
Abstract
Purpose
Extra-articular femoral or tibial malunion can distort anatomical landmarks, compromise the reliability of conventional alignment guides, and complicate total knee arthroplasty (TKA). Robotic-assisted TKA (RA-TKA) may improve the precision and reproducibility of bone preparation and component positioning in these anatomically challenging cases. This study reports one-year clinical and radiographic outcomes after single-stage RA-TKA performed without corrective osteotomy in patients with post-traumatic extra-articular deformities.
Methods
This retrospective case series included nine patients (ten knees; one bilateral case) with symptomatic Kellgren–Lawrence grade 4 post-traumatic knee arthritis and associated extra-articular deformity who underwent CT-based RA-TKA using the Robotic Arm Interactive Orthopedic System (RIO; Mako SmartRobotics™, Stryker). Clinical outcomes included Knee Society Score (KSS 2011), Knee Injury and Osteoarthritis Outcome Score (KOOS), visual analogue scale (VAS) pain, and range of motion (ROM) assessed preoperatively and postoperatively at 2 weeks, 6 weeks, 3 months, and 1 year. Radiographic alignment was assessed using Hip–Knee–Ankle (HKA) angle on scanograms and arithmetic hip–knee–ankle angle (aHKA) derived from CT-based planning and intraoperative console values.
Results
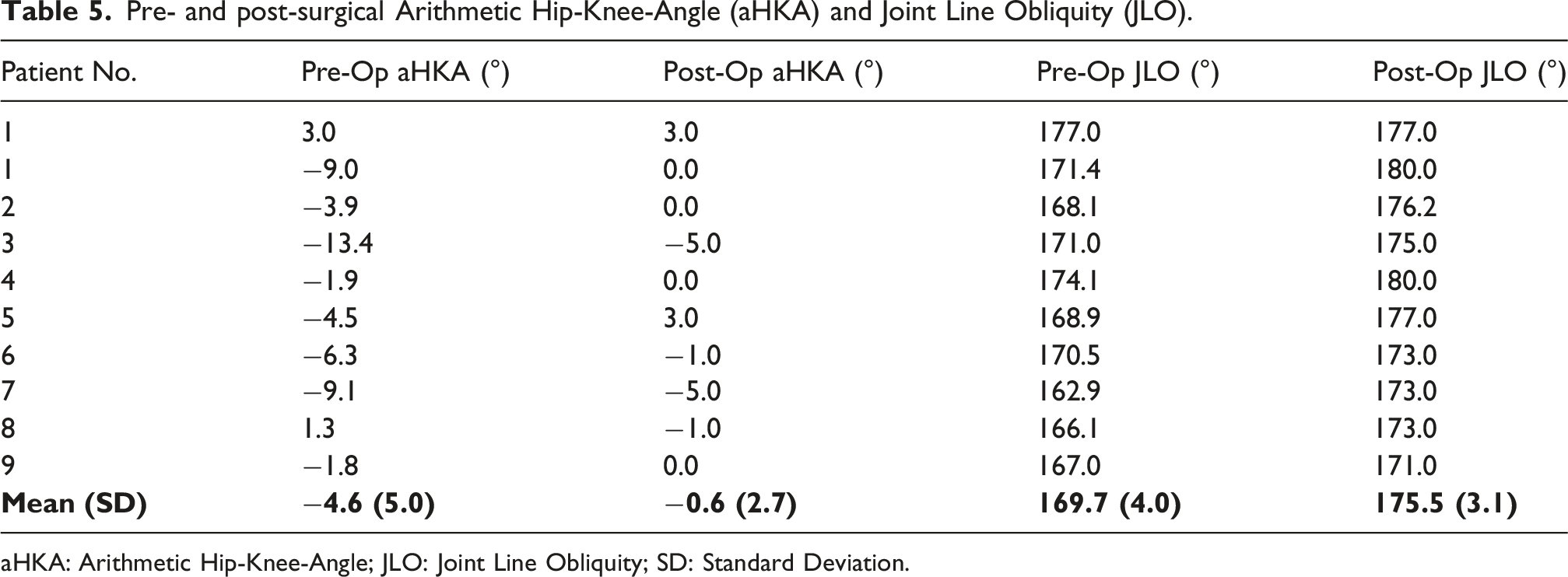
Mean HKA improved from 168.3° ± 3.8° preoperatively to 177.7° ± 1.4° postoperatively (mean correction 9.4° ± 2.8° toward neutral). Mean aHKA improved from −4.6° ± 5.0° to −0.6° ± 2.7° (mean correction +4.0°). Mean ROM increased from 95.5° ± 21.7° preoperatively to 119.5° ± 17.4° at 1 year. PROMs improved across timepoints. No major complications, including tracker pin site infection or periprosthetic fracture, were observed.
Conclusion
In selected patients with post-traumatic extra-articular deformity deemed suitable for intra-articular compensation, single-stage RA-TKA without corrective osteotomy achieved consistent coronal alignment correction toward neutral and meaningful improvements in pain, ROM, and patient-reported outcomes at 1 year.
Keywords
Introduction
Extra-articular femoral or tibial malunion can produce clinically important coronal and/or sagittal plane deformity that alters load distribution across the knee joint, accelerates post-traumatic degeneration, and complicates reconstruction once end-stage osteoarthritis develops. These cases are widely recognised as technically demanding because deformity outside the joint can distort landmarks, limit the reliability of conventional intramedullary/extramedullary guides, and increase the risk of residual malalignment or imbalance if planning and execution are not meticulous.1–3
Total knee arthroplasty (TKA) demonstrates durable long-term survivorship in degenerative arthritis, with pooled evidence suggesting many implants remain functional beyond two decades in registry data.4,5 However, in the setting of extra-articular deformity, achieving satisfactory limb alignment, joint-line orientation, and soft-tissue balance may require more complex strategies such as intra-articular compensatory resections, staged or concomitant corrective osteotomy, and/or use of increased implant constraint depending on deformity magnitude, location, and ligamentous competency.1–3,6–10 Osteotomy-based strategies can restore alignment reliably but add surgical insult, prolong rehabilitation, and introduce osteotomy-specific complications.6–10
Robotic-assisted TKA (RA-TKA) has been developed to improve the precision and reproducibility of bone preparation and component positioning, and it may be particularly useful in anatomically challenging cases where conventional instrumentation is less reliable, including extra-articular deformity.11–14 We therefore present a case series of patients with post-traumatic extra-articular deformities treated using single-stage RA-TKA without additional corrective osteotomy, reporting short-term clinical and radiographic outcomes at 1 year.
Materials and methods
Patient selection
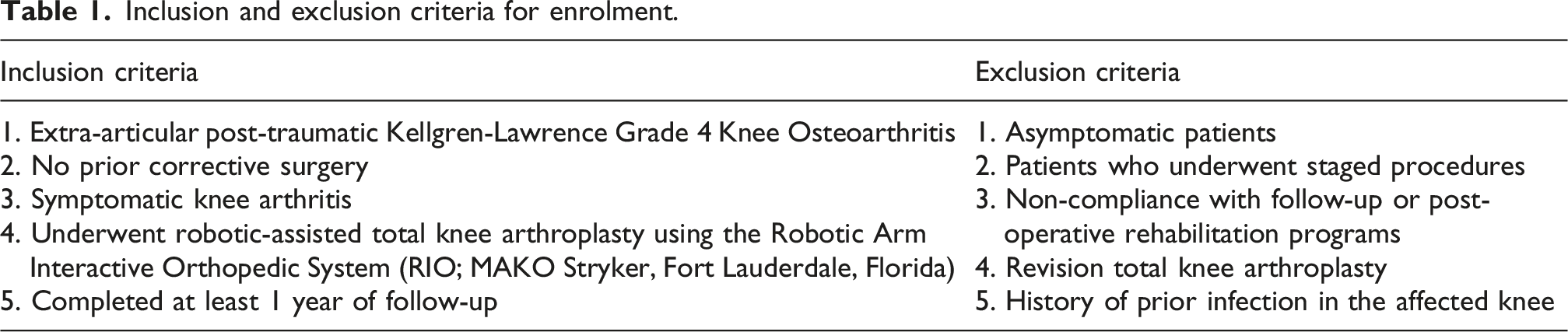
Inclusion and exclusion criteria for enrolment.
Clinical assessment
All patients were evaluated preoperatively and postoperatively at 2 weeks, 6 weeks, 3 months, and 1 year using: Knee Society Score (KSS 2011) 16 ; Knee Injury and Osteoarthritis Outcome Score (KOOS) 17 ; Range of motion (ROM), measured clinically using a goniometer. Visual Analogue Scale (VAS) for pain 18 was recorded preoperatively, at discharge, and at subsequent follow-ups. All clinical assessments were conducted by the senior author to minimize inter-observer variability.
Radiographic evaluation
At our centre, preoperative imaging included standing anteroposterior (AP) and lateral knee radiographs and full-length lower limb scanograms. In keeping with the CT-based workflow for RA-TKA, a pre-operative lower limb CT scan was also performed according to the manufacturer protocol. Radiographs were repeated at 6 weeks and 1 year post-operatively.
Mechanical axis (HKA) on scanograms
The Hip–Knee–Ankle (HKA) angle was measured on long-leg radiographs using the PACS measurement tools. HKA was defined as the angle subtended by the mechanical axis of the femur (centre of femoral head to centre of knee) and the mechanical axis of the tibia (centre of knee to centre of ankle). The femoral head centre was identified using a concentric circle method; the ankle centre was taken as the midpoint of the talar dome. 19 In this manuscript, values closer to 180° indicate a more neutral mechanical alignment; values below 180° indicate relative varus, and values above 180° indicate relative valgus.
CT-derived alignment measures and aHKA
After CT upload and segmentation, anatomical reference points were defined within the planning software by trained and certified segmentation specialists. The software generated alignment measures including the lateral distal femoral angle (LDFA), medial proximal tibial angle (MPTA), arithmetic hip–knee–ankle angle (aHKA), and joint line obliquity (JLO). The arithmetic approach defines aHKA as MPTA − LDFA. The aHKA concept and its measurement reliability relative to CT-based assessment have been described previously. 20 Post-operative aHKA was derived using intra-operative component alignment values recorded on the console (MPTA and LDFA equivalents based on implant positioning), to provide a standardised coronal alignment metric consistent with the arithmetic approach. 20
Intraoperative gap analysis
Intraoperative medial and lateral compartment gaps at full extension and 90° flexion were retrieved from the console. These data were summarised descriptively to document the achieved balance targets and to contextualise postoperative functional recovery.
Surgical technique
Preoperative CT-based 3D planning enabled detailed characterisation of the extra-articular deformity and templating of component positioning. LDFA and MPTA were used to quantify coronal plane contributions from the femur and tibia, and to determine whether the deformity could reasonably be compensated using intra-articular resections without corrective osteotomy—consistent with commonly cited principles that not all extra-articular deformities are safely correctable intra-articularly.1–3,22,23 In this cohort, deformities were deemed addressable with intra-articular correction alone, and the preoperative aHKA ranged from −13.4° to +3.0°.
After exposure using a midline skin incision and a medial parapatellar approach, femoral and tibial tracking arrays were fixed using fiducial pins (femur and proximal tibia just distal to the tibial tuberosity). Hip centre and malleoli were registered, followed by mapping of the distal femur and proximal tibia. Baseline limb alignment and gap measurements were recorded.
Virtual bone cuts were then adjusted in three planes to achieve alignment and balance targets consistent with a functional alignment philosophy: restoring a safe overall mechanical alignment envelope while accommodating patient-specific joint-line orientation where possible and achieving reproducible gap targets without excessive soft-tissue release.1–3,21 Planned intraoperative targets are summarised below (Table 2).
Bone resections were executed by the surgeon with robotic arm guidance. Trial components were inserted to confirm component positioning, gap balance, limb alignment, and patellar tracking prior to implantation of definitive components. No drains were used. Full weight-bearing ambulation began on post-operative day 1 with a four-legged walker, and outpatient physiotherapy was arranged upon discharge.
Statistical Analysis
All analyses were conducted in R (version 4.2.2) with a two-sided significance threshold of α = 0.05. Continuous variables were summarized using mean (SD), median [IQR], range, and 95% confidence intervals (CI) for the mean (one-sample t-intervals). Categorical variables were presented as counts and percentages.
PROMs (KSS, KOOS, VAS)
Given the small sample size and concerns regarding non-normality across several domains, PROMs were summarized as medians [IQR] at each timepoint. Overall change across repeated timepoints was assessed using the Friedman test. Where an overall time effect was detected, planned paired comparisons versus baseline were performed using Wilcoxon signed-rank tests with Holm adjustment for multiple comparisons. Changes are reported as Hodges–Lehmann median differences with 95% CI.
Radiographic alignment (HKA and aHKA)
Alignment targets for implant positioning according to functional alignment principles.
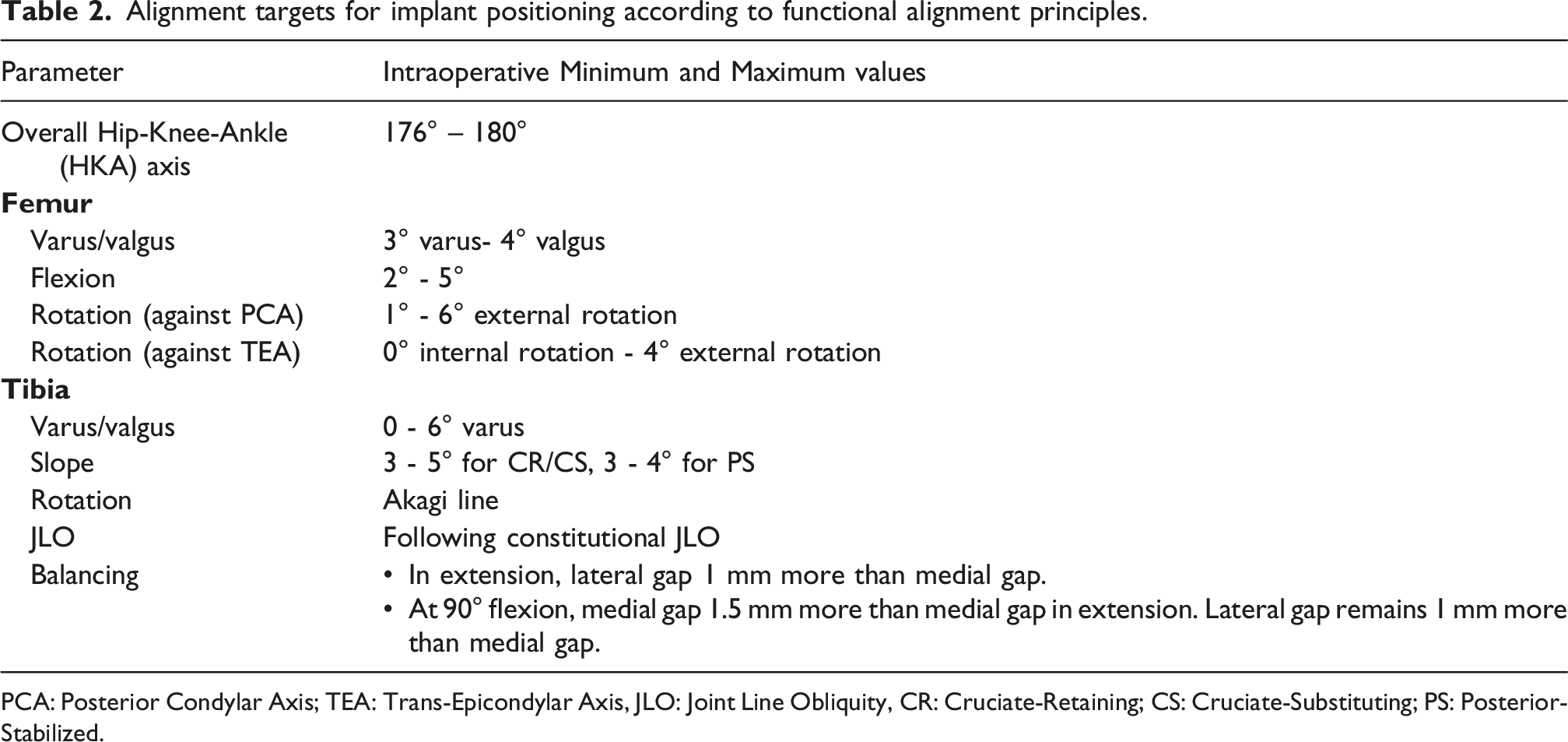
PCA: Posterior Condylar Axis; TEA: Trans-Epicondylar Axis, JLO: Joint Line Obliquity, CR: Cruciate-Retaining; CS: Cruciate-Substituting; PS: Posterior-Stabilized.
ROM
ROM change was analysed similarly with a paired Wilcoxon signed-rank test. A paired t-test was also performed as a sensitivity analysis to assess consistency of inference under approximate normality of paired differences.
Missing data
Missingness was assessed at each timepoint, with isolated gaps at the 2-week follow-up. Baseline comparisons between cases with and without missing values used the Wilcoxon rank-sum test; no significant differences were observed. No imputation was performed; analyses used available-case data.
Given one bilateral case, analyses were primarily descriptive and inferential results are interpreted cautiously with respect to potential non-independence.
Results
Patient demographics and perioperative data
Patient demographics and perioperative data (knee-level).
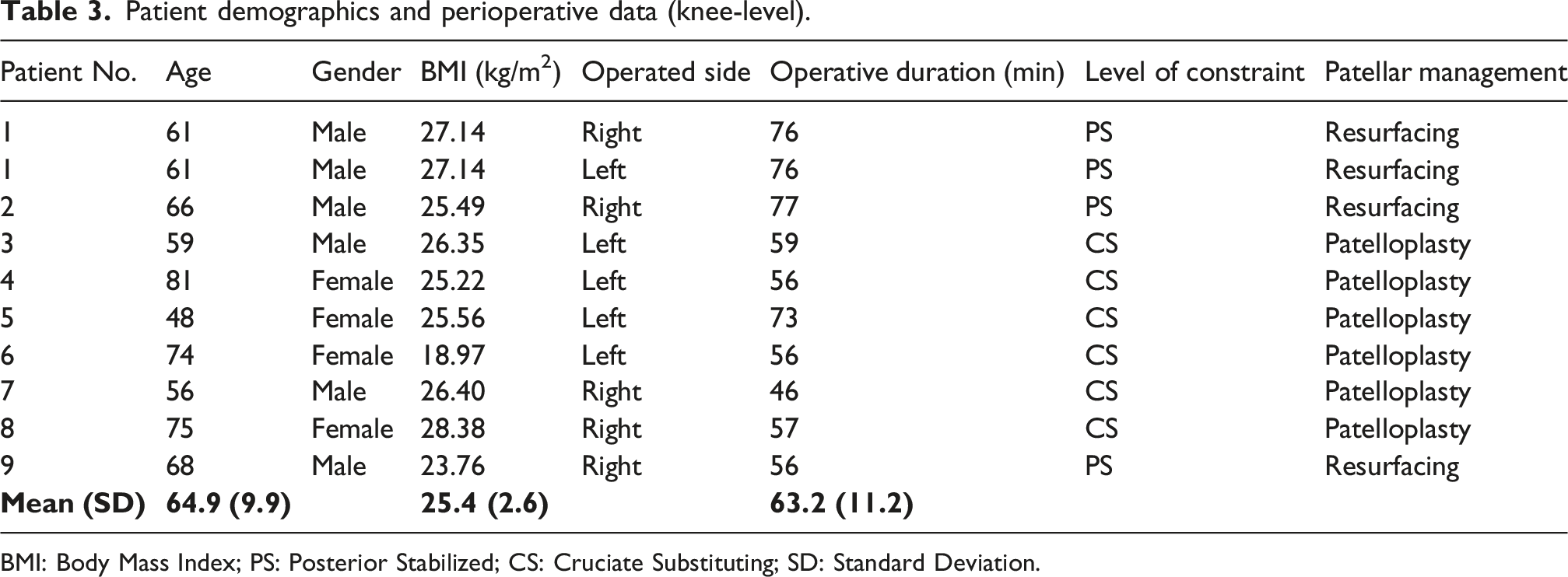
BMI: Body Mass Index; PS: Posterior Stabilized; CS: Cruciate Substituting; SD: Standard Deviation.
Radiographic outcomes
Representative pre- and postoperative radiographs from a patient in the study cohort are provided for reference (Figure 1). Pre- and postoperative radiographic assessment of the operated limb for patient #9. Standing scanogram radiographs are shown in the AP view preoperatively (A) and at 6 weeks postoperatively (B). Standing knee radiographs are shown preoperatively (C, AP; G, lateral) and at 1 year postoperatively (D, AP; H, lateral). Lateral scanogram views are shown preoperatively (E) and at 6 weeks postoperatively (F). Panels demonstrate correction of alignment and stable appearance of the knee arthroplasty components over follow-up. Abbreviations: AP: anterioposterior.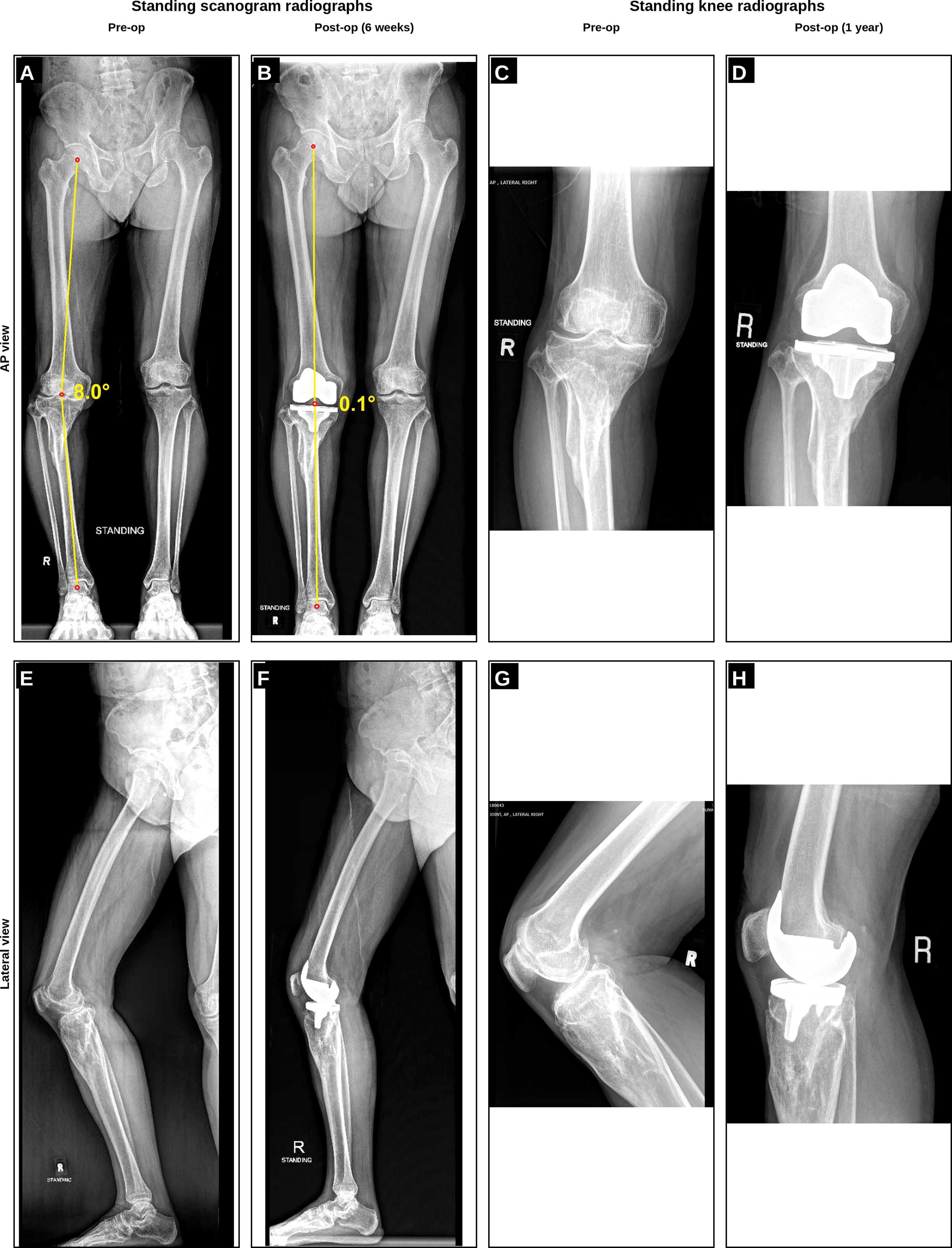
Hip-Knee-ankle (HKA) axis
Pre- and post-operative Hip-Knee-Angle (HKA) axes.
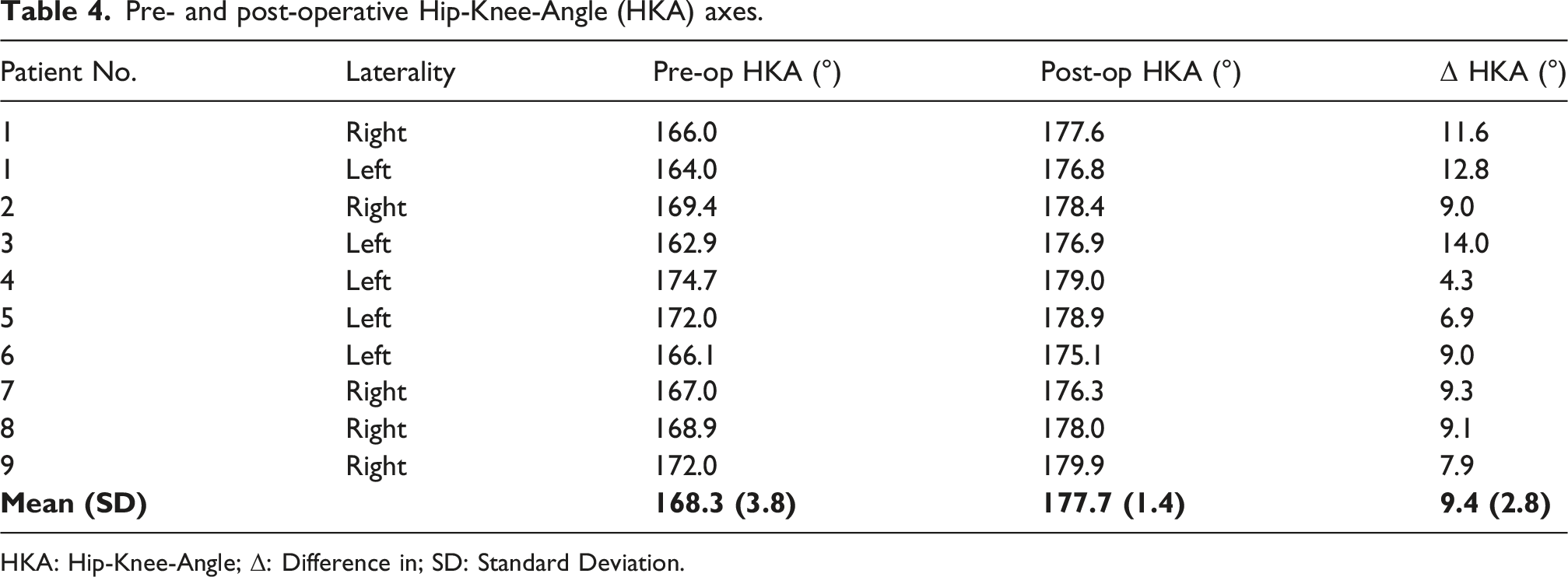
HKA: Hip-Knee-Angle; Δ: Difference in; SD: Standard Deviation.
Arithmetic hip–Knee–ankle angle (aHKA)
Preoperative aHKA averaged −4.9 ± 4.6°, improving to −0.6 ± 2.5° postoperatively, corresponding to a mean correction of 3.96 ± 3.70° (median 4.0°, IQR 1.83–6.95). The change was statistically significant (Wilcoxon W = 42.0, p = 0.0104) with a rank-biserial correlation = 0.78, representing a large effect size (Figure 2, Table 5). These results confirm consistent coronal alignment restoration toward neutral mechanical alignment across all patients. Paired plot showing pre- and post-operative mechanical Hip-Knee-Angle (mHKA) angle (°) for each operated knee (n = 10). Each line connects the same knee over time, demonstrating individual correction. ΔHKA is defined as Post–Pre; positive values indicate movement toward 180° (more neutral alignment). Abbreviations: HL, Hodges–Lehmann estimate (median paired difference); CI, confidence interval; r_b, rank-biserial correlation (effect size for Wilcoxon signed-rank test); Δ, mean paired difference (post–pre); t(df), t statistic with degrees of freedom; dz, Cohen’s dz (standardized mean change for paired data). Pre- and post-surgical Arithmetic Hip-Knee-Angle (aHKA) and Joint Line Obliquity (JLO). aHKA: Arithmetic Hip-Knee-Angle; JLO: Joint Line Obliquity; SD: Standard Deviation.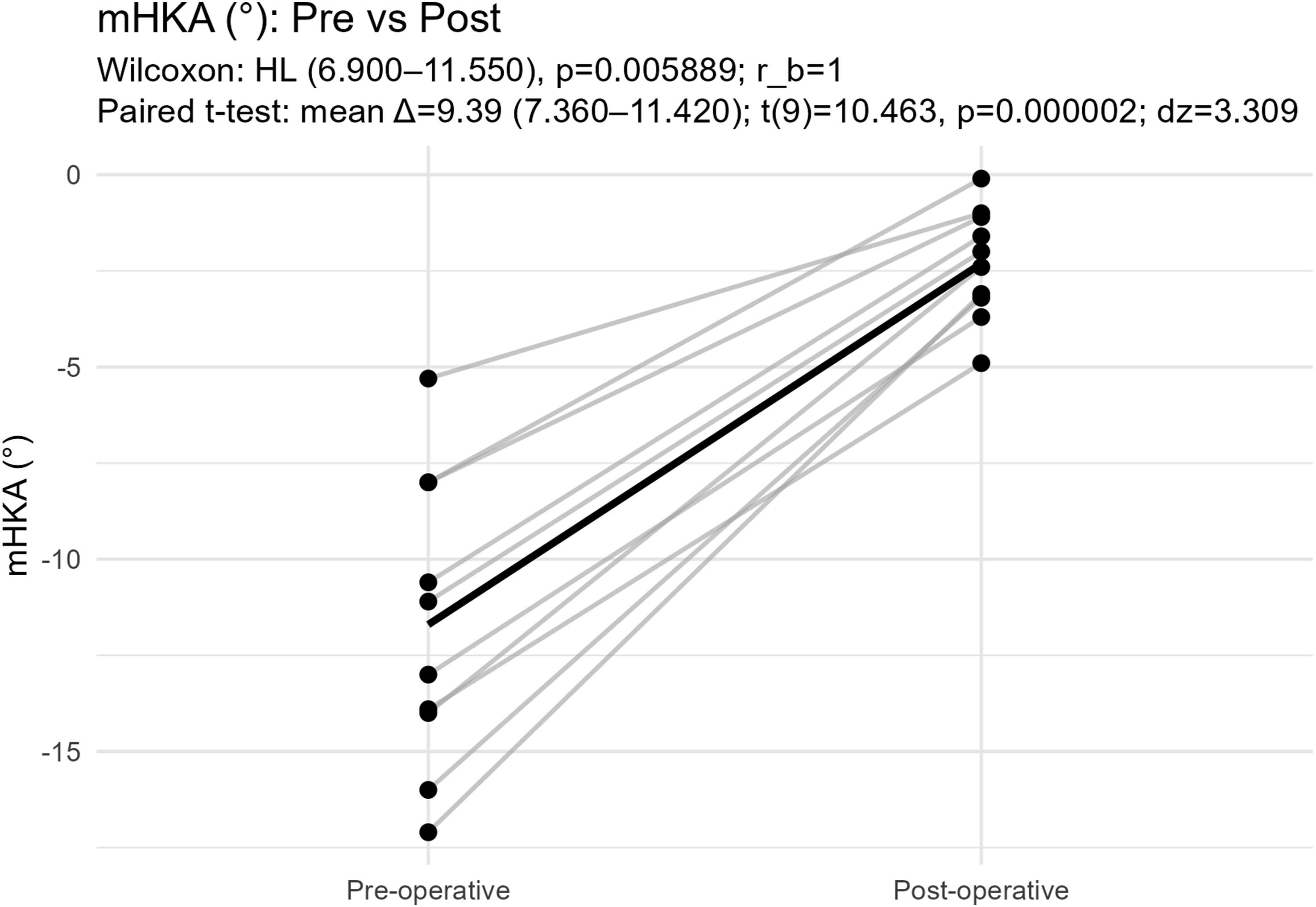
Clinical assessment
Range of motion
ROM improved by 1 year. The ROM arc increased from a pre-operative mean of 95.5 ± 21.7° (median 95°, range 70–135°) to 119.5 ± 17.4° (median 127.5°, range 100–135°) (Figure 3). Paired testing demonstrated a statistically significant improvement (paired Wilcoxon p < 0.01). Sensitivity analysis using a paired t-test on paired ROM differences was also significant (p < 0.001), supporting consistent inference across parametric and non-parametric approaches. Paired plot showing pre- and post-operative range of motion (ROM) in degrees (°) for each operated knee (n = 10).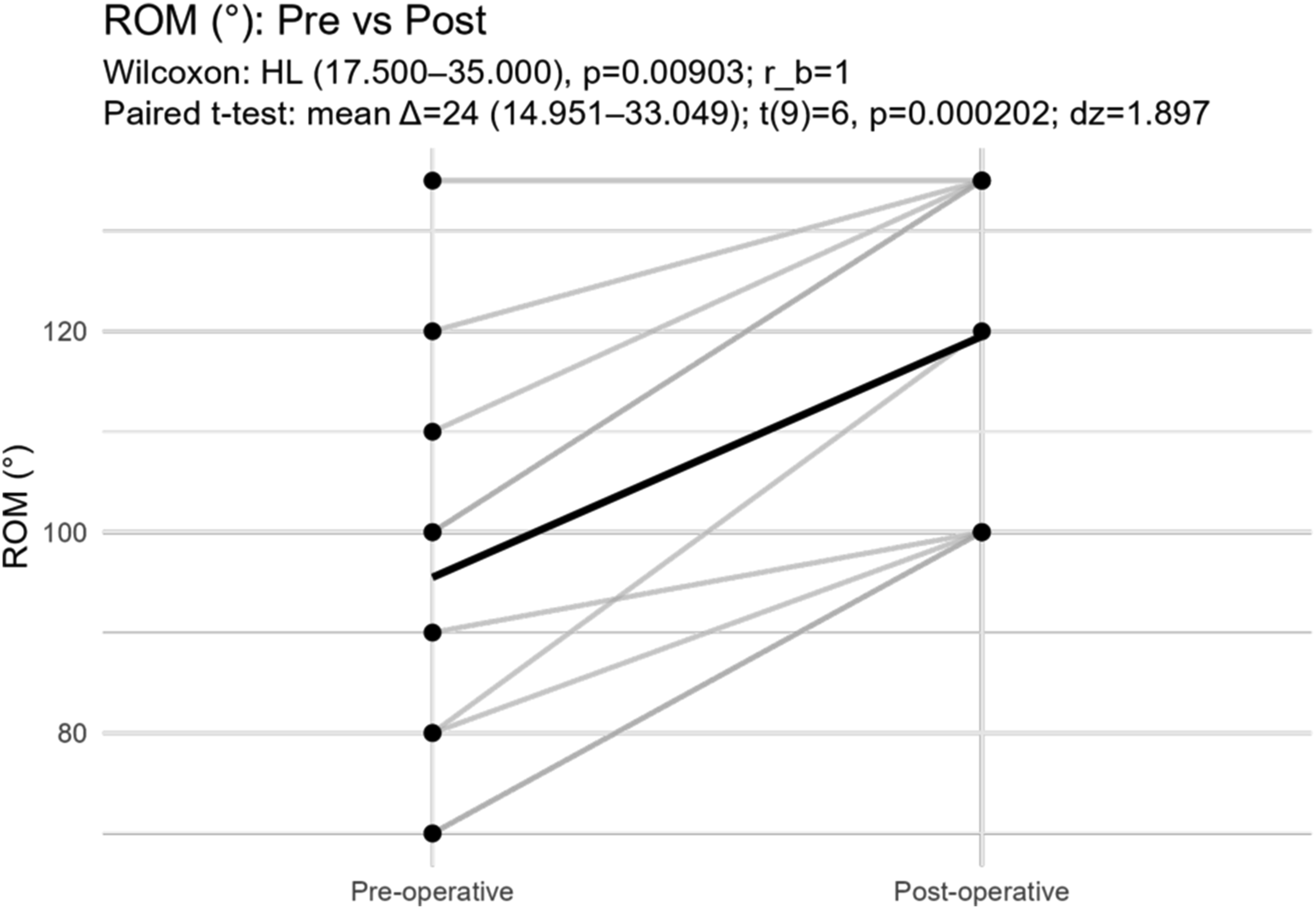
Patient reported outcome measures (PROMs)
Knee Society Score (KSS)
Objective Knee Indicators, Symptoms, and Satisfaction improved by 2 weeks after surgery with continued improvement through 1 year (Figure 4). Functional scores showed an expected early postoperative dip at 2 weeks before exceeding baseline by 6 weeks and continuing to rise thereafter. Planned paired comparisons versus baseline demonstrated significant improvement in KSS-Function by 3 months (Hodges–Lehmann +28.5, 95% CI 14.0–44.5; Holm-adjusted p = 0.0128). At 1 year, improvement was sustained with a median KSS-Function of 86 and Hodges–Lehmann change of +56.5 (95% CI 44.0–74.0; Holm-adjusted p = .0091). KSS distribution across subscales over time. Asterisks indicate significant paired differences compared with baseline (Holm-adjusted p < 0.05).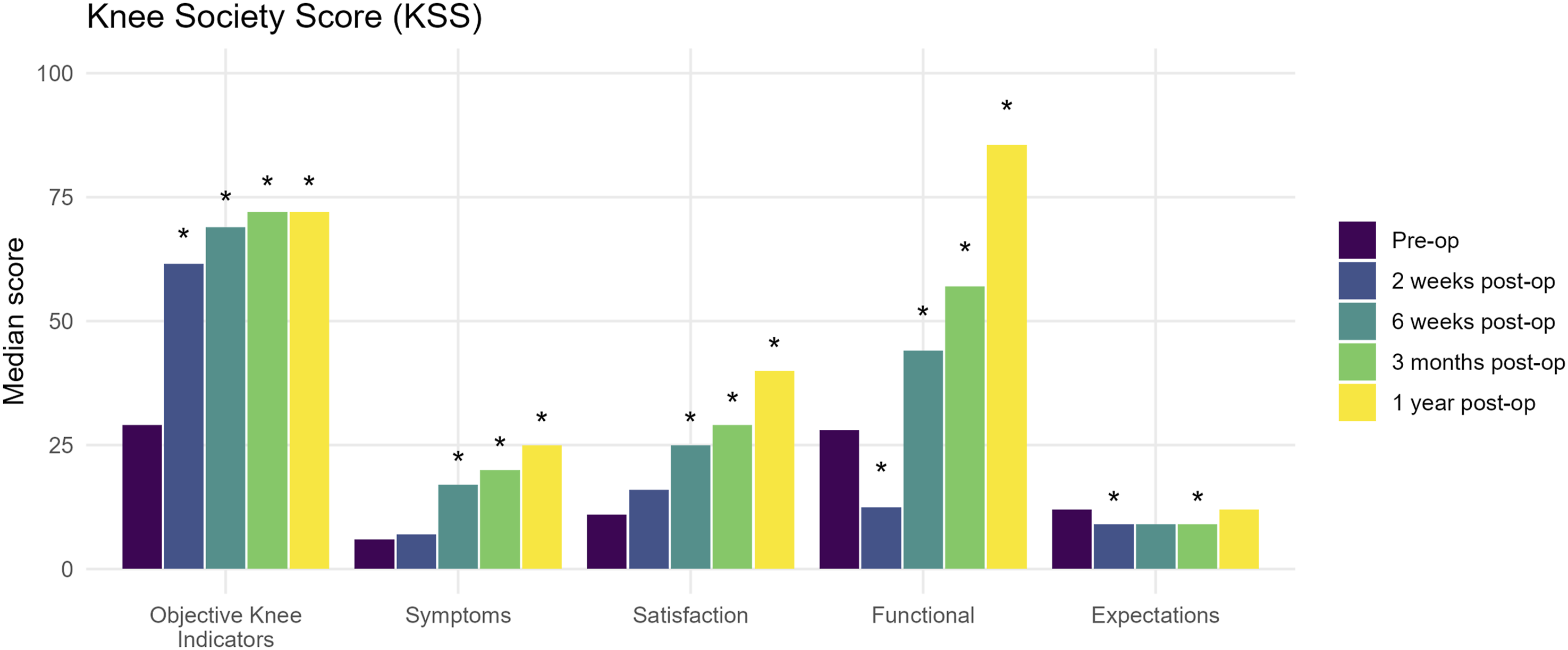
Knee Injury and Osteoarthritis Outcome Score (KOOS)
Pain and Quality of Life improved significantly as early as 2 weeks. By 6 weeks, Symptoms/Stiffness, Activities of Daily Living, and Sport/Recreation also improved significantly from baseline, with effects sustained through 1 year (Figure 5). KOOS-Symptoms showed Hodges–Lehmann improvement of +28.5 at 3 months (95% CI 2.0–49.5; Holm-adjusted p = 0.0328) and +46.0 at 1 year (95% CI 25.0–68.0; Holm-adjusted p = 0.0091). KOOS distribution across domains over time. Asterisks indicate significant paired differences compared with baseline (Holm-adjusted p < 0.05). Abbreviations: QOL: quality of life.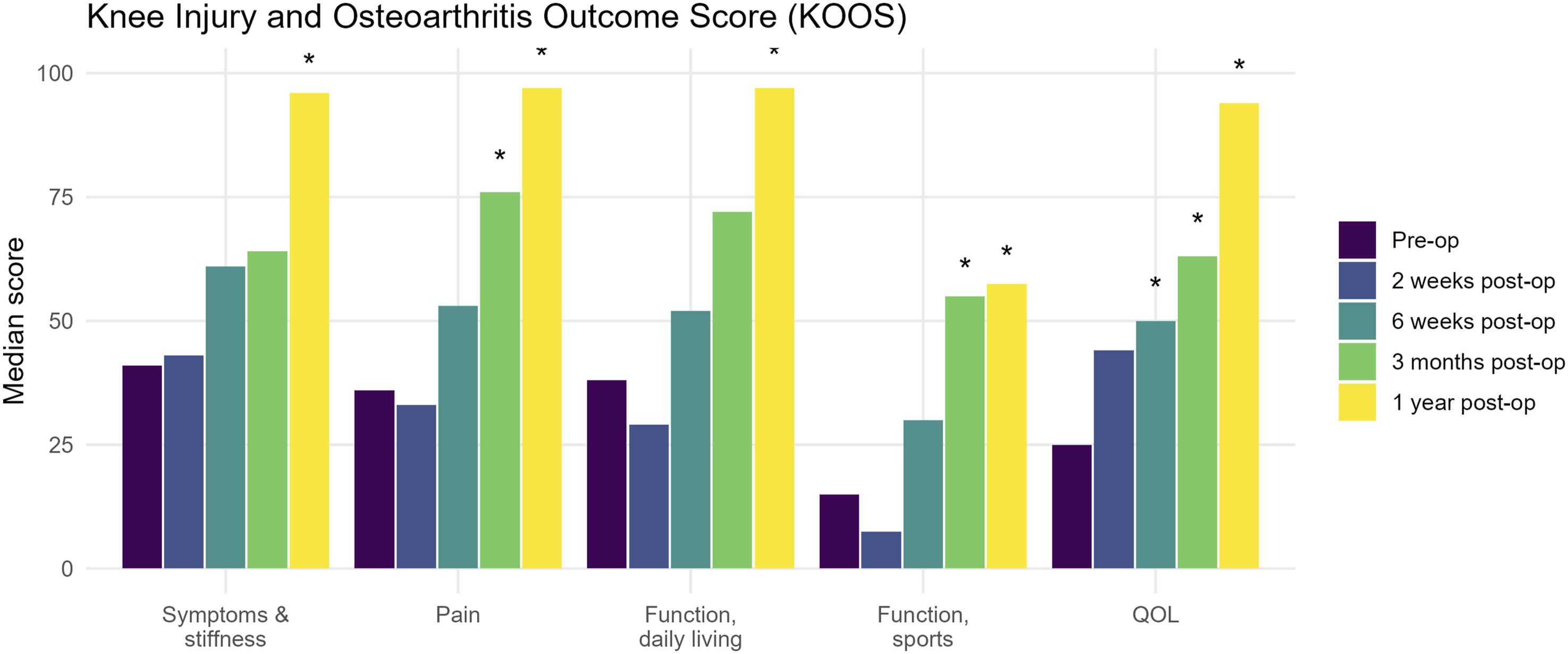
Visual analogue scale (VAS) for pain
Pain scores decreased steeply after surgery. At discharge, the Hodges–Lehmann median reduction was −8 (95% CI −9 to −5; Holm-adjusted p = 0.0083). At 6 weeks, pain remained significantly lower than baseline (Hodges–Lehmann −4, 95% CI −6.5 to −0.5; Holm-adjusted p = 0.0133). At 3 months, the reduction was −6 (95% CI −7 to −4; Holm-adjusted p = 0.0088). At 1 year, median VAS was 0 with Hodges–Lehmann reduction of −7.5 (95% CI −9 to −5; Holm-adjusted p = 0.0088).
Complications
All wounds healed within two weeks. There were no cases of superficial wound infection, deep infection, deep vein thrombosis, patellar tendon avulsion, periprosthetic fracture (patellar, femoral, or tibial), or tracker pin site infection in this cohort. No clinically significant patellar maltracking, patellar subluxation/dislocation, anterior knee pain requiring intervention, patellar fracture, or extensor mechanism complication was observed at final follow-up.
Discussion
This case series supports the feasibility and short-term safety of single-stage RA-TKA in selected patients with post-traumatic extra-articular deformity. Clinically meaningful improvements were observed in pain, function, and ROM, alongside restoration of coronal alignment toward neutral, without the additional corrective osteotomy. The central premise underlying this approach is careful patient selection—specifically deformities that can be compensated intra-articularly without producing an excessively oblique joint line or compromising collateral ligament competence—consistent with commonly cited decision-making principles in the extra-articular deformity literature.1–3,22,23
Alignment restoration without osteotomy
In this series, mean HKA improved from 168.3° to 177.7°, corresponding to a mean reduction in varus deviation from approximately 11.7° (180° − 168.3°) pre-operatively to 2.3° post-operatively (180° − 177.7°). This degree of correction was achieved without staged osteotomy and without escalation to constrained or hinged designs, suggesting that, in appropriately selected deformities, intra-articular correction can be sufficient. The broader literature recognises that while severe deformities may require osteotomy, a subset can be corrected intra-articularly if the deformity is not excessively large or too close to the joint and if planned resections do not destabilise the knee.1–3,6–10,22,23
Patellar tracking was assessed intra-operatively with robotic assistance. This assessment allowed us to perform the necessary releases and adjust femoral component rotation to obtain good patella tracking. Robotic assistance may add value in this context by enabling accurate execution of planned resections and component alignment despite distorted anatomy and less reliable conventional guides. Robotic-arm assisted and other computer-assisted techniques have been associated with improved alignment and component positioning in multiple settings, and navigation-assisted approaches have been reported as useful options in knees with extra-articular deformity.11–14,24,25
Range of motion and early functional recovery
Pre-operatively, mean ROM was 95.5°, with limited extension in many knees. By 1 year, mean ROM increased to 119.5°, with clinically meaningful recovery of extension and flexion across the cohort. Osteotomy-based strategies can achieve acceptable correction but may introduce additional biological and rehabilitation constraints related to the osteotomy site.6–10 The present results are consistent with the rationale that, when intra-articular compensation is appropriate and stable balance can be achieved, avoiding osteotomy may support a more direct rehabilitation trajectory while still delivering substantial coronal correction.
PROM improvements
PROM trajectories were consistent with expected early postoperative patterns: early symptom relief and satisfaction improvement, with functional recovery improving more gradually over time. The use of validated outcome measures (KSS 2011 and KOOS) strengthens interpretability and comparability across studies.16,17 Notably, these improvements were observed in a cohort restricted to post-traumatic deformity cases rather than mixed aetiologies, a subgroup that can be higher-risk because of altered bony anatomy, post-injury biology, and potential residual soft-tissue compromise.
Safety and implant strategy
No major complications were observed, including no tracker pin site infections or fractures. While this is reassuring, the cohort is small and follow-up is limited to 1 year. With respect to implant constraint, the predominant use of CS designs with selective use of PS designs, without constrained or hinged constructs, implies that acceptable ligament balance was achievable within the planned workflow in these selected cases. This aligns with the emphasis on preoperative deformity characterisation, intraoperative assessment of gaps, and component-level adjustment to achieve reproducible balance targets. The decision on whether to implant a CS or PS insert is dependent on a combination of intra-operative objective robotic console gap assessment with clinical validation by the senior author as well as PCL integrity. In cases where the degree of constraint had to be increased to PS, the patella was resurfaced; in other cases, patelloplasty or non-resurfacing was performed when patellar tracking was satisfactory and resurfacing was not considered necessary.
Limitations
This study has several limitations. First, the sample size is small and from a single centre, limiting generalisability. Second, the retrospective design carries inherent selection bias, particularly because only deformities deemed suitable for intra-articular correction without osteotomy were included. Third, heterogeneity in implant constraint (CS vs PS) and patellar management may confound PROM trajectories. Fourth, one patient contributed bilateral knees, introducing potential non-independence for knee-level analyses; inferential results should therefore be interpreted cautiously. Finally, follow-up is limited to 1 year, precluding conclusions about long-term survivorship, late complications, and revision risk.
Conclusion
In selected patients with post-traumatic extra-articular deformity and end-stage knee arthritis, single-stage robotic-assisted TKA without corrective osteotomy produced consistent coronal alignment correction toward neutral and meaningful improvements in pain, ROM, and patient-reported outcomes at 1 year, without major complications. This approach may offer a less morbid alternative to osteotomy-based strategies when deformity characteristics allow safe intra-articular compensation and stable soft-tissue balance.
Footnotes
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Sunway Medical Centre Independent Research Committee (SREC Reference No.: 046/2025/IND/ER). Written informed consent was obtained from all participants prior to enrolment, including consent for the use of de-identified clinical and radiographic data for research and publication. All data were anonymized prior to analysis, stored on password-protected institutional systems, and accessed only by authorized study personnel.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Datasets were generated and may be available upon request from the corresponding author.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this work the author(s) used ChatGPT 5 (Open AI) as a tool for data analysis assistance, grammar correction and formatting compliance. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.