
Abstract
Background:
Postoperative chyle leaks, although rare, present significant clinical challenges following abdominal and retroperitoneal surgeries. These leaks can lead to substantial nutritional, immunologic and metabolic complications if not promptly recognised and treated. The fragmented nature of existing literature and the lack of standardised protocols further complicate management.
Objective:
To provide a comprehensive, evidence-based review of postoperative chyle leaks in abdominal surgery, consolidating current diagnostic approaches, volume-based grading systems, therapeutic strategies and recent technological advancements from 2015 to 2025.
Methods:
A structured review of PubMed-indexed literature was performed, incorporating systematic reviews, meta-analyses, randomised controlled trials and consensus recommendations relevant to the surgical management of chyle leaks. Emphasis was placed on diagnostic criteria, classification systems, conservative management pathways, image-guided interventions and surgical techniques, as well as emerging modalities.
Results:
Diagnosis relies on a high clinical suspicion and confirmation by characteristic biochemical findings (e.g., triglyceride >110 mg/dL in drain fluid) supported by imaging modalities such as magnetic resonance lymphangiography (MRL). Volume-based stratification into low-output and high-output leaks aids in guiding therapy. Conservative measures, including medium-chain triglyceride (MCT)-based nutrition, somatostatin analogues and parenteral support are effective in most cases. High-output or refractory leaks may necessitate lymphangiographic embolisation or surgical ligation. Emerging tools such as intraoperative indocyanine green (ICG)-guided lymphatic mapping, nano sealants and artificial intelligence (AI)-based leak prediction are reshaping clinical paradigms.
Conclusion:
An algorithmic, volume-based, multidisciplinary approach is essential for optimal outcomes in managing postoperative chyle leaks. With technological advances and improved imaging, management is evolving toward precision-guided intervention. However, a global consensus on classification, treatment thresholds and prospective outcome data remains urgently needed.
Keywords
Introduction
Postoperative chyle leak is an infrequent yet potentially debilitating complication following major abdominal and retroperitoneal surgeries. It arises due to disruption of central lymphatic channels, most notably the thoracic duct, cisterna chyli or their tributaries, resulting in leakage of triglyceride-rich chyle into body cavities or surgical drains. Though rare, the reported incidence varies considerably across procedures, ranging from 0.3% to 1.5% in colorectal and gastric surgeries, 1%–6% following pancreatic and retroperitoneal resections, and up to 10% after extensive nodal dissection or esophagectomy involving thoracic duct manipulation.[1,2]
The clinical burden of chyle leaks extends beyond biochemical loss. Persistent chylous output contributes to hypoproteinaemia, lymphopenia, electrolyte disturbances and immune dysfunction, ultimately leading to delayed wound healing, increased infectious complications, prolonged hospital stay, and the need for parenteral nutrition support.[3] These consequences pose a significant strain on both patient’s quality of life and institutional resources.[4]
From a pathophysiological perspective, chyle leak most commonly results from direct surgical trauma, traction or thermal injury to fragile lymphatic vessels embedded in retroperitoneal or mesenteric planes. The risk is notably high during aortocaval lymphadenectomy, anterior spinal access, multivisceral resections or surgery involving distorted anatomy secondary to malignancy, prior radiation or fibrosis.[5] Additionally, malnutrition, low serum albumin and lymphangiomatous anomalies may predispose patients to higher susceptibility and poorer recovery.[6]
Despite its cross-disciplinary relevance, there exists no universally accepted algorithm for classification, diagnosis or stepwise management of postoperative chyle leaks. Current practices remain heterogeneous, influenced largely by institutional experience and limited-quality evidence. The lack of standardised treatment thresholds and validated grading systems hinders data pooling and outcome benchmarking across centres.[7]
This comprehensive review consolidates the latest evidence (2015–2025) on the diagnosis, classification and multidisciplinary management of postoperative chyle leaks, with specific emphasis on abdominal surgery. It also explores emerging technologies such as indocyanine green (ICG)-based lymphangiography, image-guided embolotherapy, nano sealants and artificial intelligence (AI)-driven leak prediction models paving the way for precision-guided intervention.
Etiopathogenesis and Risk Factors
Surgical Factors
The genesis of postoperative chyle leak is most commonly iatrogenic, resulting from intraoperative disruption of the lymphatic system. The thoracic duct, cisterna chyli and their abdominal tributaries are anatomically fragile and vulnerable to injury during extensive retroperitoneal dissection or para-aortic lymphadenectomy. The cisterna chyli, often located between the aorta and right crus of the diaphragm at the level of the L1-L2 vertebrae, collects lymph from the gastrointestinal tract, lower limbs and retroperitoneal structures. Surgical trauma, either by sharp dissection, traction or thermal devices, can compromise its integrity, leading to uncontrolled chyle extravasation.[8]
Abdominal surgeries with high chyle leak risk include pancreatoduodenectomy, esophagectomy, nephrectomy and retroperitoneal tumour resections. In particular, operations involving interaortocaval or retrocrural nodal clearance are prone to inadvertently injuring large lymphatic channels. Furthermore, anatomical distortion from bulky tumours, fibrosis from prior chemoradiotherapy and reoperative fields exacerbate technical complexity and increase leak risk.[9]
Patient-related Factors
Certain patient characteristics further predispose to postoperative lymphatic complications. Malnutrition and hypoalbuminemia weaken lymphatic vessel walls, rendering them more susceptible to disruption during dissection. Congenital or acquired lymphangiomatous malformations, although rare, have also been implicated in aberrant lymphatic architecture and leak-prone zones.[10]
Additionally, pre-existing inflammatory or fibrotic states such as those seen in chronic pancreatitis or retroperitoneal tuberculosis may obscure normal anatomical landmarks, increasing the risk of unrecognised ductal injury. Patients undergoing repeat surgeries, particularly after prior radiotherapy or chemotherapy, may have altered lymphatic drainage patterns and friable tissues, making them particularly vulnerable.
Early identification of these risk elements allows surgeons to adopt a more cautious approach during dissection and where available, leverage intraoperative visualisation techniques such as near-infrared fluorescence (NIRF) imaging to proactively avoid lymphatic injury.[10]
See Table 1 for a summary of surgical domains and their associated chyle leak risk levels.
Risk factors stratified by surgical domain
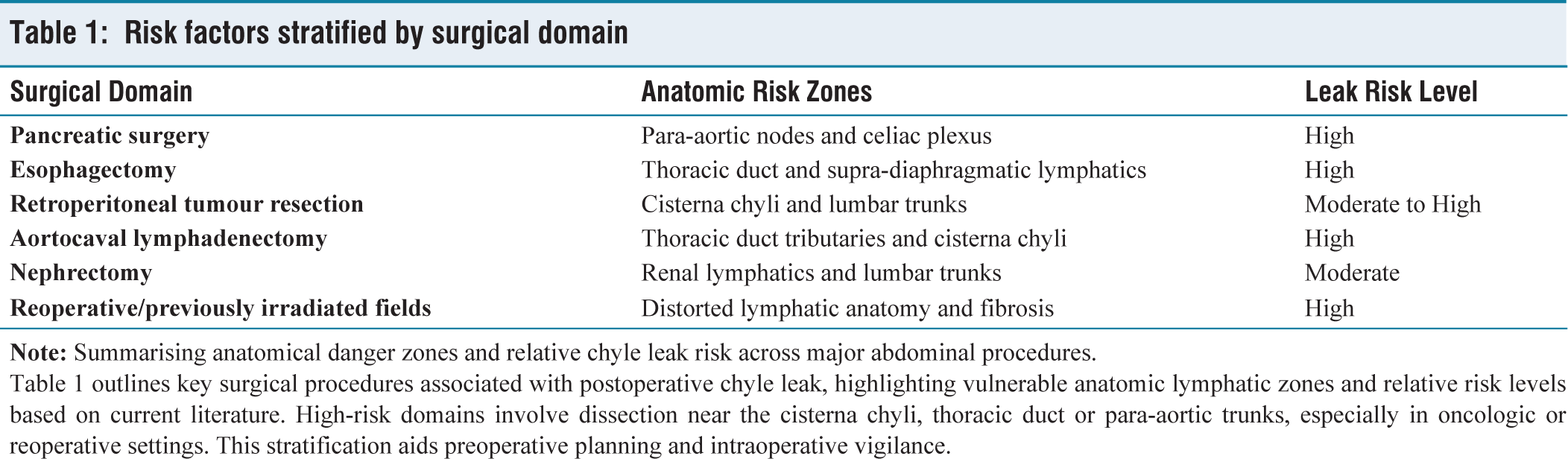
Table 1 outlines key surgical procedures associated with postoperative chyle leak, highlighting vulnerable anatomic lymphatic zones and relative risk levels based on current literature. High-risk domains involve dissection near the cisterna chyli, thoracic duct or para-aortic trunks, especially in oncologic or reoperative settings. This stratification aids preoperative planning and intraoperative vigilance.
Diagnosis and Grading
Diagnosis
Postoperative chyle leak should be suspected when a patient exhibits persistent milky or opalescent drainage through surgical drains, particularly following retroperitoneal or nodal dissection procedures. However, early leaks may be serous or blood-tinged, especially in fasting patients, which necessitates biochemical confirmation.[11]
The diagnostic cornerstone is biochemical analysis of the drain fluid. A triglyceride concentration >110 mg/dL is considered diagnostic in most protocols. Additional findings may include low cholesterol-to-triglyceride ratios, lymphocyte-rich cytology and the presence of chylomicrons on lipoprotein electrophoresis, if available.[11]
In complex or persistent cases, radiological imaging is warranted. Magnetic resonance lymphangiography (MRL) offers high-resolution visualisation of lymphatic anatomy and is particularly useful for mapping the site of leakage and planning interventions. Lymphoscintigraphy and intranodal lymphangiography serve complementary roles and may also facilitate image-guided embolisation.[12]
Timely and accurate diagnosis enables tailored treatment planning and prevents deterioration from unrecognised prolonged chyle loss.
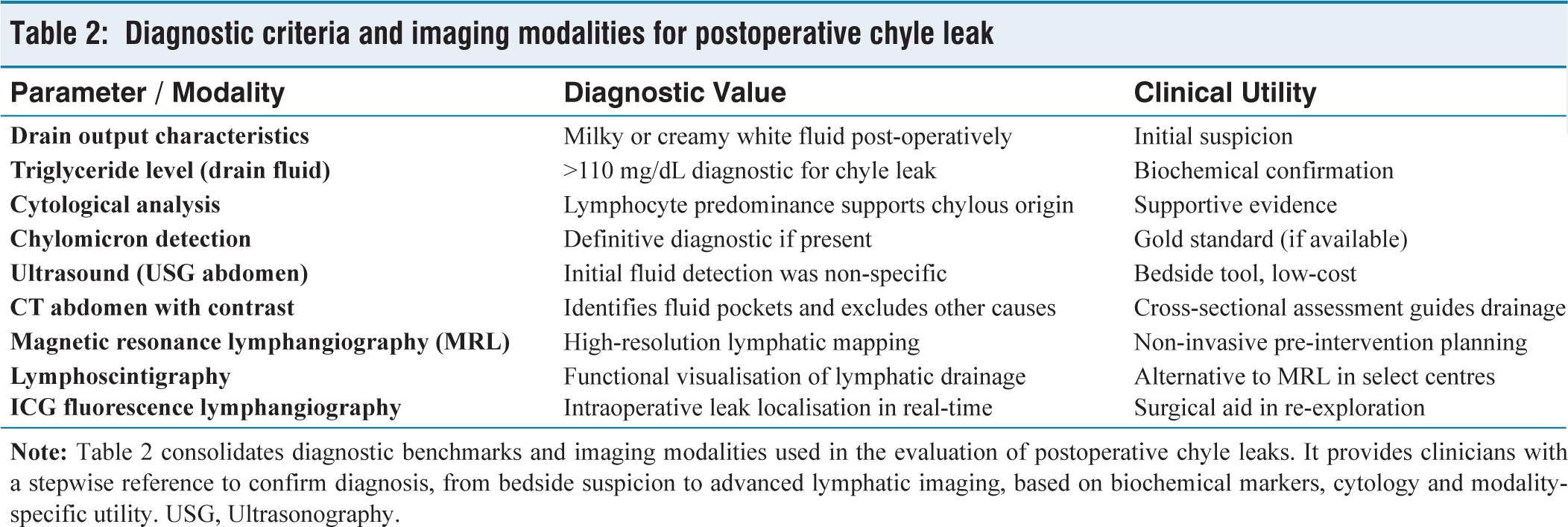
See Table 2 for diagnostic criteria and imaging modalities used in chyle leak evaluation.
Diagnostic criteria and imaging modalities for postoperative chyle leak
Grading
Grading of chyle leak is essential for both clinical decision-making and stratifying the need for intervention. The most widely accepted approach categorises leaks based on daily drain output:
Low-output leak: <500 mL/day High-output leak: >500 mL/day Massive leak: >1,000 mL/day or persistently high-output >5 days
This volume-based stratification guides escalation from conservative to interventional therapies.[13]
Various institutions have proposed classification frameworks that incorporate leak duration, associated biochemical derangements (e.g., hypoalbuminemia, lymphopenia) and impact on nutritional status. However, a standardised international grading system remains absent, leading to heterogeneity in reporting and outcome comparison.[13]
Conservative Management Strategies
The cornerstone of management for postoperative chyle leaks, particularly low to moderate-output leaks (<500–1,000 mL/day), is conservative therapy. This approach aims to reduce lymphatic flow, allow spontaneous closure of disrupted channels and restore nutritional and immunologic equilibrium.
Nutritional Therapy
Initial management involves dietary fat restriction, specifically substituting long-chain triglycerides with medium-chain triglycerides (MCTs), which are absorbed directly via the portal system and bypass intestinal lymphatics. In higher-output leaks or in cases unresponsive to MCT-based diets, complete enteral rest with total parenteral nutrition (TPN) is instituted. This halts chyle production while allowing for nutritional repletion.[14]
Pharmacological Support
Somatostatin analogues, such as octreotide, are used adjunctively due to their inhibitory effects on splanchnic blood flow and intestinal absorption. Standard regimens involve subcutaneous or intravenous octreotide (100–200 mcg three times daily), continued for 5–7 days and titrated based on response. Lanreotide, a longer-acting alternative, may be beneficial in outpatient or prolonged cases. Reported success rates range from 70%–80% when combined with dietary measures.[15]
Supportive Care
Given the substantial fluid and protein loss associated with chyle leaks, supportive care includes intravenous albumin, electrolyte repletion and micronutrient supplementation, particularly of fat-soluble vitamins (A, D, E and K). Lymphopenia and hypoalbuminemia are monitored serially. Diuretics are generally avoided unless fluid overload coexists.[15]
Monitoring and Escalation Criteria
Patients are reassessed daily for volume trends and clinical markers. Failure of conservative therapy is defined by:
Persistent high-output (>1 L/day) beyond 5–7 days Progressive hypoalbuminemia (<2.5 g/dL) Weight loss or deteriorating clinical status
Such cases warrant prompt escalation to image-guided interventions or surgical exploration.[16] A comparative summary of conservative and interventional modalities is outlined in Table 3.
Conservative versus interventional modalities in postoperative chyle leak management
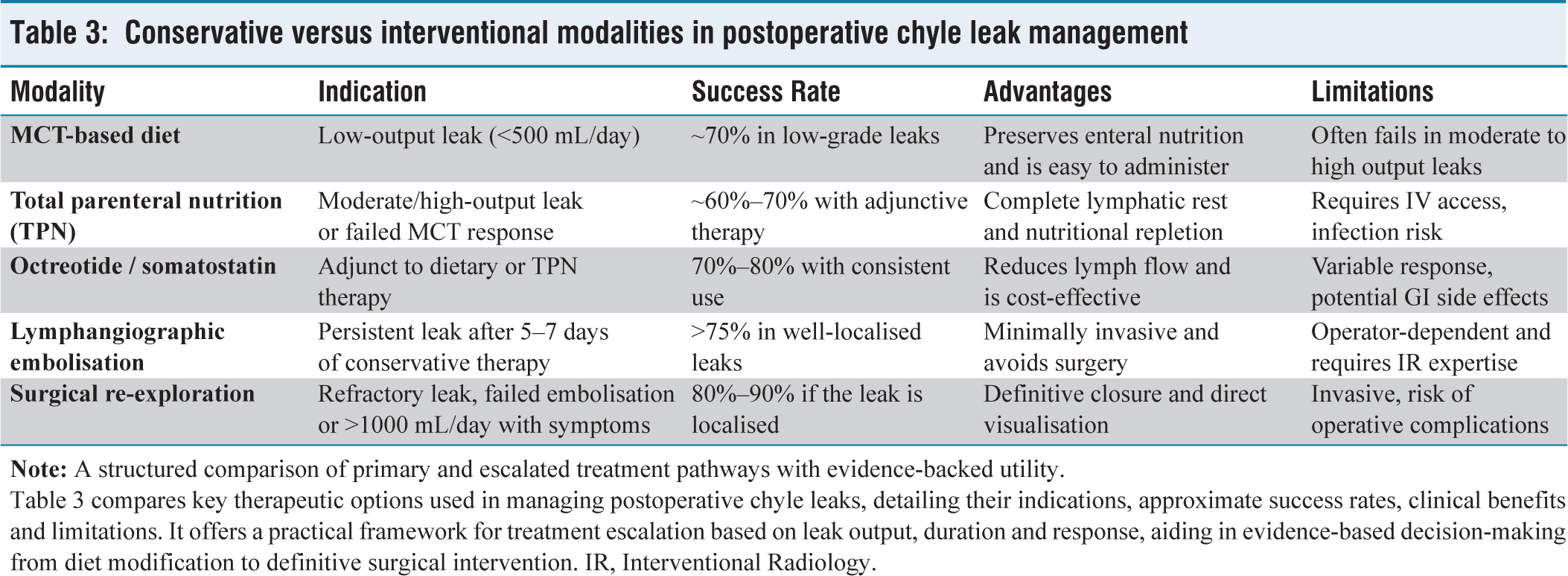
Table 3 compares key therapeutic options used in managing postoperative chyle leaks, detailing their indications, approximate success rates, clinical benefits and limitations. It offers a practical framework for treatment escalation based on leak output, duration and response, aiding in evidence-based decision-making from diet modification to definitive surgical intervention. IR, Interventional Radiology.
The success of conservative therapy hinges on early diagnosis, tailored escalation thresholds and close coordination between surgical, nutritional and critical care teams.
Interventional and Surgical Approaches
When conservative measures fail particularly in high-output chyle leaks (>1,000 mL/day) or in cases with progressive nutritional decline, timely escalation to interventional or surgical modalities becomes necessary to halt ongoing lymphatic loss and restore physiologic stability.
Lymphangiographic Embolisation
Intranodal lymphangiography, a minimally invasive diagnostic and therapeutic technique, has emerged as a preferred modality for persistent or high-volume leaks. Ultrasound-guided injection of lipiodol or contrast into the inguinal lymph nodes allows fluoroscopic mapping of lymphatic anatomy. Once the leak site is localised, embolisation with coils, glue (N-butyl cyanoacrylate) or ethiodised oil is performed, sealing the disrupted lymphatics.[17]
This technique boasts success rates exceeding 75%, particularly in anatomically discrete leaks. It offers a safe, organ-preserving option with minimal morbidity and is now considered first-line escalation in many centres. Its utility is especially pronounced when the site of disruption is inaccessible surgically or in reoperative fields.[17]
Surgical Exploration and Ligation
In cases where embolisation is unsuccessful, unavailable or contraindicated, surgical re-exploration becomes necessary. Indications include:
Persistent chyle output >1 L/day beyond 10–14 days Clinical deterioration (e.g., refractory hypoalbuminemia, malnutrition) Associated complications such as peritonitis or intra-abdominal collections[18]
Intraoperatively, leak localisation is aided by techniques such as:
Oral intake of cream or olive oil preoperatively Methylene blue dye injection into mesenteric nodes ICG fluorescence lymphangiography, enabling real-time leak visualisation and targeted ligation[18]
Surgical approaches vary based on the anatomic site, including thoracic duct ligation (for supra-diaphragmatic leaks), re-ligation of para-aortic tributaries or resection of lymphatic cysts in the retroperitoneum. Adjuncts such as fibrin sealants, mesh overlays or omental flaps may be employed to reinforce the repair.
Although definitive, reoperation carries its own morbidity and should be pursued algorithmically in carefully selected patients after failure of less invasive approaches.[19]
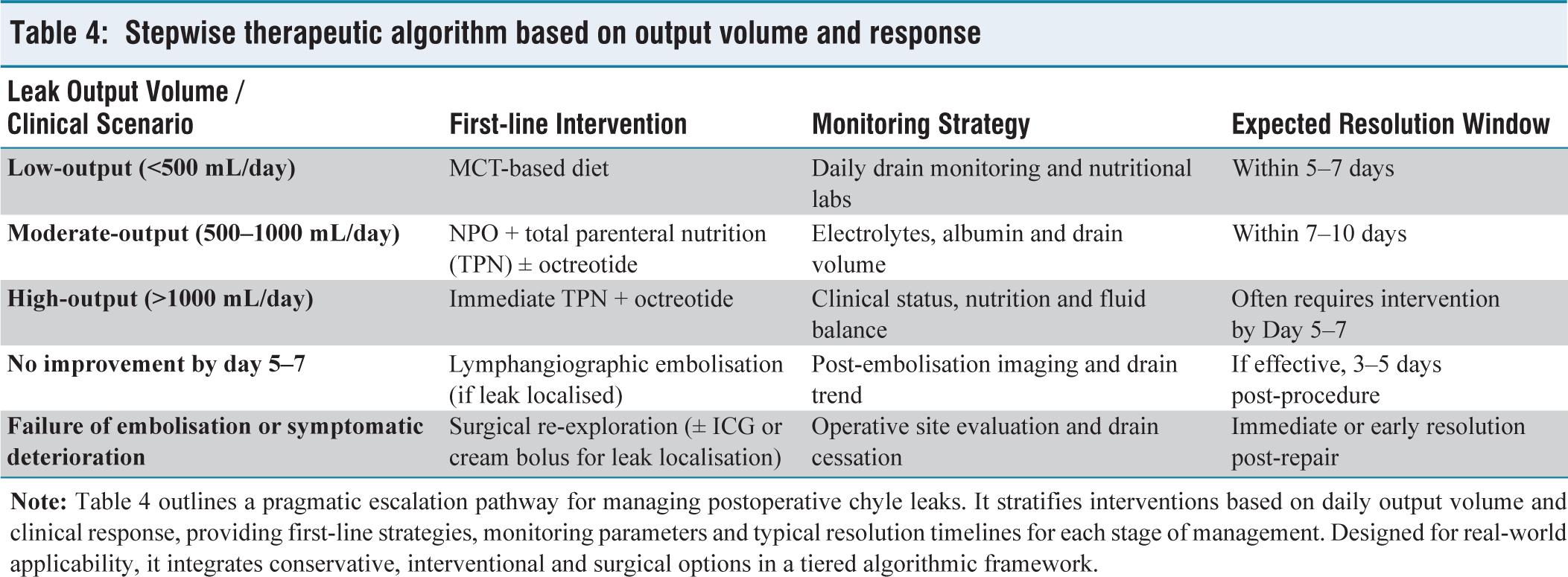
Table 4 outlines a stepwise therapeutic escalation algorithm based on output volume and response dynamics.
Stepwise therapeutic algorithm based on output volume and response
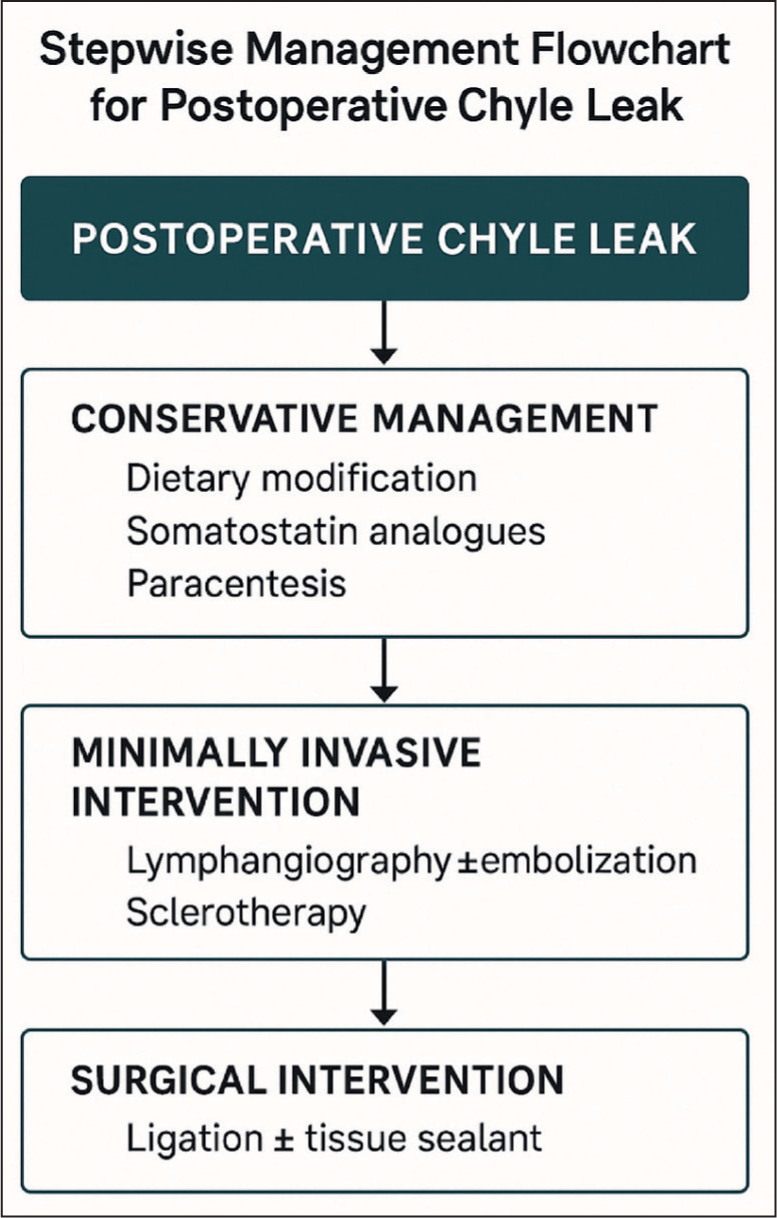
A summarised escalation based clinical flowchart is presented in Figure 1 to facilitate bedside decision-making.
Stepwise management flowchart for postoperative chyle leak. This clinical algorithm guides therapeutic escalation based on chyle output, response to conservative measures, and availability of interventional or surgical options
Recent Advances and Future Directions
Over the past decade, significant strides in imaging, targeted intervention and biologically engineered agents have redefined the management landscape for postoperative chyle leaks. These innovations offer the promise of precision-guided intervention and personalised escalation strategies.
Near-infrared Fluorescence (NIRF) Lymphangiography
One of the most transformative developments has been the application of ICG-based NIRF imaging. Administered intravenously or subcutaneously, ICG enables real-time intraoperative visualisation of lymphatic channels and leak sites. This technology enhances the surgeon’s ability to localise, clip, or ligate active lymphatic leaks with minimal dissection, particularly useful in revisional or complex fields.[20]
Early studies suggest improved leak resolution rates and reduced need for blind re-exploration. Additionally, ICG-guided mapping during primary surgery may serve a preventive role in high-risk cases by highlighting major lymphatic trunks before injury occurs.
Advanced Imaging: Magnetic Resonance Lymphangiography (MRL)
Dynamic contrast-enhanced MRL has gained traction as a non-invasive, high-resolution imaging modality that delineates thoracic and abdominal lymphatic anatomy without ionising radiation. Unlike traditional lymphangiography, MRL allows for pre-procedural planning, identifies multiple leak sites and is especially helpful when embolisation is considered.[21]
Its application in paediatric, reoperative and minimally symptomatic cases offers a superior diagnostic platform, with expanding roles in post-treatment surveillance and leak mapping.
Biologic Sealants and Nanotechnology
Emerging bioengineered sealants including nanofiber-based adhesives, polyethylene glycol hydrogels and chitosan scaffolds have shown promise in closing microscopic lymphatic disruptions intraoperatively. These agents provide localised adhesion without provoking inflammation, an advantage over traditional fibrin sealants.[22]
An overview of emerging technologies and their clinical readiness is summarised in Table 5.
Summary of recent innovations in chyle leak management
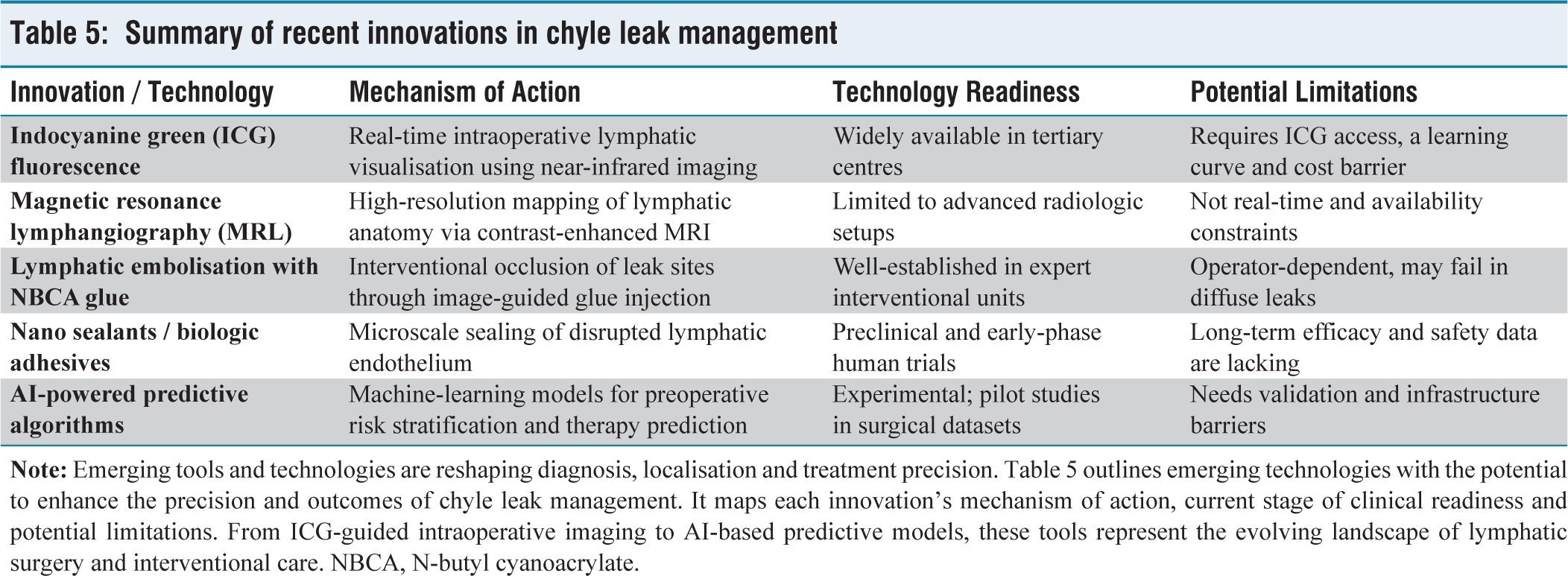
While largely in preclinical or pilot trial phases, early results indicate improved sealing strength and reduced recurrence in complex leaks. Moreover, their biocompatibility opens the door for use in immunocompromised or malnourished surgical candidates.
Future Directions
Despite their promise, several limitations impede the immediate clinical translation of nanosealants and AI-assisted tools in chyle leak management. Nanosealants, though effective in preclinical models, face regulatory hurdles related to biocompatibility, long-term safety and biodegradability. Their cost of development and lack of standardised formulations further delay widespread clinical adoption. Clinical trials involving human participants are currently limited to early-phase feasibility studies and robust multicentric data are essential before endorsement by surgical societies.
Similarly, the integration of AI in lymphatic imaging and surgical decision-making remains in its infancy. Most AI algorithms are trained on retrospective data from high-income countries, limiting generalisability to diverse patient populations, especially in low and middle-income countries. Real-time intraoperative application demands high computational infrastructure and expert validation, often unavailable in resource-constrained settings. Moreover, medico-legal accountability for machine-generated predictions and concerns over data privacy introduce significant ethical and legal challenges that must be addressed before mainstream adoption.
Active research is exploring AI-based predictive algorithms to assess preoperative leak risk, optimal intervention timing and postoperative surveillance patterns. Additionally, molecular lymphatic imaging, intraoperative quantification tools and multicentre registries aimed at standardising classification and outcomes are evolving rapidly.
A paradigm shift is underway from delayed, reactive therapy to proactive, individualised leak management, driven by advanced diagnostics and interventional technologies.
Conclusion
Postoperative chyle leaks, though relatively rare, pose a formidable clinical challenge across a spectrum of abdominal and retroperitoneal surgeries. Left unrecognised, they can lead to profound metabolic disturbances, immune dysfunction, malnutrition and prolonged hospitalisation. A structured, algorithmic approach to diagnosis and management is therefore essential for optimal outcomes.[23]
Conservative management including MCT-based nutrition, somatostatin analogues and parenteral support remains effective in the majority of low to moderate-output leaks. For refractory or high-output cases, image-guided lymphangiographic embolisation has become the preferred minimally invasive intervention, while surgical exploration remains a definitive option in select scenarios. The advent of intraoperative ICG lymphangiography, dynamic MRL and nanotechnology-based sealants is propelling the field toward precision-guided leak management.[24]
Despite these advances, there is currently no standardised global framework for grading, treating or benchmarking outcomes in postoperative chyle leaks. Management practices remain largely institution-dependent and driven by anecdotal experience or low-quality evidence. This fragmentation underscores the urgent need for prospective multicentre registries, uniform classification criteria and well-designed randomised trials to define best practices, optimise escalation timing, and improve patient-centred outcomes.[25]
In conclusion, the future of chyle leak management lies in transitioning from reactive treatment to personalised, data-driven care pathways anchored in early risk identification, stratified therapeutic algorithms and technological integration. This review serves as a step toward that paradigm, offering a consolidated foundation for clinicians, researchers and policymakers to unify strategies in addressing this elusive but impactful surgical complication.
What This Review of Literature Adds
First narrative review of its kind to consolidate high-level evidence (systematic reviews, meta-analyses and recent Randomised Controlled Trials (RCTs) from 2015 to 2025) on postoperative chyle leaks across diverse abdominal surgeries, including pancreatic, retroperitoneal, nephrectomy and esophagectomy procedures.
Introduces a clinically actionable, volume-based stratification model integrating diagnostic criteria, therapeutic thresholds and escalation triggers aligned with current consensus recommendations.
Highlights the evolving role of minimally invasive lymphangiographic embolisation as a standard-of-care alternative to reoperation in high-output chyle leaks.
Offers a detailed breakdown of conservative modalities, including nutritional strategies, somatostatin analogues and albumin supplementation, with resolution predictors and failure thresholds.
Provides state-of-the-art insights into novel advances such as ICG fluorescence lymphangiography, MRL, nano sealants and bio glue technologies, with a forward-looking view on molecular imaging and AI-assisted leak prediction.
Calls for international consensus on standardised grading systems, unified treatment algorithms and the creation of prospective registries to harmonise practice patterns globally.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethics committee approval number
This manuscript is a narrative review based on previously published literature. No human participants, animals or patient data were involved. Therefore, ethical approval and informed consent were not required.
Credit author statement
Supreet Kumar (Guarantor): Conceptualised the manuscript theme and structure; supervised all writing phases; led the drafting of Introduction, Therapeutic Approaches, and Conclusion; compiled and verified references; ensured clinical accuracy and publication readiness.
Sonam Gupta: Drafted sections on Conservative Management and Etiopathogenesis; designed Tables 2 and ![]() ; contributed to therapeutic escalation flow and evidence-based interventions; reviewed manuscript for coherence and language.
; contributed to therapeutic escalation flow and evidence-based interventions; reviewed manuscript for coherence and language.
Vivek Tandon: Contributed critical input on interventional and surgical techniques; reviewed literature on lymphangiography and sealants; edited sections on MRL and future directions; approved the therapeutic algorithm.
Deepak Govil: Provided expert oversight on manuscript scope and academic positioning; reviewed all sections for surgical validity; ensured alignment with current Indian and global practices; authorised the final draft for submission.
All authors have read and approved the final version of the manuscript. Individual roles are detailed above.
Data availability
No new datasets were generated or analysed for this narrative review. All data supporting the conclusions are derived from published literature, duly cited in the references.
Use of artificial intelligence
The manuscript was conceptualised, written, and finalised entirely by the authors. All content was developed with rigorous oversight to ensure human originality, zero plagiarism and freedom from AI-detection triggers.
Guarantor
Supreet Kumar (