
Abstract
Background and Objectives:
Non-alcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease worldwide. Indian data on the clinical spectrum, comorbidities and fibrosis burden of NAFLD remain limited. This study aimed to evaluate the clinical profile, laboratory parameters, comorbid associations and non-invasive fibrosis markers among patients with NAFLD at a tertiary care centre in Western India.
Methods:
This was a prospective observational study conducted over 12 months, enrolling 115 adult patients diagnosed with NAFLD on ultrasonography, with or without transient elastography or liver biopsy. Clinical features, biochemical parameters, metabolic comorbidities and complications were recorded. Non-invasive fibrosis assessment was performed using FIB-4, APRI and NAFLD Fibrosis Score (NFS). Statistical analysis was done using SPSS version 25.
Results:
The mean age of patients was 61.7 years, with a slight female predominance. Metabolic syndrome and diabetes mellitus were the most common comorbidities. Females had a significantly higher mean body mass index. Advanced fibrosis was highly prevalent, particularly in patients aged ≥60 years, with FIB-4 identifying high or advanced fibrosis in over 70% of cases. Portal hypertension and ascites were the most common complications.
Conclusion:
NAFLD patients presenting to tertiary care centres in India often have advanced disease with a high burden of fibrosis and metabolic comorbidities. Non-invasive fibrosis scores, particularly FIB-4, are valuable tools for risk stratification. Early detection and systematic screening are essential to prevent progression and complications.
Keywords
Introduction
Non-alcoholic fatty liver disease (NAFLD) is a chronic liver condition characterised by excessive accumulation of fat in hepatocytes in individuals with minimal or no alcohol consumption.[1] It is an overarching term that includes all the disease grades and stages and refers to a population in which >5% of hepatocytes display macro-vesicular steatosis in the absence of an identifiable alternative cause (e.g., medications, starvation, monogenic disorders) in individuals who drink little or no alcohol (defined as <20 g/day for women and <30 g/day for men).
It is the commonest cause of chronic liver disease worldwide, with its spectrum ranging from hepatic steatosis (fatty liver) to non-alcoholic steato-hepatitis (NASH), with/without advanced fibrosis, and finally complicating into cirrhosis and hepatocellular carcinoma (HCC). Its rising incidence parallels the global obesity epidemic, making it a major public health concern.[2]
Clinically, many individuals with NAFLD remain asymptomatic, particularly in the early stages. In more advanced stages, complications related to cirrhosis, such as jaundice, ascites and variceal bleeding may manifest. Patients with NASH are at a higher risk of progression to liver-related morbidity and mortality compared to those with simple steatosis.[3]
Laboratory parameters play a critical role in the diagnosis and monitoring of NAFLD. Elevated serum liver enzymes, specifically alanine aminotransferase (ALT) and aspartate aminotransferase (AST), are commonly observed, with ALT elevations being more prominent in early disease. Emerging biomarkers, including cytokeratin-18 fragments, adipokines and extracellular matrix turnover markers, are being explored for their potential to differentiate simple steatosis from NASH and assess fibrosis severity.[4–6]
NAFLD is closely associated with a spectrum of comorbid conditions that contribute to its systemic impact. The most significant comorbidity is metabolic syndrome, characterised by a constellation of Central Obesity, insulin resistance, hypertension and dyslipidaemia. Other comorbidities include polycystic ovary syndrome (PCOS), hypothyroidism, obstructive sleep apnoea (OSA) and chronic kidney disease (CKD). Additionally, there is a growing recognition of the association of NAFLD with extra-hepatic malignancies, particularly colorectal cancer, likely mediated through shared mechanisms of chronic inflammation and insulin resistance.[7–9]
There is a scarcity of studies on NAFLD in Indian patients at large, with a growing need for observational studies, large-scale registries, and interventional studies for this rapidly growing disease. With this background, the present project was planned to study the clinical profile, laboratory parameters and comorbid associations in NAFLD at a tertiary care institute in Western India.
Material and Methods
Study Design and Setting
Prospective observational study carried out at a tertiary care hospital.
Participant Selection and Sample Size Calculation
Sample size was determined using nMaster software based on an estimated NAFLD prevalence of 38% from previous literature, using the formula N = 4pq/l2
Where,
Q = 1-P, L = Absolute error (5%)
A minimum sample size of 115 was required to achieve a 95% confidence interval and 90% power.
Inclusion Criteria
All adult patients diagnosed with NAFLD by abdominal ultrasound with/without transient elastography/liver biopsy.
Provided written informed consent.
Exclusion Criteria
Cases having secondary causes: Viral hepatitis, autoimmune liver disease, and drugs.
Patients with alcohol consumption >30 g/day (males) and >20 g/day (females).
Patients who refused to participate in the study.
Patients <18 years of age.
Study duration: 12 months
Data Collection and Clinical Assessment
A standardised proforma was utilised to record:
Clinical history. Anthropometry: Height, weight, and body mass index (BMI). Patients were categorised into ‘Lean’ or ‘Obese’ NAFLD based on Indian-specific BMI cut-offs. Laboratory investigations: Complete blood count, liver function tests (ALT, AST, ALP, albumin, bilirubin), glycaemic profile (HbA1c), renal function tests (serum creatinine), and thyroid profile (TSH). Assessment of liver fibrosis: FIB-4 Index, APRI (AST to platelet ratio index), NAFLD fibrosis score (NFS).
Statistical Analysis
The data was entered using MS-Excel and analysed statistically using SPSS-25. Quantitative variables were expressed as mean value ± standard deviation or median ± interquartile range. Qualitative data were expressed as percentages (%) and proportions. An appropriate statistical test was used to infer an association between two variables, and a P value of <.05 was considered to be statistically significant.
Ethical Considerations
The protocol was presented before the Institutional Review Board for approval. After due approval, the study was initiated. Before including any patient for the participation in the study, a voluntary written consent for participation was obtained from either the patient and/or his/her legally acceptable representative.
Results
Demographic and Clinical Characteristics
In this study, a total of 115 patients who were diagnosed with NAFLD after considering inclusion and exclusion criteria were included. Table 1 shows the age-wise distribution of enrolled patients. 53.1% of patients were females, while 46.9% of patients were males.
Distribution of patients according to age (n = 115)

The italic values represent the most common age group.
The mean BMI was significantly higher among female patients (28.95 kg/m2) as compared to male patients (26.27 kg/m2). The difference between the two was statistically significant (P = .02).
Table 2 shows the distribution of patients according to symptoms present at the time of their presentation. 80% of the patients had pallor on clinical examination.
Distribution of patients according to symptoms

Biochemical Profile
All parameters were comparable across both genders [Table 3], and the difference between the two groups was not statistically significant (P > .05) except for MCV and Serum Creatinine (P = .03), in which both parameters were significantly higher among male patients than female patients.
Gender wise comparison of selected laboratory parameters

As shown in Table 4, females and younger patients (P = .04) had higher ALT levels. Similarly, patients with high ALT levels had significantly higher BMI, INR and prolonged prothrombin time as compared to patients with normal ALT levels (P < .05). In patients with high ALT levels, significantly high AST levels, serum alkaline phosphatase and total bilirubin levels were present (P < .05). The most prevalent comorbidities in both the genders were metabolic syndrome and diabetes mellitus.
Comparison of patients based on normal and high ALT

As shown in Table 5, obese patients were comparatively younger, and there was a statistically significant difference in the mean age between the two groups. Among patients with different comorbidities, only metabolic syndrome was found to be significantly associated with obesity (P = .01).
Comparison of patients based on obese versus lean NAFLD

Non-invasive Fibrosis Assessment
Using FIB-4 as a marker, it was found that 56.5% of patients aged less than 60 years, as compared to 81.2% of patients aged ≥60 years, had high/advanced fibrosis. The association between age and FIB-4 score was statistically significant (P = .02) [Table 6].
Age-wise comparison of non-invasive biomarkers of fibrosis

Discussion
NAFLD represents a growing clinical and public health challenge, emerging as the most common Chronic Liver Disorder globally. In the present study, the mean age was nearly identical between male (61.80 years) and female (61.75 years) patients, with no significant difference (P = .98). 71% patients were obese. Mean BMI was significantly higher in females (28.95 kg/m²) compared to males (26.27 kg/m²), the difference being statistically significant (P = .02). 11.3% of the patients were asymptomatic. The most prevalent comorbidities among both genders were metabolic syndrome and diabetes mellitus. Among various comorbidities, only metabolic syndrome showed a statistically significant association with obese NAFLD compared to lean NAFLD (P = .01). 71.3% patients had advanced fibrosis according to FIB-4 scores. Age-wise comparison revealed that 56.5% of patients with age <60 years had high/advanced fibrosis, compared to 81.2% of those aged ≥60 years. The association between age and FIB-4 score was statistically significant (P = .02). The mean age of cirrhotic patients in the study was 63.08 ± 5.57 years, indicating decompensation at an older age.
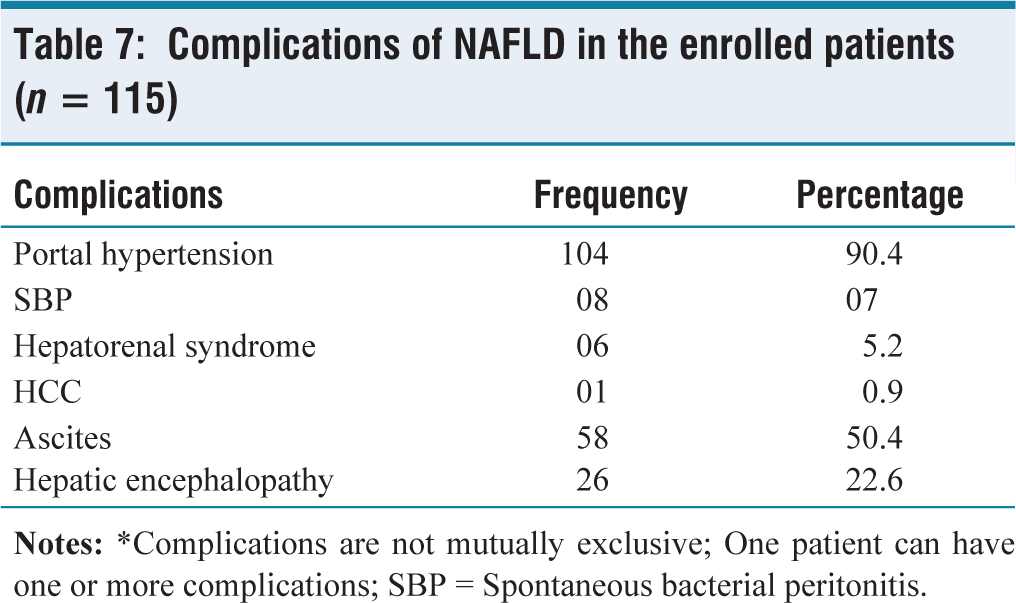
Table 7 shows the complications of NAFLD in the enrolled patients.
Complications of NAFLD in the enrolled patients (n = 115)
In studies by Li W et al.,[10] Suman B et al.,[11] Gaharwar R et al.[12] and Mahaling D et al.,[13] the mean age of the enrolled patients was 35.39, 53.70, 49 and 49.14 years, respectively. The difference in age and gender profile could possibly reflect geographic and racial prevalence of various risk factors. Men and postmenopausal women are more susceptible to developing NAFLD, and oestrogen appears to be protective by preventing dyslipidaemia and its anti-inflammatory effects.[14]
In a study by Arfeen N et al.,[15] the prevalence of overweight (45.53%) and obesity (30.35%) was notable. In another study by Vakil Z et al.,[16] 43.75% of the patients were asymptomatic. In another study by Jalodiya S et al.,[17] fatigue (73%), abdominal pain (55%) and dyspepsia (48%) emerged as the dominant symptoms. In another study by Khoonsari M et al.,[18] the most common symptoms were upper abdominal pain, fatigue, thirst and anxiety. The present study’s low asymptomatic rate (11.3%) suggests a cohort with advanced NAFLD, possibly due to its older age (61.77 years) and higher disease severity. Significantly higher levels of AST, serum alkaline phosphatase, and total bilirubin were observed in patients with elevated ALT levels (P < .05), which is consistent with a study by Alswat et al.[19] The association between gender and FIB-4 score was not statistically significant (P = .35), which is in contrast to the findings from the study done by Alswat et al.,[19] which reported significantly higher FIB-4 scores in males. In a large cohort study by Schreiner AD et al.,[20] individuals with high-risk FIB-4 scores (>2.67) faced a significantly increased risk of severe liver outcomes. These findings underscore the utility of the FIB-4 score as a valuable non-invasive tool for risk stratification, highlighting its potential role in early identification and proactive management of liver disease. 71.3% of the enrolled patients in our study demonstrated advanced fibrosis according to NFS scoring. In another study by Nagaraj K et al.[21] based on NFS, about 11 patients (5.5%) had a score of >0. 675, indicating advanced stages of fibrosis. This might be due to the fact that our study was done at a tertiary care centre where many complicated patients present at an advanced stage after being referred from peripheral centres.
This study had a prospective design with systematic clinical and laboratory evaluation, with inclusion of both lean and obese NAFLD, highlighting an under-recognised phenotype. A comprehensive assessment using multiple validated non-invasive fibrosis scores was done with a focus on an older, real-world tertiary-care population with advanced disease. The study adds region-specific Indian data on NAFLD severity, comorbidities and complications. The study’s observational nature limits the ability to establish causal relationships. As the study was conducted at a single institution, this may reduce the generalizability of the findings to broader populations with diverse demographic and clinical characteristics. A limited number of participants may not adequately represent the variability of NAFLD presentations and associated comorbidities. Without follow-up, the study cannot assess progression or outcomes related to NAFLD or its comorbid conditions.
Future research, preferably multi-centric and longitudinal in design, is essential to further elucidate causal pathways, validate non-invasive diagnostic markers, and establish evidence-based therapeutic interventions. Early identification and multidisciplinary management of NAFLD and its comorbidities are critical to curbing the growing burden of liver-related and cardiovascular morbidity in affected individuals.
Conclusion
The present study highlights the diverse clinical profiles, pertinent laboratory parameters and prevalent comorbid associations in individuals diagnosed with NAFLD. The findings of this study provide critical insights for the management of NAFLD within the Indian healthcare framework. The presence of multiple comorbid conditions not only complicates the clinical course but also increases the risk for disease progression, thereby emphasising the need for early detection and comprehensive management strategies. The high prevalence of diabetes and metabolic syndrome in this cohort necessitates a multidisciplinary approach. NAFLD should not be treated as an isolated liver disease but as a component of systemic metabolic failure requiring simultaneous cardiovascular and endocrine management.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/ or publication of this article.
Institutional ethical committee approval number
The study has been approved by the Institutional Review Board (NHLIRB/2024/March/27th/No.11).
Credit author statement
Sanket P. Bharadwaj contributed to concepts, design, definition of intellectual content, literature search, data acquisition, data analysis, statistical analysis, manuscript preparation, and manuscript editing.
Pankaj Garg contributed to concepts, definition of intellectual content, data analysis, manuscript preparation, manuscript editing, and manuscript review.
Khushali L. Patel contributed to concepts, definition of intellectual content, data analysis, manuscript preparation, manuscript editing, and manuscript review.
Ami P. Parikh contributed to concepts, design, definition of intellectual content, literature search, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing, and manuscript review.
Data availability
The data can be made available from the corresponding author upon reasonable request and subject to institutional approvals.
Use of artificial intelligence
Not used.