretinoin leads to long-term remission in many patients, making it the treatment of choice for nodulocystic and scarring acne.[1]
However, oral retinoids are associated with a wide spectrum of adverse effects that can limit their utility. These range from mucocutaneous side effects, such as dryness of the skin and lips, to more serious systemic effects, including hepatotoxicity, hyperlipidaemia, and teratogenicity.[2] In our study, we have focused on potential hepatotoxicity and lipid abnormalities due to the use of isotretinoin.
The teratogenic potential of oral retinoids, particularly isotretinoin, is perhaps the most well-known and serious adverse effect, necessitating strict pregnancy prevention programs for women of childbearing age. The risk of severe foetal malformations mandates the use of effective contraception during treatment and for a period after discontinuation.[3] Additionally, isotretinoin has been linked to psychiatric disturbances, including depression and suicidal ideation, although the relationship remains controversial. The psychological effects of acne itself, particularly in adolescents, may confound the interpretation of these psychiatric events.[4]
Given the efficacy and risks associated with oral retinoids, the decision to initiate treatment requires careful patient selection and monitoring. Current guidelines recommend reserving oral retinoids for patients with severe, treatment-resistant acne, particularly when other systemic agents have failed or are contraindicated.[5] The aim of this study protocol is to evaluate the current patterns of drug use in acne vulgaris with a particular focus on oral retinoids, exploring both their benefits and potential risks in real-world clinical practice. The research will involve a review of patients treated with oral retinoids for acne vulgaris, assessing treatment outcomes, adverse effects, and adherence to safety protocols.
Understanding the risk-benefit profile of oral retinoids in acne management is critical to optimising patient outcomes while minimising harm. This study will contribute to the growing body of evidence on the safe and effective use of these agents, ultimately informing clinical practice in dermatology and pharmacology.
This research aims to investigate the effectiveness and safety of retinoid therapy in patients prescribed the treatment by their physician, with a focus on patients’ QoL. Our Objectives were to evaluate drug use in acne, with a focus on retinoids, and to evaluate QoL in such patients before and during treatment using the Cardiff Acne Disability Index (CADI).
Methodology
This study was a prospective follow-up study conducted to assess the efficacy, drugs used in treatment, and impact on the quality of life (QoL) of patients with moderate to severe acne vulgaris receiving treatment. The sample size is duration-based, including all eligible patients presenting to the dermatology outpatient department of a tertiary care hospital during the study period.
Individuals diagnosed with moderate to severe acne vulgaris, as determined by their physicians using the Global Acne Grading System, were selected for inclusion in the study. Following Institutional Review Board approval, eligible patients were enrolled after obtaining written informed consent in their preferred language.
Demographic data, clinical history, and prescription details, including drug type, dose, frequency, and duration, were recorded using a structured case record form. Baseline laboratory investigations, including lipid profiles and liver function tests, were conducted at enrolment (day 0) and repeated at three months to assess any treatment-related changes. The QoL of participants was measured using the CADI at baseline and three months. The higher the score, the more impaired the QoL.
Statistical analysis was performed using SPSS version 26 software, with paired t-tests applied to evaluate changes in laboratory parameters and QoL scores over the study period.
Ethical considerations include ensuring patient data confidentiality through anonymisation and securing informed consent before participation.
Results
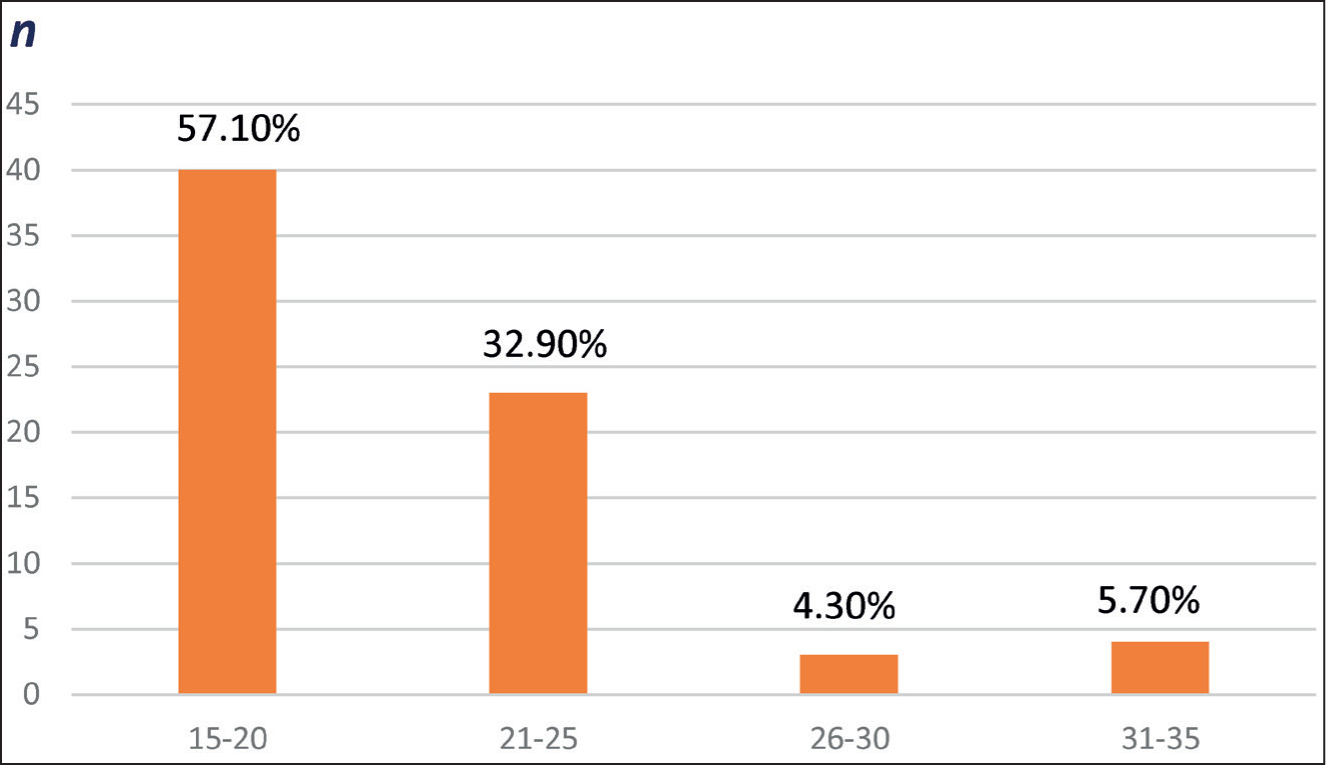
A total of 70 patients participated in the study. The average age of the patients was 20.63 ± 3.91 years, with the male-female ratio being 0.59:1, indicating a preponderance of acne vulgaris among females.
Out of 70 patients, 40 patients belong to the 15–20 years age group. Age distribution is shown in Figure 1.
Grading
All patients were diagnosed with acne vulgaris, with severity categorised as moderate, severe, or very severe, out of which 33 (47.1%) patients had moderate, 32 (45.7%) patients had severe, and 5 (7.1%) patients had very severe acne.
Drug Use Pattern
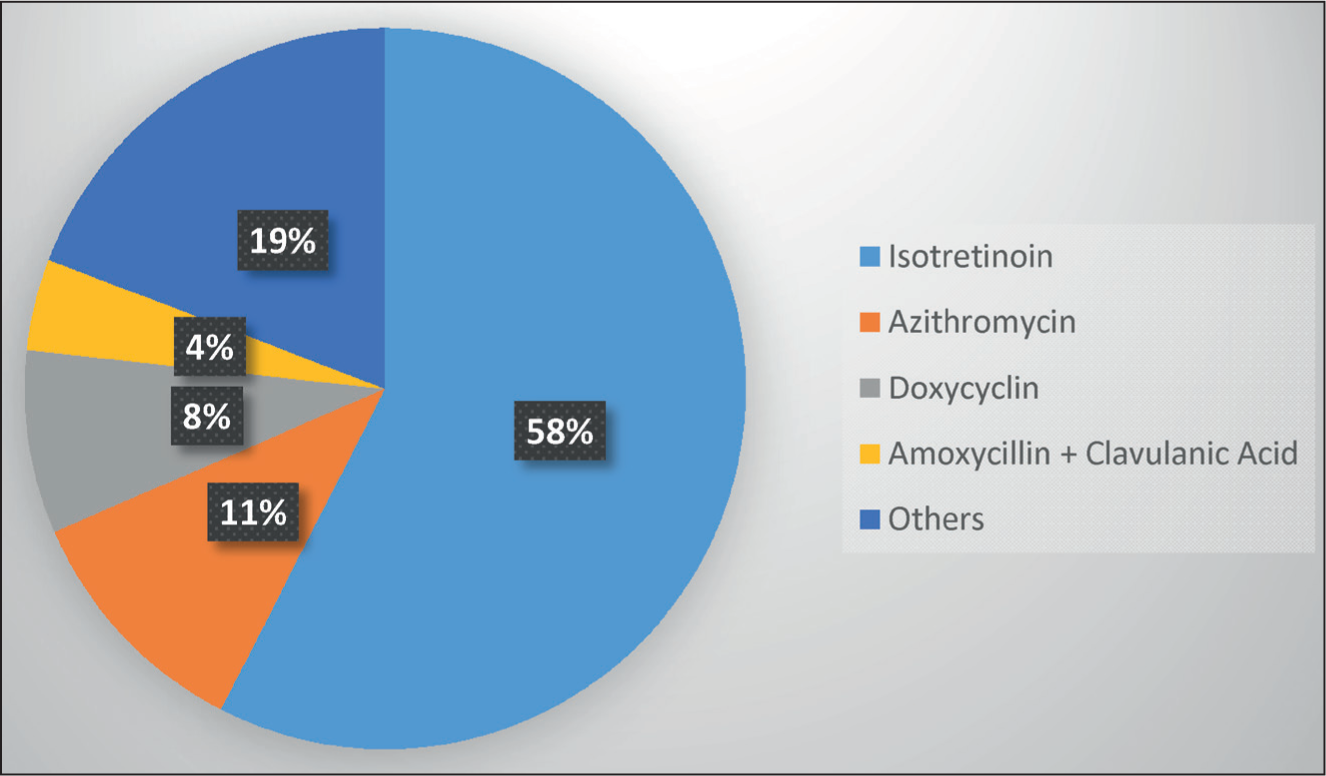
A total of 250 drugs were prescribed to 70 patients over 12 weeks, out of which 72 (28.8%) were prescribed systemically and 178 (71.2%) were prescribed for topical application. The number of drugs received by each patient was 3.57. Isotretinoin followed by azithromycin was the most prescribed systemic oral medication, whereas Nadifloxacin 1% w/w followed by the adapalene plus benzoyl peroxide combination was the most prescribed topical medication. Most patients received oral isotretinoin 20 mg/day for three months. These findings are shown in Figures 2 and 3 below.
Age distribution
Drugs prescribed orally (n = 42)
Drugs prescribed topically for local application (n = 28)

Lipid profiles and liver function tests (including Alanine Aminotransferase [ALT] and Aspartate Aminotransferase [AST]) were obtained at baseline (day 0) and again at the three-month follow-up in both groups, which are shown in Tables 1 and 2.
Changes seen on lipid profile and liver functions in isotretinoin receiving patients (n = 42, P value < .05 is significant, value with * is statistically significant)

Changes seen on lipid profile and liver functions in patients not receiving isotretinoin (n = 28, P value < .05 is significant, value with * is statistically significant)

In the group receiving isotretinoin, significant changes were observed in lipid parameters and liver enzymes. Serum cholesterol increased from a baseline of 146.57 to 177.36 mg/dL (P < .05). Similarly, triglycerides rose from 88.05 to 109.24 mg/dL (P < .05), while Low-Density Lipoprotein (LDL) levels increased from 91.14 to 107.93 mg/dL (P < .05). Serum Glutamic-Pyruvic Transaminase (SGPT) and Serum Glutamic-Oxaloacetic Transaminase (SGOT) levels also showed significant increases, with SGPT rising from 25.55 to 32.52 U/L (P < .05) and SGOT increasing from 24.40 to 32.74 U/L (P < .05). High-Density Lipoprotein (HDL) levels, however, showed a minor reduction from 44.50 to 43.76 mg/dL (P > .05) which is not significant.
In the group not receiving isotretinoin, similar parameters exhibited less pronounced changes. Serum cholesterol increased modestly from 143.96 to 151.04 mg/dL (P < .05), while triglycerides rose from 93.46 to 100.54 mg/dL (P < .05). Unlike the isotretinoin group, LDL levels slightly decreased (87.00 to 85.50 mg/dL, P > .05), and HDL levels showed a minor increase (44.32 to 45.04 mg/dL, P > .05). Liver enzyme levels also increased, but to a lesser extent compared to the isotretinoin group.
These findings indicate that isotretinoin use in acne treatment is associated with significant increases in lipid levels and liver enzymes, suggesting potential metabolic and hepatic side effects. In contrast, the non-isotretinoin group exhibited milder alterations, highlighting the need for close monitoring of lipid profiles and liver function in patients undergoing isotretinoin therapy.
The CADI was used to assess the QoL of the patients at baseline (day 0) and at the three-month follow-up. The results of the CADI scores are presented in Table 3.
Comparison of CADI scores in both groups, baseline and after three months of treatment (P > .05 is significant)

The CADI scores presented in the table assess the QoL of patients, with higher scores indicating a greater impairment in QoL due to acne. The table compares patients treated with isotretinoin to those not treated with isotretinoin over a three-month follow-up period.
At baseline (day 0), patients in the isotretinoin group had a higher mean CADI score (11.62 ± 2.17) compared to the non-isotretinoin group (9.11 ± 2.53), indicating that those prescribed isotretinoin experienced a greater initial impact of acne on their QoL. After three months of treatment, the mean CADI score in the isotretinoin group decreased significantly to 3.21 ± 1.80, showing a marked improvement in QoL. Conversely, the non-isotretinoin group also showed improvement, but their CADI score decreased to 4.29 ± 2.24, reflecting a less pronounced improvement.
An unpaired t-test was conducted to compare the change in QoL scores between patients treated with isotretinoin and those receiving other treatments. The results indicated a statistically significant improvement in the QoL in the isotretinoin group compared to the other group (t (68) = 6.089, P < .001).
The results suggest that isotretinoin is more effective in reducing the negative impact of acne on QoL over the short study period compared to other treatments. The greater reduction in CADI scores among isotretinoin users highlights its potential for significantly improving the psychological and social burden of acne. This outcome reinforces isotretinoin’s effectiveness, particularly for patients with more severe initial impairment.
Discussion
This study is a prospective follow-up study to evaluate the use of isotretinoin in patients with acne vulgaris. The authors have previously conducted studies on drug utilisation for acne vulgaris and the impact of the disease on QoL. However, those studies did not focus on isotretinoin and its effect on lipid profile and liver enzymes.[6]
The use of oral retinoids, particularly isotretinoin, has marked a paradigm shift in the treatment of acne vulgaris, especially in severe or treatment-resistant cases. By targeting multiple pathogenic factors, including sebaceous gland hyperactivity, hyperkeratinization, and inflammation, oral retinoids provide a comprehensive solution for patients whose conditions do not respond to conventional therapies. Their efficacy often translates to significant clinical improvement and, in many cases, long-term remission, elevating them to a gold standard in dermatological care for moderate to severe acne.
However, the benefits of these drugs are counterbalanced by their potential for significant side effects, making their use a nuanced decision requiring careful deliberation. Among patients receiving oral isotretinoin medication, serum lipid alterations are the most frequent laboratory abnormality.[7] Isotretinoin can potentially bind with certain active sites of proteins or enzymes involved in lipid metabolism, such as hydroxymethyl glutaryl reductase, a vital enzyme responsible for regulating cholesterol synthesis.
As it metabolises in the liver, it may lead to increased hepatic enzyme activity, resulting in elevated levels of liver enzymes, such as ALT, AST, and alkaline phosphatase. These changes are primarily due to oxidative stress and inflammation caused by the drug’s effects on hepatocytes.
Isotretinoin is well-absorbed orally, with its bioavailability enhanced by food. It binds extensively to plasma proteins (>99.9%), is metabolised in the liver by cytochrome P450 enzymes, and is eliminated equally in urine and faeces as conjugates. Its elimination half-life averages 20 hours, while the primary metabolite, 4-oxo-isotretinoin, has a half-life of approximately 25 hours.[8,10] Guidelines for isotretinoin usage suggest doses of 0.3–1.0 mg/kg/day, depending on the severity of acne and patient tolerability, with treatment courses lasting 16–24 weeks or until a cumulative dose of 120–150 mg/kg is reached. In our study, the prescribed dose of isotretinoin was 20 mg per day.
Importantly, the drug requires strict monitoring due to its teratogenic potential, mandating adherence to pregnancy prevention programs, such as iPLEDGE in the US. The iPLEDGE program in the United States is a risk management distribution program designed to prevent foetal exposure to isotretinoin. The drug is contraindicated in pregnancy due to its high teratogenic risk, linked to foetal loss and congenital malformations including craniofacial abnormalities (e.g., cleft palate), cardiovascular malformations, thymic defects, and central nervous system anomalies. Up to 20%–30% of exposed foetuses may develop congenital anomalies. It is also associated with spontaneous abortions and neurodevelopmental delays in some cases. In such cases, stringent contraceptive measures are required during therapy and up to one month post-treatment.[9,10]
In this study, isotretinoin was the most prescribed (in 60% of the patients) drug for acne, followed by azithromycin and doxycycline. A similar kind of study was conducted in the past in our setup, where drug use patterns and analysis of QoL in patients were assessed, and, in that study, isotretinoin was the third most prescribed medicine following azithromycin and doxycycline.
In the isotretinoin group, significant changes were observed in lipid parameters and liver enzymes, with notable increases in serum cholesterol, triglycerides, LDL, and liver enzymes SGPT and SGOT. HDL levels decreased slightly. In contrast, the group of patients not receiving isotretinoin exhibited milder changes, including modest increases in cholesterol and triglycerides and a slight rise in HDL levels. These changes can be due to the use of other systemic antimicrobials as well. The overall effect on HDL was inconclusive.
The CADI revealed greater baseline QoL impairment in the isotretinoin group (11.62 vs. 9.11), but after three months, this group showed a more substantial improvement (CADI: 3.21 vs. 4.29), underscoring isotretinoin’s efficacy in enhancing QoL despite its metabolic side effects. Significant changes in cholesterol and triglyceride levels did not result in therapy cessation because they were within the normal laboratory range.
In a recent study in Iran by Nejad et al. a total of 65 patient records were evaluated, with an average age of 22.21 ± 6.25 years. The majority of patients (84.6%) were female, according to the results. The mean cholesterol levels at baseline and 120 days after starting isotretinoin treatment were 154.97 ± 26.67 and 167.57 ± 32.01 mg/dL, respectively. Serum cholesterol levels significantly increased as a result (P < .001). The serum triglyceride level, however, did not change significantly, according to the results (P = .259). HDL levels did not significantly change (P = .626), despite a considerable increase in LDL levels (P = .04).[11]
Patients taking 20 mg of isotretinoin daily showed no change in HDL and a marked increase in LDL levels, according to a study conducted in India in 2021 by Sarkar et al.[12]
On the other hand, a recent study conducted in Jordan by Khabour et al. revealed that following 40 mg/day of isotretinoin medication, HDL levels dramatically reduced (P = .05).[13] However, Kutlu et al. found a significant rise in both LDL and HDL[14] in 120 patients with severe or very severe acne vulgaris who had been treated with isotretinoin (0.5–1 mg/day) for at least three months. Individuals who received 40 mg/day of isotretinoin (the same dosage used in Khabour’s study) showed a little decrease in HDL levels in Zanganeh’s study conducted in Iran in 2021, but individuals who received 20 mg/day of isotretinoin showed no discernible change.[15]
The advantages of isotretinoin are particularly notable in cases of nodulocystic or scarring acne, where its ability to reduce sebaceous gland activity and regulate cell differentiation achieves results unmatched by other treatments. Clinical studies demonstrate a high success rate, with up to 80% of patients achieving complete or near-complete clearance of acne after a single course of therapy.[16] Nevertheless, the safety profile of oral retinoids remains a major consideration. Adverse effects, such as mucocutaneous dryness, teratogenicity, and psychiatric symptoms, including depression and suicidal ideation, have been well-documented.[17] Moreover, rare but serious side effects like hepatotoxicity and inflammatory bowel disease add to the complexity of their use.[18]
Hypertriglyceridemia is believed to occur, at least in part, due to the activation of Retinoid X Receptors (RXRs), which enhance the expression of apo C-III, a molecule known to inhibit the breakdown of plasma triglycerides.[19] The RXRs have been implicated in the development of metabolic syndrome and are thought to play a role in the onset of polycystic ovary syndrome.[20,21]
An 18-year-old girl with grade four nodulocystic acne developed pancreatitis after starting isotretinoin 20 mg, despite normal baseline investigations. While isotretinoin-induced hypertriglyceridemia is somewhat predictable, pancreatitis is rare unless triglyceride levels exceed 500 mg/dL. An increase in triglycerides poses a risk factor for acute pancreatitis, primarily in patients with pre-existing lipid abnormalities. Acute pancreatitis, often linked to hypertriglyceridemia or idiosyncratic reactions, has been documented in only a few cases, primarily in older patients or those with pre-existing lipid abnormalities.[22]
Overall, it is advisable that 20 mg isotretinoin for a short duration of treatment (12–16 weeks) can be administered with minimal concern regarding changes in serum transaminase and lipid levels, as the side effects are dose-related; however, although severe laboratory alterations were not noted in our study, routine monitoring of lipid profile is needed. At our setup, patients receiving isotretinoin therapy were undergoing regular follow-up and laboratory testing. We advise physicians to use caution when administering isotretinoin in patients with a history of abnormal findings.
The Strength of this Study
The strength of this study lies in its comprehensive evaluation of the effects of isotretinoin therapy on both physiological and QoL parameters in patients with acne. By assessing liver function and lipid profiles alongside QoL changes, the study provides a holistic view of isotretinoin’s impact, integrating objective biochemical markers with subjective patient-reported outcomes. The longitudinal design enables the tracking of changes over time, enhancing the reliability of findings. Furthermore, the inclusion of QoL measures highlights the importance of patient-centred outcomes, which are often underrepresented in similar studies. These multifaceted insights contribute to a more nuanced understanding of isotretinoin’s therapeutic and safety profile, aiding in better-informed clinical decision-making.
Limitations of this Study
This study’s limitations include a comparatively small sample size, which may restrict the applicability of the results to larger populations. Moreover, the three-month follow-up duration might be insufficient to assess the long-term impact of isotretinoin on liver function, lipid levels, and overall QoL. Factors, such as dietary habits, baseline metabolic conditions, and concurrent medication use, which could influence lipid and liver enzyme changes, were not controlled for.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
NHL Institutional Review Board (NHLIRB) approval was received from SMT NHL Municipal Medical College.
Sources of support
Nil.
Credit author statement
Concepts: K.D., M.A., S.M.
Design: K.D., M.A., S.M.
Definition of intellectual content: K.D., M.A., S.M.
Literature search: K.D., M.A.
Clinical studies: K.D., M.A.
Experimental studies: K.D., M.A.
Data acquisition: K.D., M.A., P.A.
Data analysis: K.D., M.A., P.A., S.M.
Statistical analysis: K.D., P.A., S.M.
Manuscript preparation: K.D., M.A., S.M.
Manuscript editing: K.D., M.A., P.A., R.C., K.B., S.M.
Manuscript review: R.C., K.B., S.M.
Guarantor: R.C., K.B., S.M.
Data availability
The data supporting the findings of this study are not publicly available due to [privacy/ethical/legal restrictions] but can be made available from the corresponding author upon reasonable request and subject to institutional approvals.
Use of artificial intelligence
The authors used ChatGPT (OpenAI, San Francisco, CA, USA; version accessed March 2025) for language editing of the manuscript draft. All content was reviewed and verified by the authors, who take full responsibility for the final version.