
Abstract
Keywords
Introduction
Metatarsalgia, characterized by pain in the plantar region of the forefoot, is a prevalent condition that can significantly impair daily activities and quality of life. 1 Its etiology is multifactorial, encompassing anatomical abnormalities, biomechanical dysfunctions, and systemic conditions. 2 Notably, isolated gastrocnemius tightness has been identified as a potential contributor to forefoot pain, causing increased forefoot pressure during gait. 3
The gastrocnemius muscle, part of the triceps surae complex, crosses both the knee and ankle joints and plays a pivotal role in lower limb biomechanics. 4 Limited dorsiflexion resulting from gastrocnemius tightness can trigger compensatory mechanisms during gait, thereby increasing pressure on the forefoot. 5 This biomechanical alteration may predispose individuals to metatarsalgia. 6
Addressing gastrocnemius tightness through surgical intervention, specifically gastrocnemius recession, has been proposed as a treatment modality for metatarsalgia. 7 Several surgical techniques have been described in the literature, characterized by distinct anatomical considerations and approaches. The Strayer procedure involves a transverse incision in the posterior calf to access and release the gastrocnemius tendon at its insertion on the posterior surface of the tibia.8,9 The Baumann procedure entails an intramuscular lengthening of the gastrocnemius, through a medial approach, preserving the integrity of the aponeurosis while effectively lengthening the muscle.3,10 Proximal medial gastrocnemius release (PMGR), as described by Barouk, addresses gastrocnemius tightness through a controlled selective lengthening of the medial gastrocnemius at the popliteal fossa, preserving the Achilles tendon integrity, significantly enhancing ankle dorsiflexion and reducing postoperative morbidity.11,12 Additionally, endoscopic gastrocnemius recession utilizes minimally invasive techniques, offering reduced surgical trauma and potentially lower complication rates compared to open procedures.13,14
Despite the variety of surgical techniques available, the overall efficacy and safety profiles of gastrocnemius release procedures for metatarsalgia remain topics of ongoing investigation.6,7 This systematic review aims to critically evaluate the current literature on gastrocnemius release as a surgical treatment for metatarsalgia, focusing on patient outcomes, complication rates, and the quality of existing evidence.
Materials and methods
The review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines,
15
ensuring a thorough and systematic approach to data collection and analysis (Figure 1). This systematic review has also been registered with the International Prospective Register of Systematic Reviews (PROSPERO), under registration number CRD420251043727. PRISMA flowchart.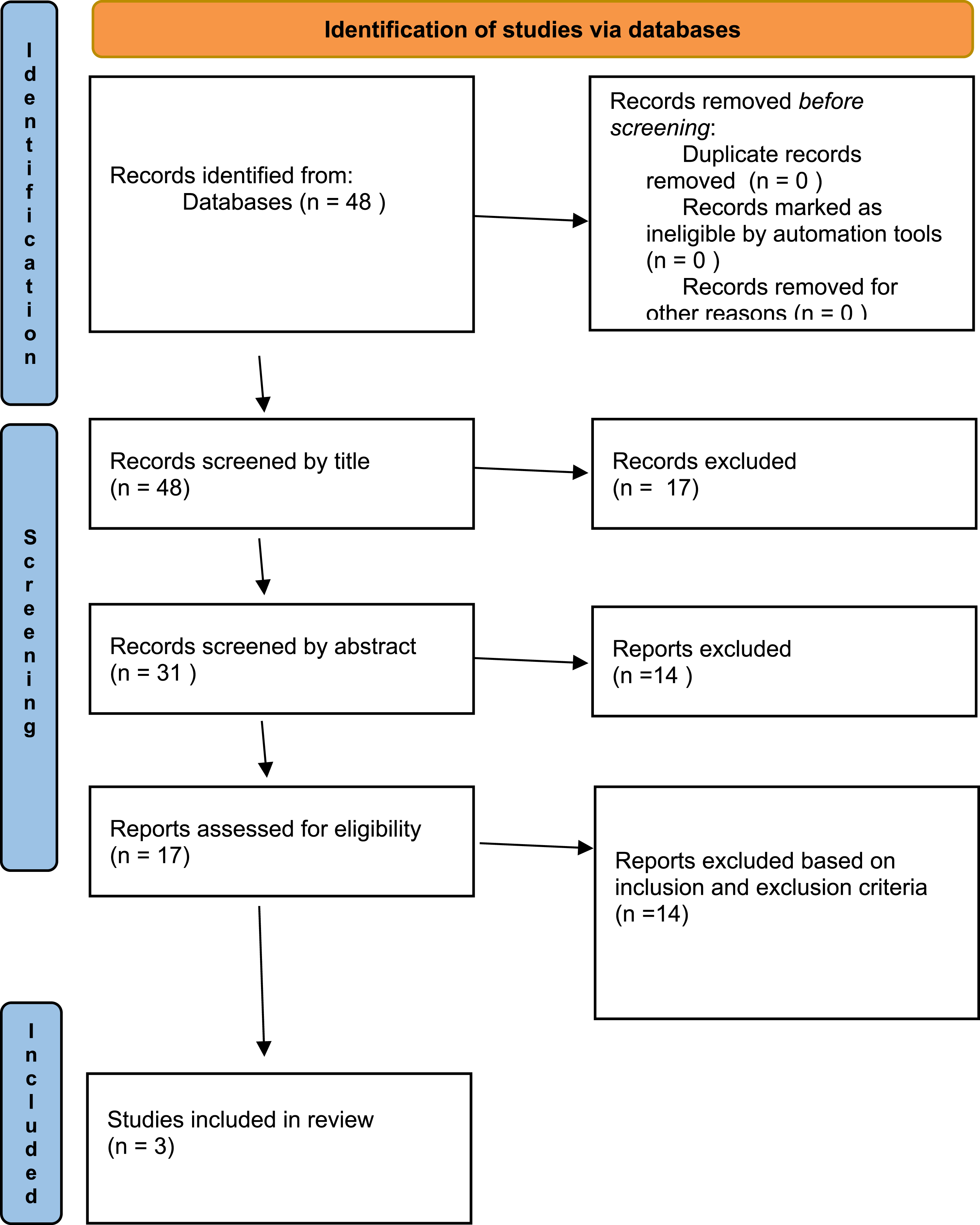
Search strategy
The search was performed across several online databases, including PubMed, Scopus, and Google Scholar. The search string used in PubMed was as follows: ‘Metatarsalgia’ AND ‘Gastrocnemius’.
We carefully examined the titles and abstracts of all retrieved articles to assess their eligibility for inclusion in the review. When there was uncertainty, the full article was retrieved for further examination. The senior author and the content area experts then obtained the full text of all articles and reviewed them to minimize any bias that could arise from preconceived opinions about the studies and their findings. This process was further enhanced by following up on the reference lists of relevant studies to identify additional articles. Two authors (A.G. and G.B.) independently reviewed the abstracts, obtaining the full texts for any abstracts that were inconclusive. Any differences between the reviewers were discussed, and if disagreements remained, the senior author (R.V.) was consulted. The reference lists of the selected articles were manually checked to identify additional relevant studies. All selected studies were then analyzed retrospectively by three authors (S.C., G.B., and G.M.), who extracted and entered the data into an Excel worksheet. Finally, the data sheet was reviewed by four authors (R.V., A.G., S.C. and G.M.), who reached an agreement on the extracted data. Additionally, three authors (S.C., G.M., and R.V.) independently evaluated the risk of bias using standardized criteria. The references of the identified papers were searched to find further relevant articles, and all journals were considered.
Inclusion and exclusion criteria
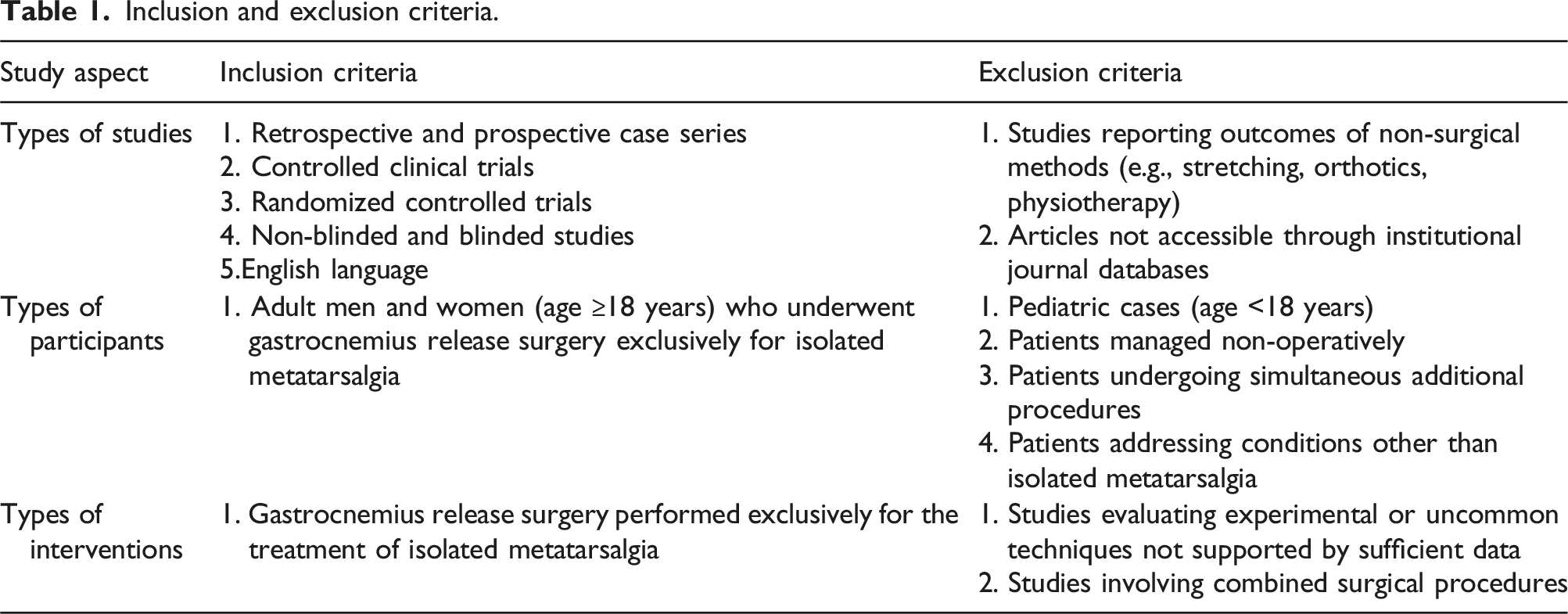
The eligibility criteria for our analysis were established to select studies that met high methodological and reporting standards. We included studies involving adult men and women aged 18 years or older who underwent gastrocnemius release surgery performed exclusively for the treatment of isolated metatarsalgia, without any concomitant additional surgical procedures. Studies that included patients undergoing simultaneous additional procedures or addressing conditions other than isolated metatarsalgia were excluded. Acceptable study designs comprised retrospective and prospective case series, controlled clinical trials, and randomized controlled trials. Only studies published in English language that reported clinical, radiological or complication outcomes with a follow-up period of at least 6 months were considered and with a minimum sample size of ten. Additionally, all articles had to be accessible through institutional or public journal databases.
Inclusion and exclusion criteria.
Data extraction and analysis
Data extraction was performed retrospectively by two independent authors (S.C. and A.G.) using a standardized Excel worksheet to ensure consistent and comprehensive data collection. Extracted data included study characteristics, patient demographics, details of surgical techniques, clinical outcomes, and follow-up durations. A third author (R.V.) independently reviewed the extracted data for accuracy and completeness. Discrepancies were resolved through consensus. To enhance reliability and minimize bias, all included studies underwent evaluation by two independent investigators.
Results
Search and literature selection
The initial electronic database search identified 48 articles.
Following the PRISMA guidelines, 15 only 3 articles9,16,17 met the inclusion criteria and were included in the review.
Of the three selected studies, two were retrospective and one was prospective. Although two studies described gastrocnemius recession, they also addressed conditions other than isolated metatarsalgia. Therefore, only data specifically about gastrocnemius release procedures performed exclusively for metatarsalgia were considered.
Patient demographics
We analyzed a total of 154 patients, among whom 112 feet were treated for isolated metatarsalgia. The mean follow-up was 37.5 months. Gender was reported in all three studies, with a total of 32 males (20.8%) and 122 females (79.2%), indicating a clear female predominance.
Age was reported in two studies, with a mean age of 51.3 years.
Demographic data (M = male, F = female).

Regarding surgical techniques, Morales-Muñoz et al. 17 performed Barouk surgery, while Molund et al. 16 and Maskill et al. 9 performed gastrocnemius recession at the musculotendinous junction. Post-operative management differed across studies:
Morales-Muñoz et al. 17 used a heel-supported shoe, allowing full weight-bearing from 2 weeks postoperatively, followed by standard flat shoes for 3 months.
Molund et al. 16 applied a plaster cast maintaining the ankle at approximately 10° dorsiflexion for 2 weeks, allowing weight-bearing as tolerated. Afterward, the plaster cast was split, and the dorsal half was utilized as a night splint for four additional weeks.
Maskill et al. 9 placed patients into pneumatic walking boots for 2 weeks, allowing weight-bearing as tolerated. After 2 weeks, patients transitioned to standard shoes and performed a home stretching program to maintain ankle range of motion. Follow-up visits occurred at 2 weeks (wound check) and again at 12 weeks.
Clinical results
Clinical Outcomes (APF = ankle plantar flexion).
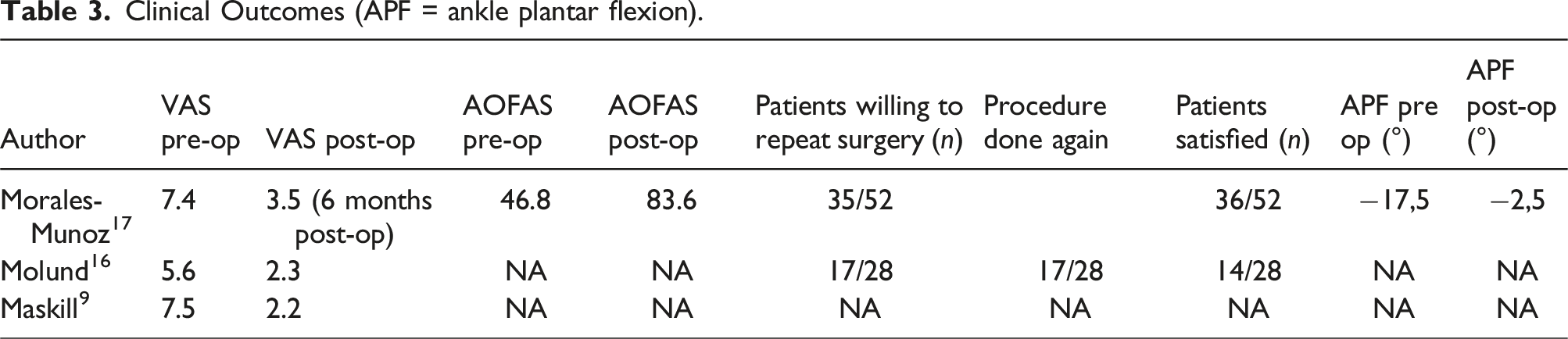
Morales-Muñoz et al. reported significant improvements in both the VAS (Visual Analogue Scale) and AOFAS (American Orthopaedic Foot and Ankle Society) scores, with VAS decreasing from 7.4 to 3.5 and AOFAS increasing from 46.8 to 83.6 at 6-month follow-up. Furthermore, 67.3% of patients (35 out of 52) stated they would undergo the procedure again, and none reported symptom worsening. A notable improvement in Ankle Plantar Flexion (APF) was also observed, with a correction from −17.5° preoperatively to −2.5° postoperatively, indicating a restoration of more physiological forefoot alignment. Ankle plantar flexion strength was preserved at follow-up. 17
Molund et al. also reported favorable clinical outcomes, with VAS scores improving from 5.6 to 2.3, and 17 out of 28 patients (60.7%) indicating they would repeat the surgery. Moreover, 17 patients rated their outcomes as excellent. 16
Maskill et al. observed a VAS reduction from 7.5 to 2.2 and an overall patient satisfaction rate of 93.1%. 9
Complications
Complications.

Morales-Muñoz et al. 17 noted mild complications in 21 of 52 patients, primarily bruising distal to the operative site, which resolved spontaneously. Four patients reported numbness of the medial gastrocnemius region, with persistent symptoms in one patient at 8-month follow-up.
Molund et al. 16 reported various complications, but data were not stratified specifically for the metatarsalgia diagnosis.
Maskill et al. 9 reported ongoing pain medication usage in 8 out of 29 patients; however, no infections or skin-related complications were noted.
Discussion
Gastrocnemius shortening is frequently associated with multiple foot disorders, including metatarsalgia. Although gastrocnemius recession is a well-established surgical technique for various foot and ankle pathologies, its effectiveness and safety specifically for metatarsalgia treatment require further investigation.3,18 Di Giovanni et al. 2 demonstrated a significant association between gastrocnemius contracture and foot pathologies, highlighting pain reduction following gastrocnemius recession in patients with isolated gastrocnemius tightness.
The gastrocnemius recession procedure has been also used as a tool to relieve pressure on the foot, specifically with diabetic foot ulcers and significant foot deformity.19,20 Multiple authors have supported this anecdotally. 21
Sammarco et al. 22 looked at patients who had undergone a gastrocnemius recession with numerous other concomitant procedures. Strength testing 2 years postoperatively showed increasing strength over a 18-month period to 82% strength relative to the unoperated contralateral limb, supporting the idea that a recession may not sacrifice significant strength. Complications associated with gastrocnemius lengthening, such as Achilles rupture, over lengthening, or prolonged postoperative course, are well known risks for a gastrocnemius recession. The biggest risk associated with this procedure is injury to the sural nerve and, to a lesser extent, skin dimpling and weakness.22–24 If appropriately observed and retracted, damage to the sural nerve should be minimized.
This systematic review aimed to critically evaluate the clinical efficacy of gastrocnemius recession for isolated metatarsalgia.
This systematic review evaluated the role of gastrocnemius recession specifically for isolated metatarsalgia, an area still lacking high-quality evidence.
All included studies documented clinical improvements following surgery, supporting its potential value in reducing forefoot pain. However, detailed stratification by diagnosis was limited in most studies. Only Morales-Munoz et al. 17 provided comprehensive outcome data specifically for isolated metatrsalgia, while other studies grouped result under broader indications. This limits generalizability and highlights the need for focudes research. The multifactorial nature of metatarsalgia was evident, as up to 30% of patients required additional forefoot procedures despite clinical improvement. This suggests that isolated gastrocnemius recession may not fully address all biomechanical contributors and should be considered as part of a broader treatment algorithm.
Additional studies have further corroborated these findings. Cychosz et al. 7 systematically reviewed the role of gastrocnemius recession across multiple forefoot disorders, highlighting a substantial reduction in forefoot pressures postoperatively, thus supporting the biomechanical rationale for the procedure. Similarly, Iborra et al. 25 introduced innovative minimally invasive techniques such as ultrasound-guided needle-based gastrocnemius lengthening, demonstrating promising early clinical outcomes in managing plantar forefoot pain with minimal morbidity.
An essential factor highlighted by our review is the variability of surgical techniques employed by the different authors. Morales-Muñoz et al. 17 performed recession at the proximal medial gastrocnemius region, while Molund et al. 16 utilized a modified Strayer technique, 8 and Maskill et al. 9 executed recession at the musculotendinous junction. Literature indicates different biomechanical outcomes depending on the specific gastrocnemius recession technique, underscoring the need for standardized protocols to improve outcome comparability and clinical decision-making.4,13,26
In this regard, Chimera et al. 26 emphasized that proximal gastrocnemius release tends to maintain better calf strength postoperatively compared to distal techniques, possibly favoring functional recovery, particularly in active individuals. Furthermore, Saxena et al. 13 reported that endoscopic gastrocnemius recession allows for a quicker return to activity with a low incidence of complications, supporting the growing trend toward minimally invasive approaches.
Postoperative management protocols varied across studies and may have influenced outcomes. The lack of standardized rehabilitation strategies makes it difficult to compare clinical results.
Consensus guidelines on weight-baring progression, stretching protocols and activity resumption could optimize recovery and improved patient satisfaction.
Additionally, the variability in postoperative management protocols across studies could have influenced patient outcomes, highlighting the necessity for consensus and standardization in postoperative care following gastrocnemius recession. 27
Recent evidence by Holtmann et al. 27 reinforces the role of early mobilization and structured rehabilitation programs in enhancing ankle dorsiflexion and patient satisfaction after gastrocnemius recession. Future guidelines should integrate specific postoperative pathways to optimize functional recovery and minimize complications.
Future research should focus on prospective, randomized trials with standardized surgical techniques and validated outcome measures to provide clearer insights into the efficacy and safety of gastrocnemius recession specifically for metatarsalgia. 25
In conclusion, while existing studies suggest gastrocnemius recession may be beneficial in selected patients with isolated metatarsalgia, the current evidence is insufficient to establish it as a standalone solution. High-quality studies with standardized designs are needed to better define its role in clinical practice.
Study limitations
This systematic review has several limitations that should be considered. The small number of eligible studies — only three retrospective analyses — limits the overall strength of the evidence. Significant heterogeneity in surgical techniques, postoperative protocols, and outcome measures complicates direct comparisons and reduces the generalizability of the results. Moreover, the absence of randomized controlled trials and prospective comparative studies prevents definitive conclusions regarding the efficacy of gastrocnemius recession for isolated metatarsalgia. Incomplete reporting of patient demographics, such as age and gender, further restricts subgroup analyses. The relatively short follow-up periods and the widespread use of non-standardized, non-validated patient-reported outcome measures also affect the reliability of the findings. Future research should focus on high-quality, prospective randomized studies with standardized surgical techniques and validated outcome assessments to better define the role of gastrocnemius recession in the management of isolated metatarsalgia.
Conclusion
Gastrocnemius recession is a promising surgical option for the management of isolated metatarsalgia, offering significant pain relief, high patient satisfaction, and a low complication rate. However, due to the multifactorial nature of metatarsalgia, adjunctive procedures may sometimes be necessary to address residual biomechanical issues. The current evidence is limited by the retrospective design of available studies, heterogeneity in surgical techniques, and inconsistent use of validated outcome measures. Future high-quality, prospective randomized studies are needed to better define indications, optimize surgical techniques, and establish standardized postoperative protocols to improve patient outcomes. 28
Footnotes
Author Contributions
All authors have contributed to the conception and design of this study, acquisition of data, in drafting the article, in its revision, and all the authors approved the final draft of the submitted article. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Ethical statement
Data Availability Statement
All the data we analyzed and tables we compiled are available for any clarification.