
Abstract
Background and Aims:
Renal involvement is an increasingly recognised but under-reported complication of paediatric dengue. Data from the Indian subcontinent, particularly using the standardised acute kidney injury (AKI) definition (Kidney Disease: Improving Global Outcome [KDIGO]) and prospective design, remain limited. Hence, this study was undertaken with the aim to describe the clinical spectrum of renal involvement in children with dengue and identifying the associated risk factors.
Methods:
This prospective observational study was conducted between 1st March and 30th November 2025 at a tertiary care hospital in northern India in children ≤18 years having dengue infection. Clinical, laboratory and outcome data were collected and analysed.
Results:
Among 152 children ≤18 years (median age 108 months) admitted with confirmed dengue, renal involvement was observed in 42.1% (n = 64). Haematuria was seen in 23.7%, proteinuria in 22.3%, and AKI in 17.8%, with most AKI being Stages 1 or 2; only one child required dialysis. Children with renal involvement more often had severe dengue, clinical bleeding, clinical fluid overload, neurological involvement, hepatomegaly, hypoalbuminemia, severe thrombocytopenia and had higher serum creatinine and prolonged international normalised ratio. On multivariable analysis, older age (aOR = 1.028; 95% CI: 1.004–1.053; P = .020) and hepatomegaly (aOR = 18; 95% CI: 1.7–198; P = .017) were independent predictors of renal involvement. Length of hospital stay and in-hospital mortality were not significantly different between groups.
Conclusion:
Renal involvement is common in hospitalised children with dengue, but is usually mild and reversible. Hepatomegaly can serve as a simple bedside marker to identify children at higher risk who require closer renal monitoring and timely supportive care.
Introduction
Dengue fever, caused by the dengue virus (DENV), is one of the most common mosquito-borne infections worldwide and remains a major public health concern in tropical and subtropical regions. According to the World Health Organization (WHO), around 400 million infections occur each year, of which nearly one quarter manifest clinically.[1] Children contribute substantially to this burden, particularly in endemic countries such as India, where recurrent epidemics are reported.[1,2]
The clinical spectrum of dengue infection ranges from asymptomatic or mild febrile illness to severe forms, including dengue haemorrhagic fever (DHF) and dengue shock syndrome (DSS).[3] While plasma leakage, bleeding manifestations and hepatic dysfunction are well recognised, renal involvement has emerged as an increasingly reported but underappreciated complication.[4–6] The renal manifestations vary from transient proteinuria and haematuria to acute kidney injury (AKI), which may necessitate dialysis and significantly increase morbidity and mortality.[5,7]
The pathogenesis of renal involvement in dengue is multifactorial. Hemodynamic instability secondary to plasma leakage and shock, direct viral invasion of renal tissue, immune-mediated injury, rhabdomyolysis and multiorgan dysfunction in severe disease are the proposed mechanisms.[4,8] Several studies have highlighted the association of AKI with severe dengue, delayed presentation, shock and hepatopathy, suggesting that renal impairment is both a marker of disease severity and an independent predictor of poor outcomes.[5,9,10] However, the true incidence of renal involvement in paediatric dengue remains variable across studies, ranging from 2% to over 20%, depending on case definitions, study population and level of care.[4–6]
Early recognition of renal complications is crucial, as timely intervention can improve outcomes and prevent long-term sequelae. Despite its clinical significance, data on the spectrum and risk factors of renal involvement in children with dengue in the Indian subcontinent remain limited. Most available evidence is derived from adult cohorts or mixed populations, with fewer paediatric-focused studies.[10–12] In this context, we conducted a prospective study in children diagnosed with dengue fever at a tertiary care hospital. The primary objectives of this study were to describe the clinical spectrum of renal involvement in paediatric dengue and to identify the risk factors associated with its development.
Methods
This study was conducted at a tertiary care centre in northern India over a period of 9 months after approval from the institutional ethics committee. All the patients up to 18 years of age with a confirmed diagnosis of dengue between 1st March 2025 and 30th November 2025 were included. All the clinical and demographic details were recorded on a pre-designed proforma. Informed consent was obtained from parents/caregivers of all the participants, while assent was taken from those 7 years and above.
Dengue was diagnosed based on WHO criteria, that is, presence of clinical features plus either detection of NS1 antigen by ELISA/RDT or seroconversion/four-fold increase in antibody titre.[13] Only confirmed dengue cases were included in the analysis. Patients with incomplete records or those having preexisting chronic kidney disease were excluded from the study. Severity of dengue was graded as per WHO guidelines into dengue without warning signs, dengue with warning signs and severe dengue.[14]
Renal involvement was considered when a patient had either one or more of these findings: presence of proteinuria (urine protein ≥1+; 30 mg/dL) by dipstick, haematuria (urine RBC ≥5 per high power field in a fresh centrifuged specimen) or AKI. AKI was defined based on Kidney Disease: Improving Global Outcome (KDIGO) criteria as an increase in serum creatinine (SCr) of ≥0.3 mg/dL within 48 h or a rise to ≥1.5 times the baseline, which is known or presumed to have occurred within the prior 7 days.[15] Baseline SCr was defined as the lowest available value within the preceding 3 months.
In children without prior creatinine measurements, baseline creatinine was estimated by back-calculating from an assumed age-appropriate eGFR using the bedside Schwartz equation. AKI severity was further classified into Stages 1–3 as per KDIGO criteria.[15] Estimated glomerular filtration rate (eGFR) was calculated by using the bedside Schwartz equation (<18 years), that is, 0.413 × ht (cm)/SCr (mg/dL).[15] All the patients were investigated and managed as per hospital protocol.
Descriptive statistics were used to summarise baseline values and demographic data. Qualitative variables were presented as frequencies and proportions. For quantitative variables, assessment of normality was performed using the Shapiro-Wilk test together with visual inspection of histograms and Q-Q plots. Variables showing normal distribution were expressed as mean (standard deviation), whereas skewed variables were summarised using median (Interquartile range). Comparison of categorical variables between two groups (renal involvement vs. no renal involvement) was done using χ2-test or Fisher’s exact tests as appropriate, and the independent Student’s t-test/Mann-Whitney U test (based on normality) was used for analysing continuous data. For assessment of predictors of renal involvement, all the variables with a P < .1 were added in the multiple regression model. A P value of <.05 was considered significant for all inferential analyses in the study. IBM SPSS Statistics for Windows, Version 27.0 (IBM Corp., Armonk, NY, USA) was used for compiling and analysing data.
Ethics
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee at which the study was conducted (approval number-IEC/2025/AIR/85) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Results
Baseline Characteristics
A total of 152 children with dengue were included in the study [Table 1], with a male-to-female ratio of 1.7:1 (62.5% males). The median age was 108 months (IQR: 84–168), with the youngest being 2 months old and the oldest being 17 years. Among these, 12.5% (n = 19) had dengue without warning signs, 48% (n = 73) had dengue with warning signs, and 39.5% (n = 60) had severe dengue. The most common clinical feature was the presence of bleeding manifestation in nearly half (45.4%, n = 69) of subjects, followed by fever (40.1%) and hepatomegaly (mild to moderate, 29.6%). More than half of the patients (55.9%) required ICU admission, nine (5.9%) patients required mechanical ventilation, and inotropes were used in 16 (10.5%).
Baseline clinico-demographic characteristics of the study population
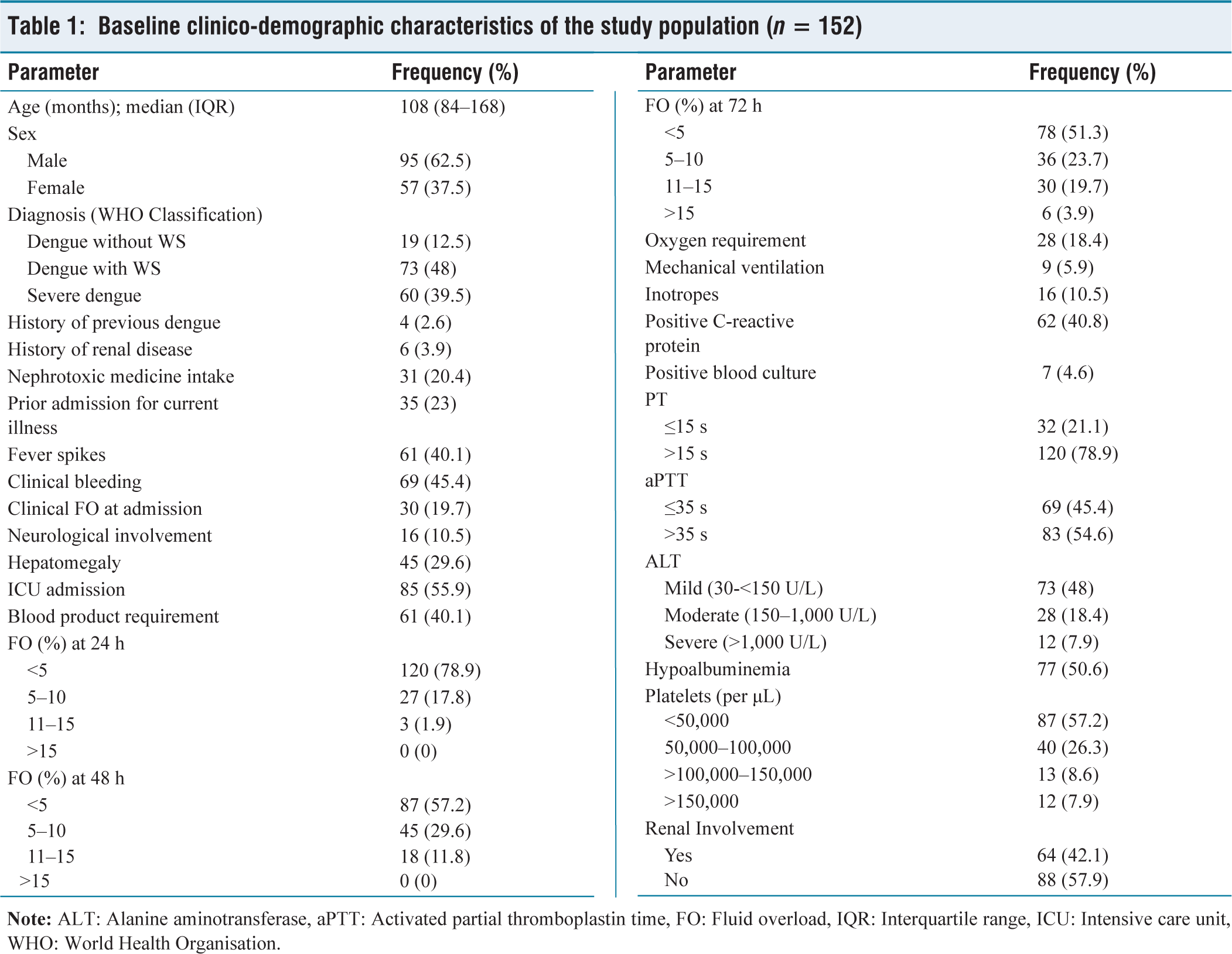
At admission, 40.8% had elevated C-reactive protein, while 4.6% of blood cultures were positive. Coagulation abnormalities were seen in the majority of the patients, with 78.9% having prolonged PT (>15 s) and 54.6% prolonged aPTT (>35 s). Liver involvement was common: 48% had mild elevation of ALT, 18.4% moderate, and 7.9% severe. Thrombocytopenia was marked, with 83.5% having platelets below 100,000/μL. Overall, renal involvement was seen in 64 patients (42.1%).
Pattern of Renal Involvement
Among those with renal involvement (n = 64), haematuria was the most common finding (23.7%), of which 58.3% had only microscopic, while 41.7% had gross haematuria [Table 2, Figure 1]. Proteinuria was present in 22.3% (n = 34), with 8.8% subjects having 3+ grade. Twenty-seven (17.8%) patients developed AKI, with the majority having KDIGO Stage 1 (44.4%) or Stage 2 (44.4%), while Stage 3 was seen in 11.1% (n = 3). Only one patient required renal replacement therapy (RRT).
Type and severity of renal involvement
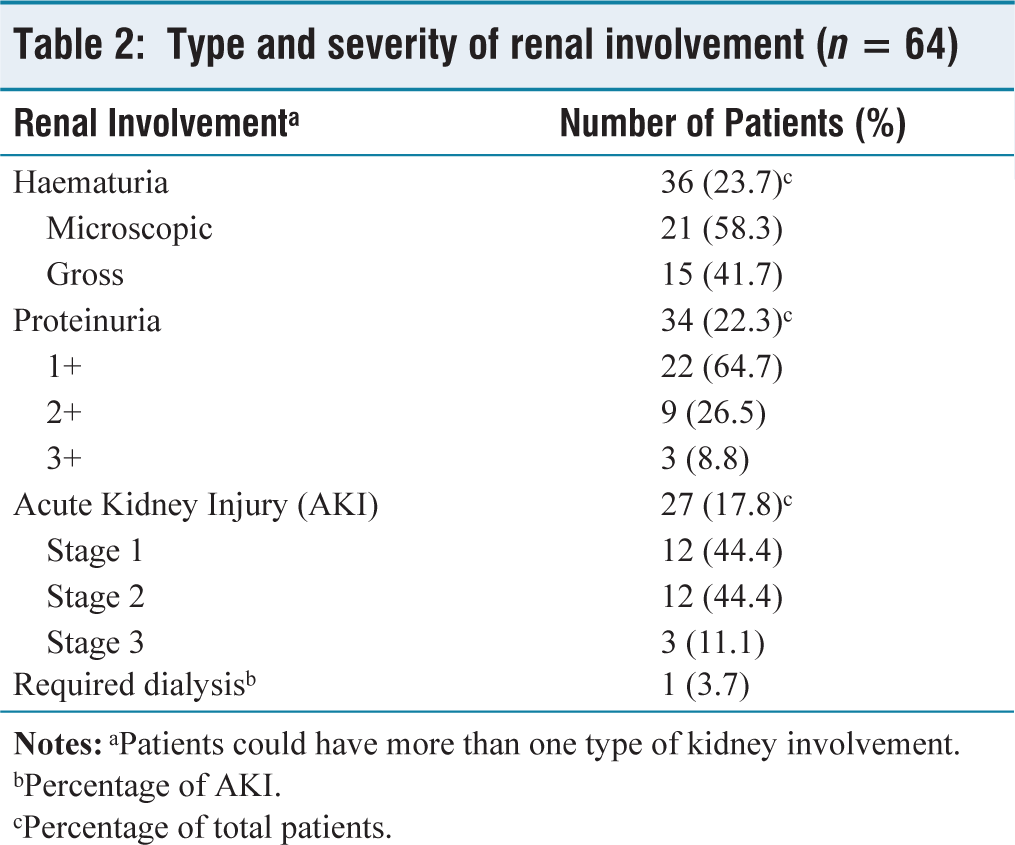
bPercentage of AKI.
cPercentage of total patients.
Laboratory Comparison
Children with renal involvement had overall significantly higher blood urea (P < .001), SCr (P < .001) and international normalised ratio (INR) (P < .001) levels compared to those without renal involvement [Table 3]. Platelets and serum albumin values were significantly lower among those with renal involvement.
Comparison of laboratory parameters among dengue patients with and without renal involvementa
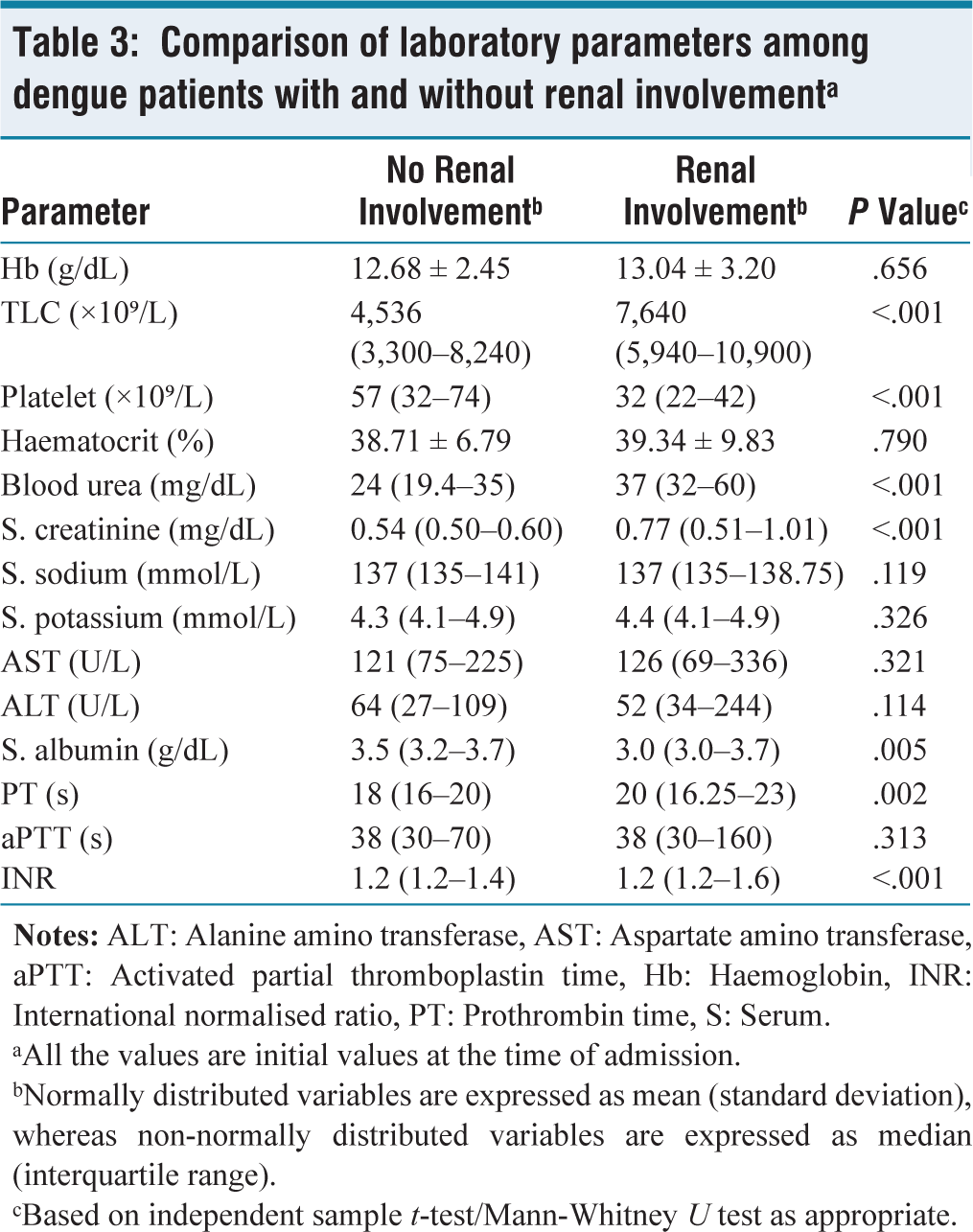
aAll the values are initial values at the time of admission.
bNormally distributed variables are expressed as mean (standard deviation), whereas non-normally distributed variables are expressed as median (interquartile range).
cBased on independent sample t-test/Mann-Whitney U test as appropriate.
Predictors of Renal Involvement
On bivariate analysis, older age, severe dengue, clinical bleeding, clinical fluid overload on admission, neurological involvement, hepatomegaly, elevated ALT, need for PICU, blood products requirement, hypoalbuminemia and severe thrombocytopenia were significantly associated with renal involvement [Table 4]. Multiple regression identified two independent predictors: age (OR = 1.028; 95% CI: 1.004–1.053; P = .020) and hepatomegaly (OR = 18; 95% CI: 1.7–198; P = .017).
Predictors of renal involvementa
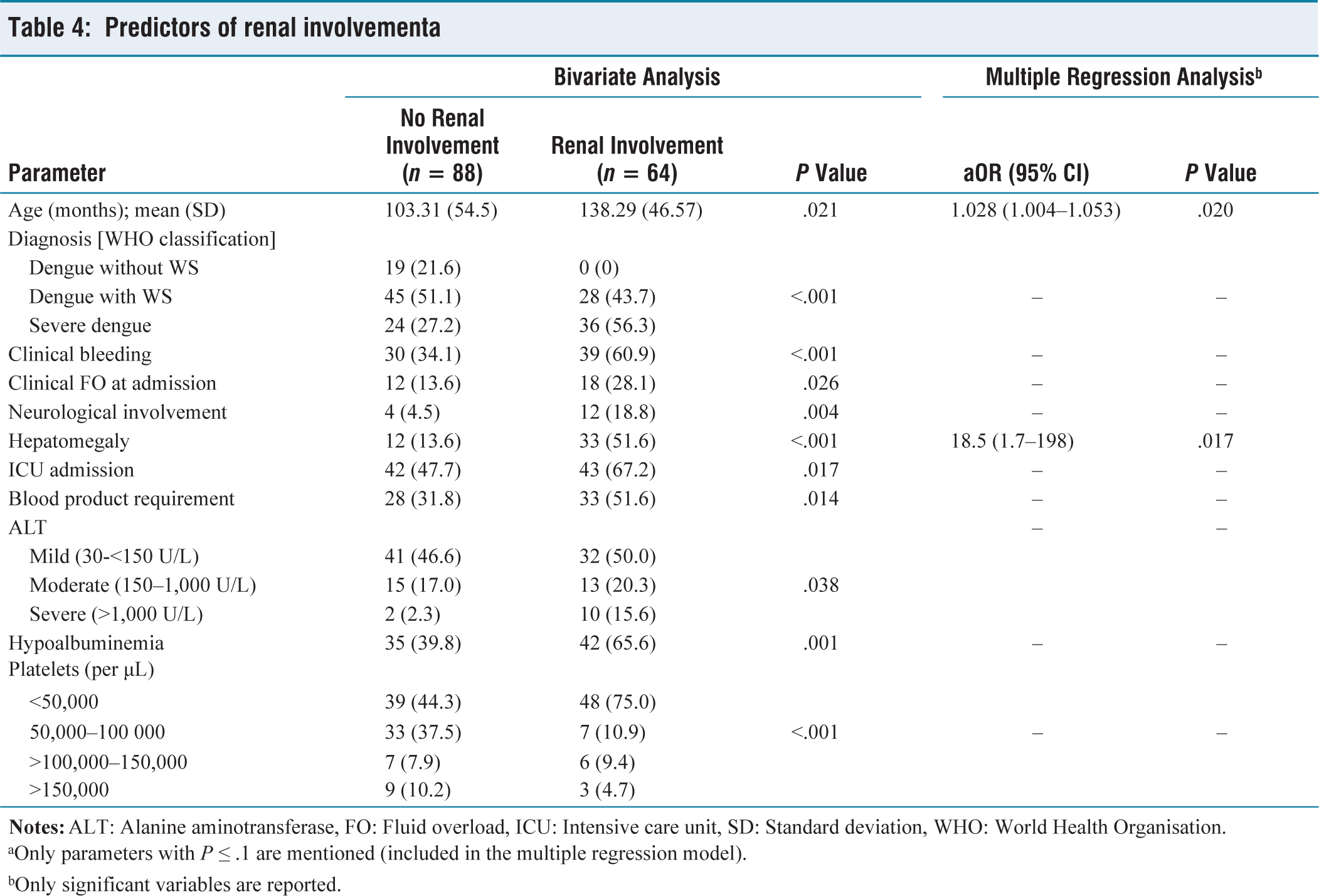
aOnly parameters with P ≤ .1 are mentioned (included in the multiple regression model).
bOnly significant variables are reported.
Outcomes
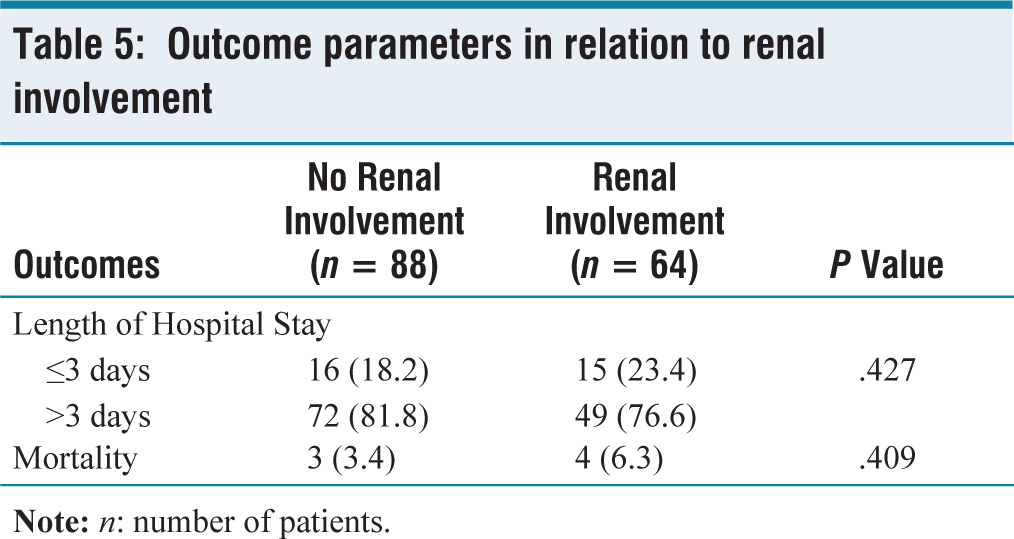
The median duration of hospital stay did not differ significantly between groups (P = .427). Mortality was low and comparable (6.3% vs. 3.4%; P = .409) in patients with and without renal involvement, respectively [Table 5].
Outcome parameters in relation to renal involvement
Discussion
In this cohort of 152 children with dengue, we observed a relatively high frequency of renal involvement (42.1%), with a spectrum ranging from microscopic haematuria and proteinuria to AKI, underscoring that renal injury is a clinically relevant but often under-recognised component of dengue in children. The pattern, risk factors and largely favourable short-term outcomes in this study add important paediatric data from northern India to a literature still dominated by adult and mixed-age series.[7,10,11]
A recent paediatric review similarly emphasises the importance of early risk stratification and recognition of organ involvement in children with dengue.[16]
Incidence and Spectrum of Renal Involvement
In this study, 42.1% of children had evidence of renal involvement, markedly higher than the 9.8% (of 316 children) incidence reported by Sultana et al. from Bangladesh.[4] The higher burden in the present study likely reflects inclusion of a greater proportion of severe dengue and dengue with warning signs (87.5%) in contrast to only 33.5% patients with DHF and DSS in the study by Sultana et al., wherein involvement clustered predominantly among these cases.[4]
Among the various renal abnormalities, haematuria (predominantly microscopic) and low-grade proteinuria were common, while AKI occurred in 17.8% of the total cohort, with most cases in KDIGO Stages 1 or 2 and only a single child requiring dialysis. This pattern mirrors earlier paediatric observations where transient proteinuria and haematuria dominate the spectrum, with a smaller subset progressing to AKI and is biologically congruent with mechanisms ranging from hemodynamic instability and tubular injury to immune-mediated glomerular involvement and dengue-associated glomerulonephritis.[4,5,17] Rajan et al.[5] similarly reported microscopic haematuria as the most common urinary abnormality (20.4%), followed by proteinuria (18%) and glucosuria (3%) among 127 Indian children with dengue requiring paediatric intensive care unit (PICU) admission.[5]
Comparison of AKI Burden with Existing Literature
The AKI frequency in this study is comparable to that of previous paediatric cohorts.[5,6] Rajan and co-workers from Chennai described AKI in 20.5% of 127 children requiring PICU admission, with staging by KDIGO criteria showing 42.3% in Stage 1, 30.7% in Stage 2 and 27% in Stage 3, which is in line with our findings.[5] Similarly, Mekangkul et al.[5] reported AKI in 21.6% of 259 hospitalised Thai children with dengue using KDIGO criteria.[6] On the contrary, compared to the study by Sultana et al.[4] (4.1%), the higher burden of AKI in the present series likely reflects inclusion of a greater proportion of severe dengue (39.5%) and dengue with warning signs (48%).[4] This is consistent with the observation of Rajan et al. that children with severe dengue contributed a significantly higher number of AKI cases.[5] Moreover, methodological differences such as diagnostic criteria (pRIFLE vs. KDIGO) likely account for disparities in reported frequencies, underscoring that standardised definitions yield higher and more consistent incidence estimates, facilitating comparability and emphasising the burden of renal complications in dengue.
Adult and mixed cohorts synthesised by several groups also demonstrate that renal injury clusters with severe dengue phenotypes, reinforcing that the observed AKI rate in this paediatric tertiary-care series likely reflects referral of more critically ill children rather than a population-level incidence.[10,18] Notably, even within this higher-risk context, the predominance of Stages 1–2 AKI suggests that early recognition and supportive management may have mitigated progression to severe kidney failure, echoing the emphasis on timely risk stratification.
Risk Factors and the Central Role of Hepatomegaly
Several clinical features—older age, severe dengue, bleeding manifestations, clinical fluid overload, neurological involvement, hepatomegaly, elevated ALT, need for PICU, blood products requirement, hypoalbuminemia and severe thrombocytopenia—were associated with renal involvement on bivariate analysis in our cohort, but only age (OR = 1.028, 95% CI 1.004–1.053) and hepatomegaly (OR = 18.5, 95% CI 1.7–198) remained independent predictors on multivariable modelling.
The age effect is consistent with broader dengue-AKI literature in which older age and DSS/DHF have repeatedly emerged as risk factors, as highlighted by Mekangkul et al. and Sultana et al.[4,6] Sultana and colleagues linked AKI to higher haematocrit and mortality, mirroring the severity-related pattern observed here.[4] Rajan and workers similarly identified severe dengue, need for colloids, inotropes, ventilation and secondary HLH as risk factors, alongside significantly elevated liver enzymes and INR in AKI, underscoring a hepato-renal axis.[5] In our cohort, the significantly higher blood urea, creatinine and elevated INR in children with renal involvement support a possible interconnection between coagulation derangement, hepatic dysfunction and renal injury. Adult and mixed-population data extend these observations: Khalil et al. reported male sex, DHF/DSS, neurological involvement and prolonged aPTT as independent AKI predictors, while Diptyanusa and Awad et al. highlighted severe dengue, multiple organ involvement, diabetes, rhabdomyolysis, coagulopathy and nephrotoxic drugs as consistent AKI determinants.[9,10]
The strong association between hepatomegaly and renal involvement is clinically intuitive but has been less systematically documented in children; recent work by Aung and co-authors identified hepatomegaly as an early-phase marker of severe dengue, suggesting that hepatic involvement may be a proxy for systemic endothelial dysfunction and capillary leak that, in turn, predispose to renal injury.[19] Moreover, liver enlargement in dengue is commonly associated with hepatic inflammation, plasma leakage, coagulopathy and multiorgan involvement. These same pathophysiological processes may predispose to renal hypoperfusion, tubular injury and AKI. In addition, severe inflammatory response, cytokine-mediated endothelial injury and hemodynamic instability may contribute to simultaneous hepatic and renal dysfunction.[7,8] Supporting this concept, Chidambaram and Kumarasamy highlighted the role of inflammatory cytokines (IL-6 and IL-8) in severe dengue, while Krishnan and Yadav demonstrated that aminotransferase elevation correlates with disease severity and adverse outcomes, reinforcing the contribution of immune-mediated hepatic involvement to multiorgan dysfunction.[20,21]
The present findings extend this concept by linking clinically evident hepatomegaly to composite renal outcomes, thereby bridging the growing literature on dengue-associated liver dysfunction. In our cohort, hepatomegaly was transient in most patients and resolved within days of supportive management, with clinical resolution observed before discharge in nearly all children. Together, these data support hepatomegaly as a simple bedside marker integrating systemic severity and renal risk in paediatric dengue.
Short-term Outcomes and Prognosis
Although mortality in our cohort was low and not statistically different between renal involvement groups, the trend towards worse outcomes in those with renal dysfunction is consistent with paediatric and mixed-age studies showing that dengue-associated AKI contributes to increased mortality and prolonged hospital stay.[5–7,10]
The predominance of non-severe proteinuria and haematuria, together with the low requirement for RRT in our cohort (only one patient), suggests that much of the renal injury may be functional or subclinical and potentially reversible. This parallels the experience described by Khalil et al., wherein 81.7% of survivors had complete recovery of renal function at discharge, with only 7% continuing to have some degree of renal dysfunction.[7] Similarly, Rajan et al. reported that among 26 children with AKI, 23 recovered and only three died (all with multiorgan dysfunction syndrome).[5]
Implications for Practice
These data reinforce the importance of systematic urine screening and serial monitoring of renal function in all hospitalised children with dengue, particularly those who are older and who have hepatomegaly or other markers of severe disease. Further paediatric studies with standardised GFR estimation, structured post-discharge follow-up and incorporation of novel renal injury biomarkers (such as neutrophil gelatinase-associated lipocalin) are needed to define the trajectory of recovery, delineate the true burden of chronic kidney sequelae and validate simple bedside predictors such as hepatomegaly for early risk stratification in diverse dengue-endemic settings.
Strengths and Limitations
The strengths of our study include its prospective design, decent sample size, use of recognised AKI diagnostic criteria and multivariable analysis to control for confounding. Limitations include a single-centre design and the lack of structured long-term follow-up to assess persistent renal sequelae. Large multi-centre studies are warranted to confirm these associations and to evaluate whether early intervention in high-risk children alters renal and overall outcomes.
Conclusion
Renal involvement is a frequent complication of paediatric dengue, with manifestations ranging from transient urinary abnormalities to AKI. Increasing age and hepatomegaly were independent predictors, highlighting hepatomegaly as a simple bedside marker of renal risk. Although most cases were mild and outcomes favourable, the high prevalence of renal abnormalities underscores the need for routine renal monitoring in children with dengue.
Supplemental material
Supplemental material for this article is available online.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
IEC/2025/AIR/85, Institutional Review Board, Venkateshwara Institute of Medical Sciences, Gajraula, Amroha, Uttar Pradesh, India.
Informed consent
Written informed consent was obtained from parents/ caregivers of all participants. Assent was obtained from children aged 7 years or above.
Credit author statement
RM: Conceptualisation, Methodology, Data curation, Formal analysis, Investigation, Writing - original draft, Visualisation.
SA: Methodology, Validation, Supervision, Writing - review & editing.
MO: Conceptualisation, Supervision, Project administration, Writing - review & editing.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article and are available on reasonable request from corresponding authors.
Use of artificial intelligence
During the preparation of this work, the author(s) used ChatGPT (OpenAI) in order to check grammar and improve language. After using this tool, the author(s) reviewed and edited the content as needed and take full responsibility for the content of the published work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.