
Abstract
Background:
The APACHE IV score is a widely used tool for predicting outcomes in critically ill patients. However, in resource-limited settings, complete data required for its calculation may not be readily available, and manual computation without automated systems can be resource-intensive. This study aimed to identify key APACHE IV variables that reliably predict mortality.
Methods:
In this prospective cohort study, 150 critically ill patients admitted to a multidisciplinary ICU were categorised into survivor and non-survivor groups based on ICU and hospital outcomes. Clinical and laboratory variables used to calculate APACHE IV score were recorded during the first 24 hours of admission, and the worst values were analysed. Comparisons were performed using independent sample t-tests and chi-square tests, with P < .05 considered significant. Receiver operating characteristic (ROC) curve analysis was used to evaluate the predictive performance of the APACHE IV score and selected variables.
Results:
Significant predictors of ICU mortality included lower mean arterial pressure (62.6 vs. 81.8 mm Hg, P = .002), lower systolic BP (110.7 vs. 128.2 mm Hg, P = .008), and reduced GCS score (4.7 vs. 11.7, P < .001). Non-survivors had elevated urea levels (96.1 vs. 58.5 mg/dL, P = .026), high bilirubin (1.9 vs. 0.8 mg/dL, P < .001), low albumin (2.9 vs. 3.6 g/dL, P = .001) and low platelet counts (154,328/mm³ vs. 245,977/mm³, P = .008). Hospital mortality showed similar patterns, with non-survivors demonstrating lower GCS, increased FiO2 requirements (44.1% vs. 33.1%, P = .010), elevated urea, lower albumin and reduced platelet counts. The need for mechanical ventilation was more common among both the ICU and hospital non-survivors. ROC analysis demonstrated excellent predictive ability of the APACHE IV score for ICU mortality (AUROC: 0.863) and good performance for hospital mortality (AUROC: 0.760). GCS and albumin also showed good discrimination for ICU mortality and acceptable discrimination for hospital mortality.
Conclusion:
Lower MAP, SBP, and GCS, along with reduced platelet count and albumin levels, and elevated urea and bilirubin levels, as well as the need for mechanical ventilation, are key predictors of ICU and hospital mortality. The APACHE IV score demonstrates excellent predictive performance for mortality. Selected variables, particularly GCS and serum albumin, also show good discriminatory power and may serve as practical tools for mortality prediction in resource-limited settings.
Introduction
Mortality is a key quality metric that reflects many aspects of patient care, including the use of best practices, accurate diagnosis and effective, timely therapies.[1] Evaluating a patient’s condition and selecting appropriate diagnostic and treatment tools are crucial steps in determining the required level of care, ultimately enhancing the quality of health services provided to ICU patients.[2] The APACHE IV score is one of the most commonly used tools for mortality risk stratification in the ICU. It combines multiple physiological and biochemical variables along with demographic data to provide an estimate of mortality risk.[3] Despite its widespread use, the complexity and data demands of the APACHE IV scoring system pose significant challenges, especially in low-resource settings where access to advanced diagnostic tools and monitoring is limited. Not all variables needed for APACHE IV calculation are obtained at ICU admission due to cost implications. Moreover, in the absence of an electronic health information system, calculating APACHE IV necessitates trained personnel and quality medical records. With limited resources and cumbersome data collection and calculation needed to compute APACHE IV, most ICUs in resource-limited settings do not utilise any severity scores, making research, quality control and risk prediction of outcomes difficult.
In this study, a comparative analysis of the various variables within the APACHE IV scoring system was done to identify key components that were associated with ICU and hospital mortality of critically ill patients. Identifying key elements would enable ICUs with limited resources to at least collect this data and utilise it for baseline risk prediction.
Materials and Methods
This prospective observational cohort study investigated the association of clinical and biochemical parameters included in the APACHE IV score with ICU and hospital mortality among critically ill patients. After clearance from the institutional ethical committee (072/11–22), informed consent was obtained, and we studied 150 adult patients (≥18 years) at index admission to the multidisciplinary critical care unit during the period (September 2022 to August 2023). Exclusion criteria included ICU readmission during the same hospitalisation, interhospital ICU transfers, and the presence of DNI/DNR/DNE orders or discharge against medical advice (DAMA) at any point during the ICU and hospital stay. Data were collected from medical records during the initial 24 hours of admission. Variables included demographic data (age, gender), hemodynamic parameters (MAP, SBP), neurological status (GCS), respiratory parameters (Respiratory rate, FiO2%, ABG), biochemical markers (urea, creatinine, albumin, bilirubin, Blood sugar, Sodium, Haemoglobin, Haematocrit, WBC, platelet count) and other clinical factors (need for mechanical ventilation, need for emergency surgery) and pre-ICU length of stay. Patients were followed until discharge from the ICU and hospital, and outcomes were documented as survivors or non-survivors. Statistical analysis was performed using the Shapiro–Wilk test for normality, and the data obtained were presented as median or the mean and SD (standard deviation). The continuous variables were compared using the independent-samples t-test. Categorical variables were compared using either the Chi-square test or Fisher’s exact test, depending on the number of observations, and a P < .05 was considered statistically significant. Discrimination was assessed by calculating the AUROC (Area Under ROC) along with its 95% confidence interval. AUROC values were interpreted as poor when ≤0.70, adequate between 0.71 and 0.80, good between 0.81 and 0.90, and excellent when ≥0.91.
Results
The study cohort consisted of 150 patients, of whom 62% were males and 38% were females, with a mean age of 62.1 years (range 20–95 years). A comparison of clinical and laboratory parameters based on ICU mortality showed that ICU non-survivors had lower mean arterial pressure (MAP) (62.6 vs. 81.8 mm Hg, P = .002) and systolic blood pressure (SBP) (110.7 vs. 128.2 mm Hg, P = .008), indicating significant hemodynamic instability. Neurological function, as measured by the Glasgow Coma Scale (GCS), was markedly poorer in non-survivors, with a mean score of 4.7 compared to 11.7 in survivors (P < .001). Among the biochemical parameters, non-survivors had elevated bilirubin levels (1.9 vs. 0.8 mg/dL, P < .001) and reduced albumin levels (2.9 vs. 3.6 g/dL, P = .001). Platelet counts were significantly lower among non-survivors (154,328.6 vs. 245,977.9 μL, P = .008), while urea levels were high (96.1 vs. 58.5 mg/dL, P = .026). Moreover, the requirement for mechanical ventilation (P = .001) was significantly more frequent among non-survivors [Table 1].
Comparison of clinical and laboratory parameters of APACHE IV score based on ICU mortality

Hospital mortality outcomes exhibited similar patterns to ICU mortality [Table 2]. Although differences in MAP and SBP between hospital survivors and non-survivors were not statistically significant, the trends aligned with those observed in ICU outcomes. GCS was significantly impaired in non-survivors (7.0 vs. 11.6, P < .001). Biochemical markers revealed higher bilirubin (1.5 vs. 0.8 mg/dL, P = .007) and urea levels (89.6 vs. 57.7 mg/dL, P = .028), lower albumin levels (3.0 vs. 3.6 g/dL, P < .001), and reduced platelet counts (172,030.0 vs. 247,484.6 μL, P = .011) in non-survivors. Respiratory parameters demonstrated that non-survivors required higher FiO2 (44.1% vs. 33.1%, P = .010) along with mechanical ventilation (P = .003). Gender differences, emergency surgery and pre-ICU length of stay were not significantly linked to either ICU or hospital outcomes.
Comparison of clinical and laboratory parameters of APACHE IV score based on hospital mortality

The APACHE IV score was significantly higher among non-survivors compared to survivors for both ICU mortality (115.0 ± 32.3 vs. 72.8 ± 23.9, P < .001) and hospital mortality (103.0 ± 34.9 vs. 72.8 ± 24.2, P < .001) [Table 3].
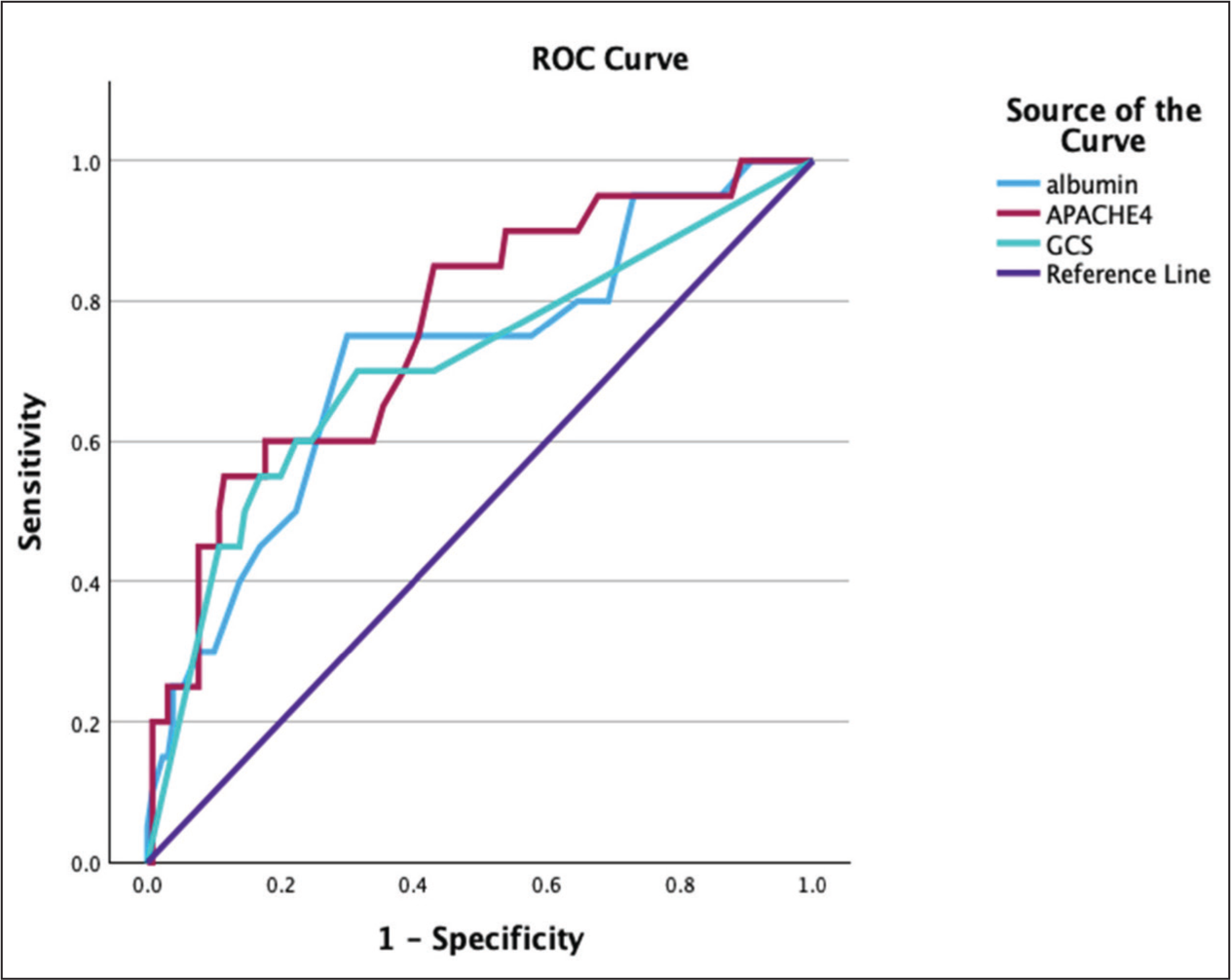
Receiver operating characteristic (ROC) curve [Figures 1 and 2] analysis demonstrated that the APACHE IV score had excellent predictive ability for ICU mortality (AUC: 0.863) and good predictive ability for hospital mortality (AUC: 0.760). Among individual variables, GCS showed good discrimination for ICU mortality (AUC: 0.825) and adequate discrimination for hospital mortality (AUC: 0.708). Serum albumin demonstrated adequate predictive ability for ICU mortality (AUC: 0.761) and hospital mortality (AUC: 0.716) [Tables 4 and 5].
APACHE IV score and outcomes

Area under ROC of APACHE IV score, GCS and albumin for predicting ICU mortality

Area under ROC of APACHE IV score, GCS and albumin for predicting hospital mortality

ROC curve demonstrating the predictive performance of APACHE IV score, GCS and Albumin for ICU mortality. The APACHE IV score showed the highest discriminatory ability, followed by GCS and albumin

ROC curve demonstrating the predictive performance of APACHE IV score, GCS and albumin for hospital mortality. The APACHE IV score showed the highest discriminatory ability, followed by albumin and GCS
Overall, the APACHE IV score demonstrated superior discrimination compared to individual variables for both ICU and hospital mortality, although selected individual parameters retained clinically meaningful predictive ability, which may be helpful in settings with limited resources.
Discussion
This study aimed to identify and compare key clinical and laboratory parameters of the APACHE IV score that can effectively predict ICU and hospital mortality. Significant differences were observed in hemodynamic, respiratory, and laboratory variables between survivors and non-survivors, providing valuable insights for early prognosis and intervention. Although previous studies have identified age as a consistent predictor of mortality in ICU patients,[2,4] our analysis found no significant differences in age or gender between survivors and non-survivors. Neurological status, measured by GCS, was significantly lower among non-survivors, highlighting its role as a reliable mortality predictor. The strong discriminatory ability of GCS observed in our ROC analysis further supports its clinical relevance. This finding aligns with existing literature highlighting GCS as a crucial indicator of neurological function, which has been integrated into various predictive models.[5]
Non-survivors of the ICU in our study consistently exhibited lower MAP and SBP. Additionally, the need for mechanical ventilation was significantly higher among non-survivors of both ICU and hospital, reflecting greater illness severity. Parajuli BD et al., in their study, have reported a significantly higher need for inotropes and mechanical ventilator support among non-survivors compared with the survivors, which correlates with our study findings.[6] A prospective multicentre cohort study conducted by Atumanya P et al. in Uganda to evaluate the characteristics and outcome of patients admitted to the ICU have also shown a statistically significant need for mechanical ventilation and vasopressors among ICU non-survivors.[7] Caires et al., in their retrospective study in predicting hospital mortality from clinical and laboratory data, found a significant association between hospital mortality and factors such as need for intubation and cardiovascular involvement. Among the variables, MAP, temperature, pH, lactate, creatinine, albumin, bilirubin and platelet values were significantly associated with death outcome.[8] This is comparable to our findings, where non-survivors exhibited elevated bilirubin and reduced albumin and platelet counts. Similarly, Khawannimit et al. reported that non-survivors had significantly lower GCS, lower SBP, higher bilirubin and creatinine values, lower platelet count and also more need for mechanical ventilation compared to survivors in their study predicting mortality in septic shock patients.[9] Zhi D et al. have also found that non-survivors had significantly higher bilirubin, creatinine and BUN levels, while patients who survived had higher GCS, platelet count and haemoglobin in their study, evaluating in-hospital mortality among patients with sepsis.[10] Elevated bilirubin levels, widely reported as a mortality predictor in sepsis[11] were strongly associated with mortality in our analysis as well. In the context of COVID-19 patients, Beigmohammadi MT et al. identified significant differences in WBC count, platelet count, urea, creatinine, bilirubin, and albumin levels between survivors and non-survivors, alongside a higher requirement for inotropic support among non-survivors.[12] These findings align with the broader applicability of these parameters across critically ill populations, including those in our study.
The APACHE IV score demonstrated excellent predictive performance for ICU mortality and good performance for hospital mortality, consistent with its established role as a comprehensive severity-of-illness scoring system. Importantly, ROC analysis confirmed that APACHE IV had superior discriminatory ability compared to individual variables. However, selected parameters such as GCS and serum albumin also demonstrated good to acceptable predictive performance, highlighting that lower albumin levels and low GCS are simplified important prognostic markers.
Although several variables were significantly associated with mortality, only GCS and serum albumin were included in the ROC analysis alongside the APACHE IV score. These variables were selected based on their strong clinical relevance, statistical significance, and ease of availability at the bedside. This streamlined approach enhances interpretability while adequately representing critical domains of neurological status and systemic severity.
The findings of this study have important implications for resource-limited settings. While APACHE IV remains a robust and comprehensive predictor, its calculation may be constrained by the need for multiple variables and the lack of automated systems. In such scenarios, a limited set of readily available parameters—such as GCS, albumin, urea, and platelet count—may serve as pragmatic tools for early risk stratification. These variables partially overlap with components of established scoring systems, such as the SOFA score, but are fewer and simpler to obtain, enhancing feasibility in routine clinical practice.
The study results emphasise integrating targeted hemodynamic, respiratory and laboratory parameters into ICU admission protocols. Incorporating these variables into simple bedside algorithms could improve prognostic accuracy, particularly in heterogeneous patient populations and resource-constrained environments. While this study does not propose a validated alternative scoring system, it provides a foundation for the development of simplified prognostic models derived from key APACHE IV components.
The study has some limitations. The single-centre design may limit the generalizability of the findings, and the relatively small sample size may have reduced statistical power for some variables. Additionally, certain confounders, such as pre-existing comorbidities, were not controlled for, which may have influenced outcomes. Future multicentre prospective studies with larger cohorts and more comprehensive data collection are warranted to validate and expand upon these findings.
Conclusion
Our study findings have identified specific clinical and laboratory variables within the APACHE IV score that predict mortality in settings where data may be limited. Early identification of high-risk patients through these parameters could enable tailored interventions, potentially improving survival rates. Further research validating these markers in a larger population is warranted to validate their clinical utility.
Footnotes
Acknowledgements
The authors would like to thank all the consultants and staff of the multidisciplinary team involved in the patient care at Apollo Hospital, Greams Road, Chennai. We also thank the research team for their valuable support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Institutional ethical committee approval was obtained for conducting the study (072/11–22).
Informed consent
Informed consent was obtained.
Credit author statement
Conceptualisation: Dr Ramesh Venkataraman.
Patient management and clinical data collection: All authors.
Data curation: All authors.
Writing - original draft: All authors.
Writing - review & editing: All authors.
Supervision: Dr Ramesh Venkataraman and Dr Nagarajan Ramakrishnan.
Final approval of the manuscript: All authors.
All authors have read and approved the final manuscript and agree to be accountable for all aspects of the work.
Data availability statement
Within the article.
Use of artificial intelligence
Not applicable.