
Abstract
The rat model has been extensively utilized in numerous studies on the rotator cuff. This review analyzes these studies and categorizes their findings into three primary areas: (1) the effects of external interventions on the intact shoulder/supraspinatus tendon, (2) surgical healing under varied conditions, and (3) the combined impact of surgery and external interventions on the biological healing response of the supraspinatus tendon. These studies consistently highlight the Sprague-Dawley rat as a valuable animal model. Several key themes emerge from research on rat shoulders. First, both intrinsic and extrinsic mechanisms contribute to changes in the supraspinatus tendon. Second, many studies report suboptimal tendon-bone healing, emphasizing the need for improved surgical repair techniques. Timely repair of acute tears facilitates smoother surgeries, enhances healing outcomes, and reduces the risk of failure. Additionally, reduced post-surgical activity levels have been associated with superior healing. Finally, ongoing research using this model continues to advance our understanding of the complex rotator cuff healing process.
Introduction
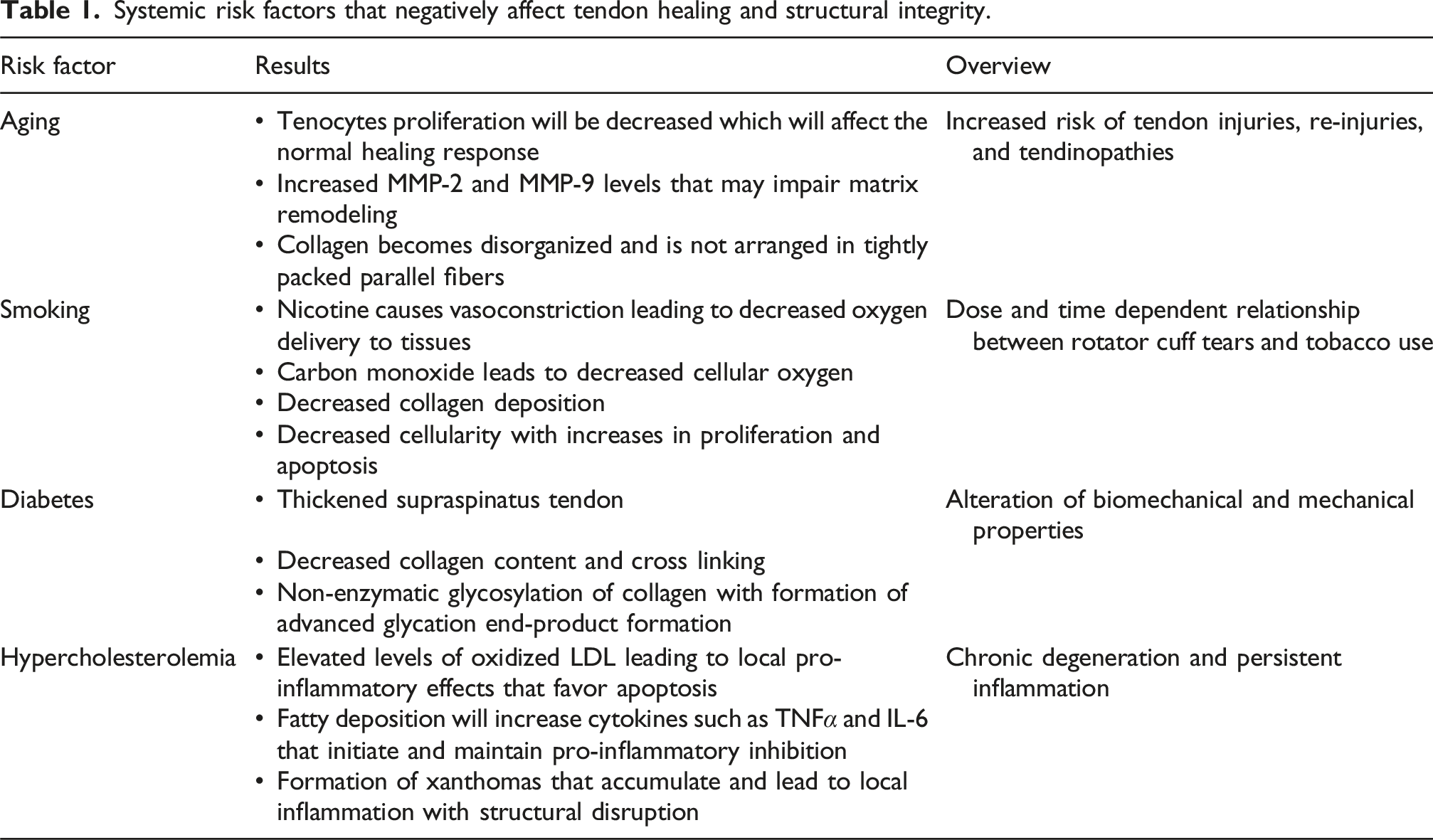
Systemic risk factors that negatively affect tendon healing and structural integrity.

Schematic representation of the rat rotator cuff model. The magnified inset highlights the anatomical location of the supraspinatus tendon attaching to the humeral head, with a full-thickness tear illustrated in red. This model is commonly used in preclinical research due to the anatomical and biomechanical similarities between the rat and human shoulder.
In 1996, Soslowsky et al. 3 studied 33 different potential animal models based on 34 different criteria. Their research concluded that the Sprague-Dawley rat emerged as the most suitable animal model due to its similarities in bony configuration, particularly in the coracoacromial arch, muscular anatomy, and articulations and motions. Practical considerations such as cost and ease of handling further supported its selection. However, ongoing studies continue to investigate alternative animal models, including pigs, 4 sheep, 5 rabbits, 6 and other mammals, to better understand the etiology and pathogenesis of rotator cuff tears (RCTs) and assess novel treatment strategies. It is important to recognize that no single animal model can fully replicate all aspects of the human shoulder. Each model has distinct advantages and limitations that must be carefully considered based on the specific research question.
For example, the mouse model presents several advantages over larger animals while remaining a cost-effective option similar to rats. It has been particularly useful in demonstrating the pathophysiological changes associated with chronic rotator cuff tears, such as fatty infiltration, muscle atrophy, and fibrosis, opening avenues for further research. 7 The application of the rat model to study the supraspinatus in relation to the human shoulder has shown promising results, as it allows for the induction of reproducible, controlled injuries in the rotator cuff, providing valuable insights into RCTs.
Over the past two decades, rat models have been widely utilized in studies examining the rotator cuff. This review aims to analyze these published studies and categorize their findings into three major areas: (1) disease models that induce rotator cuff injury, (2) studies investigating surgical healing under various conditions, and (3) research combining surgical intervention with external treatments to enhance the biological healing response.
Mechanisms of injury studies
The first class of experiments using the rat model supraspinatus involved external interventions that induced injury to the tendon. These studies utilized chemical (enzymes, steroids, and cells) or extrinsic (overuse or compression) mechanisms of injury. Muscle overuse in all studies was induced by downhill treadmill running to simulate a repetitive overuse model similar to human high-repetition activities such as swimming. Compression effects were achieved by using some mechanical means to eliminate or reduce the subacromial space.
Chemical interventions – chemical alterations of subacromial space
Several studies have assessed the impact of corticosteroids on the rotator cuff, yielding consistent findings. Repeated injections of triamcinolone, methylprednisolone, and betamethasone have demonstrated increased focal inflammation, tissue necrosis, and collagen fragmentation. Histologically, corticosteroid injections lead to loss of cellular orientation, a heightened polygonal and flattened appearance of cells, and reduced vascular proliferation. 8 However, these effects are transient, with studies indicating a return to normal cell morphology within 21 days post-injection. 9 In a biomechanical comparison study investigating the effects of steroids on both healthy shoulders and those with acute tears, their conclusions aligned with previous research, indicating that steroids significantly weaken an injured cuff compared to controls. Nevertheless, this effect is temporary, as a return to control-level biomechanical properties is observed within 3 weeks. 10 Moreover, steroids exhibit a dose-dependent effect on rotator cuff function, with increasing concentrations of corticosteroid injections having a more pronounced impact on the mechanical resistance of rotator cuff tears. 8
External interventions – overuse/compression model
In this group of studies, Schneeberger et al. 11 considered the mechanical effects of subacromial impingement on intact rotator cuffs. By artificially narrowing the joint space, they showed that more narrowing and a longer time with impingement leads to larger tears. Their analysis supported the hypothesis that subacromial impingement was not the primary cause of cuff tears involving the articular side of tendon but may be the primary cause of bursal side tears. Soslowsky 12 examined extrinsic overuse by creating an overuse protocol consisting of decline treadmill running simulating a swimmer’s workout. His experiment demonstrated that 4 weeks of overuse was enough time to cause changes in the tissue, resulting in lower-quality tendon that could not regain its original mechanical properties within the given endpoint. In an additional study, Soslowsky 13 examined compression and overuse together, finding that extrinsic compression had a significant effect when combined with overuse, but that without overuse, compression alone may be insufficient to cause tendinosis. Jelinsky et al. 14 built upon the rat overuse model and evaluated the role of rest in treating overuse injury. This study showed that the gene expression and biochemical composition returned to near-normal levels with as little as 2 weeks of rest in the overuse model. Using this overuse model, a subset of studies examined various cytokines that could be markers of tendinopathy or targets for prevention.
Perry et al. 15 examined the levels of inflammatory and angiogenic markers with overuse and found that FLAP and COX-2 possibly represent an ongoing adaptation to overuse, while VEGF and vWF reveal that angiogenesis occurs early and continues throughout overuse. Szomor et al. 16 investigated nitric oxide synthase (NOS) isoforms in an overuse exercise experiment, and results suggested that nitric oxide (NO) was involved in the tissue response to overuse. Millar used the overuse model in two uniquely designed studies comparing the results with human tendon samples for correlation. In that study, 17 they suggest that pro-inflammatory cytokines and apoptotic genes may play a role in tendinopathy. Another study 18 of the same design confirmed increased levels of heat shock protein and apoptotic genes in both human tears and exercised rats, suggesting that overuse may lead to the upregulation of these proteins and genes and, ultimately, to degeneration and tendinopathy. Similarly, Archambault et al. 19 examined the expression of cartilage markers in overuse and discovered that repetitive loading and compression of the supraspinatus tendon led to increased cartilage gene expression, suggesting conversion to a fibrocartilage phenotype. They investigated in rats with ovarectomies if improving bone density at the rotator cuff footprint would strengthen the failure stress of the supraspinatus tendon and found that the bisphosphonate treated group had greater bone density, greater failure stress, and improved bone density at the rotator cuff footprint enhancing supraspinatus failure stress. 20 These injury-inducing studies may lead the way for more research in preventative medicine for rotator cuff injuries.
External interventions - combined model
Both Soslowsky 13 and Carpenter 21 studied intrinsic plus extrinsic mechanisms of injury using collagenase and/or compression. Both found that both intrinsic and extrinsic models can induce change in the rat supraspinatus tendon. Clinically, the significance of these papers was that they confirm theories and/or reaffirm current knowledge. For example, repetitive steroid use can negatively affect the tendon, subacromial impingement may lead to cuff tears, and overuse leads to tissue inflammation, while rest allows for recovery. They tell us that we have a clear understanding of the mechanisms and pathophysiology behind rotator cuff tendinitis and tears. Furthermore, a subset of these studies begins to examine injury prevention by identifying potential targets for intervention to help avoid tears and surgery altogether.
Surgery and healing
The following studies were designed to evaluate an acute or chronic model of injury with surgical repair, with focus on assessing the healing process.
Surgery and healing – supraspinatus defect injury model
One of the first studies looking at the rat rotator cuff model, published in 1998, demonstrated defect healing over time in the normal supraspinatus tendons and tendons with an intrinsically reduced capacity to heal (via freezing with liquid nitrogen). 21 This histologic study showed that there were histologic improvements that happened over 12 weeks, but not complete healing, validating the rat supraspinatus defect model for to examine surgical repair and healing.
Surgery and healing – supraspinatus repair injury model
Thomopoulos et al. 22 evaluated the healing response of the acute supraspinatus tear after immediate surgical single suture repair to show there was a response to injury yet poor healing at the tendon to bone insertion. Many other surgical protocol experiments examined the best post-operative course of action. These studies set out to determine where along the spectrum of activity level was best for recovery – ranging from total immobilization to cage activity to early exercise. Sarver 23 measured mechanics with and without immobilization and discovered that, while there is an increase in rotational stiffness due to immobilization, it is transient and does not outweigh the benefits of improved healing. Studies by Thomopoulos24,25 concluded that insertion sites treated with decreased activity healed better than those with increased activity. While exercise increased matrix production, it was mostly scar tissue with poor organization and low material properties. Gilotra 26 examined the effect of load and the role of the mechanical environment on healing. Botox was used to paralyze the supraspinatus of one group of rats post-operatively compared to a group of casted rats. The casted rats had greater scar volume and cross-sectional area leading to the conclusion that complete load removal was detrimental to healing, particularly when in combination with immobilization. A related study by Gimbel and colleagues 27 found that immobilization had a positive effect on tendon to bone healing by improving collagen organization and mechanical properties. Recently, Peltz et al. 28 set out to examine the potential role of passive motion on joint mechanics post-operatively compared to immobilization. Their results showed that both total range of motion and joint stiffness were better in the immobilized group compared to both passive motion groups. The authors hypothesized this difference was due to increased scar formation in the motion groups, as there was no difference in collagen organization or mechanical properties across the groups.
One subset of surgical studies considered the effects of torn rotator cuff tendons on the remaining intact structures. The first study by Perry 29 examined various combinations of tendon detachments including supraspinatus, supraspinatus and infraspinatus, and supraspinatus plus subscapularis. As expected, they noted that the intact tendons had decreased mechanical properties and increased cross-sectional area over time. In a slightly different study, Peltz et al. 30 examined the effects of a tendon tear on the biceps tendon. Similar to the previous study, they found that the tendon had increased cross-sectional area and decreased modulus, with more significant changes with greater defects. These studies support the thinking regarding the evolution of pathology created by a rotator cuff tear and mimic our findings in the human population. To further evaluate the tendon healing environment, Wurgler-Hauri 31 examined the temporal expression of eight different growth factors and found an increase in expression of all of these growth factors at 1 week with a return to undetectable levels at sixteen weeks. The authors noted the importance of growth factors in the healing process as, for the first time, they qualitatively demonstrated these growth factor effects over time. Galatz et al. 32 determined the role of collagen types I and III, and TGF- β on tendon to bone healing. Capillary proliferation began at 3 days and reached a maximum at 7 days, at which time fibroblast proliferation began, before peaking at 10 days. Biomechanic results showed both ultimate force and stiffness increased over time, and relaxation force did not change with time. Type I and III collagen mRNA were increased at 10 days, then decreased closer to normal while TGFβ1 mRNA localized to scar tissue, the insertion site, and the articular surface.
Surgery and healing – supraspinatus detachment injury model
In these studies, the supraspinatus tendon was sharply and fully detached, but not repaired. The tendon was allowed to freely retract, creating a model more consistent with a chronic tear. Gimbel et al. 33 showed that in this model, histological and biomechanical properties followed a pattern of dramatic early response with improvement over time. The tear space filled with scar tissue with the late time points revealed a larger, stiffer tendon consistent with that seen in a chronic injury. Later, Barton et al. 34 examined the time course of changes to the supraspinatus in a tendon detachment injury, attempting to determine if the potential changes recapitulate those found in muscles from human patients. Examination revealed a shoulder model consistent with chronic injury – the musculotendinous unit was retracted, and disorganized scar tissue was present but decreased over time. Additionally, muscle mass decreased by the first week and remained through 4 weeks. By 8 weeks, muscle mass returned to normal, likely due to a return of load via scar adhesions. Under the same model, Gimbel’s 35 biomechanical analysis revealed increased stiffness for all injury groups relative to control. Peak repair tension, equilibrium repair tension, and repair distance increased rapidly after detachment during the first 2 weeks and continued to increase with time. This series of studies confirmed that repair should be considered early after the onset of symptoms of a rotator cuff tear. Yokota et al. 36 designed a study in the same manner, but examined molecular biology as well. Morphology results were consistent with other studies. Their molecular biology data was consistent with that seen in human studies and indicated that the molecular composition of tendon and scar tissue changed drastically initially and remained altered for months, which may explain why chronic tears heal differently than acute tears.
Surgery and healing – supraspinatus detachment delayed repair injury model
Galatz et al., 37 examined the biomechanical properties, histology, and bone density of the tendon-bone repair site after both acute and delayed repair. This supported the theory that rotator cuff healing is inferior when there is a delay between the time of injury and repair. This was likely due to the stiffening of the tendon during the delay period before repair, and the deterioration of the repair over time. Also, the changes in tendon properties and bone loss may contribute to the poor healing noted. Later, Gimbel et al. 38 also examined the effects of delayed repair. They found that repair tension increased over the delay time. This is a critical finding because an increase in tension can have detrimental effect on the failure properties of the tendon and may stimulate the production of scar tissue. Lin et al. 39 began to examine this in their experiment using bipolar radiofrequency energy (bRFE) with a delayed repair of acute supraspinatus tears. Their study showed no statistically significant difference when using bRFE at their study parameters.
This second category of studies revealed additional science behind rotator cuff tears and allowed for comparison between acute and chronic tears. They showed us which growth factors play a role in healing and scar formation and provide an opportunity for future research and the potential to improve the results of repairs. Clinically, they tell us that early intervention and repair of a torn tendon is key not only for surgical success, but also to spare the remaining tendons from wear. Also, they tell us that there is a balance of post-operative management of activity level, with immediate immobilization, yet perhaps allowing for some loading to allow for better outcomes.
Surgery combined with external intervention
This third category of studies consisted of surgery with added interventions to examine their ability to aid or hinder healing.
Surgery combined with external chemical intervention
Cohen et al. 40 determined if traditional NSAIDs and COX-2 inhibitors would impair tendon to bone healing using celecoxib or indomethacin post-op. The drug group tendons were less robust and organized with lower failure loads compared to controls. Connizzo 41 further studied NSAID administration, specifically the impact of Ibuprofen’s timing of administration on early and delayed tendon healing. As expected, Ibuprofen was detrimental to healing when administered early but not delayed. In a related study, Galatz et al. 42 investigated the effects of nicotine on rotator cuff repairs. Histological results indicated that 1acute inflammation was persistent in the nicotine group, suggesting that nicotine causes a delay in tendon to bone healing. Chronic inflammation and decreased cellular proliferation was postulated to explain the inferior biomechanical properties observed. Wei 43 characterized the molecular response to acute injury and corticosteroid treatment by using the collagen type I to type III ratio using the infraspinatus tendon. This study showed that a single steroid dose does noy alter the acute phase response of an injured tendon, but the same dose in uninjured tendons initiates a response equivalent to a structural injury. Using the same design, Thomopoulos 44 investigated whether a repaired rotator cuff’s healing capacity could be enhanced with the addition of growth factors from an exogenous clot placed in the defect space of repaired shoulders. Analysis showed that adding fibrin clot (which remained present in all shoulders at 3 weeks and in half the specimens at 6 weeks) was detrimental at 3 weeks and not beneficial at longer time points. A subset of the external additive studies specifically examined various growth factors. Uggen et al., 45 used the surgical model plus a gene-modified tendon tissue construct using rat tendon fibroblasts transduced with either IGF-1 or PDGF-β. The experimental group with PDGF-β had near complete restoration, showing re-establishment of the normal crimp pattern and collagen bundle longitudinal alignment. This study demonstrated that tendon fibroblasts can be engineered to deliver therapeutic peptides locally to stimulate repair, and that the bioactive implant is effective in repair of the rotator cuff injury. Murray et al. 46 conducted a study using CDMP-2 showing stronger repairs and more organized healing with the addition of the growth factor. More recently, Gulotta 47 tried using bone marrow-derived mesenchymal stem cells to see if they help healing in the surgical model. They found no difference in collagen organization or biomechanical analysis with the MSCs, concluding that despite evidence of MSC metabolic activity, there was no improvement in healing. Another publication by Ide et al. 48 looked at FGF-2 in a fibrin sealant as an adjunct to healing the surgical repair. Histology showed improved scores, and biomechanics exhibited greater strength at early time points. This study revealed the possibility of FGF-2 as a clinically significant growth factor that accelerates early tendon-bone interface remodeling. Additionally, more recent studies have evaluated clinically translatable biologic adjuncts such as platelet-rich plasma (PRP) and erythropoietin (EPO). Hapa et al. 49 demonstrated that PRP treatment reduced inflammation and vascularity at both time points, improved tendon continuity at 2 weeks, and resulted in greater biomechanical strength at 2 weeks compared to controls, whereas greater new bone formation was observed in controls at 4 weeks. Similarly, Oda et al. 50 reported that PRP combined with a stem cell–seeded tendon hydrogel improved biomechanical outcomes in a rat chronic rotator cuff model, though no dose-dependent or synergistic effects were observed with higher PRP concentrations. Oztermeli et al. 51 revealed systemic EPO administration enhances rotator cuff healing in rats, demonstrating improved early biomechanical strength and superior late histopathologic outcomes compared to local EPO and control groups.
Surgery combined with patches and grafts
In patients with risk factors such as a massive rotator cuff tear, 52 advanced age, 53 or muscle atrophy, 54 the tendon-bone interface may experience challenges in healing. To address this, the use of patches or grafts has been suggested. These interventions are thought to enhance cell interaction, boost the presence of growth factors required for healing, and provide additional extracellular matrix support, thereby bridging the tendon defect and promoting full-width tendon regeneration. 55 Zalavras et al. 56 first evaluated the efficacy of a small intestine submucosa (SIS) xenograft intestine patch for a supraspinatus defect. Under microscopic inspection, the SIS group revealed fibroblast ingrowth, neovascularization, and collagenous ECM, and biomechanics were improved. This data provided evidence that the xenograft SIS patch promoted tissue ingrowth and that ultimate load-to-failure approached normal at sixteen weeks. In a similar model, a SIS patch is used to replace a supraspinatus surgical defect using both acute and delayed repairs. In chronic repairs, this SIS patch significantly reduced the cross-sectional area of the healing tendon and increased the modulus.
Moving away from xenografts, there has been a big push for bioengineered patches due to having less reactivity. Ide et al. 57 experimented with acellular dermal matrix (ADM) grafts for bridging large defect cuff tears and proved the potential of ADM grafts for reconstruction of large rotator cuff defects. Despite showing the formation of new enthesis, there was poor cellular organization and biomechanical strength, necessitating experiments with other methods. Other materials such as non-resorbable polycarbonate polyurethane patch also demonstrated excellent biocompatibility with incorporation of the patch with organized collagenous tissue, no hypertrophic scar tissue, and no inflammatory changes. 55 However, in a study comparing non-Dualmesh, Seprafilm, silicone sutured over the rotator cuff at 6 weeks, they found diffuse fibrosis and collagen accumulation at the site compared to the control groups. 58
Biodegradable materials for rotator cuff repairs have also been studied in recent years. Polycaprolactone (PCL) electrospun nanofibers have been shown to have a higher electrical stimulus effect of topographical and electrical cues reducing gaps in muscle fibers. 59 These bioengineered patches are fabricated with mechanical properties to match native tendons and biological effects to promote tendon-bone healing. In a separate study, researchers found that grafting kartogenin onto polyurea/gelatin composite nanofibrous patches significantly enhanced tissue cellularity and collagen alignment. This approach also accelerated fibrocartilage regeneration and bolstered the biomechanical strength of the repaired enthesis. 60
Iwata et al. 61 investigated the utilization of autologous tissue grafts for repairing significant cuff defects. They devised a grafting model using fluorescent protein transgenic rats and employed tendons from these rats to replicate an autologous transplant. Their findings revealed that host cells were responsible for initiating proliferation and infiltration into the graft, while the graft cells actually decreased over time. This discovery underscores the pivotal role of host cells in rotator cuff remodeling, rather than the implanted graft cells.
In conclusion, this final set of studies delved into the clinical aspects of supraspinatus tears, focusing on both current and future management strategies. They confirmed that nicotine, NSAIDs, and steroids have adverse effects on tendons and healing. Additionally, they highlighted the potential benefits of certain growth factors, such as PDGF-B and IGF-1, in enhancing surgical repair outcomes. Furthermore, the studies demonstrated improved operative results using various patches, including SIS, polycarbonate polyurethane, and ADM patches. Importantly, these findings underscored the leading role of host cells in tendon repair, suggesting that the patch may serve more as a scaffold than a permanent structure.
Discussion
Summary table of cited studies.

Phases of tendon healing with associated cellular, molecular, and collagen responses.

Experiments exploring overuse found that compression alone does not cause injury but can predispose to injury when combined with overuse. The level of subacromial impingement correlates with damage to the bursal side of the tendon. Overuse alone can also cause injury and a biological response, leading to increased levels of NO, FLAP, COX-2, VWF, and VEGF. Many studies showed poor tendon-bone healing, highlighting the importance of strong surgical repair. Repairing an acute tear earlier results in easier surgery, improved healing, and a lower risk of failure, with decreased post-op activity correlating with better healing.
Muscle-based gene therapy and implantable bioactive fibroblasts delivering therapeutic peptides may be beneficial. SIS and ADM patches encourage tissue ingrowth for large defects, while the polycarbonate polyurethane patch shows good biocompatibility with no inflammatory changes. These experimental treatments hold promise for superior rotator cuff repair.
Based on the conclusion that immobilization is appropriate post-operatively, treatments that only improve initial results may not have clinical benefits when patients are still not using their shoulders. However, treatments promoting early healing may allow for shorter immobilization periods, potentially leading to improved outcomes. These subjects warrant further evaluation in future studies.
Additionally, it is important to consider that in many countries, the use of animals in biomedical research is declining due to increasing ethical concerns, regulatory changes, and the development of alternative research methods. Although animal models have historically been essential for understanding disease mechanisms and testing therapies, their limitations, including species differences and translational challenges, have encouraged the exploration of alternative approaches. Guimarães emphasizes both the advantages and drawbacks of animal models while highlighting emerging technologies such as organoids and organ-on-chip systems. 62 Similarly, Vashishat et al. describe modern alternatives including stem cell–based models, 3D bioprinting, and computational simulations that aim to improve human relevance while supporting the principles of reduction, refinement, and replacement (3 Rs) in biomedical research. 63
Conclusion
Injury to the rotator cuff is a prevalent orthopedic concern, and research has significantly advanced our understanding of it. The rat shoulder model remains a crucial tool in studying this condition. Current literature indicates a strong focus on enhancing surgical repairs and healing, as surgeons strive for better outcomes. Future experiments using this animal model will likely contribute to a deeper understanding of rotator cuff pathophysiology, while advancements in tissue engineering are expected to enhance supraspinatus healing. The evolving knowledge of targeted therapies and techniques will likely be applied to improving care for human shoulders in the future.
Footnotes
Authors’ contributions
WF conceived the study, WF and TV designed the methodology, WF. / YR. / GK. Did writing of the original draft, all authors contributed to review and editing, TV supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.