
Abstract
Introduction:
The World Health Organisation (WHO) estimated the annual incidence of leptospirosis as 0.1–1 case per 100,000 population in temperate and non-endemic areas, while it is 10–100 cases per 100,000 population in humid, tropical and endemic areas. The clinical features may vary from asymptomatic to lethal disease and are based on the virulence of the infective serovar, infective dose, age, occupation and immunological status of the host. Laboratory diagnosis is pivotal because of the diverse clinical manifestations of the disease, which are mainly achieved by isolation of the organism by culture or by demonstration of a rise in specific serum antibody. This study aims to compare the performance of polymerase chain reaction (PCR) and Immunoglobulin M (IgM) enzyme-linked immunosorbent assay (ELISA) with the gold standard microscopic agglutination test (MAT) in diagnosing human leptospirosis.
Methodology:
The present cross-sectional study was conducted in the Department of Microbiology of a tertiary care centre for six months from July 2022 to December 2022 after collecting
100 serum samples from suspected leptospirosis patients.
Results:
Diagnosis of leptospirosis using PCR, MAT and IgM ELISA was 6%, 9% and 24%, respectively.
Conclusion:
Both ELISA and MAT can be done if a single sample is available. PCR can be used as a complementary test in the early phase of infection, especially when the antibody detection is negative.
Keywords
Introduction
The World Health Organisation (WHO) estimated the annual incidence of leptospirosis as 0.1–1 case per 100,000 population in temperate and non-endemic areas, while it is 10–100 cases per 100,000 population in humid, tropical and endemic areas.[1] The number of cases reported is approximately 300,000–500,000 cases worldwide every year, with a case fatality rate of 30%.[2] The prevalence of leptospirosis in Tamil Nadu, India, is 45%.[3] Outbreaks often occur during heavy rainfall and flooding during the monsoon.[4] The clinical features may vary from asymptomatic to lethal disease, which is based on the virulence of the infective serovar, infective dose, age, occupation and immunological status of the host.[5] Laboratory diagnosis is pivotal because of the diverse clinical manifestations of the disease, which are mainly achieved by isolation of the organism by culture or by demonstration of a rise in specific serum antibody. Culture is of undoubted epidemiological importance and takes a long time, allowing only a retrospective diagnosis. The serovar-specific microscopic agglutination test (MAT), a gold standard special test still a standard reference test, is not performed routinely in all diagnostic laboratories.[6] The rapid immunochromatography test and enzyme-linked immunosorbent assay (ELISA), which detect Immunoglobulin M (IgM) antibody, have been used for the diagnosis in most of the laboratories. This study aims to compare the performance of polymerase chain reaction (PCR) and IgM ELISA with the gold standard MAT in diagnosing human leptospirosis.
Material and Methods
The present cross-sectional study was conducted in the Department of Microbiology of a tertiary care centre for a period of six months from July 2022 to December 2022 after obtaining permission from the Institutional Ethics Committee (Tirunelveli Medical College Institutional Research Ethics Committee [TIREC] Reference No.: 20222450, dated October 26, 2022).
Inclusion Criteria
Fever with clinically suspected leptospirosis cases above 18 years of age.
WHO definition for suspected leptospirosis cases.
‘Any patient presenting with an abrupt onset of fever, chills, conjunctival suffusion, headache, myalgia, oliguria, jaundice, breathlessness and haemoptysis’.
Exclusion Criteria
Patients <18 years of age, with conditions such as malaria, dengue or hepatitis.[7]
A total of 100 patients with a history of fever of more than five days associated with exposure to risk factors were included in this study. The sociodemographic data, including age, gender, occupation and risk factors, were collected from the patients with a structured proforma. Under aseptic precautions, the serum sample was collected from 100 patients who fulfilled the inclusion criteria. Each samples were tested for anti-Leptospira IgM antibodies using the Indirect IgM ELISA (Lepto IgM Microlisa using recombinant Leptospira antigens representing key immunodominant epitopes, J. Mitra and Co. Pvt. Ltd., New Delhi, India
Statistical Analysis
The clinical data were entered in Microsoft Excel and analysed using mean and standard deviation for continuous variables and the chi-square test for categorical variables. (P value: < .05).
Results
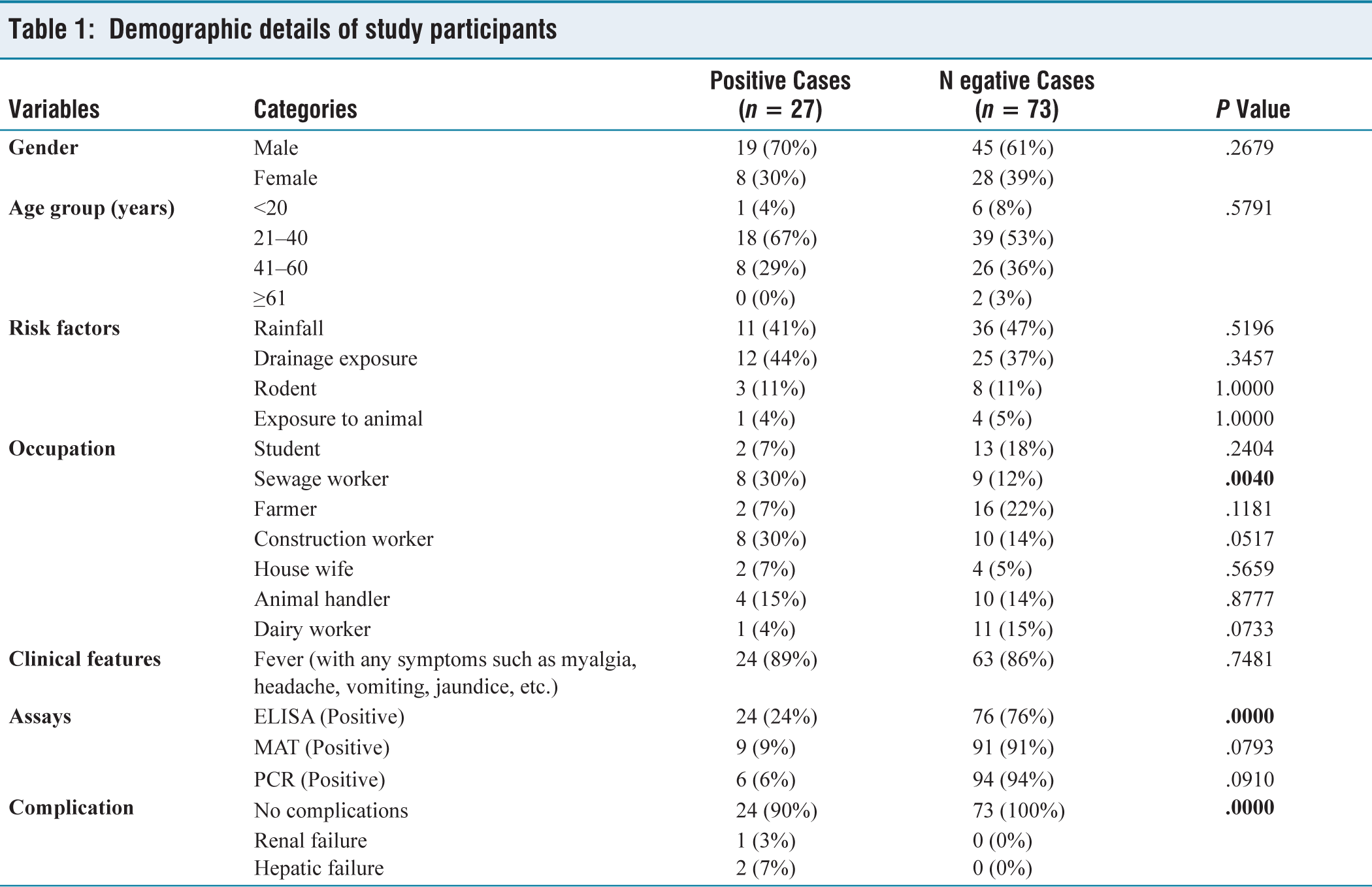
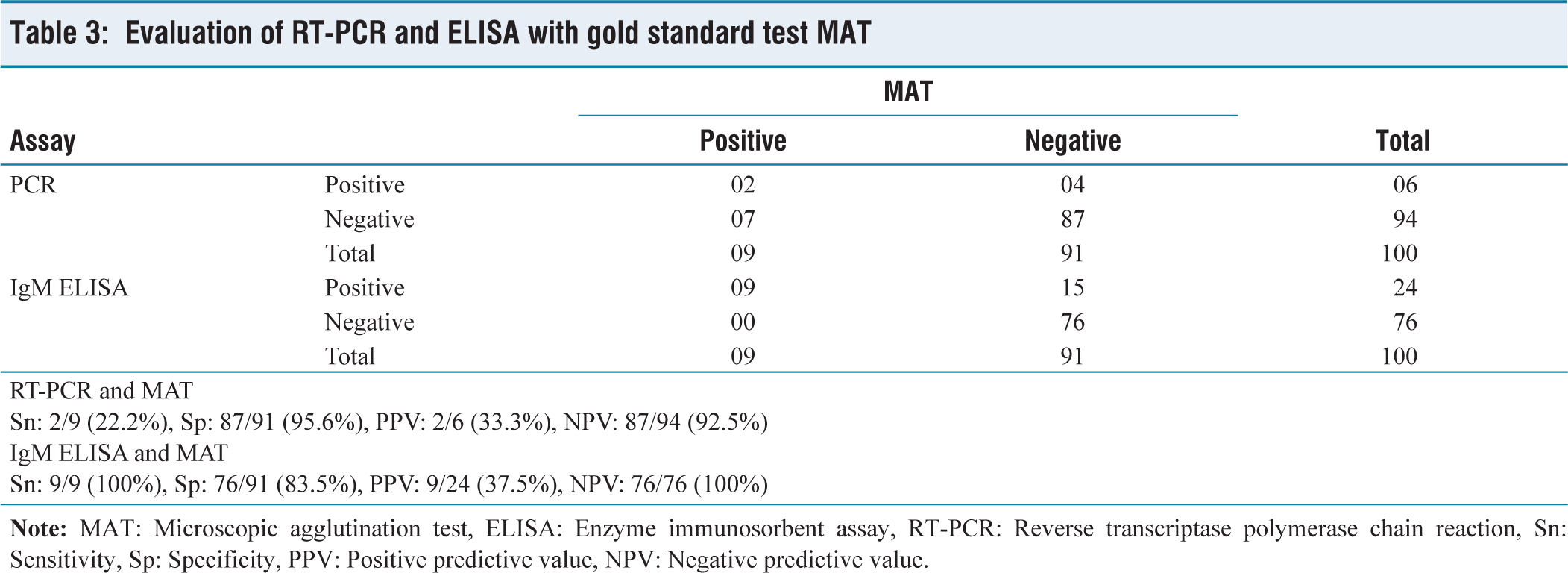
Out of 100 study participants, 65% were male, with the highest prevalence of leptospirosis observed in individuals aged 21–40 years (67%). Environmental risk factors, such as rainfall exposure (47%) and drainage contact (37%), were commonly observed. Occupations involving sewage and construction work were notably associated with higher positive case rates, eight each (30%). Of the 100 cases, Leptospira positive by ELISA, MAT and Reverse Transcriptase–Polymerase Chain Reaction (RT-PCR) was 24%, 9% and 6%, respectively [Table 1]. A total of 27 cases were detected by any one of these assays, which included ELISA only (14), MAT only (0), PCR only (3), ELISA and MAT (7), ELISA and PCR (1), ELISA, PCR and MAT (2) [Table 2]. By MAT, the various serovars detected were L. grippotyphosa (4), L. australis (3) and L. autumnalis (2). Males represented 19 (70%) of positive cases, with fever being the most frequent clinical feature in 24 (89%). In comparison with MAT the gold standard test, RT-PCR showed the sensitivity (22.2%), specificity (95.6%), positive predictive value (PPV) (33.3%) and negative predictive value (NPV) (92.5%)Similarly, in comparison with MAT, ELISA showed the sensitivity (100%), specificity (83.5%), PPV (37.5%) and NPV (100%) [Table 3].
Demographic details of study participants
Distribution of assay positivity among the study participants

Evaluation of RT-PCR and ELISA with gold standard test MAT
Discussion
Leptospirosis has a biphasic clinical presentation with an initial septicemic phase followed by an immune phase. The most severe form of the disease with multisystem involvement, including vascular, hepatic, renal and pulmonary and skeletal muscle injury, is designated as Weil’s disease.[8,9] Martinez-Lopez et al. recorded that pathogenic Leptospires do not cause apoptosis or necrosis; instead, they significantly disrupt the endothelial layer, resulting in haemorrhagic manifestations.[10] Because of its protean manifestations and elusive features, it is difficult to diagnose leptospirosis clinically.[11] Further, it mimics other fevers such as influenza, malaria, dengue fever, brucellosis, Q fever, viral haemorrhagic diseases and typhoid fever.[12,13] It responds well to antibiotic therapy and if left untreated, it may result in mortality.
MAT is the cornerstone in the diagnosis of leptospirosis, which identifies the serovar, useful in epidemiology. It is a complicated test as it involves a variety of Leptospires with differing antigenic structures to cover the spectrum of Leptospira infection; hence, it is essential to maintain the stock cultures. It is a laborious test with a subjective interpretation and often requires paired serum for confirmation. Initial high titres or a rise in titres are diagnostic; it begins to rise by the end of the first week and peaks at the third or fourth week. The high MAT titres take quite a long time to drop, which is useful for epidemiological surveys. It detects both IgM and Immunoglobulin G (IgG), hence a large proportion of the population may have persisting antibodies that interfere with the diagnosis of current infection.[14]
ELISA IgM is a simple test that detects genus-specific antibodies, which start to rise in the early phase (fifth day) and decline early (60 days). Some studies mentioned that Leptospira IgM and IgG may persist for years.[15] It helps in the rapid diagnosis of present infection, but it will not identify the infecting serogroup. The antigens used in this test can be from pathogenic Leptospires (L. icterohaemorrhagiae) or saprophytic Leptospira (L. biflexa). If the initial titres are low, repeat testing is required or a high titre in a single sample can be diagnostic. If a single sample is available, it is better to do both ELISA and MAT. Because ELISA IgM will help in the diagnosis of present infection and MAT will identify the serogroup.[14] The repeated contact with the same circulating spirochetes, especially in sewage workers and farmers, leads the immune system to produce antibodies regularly and attenuate the symptoms during reinfection.[16]
The prevalence of leptospirosis varies from region to region. Diagnosis of leptospirosis using PCR, MAT and IgM ELISA was 6%, 9% and 24%, respectively, in the present study. This wide difference could be due to the differences in the serovars or serogroups tested.[16]
In the present study, PCR was positive in 6% of cases. The low positivity in blood may be due to PCR inhibitors such as urea, creatinine and haemoglobin derivatives. Also, the specimens were collected 5-9 days after the onset of fever, after which the bacteraemia generally begins to fall. Hence, PCR can be used as a complementary test in the early phase of infection when antibody detection by serology is negative.
Paired sera were not tested for the serological test and PCR was done only after five days of infection, which are the major limitations of the present study.
Conclusion
In the present study, diagnosis of leptospirosis by MAT (9%), ELISA (24%) and PCR (6%) was recorded. Both ELISA and MAT can be done if a single sample is available. PCR can be used as a complementary test in the early phase of infection, especially when the antibody detection is negative.
Footnotes
Acknowledgements
We thank all the Laboratory Technicians for sample processing and testing. No contributor has been omitted.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
TIREC Reference No.: 20222450, dated October 26, 2022.
Informed consent
Written informed consent was obtained from all participants prior to sample collection.
Credit author statement
I hereby certify that I have made a substantial contribution to this manuscript in (a) conception and design or acquisition of data or analysis and interpretation of data; (b) drafting the article or revising it critically for important intellectual content and (c) final approval of the version to be published.
Data availability
The data have not been published or presented anywhere else.
Use of artificial intelligence
No artificial intelligence tools were used in the conduct, analysis, or reporting of this study.