
Abstract
Adjunctive strategies that effectively incorporate adolescents’ developmental needs may augment the therapeutic benefits of cognitive behavioral therapy (CBT) for adolescents with attention deficit hyperactivity disorder (ADHD). This preliminary study evaluated a combined CBT and music-based treatment designed to enhance emotion-regulation skills in adolescents with ADHD. Utilizing a single-case experimental design, eight adolescents with ADHD were assigned to a 3-week baseline assessment phase followed by 12 weekly individual sessions of treatment and a 2-month follow-up phase. The intervention was effective in reducing the core symptoms of ADHD, such that, participants showed an increase in adaptive emotion-regulation strategies (cognitive reappraisal) and decrease in maladaptive emotion-regulation strategies (expressive suppression). The intervention was also found to be highly acceptable to participants. The findings provide initial support for combining standard CBT with music-based treatment designed to enhance emotion-regulation skills, and add to the growing body of literature showing that adjunctive strategies can augment the therapeutic benefits of CBT for adolescents with ADHD.
Attention deficit hyperactivity disorder (ADHD) is the second most common mental health disorder in children and adolescents (Barican et al., 2022; Merikangas et al., 2009). The estimated prevalence is 5%–10% worldwide, with males being two to five times more likely to be affected than females (DuPaul et al., 2020; Erskine et al., 2017; Mohammadi et al., 2021). The disorder is characterized by developmentally problematic symptoms of inattention and/or hyperactivity/impulsivity and typically manifests in early childhood (American Psychiatric Association, 2013). If unidentified and left untreated, the symptoms of ADHD run a chronic course and persist into adulthood producing adverse long-term outcomes and the risk of comorbidities (Barkley et al., 2002; Mechler et al., 2021; Sibley et al., 2017; Spencer et al., 2014; Thomson et al., 2020).
Traditionally, the primary neurocognitive deficits of ADHD were considered to be inattention and hyperactivity–impulsivity (American Psychiatric Association, 2000). Recent neuroimaging research indicates that ADHD is a complex and heterogeneous disorder that involves several brain networks regulating cognitive, motivational, and emotional activity (Antonietti et al., 2018; Morris et al., 2020; Wolraich et al., 2019). These findings suggest that deficits in emotion regulation are core features of ADHD that should be incorporated into theoretical conceptualizations and diagnostic criteria (Musser et al., 2017; Silverman et al., 2021). Therefore, apart from the core symptoms used to classify ADHD, emotion dysregulation is an associated feature supporting the diagnosis of ADHD (American Psychiatric Association, 2013; Asherson et al., 2016). In ADHD, emotion dysregulation is characterized by problems with emotional control, which include feelings of irritability and frequent outbursts of short duration; emotional over-reactivity, which includes a diminished ability to handle typical life stresses, resulting in frequent feelings of being hassled and overwhelmed; and mood lability, which includes short and unpredictable shifts from normal mood to depression or mild excitement (Reimherr et al., 2005; Steinberg & Drabick, 2015; Zemestani et al., 2018). In other words, deficient emotion regulation involves a failure to inhibit negative emotions that leads to negative, affectively driven impulsive behavior in ADHD (Bunford et al., 2015; Graziano & Garcia, 2016; Seymour et al., 2014). Thus, in ADHD, emotions are moderated and/or regulated to a lesser extent by top-down, effortful executive control (Antshel et al., 2014; Barkley et al., 2010), and it is important that deficits in emotion regulation are incorporated into treatment models and targeted via interventions (Rosen et al., 2019; Zemestani, Hoseinpanahi, et al., 2022). Targeting emotion-regulation deficits in ADHD may result in the reduction of symptoms including affectively driven impulsive behaviors and emotional–behavioral dysfunctions.
Current clinical guidelines for the treatment of ADHD in children and adolescents recommend an individualized multimodal treatment approach including pharmacological and psychosocial interventions (E. Chan et al., 2016; Wolraich et al., 2019). Pharmacological interventions, particularly those involving the administration of stimulant medication, are first-line treatments for ADHD (Cortese et al., 2018; Mechler et al., 2021). While outcomes from first-line pharmacological treatments can be successful, a large proportion of individuals with ADHD do not improve and as many as half discontinue taking medication within 3 years of initiating treatment (Jangmo et al., 2019; Zetterqvist et al., 2013) due to adverse side effects, acceptability, and social stigma associated with the use of psychiatric medication (Brinkman et al., 2018; Golubchik et al., 2020; Jangmo et al., 2019; Madjar et al., 2020; Massuti et al., 2021). Psychosocial interventions therefore represent an alternative form of treatment (DuPaul et al., 2020; Lambez et al., 2020; Mechler et al., 2021).
Most psychosocial interventions for young people with ADHD are based on behavioral principles (Fabiano et al., 2009; Guo et al., 2021; López-Pinar et al., 2018). Behavioral interventions in the form of family- and school-based behavior management techniques, such as parent training and classroom management are first-line psychosocial treatments for young people with ADHD (Chronis et al., 2006; Evans et al., 2014; Pelham & Fabiano, 2008). These approaches are effective for young children (i.e., < 8 years of age) and preadolescents (i.e., < 12 years of age); however, research among adolescents suggests only modest benefits (Barkley et al., 2001; Chafouleas et al., 2012; E. Chan et al., 2016), which highlights the need for adjunctive and/or adjuvant strategies to augment treatment (E. Chan et al., 2016; Lachaine et al., 2012).
One possible explanation for insufficient results in adolescents with ADHD is that developmental changes in the adolescents and contextual changes in the schools and families do not keep adolescents engaged in the treatment process and thereby reduce their adherence to treatment (Evans et al., 2014; Lachaine et al., 2012; Wolraich et al., 2019). Successful treatment of most adolescents with ADHD requires ongoing involvement and adherence to the therapy (DuPaul et al., 2020; Wolraich et al., 2019). Clinical trials among adolescents with ADHD suggest that they are more likely to engage with and comply with their treatment when they have an active role in the treatment process (DuPaul et al., 2020; Sibley et al., 2017). According to recent treatment guidelines, developmentally appropriate types of treatment (modalities) and adjunctive strategies that effectively incorporate adolescents’ developmental needs and preferences may increase treatment adherence and amplify the therapeutic benefits of current psychosocial interventions (DuPaul et al., 2020; Mücke et al., 2021; Wolraich et al., 2019; Zemestani et al., 2021). However, little research has been conducted on potential adjunctive modalities for augmenting the therapeutic benefits of current psychosocial interventions for adolescents with ADHD.
One possible adjunctive modality effectively incorporating the developmental needs and preferences of adolescents with ADHD that may augment the therapeutic benefits of psychosocial interventions is the music-based intervention (Antonietti et al., 2018; Dursun et al., 2021; Maloy & Peterson, 2014; Stegemann et al., 2019). The emotional, cognitive, and developmental needs of young people with ADHD can be addressed through musical experiences (Antonietti et al., 2018; Zhang et al., 2017). A growing literature has emerged in recent decades supporting the use of music interventions as a therapeutic modality (Aalbers et al., 2020; Aldridge, 1993; Davis et al., 2008; Hillecke et al., 2005; Thaut, 2015). Although the boundaries of musical interventions continue to be debated, the interventions themselves can involve either active or receptive methods (Aalbers et al., 2019; Freer & Evans, 2019; Raglio et al., 2015; Wan & Schlaug, 2010). In active methods, participants make music; in receptive methods, participants listen to music (Aalbers et al., 2021; Gardstrom et al., 2015; Wheeler, 2015).
Among various forms of therapeutic music interventions, group and individual receptive music listening interventions have been used with both clinical and healthy populations (Maloy & Peterson, 2014; Mok & Wong, 2003). For this reason, such interventions are sometimes referred to collectively as music medicine rather than music therapy (Bradt & Dileo, 2014; Raglio et al., 2015; Yinger & Gooding, 2014). Group and individual music listening interventions are potentially useful in adjunctive approaches to standard-care interventions. Although music-based interventions are used in both music therapy and music medicine, it is important to understand the differences between them, because they have different therapeutic applications and require different levels of musical training on the part of the practitioner. Music medicine is defined as passive listening to pre-recorded music provided by clinicians (Bradt & Dileo, 2014; Bradt et al., 2015). In treatment involving music medicine, listening interventions are often administered through loudspeakers or headphones, and individuals may or may not have the opportunity to select the music they hear (Bradt et al., 2013). Moreover, although music therapists undergo specialized training and are not permitted to practice music therapy without certification, neither specialized training nor certification is required to practice music medicine (Yinger & Gooding, 2014).
When added to standard protocols for people with serious mental disorders, music listening as a therapeutic modality has been shown to have significant effects on symptoms and functioning (Bradt et al., 2013; Ekitli & Özgür, 2021; Gold et al., 2009; Moore, 2013). Although the available research suggests that music-based interventions could help to improve the cognitive-emotional and cognitive-behavioral deficits of young people (Abrahams & van Dooren, 2018), research on the effects of these interventions on the deficits specific to ADHD in young people is scarce (Dursun et al., 2021; Zhang et al., 2017) because, to date, there is limited research on such interventions among young people with ADHD. A meta-analysis of research on the effectiveness of music-based interventions for young people with ADHD showed limited effects on task performance (Maloy & Peterson, 2014), although preliminary behavioral studies of individuals with ADHD have produced promising results suggesting that music listening can be used to regulate emotions (Dursun et al., 2021; Moore, 2013; Zhang et al., 2017), enhance cognitive performance (M. M. Chan & Han, 2021; Lim et al., 2021), and control impulsive behaviors (Antonietti et al., 2018; Dursun et al., 2021).
Although preliminary evidence supports the use of purely music-based interventions to improve the cognitive-emotional and cognitive-behavioral symptoms of ADHD, to the best of the authors’ knowledge, there are no known studies investigating the addition of a music-based emotion-regulation protocol to the standard cognitive behavioral therapy (CBT) protocol to reduce the symptoms of ADHD in adolescents. The purpose of this preliminary study was therefore to determine whether adding music-based treatment designed to enhance emotion-regulation skills to standard-practice CBT for ADHD is associated with improved emotion regulation and reduced ADHD symptoms. Specifically, would the combination of the two forms of treatment improve the cognitive (i.e., attention), behavioral (i.e., hyperactivity/ impulsivity), and overall symptoms of ADHD?
Method
Design
Since this approach has not been studied before, a single-case experimental design was used to assess the effects of the intervention and refine it (Kazdin, 2011). The single-case design has several advantages, the most important of which is that it requires fewer participants because they act as their own controls, thus increasing statistical power (Barlow et al., 2009; Kazdin, 2011; Zemestani, Davoudi, et al., 2022). We employed an A–B single-case experimental across-participants design with follow-up using the single-case reporting guidelines for behavioral interventions (Barlow et al., 2009; Kazdin, 2011; Tate et al., 2016). The study took place in three phases. First, the participants underwent a 3-week baseline assessment phase (B1–B2–B3), during which they met with the therapist and completed measures during each session. The therapist did not provide any treatment during this phase but merely reviewed the self-report or parent-report measures briefly. Second, the participants entered the intervention phase. This consisted of 12 weekly individual sessions, face-to-face, of standard CBT for adolescents with ADHD (Sprich & Burbridge, 2019; Sprich et al., 2015; Sprich & Safren, 2020) and adjunctive music-based emotion-regulation skills (T1–T4–T8–T12). Finally, the maintenance of treatment gains was evaluated in a 2-month follow-up period. All the participants (adolescents and their parents) completed the standardized Emotion Regulation Questionnaire for Children and Adolescents (ERQ-CA) and Conners’ Parent Rating Scale-Revised Short Form (CPRS-RS) psychometric measures at the end of each session during each of the three phases, so that changes could be tracked.
Participants
Participants were eight adolescents, five females and three males with a mean age of 15.87 years (SD = 1.12, range = 13–17 years), with a principal diagnosis of ADHD recruited from six high schools in the city of Kuhdasht (Lorestan Province, Iran) between February and September 2021. Participants were recruited through school psychologists and counselors. Information about the study was given to the psychologists and counselors, and they were encouraged to refer interested and potentially eligible students, with the permission of the student and their family, to the research team. Families were subsequently contacted and invited to take part in a face-to-face eligibility and clinical assessment in an outpatient clinic. Assessment sessions lasted 30–45 min.
Participants had to fulfill the following criteria: (1) meet the criteria for ADHD set out in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013) as assessed by a master’s-level clinical psychologist using the Persian version of the Structured Clinical Interview for DSM-5 (SCID-5) (First & Williams, 2016; Mohammadkhani et al., 2017); (2) be aged between 13 and 17 years; and (3) participate on a voluntary basis with informed parental consent and adolescent assent. Exclusion criteria included (1) severe comorbid conditions that would interfere with participation (current major depression, panic disorder, active suicidality, conduct disorder, bipolar or psychotic disorders, substance abuse or dependence, or developmental disabilities); (2) receiving psychotherapy and taking any medications for ADHD in the past year and/or during the study. Students who met the inclusion criteria were contacted after a 7-day reflection period. In the pre-test assessment, participants and their parents completed a number of standardized measures before entering the baseline phase. Participants’ sociodemographic and clinical characteristics are presented in Table 1.
Participants’ sociodemographic and clinical characteristics.
Note. P = participant; F = female; M = male; ADHD = attention deficit hyperactivity disorder; ODD = oppositional defiant disorder; OCD = obsessive-compulsive disorder.
Ethics
The study was approved by the University of Kurdistan Research Ethics Committee (IR.UOK.REC.1400.001), which follows the Declaration of Helsinki for the ethical principles of medical research involving humans. Written informed consent was obtained from all parents and assent was obtained from all the adolescent participants.
Intervention
The intervention protocol consisted of 12 individual weekly sessions each lasting 60 min and followed standard-practice CBT for adolescents with ADHD (Sprich & Burbridge, 2019; Sprich et al., 2015; Sprich & Safren, 2020) and adjunctive music-based treatment to enhance emotion-regulation skills. The conceptual framework, strategies, and targets for the latter were adapted from theory and research related to both music-based interventions (Aalbers et al., 2019, 2021), and emotion-regulation skills (Marik & Stegemann, 2016; Rosen et al., 2019). We chose music-based emotion-regulation strategies to augment standard-practice CBT for ADHD on the basis of its track record in addressing emotion-regulation deficits (Dursun et al., 2021; Zhang et al., 2017). The intervention aimed to improve emotion regulation and, in turn, the core symptoms of ADHD.
The standard-practice CBT for ADHD treatment (Sprich & Burbridge, 2019; Sprich et al., 2015; Sprich & Safren, 2020) and adjunctive music-based emotion-regulation modules included: psychoeducation, treatment planning and motivational interviewing (two sessions), coping skills (one session), emotion recognition and regulation (two sessions), music-based emotion-regulation training (two sessions), distractibility (two sessions), adaptive thinking (two sessions), and relapse-prevention techniques (one session). Each session consisted of core treatment modules; after the fifth session, modules placed particular emphasis on improving emotion-regulation skills, since a primary goal of the protocol was to help adolescents learn how to experience emotions in a mindful and nonjudgmental manner and how to respond to them in more adaptive ways. In this way, treatment aimed to improve emotion regulation and, in return, ADHD symptoms (i.e., distractibility, racing thoughts, impulsivity, restlessness). Homework involved discussing what may be helpful to practice at home to improve emotion regulation in daily situations, for example, listening to calm music and walking or talking to feel or express emotions and thoughts. To increase adherence, participants received emotion-regulation and CBT homework cards, and discussed homework.
Each participant was exposed individually to the music they had chosen under the supervision of a certified music therapist via their personal cellphone (hands-free) at the clinic for 15 min before the start of each CBT session, through the cellphone speaker at the clinic for 30 min during each CBT session as within-session background music, and via the cellphone (hands-free) out of the clinic for 30 min each day as their between-session CBT homework assignments. Music in the new-age genre was used in the intervention. This is low-frequency soothing music, referred to in the literature as relaxing or sedative music, and is commonly used by listeners for mindfulness, meditation, or yoga (Smith & Joyce, 2004). We selected low-frequency soothing music because it has been found that exposure to sounds with a low frequency—between 125 and 1,000 Hz—has calming and relaxing effects. Slow-tempo repetitive music can positively influence the neuropsychological indicators related to emotion regulation and cognitive performance (Antonietti et al., 2018; M. M. Chan & Han, 2021; Dursun et al., 2021; Laukka et al., 2013; Linnemann et al., 2015; Marik & Stegemann, 2016). The specific pieces of music used in the intervention were selected at the suggestion of a master’s-level certified music therapist. They were sent to the participants’ cellphones electronically via Telegram or WhatsApp. The participants indicated their interest in particular pieces that were categorized and archived for each participant. The final selection of music for each participant was based on their individual preference. It should be noted that the music intervention presented in this study reflected music medicine, or passive listening to pre-recorded music provided by clinicians (Bradt & Dileo, 2014; Bradt et al., 2015), rather than active music therapy.
Although parents attended the clinic, for the most part they stayed outside the treatment room and were not present for sessions. At the end of each session, however, they were given questionnaires and handouts. These provided in-depth discussion of the topic of each session, and exercises and activities to help them understand the topics better, and to be aware and supportive of the skills their child was being taught in the sessions. For more consistency with the standard-practice CBT for adolescent ADHD (Sprich & Burbridge, 2019; Sprich et al., 2015; Sprich & Safren, 2020), parents participated in two full sessions with the adolescent, one early (Session 2) and one late in the course of treatment (Session 10).
The intervention was conducted by a therapist with a CBT orientation who was a master’s-level clinical psychologist with two years of clinical experience. She had undergone 6-month additional training in the delivery of music therapy prior to the study. Her supervisors were an associate professor in psychology specializing in CBT, and a master’s-level certified music therapist. Neither was directly involved in conducting the intervention.
Participants’ adherence to treatment was assessed by their attendance at treatment sessions and homework completion using forms developed for the protocol that were filled out by the therapist following each assessment session during the intervention (T1, T4, T8, and T12). Each component of the adolescents’ adherence was rated on a scale from 0 (not implemented as intended) to 2 (thoroughly implemented as intended). Scores across items on adherence forms were summed and a mean adherence rating for each assessment session coded was computed (ranging from 0 to 2).
Materials: Measures
Structured Clinical Interview for DSM-5
The SCID-5 (First & Williams, 2016) is a semi-structured clinical interview used to assess whether an individual meets criteria for any diagnoses as defined by the DSM-5 (American Psychiatric Association, 2013). In the current study, the SCID-5 was administered in person at the baseline assessment. A trained master’s-level clinical psychologist with expertise in the assessment of psychiatric disorders conducted the clinical interview. The SCID-5 has good internal consistency (a > .80), as well as excellent reliability and validity, in the diagnosis of severity of mental disorders (Shankman et al., 2018). It has been shown to be reliable and valid for use with Persian samples (Mohammadkhani et al., 2017; Zemestani, Hosseini, et al., 2022).
Conners’ Parent Rating Scale-Revised: Short Form
Parents evaluated the levels of their adolescent children’s cognitive, emotional, and behavioral problems using the CPRS-RS (Conners, 1997). This is one of the scales used most often for assessing the presence and severity of ADHD symptoms in young people aged 3–17 (Conners, 1997). It assesses different aspects of the cognitive, emotional, and behavioral disturbances typical of ADHD. It consists of 27 items each rated on a 4-point Likert-type scale from 0 (not true at all) to 3 (very much true) in four subscales: cognitive/attention deficit problems (six items), impulsivity/hyperactivity (six items), oppositional (six items), and ADHD index (nine items). A benchmark scores equal to or greater than 65 usually indicates significant clinical problems. The original version of the CPRS-RS has good psychometric properties (Conners et al., 1998). The Persian version of CPRS-RS, which has acceptable psychometric properties with a Cronbach’s alpha coefficient of 0.73 for the total score among Iranian young people (Shahaeian et al., 2007), was used in the present study.
Emotion-Regulation Questionnaire for Children and Adolescents
The ERQ-CA (Gullone & Taffe, 2012) is a revised version of the adult measure of ERQ (Gross & John, 2003), designed to assess the habitual use of emotion-regulation strategies in young people aged 10–18 (Gullone & Taffe, 2012). It is a 10-item self-report measure assessing two emotion-regulation strategies. Six items address cognitive reappraisal (CR, e.g., “When I want to feel happier, I think about something different”) and four items address expressive suppression (ES, e.g., “When I am feeling happy, I am careful not to show it”). Items are rated on a 5-point Likert-type response scale ranging from 1 (strongly disagree) to 5 (strongly agree), with higher scores on each scale indicating greater use of the corresponding emotion-regulation strategy. The range of scores for each subscale is 6–30 for CR items and 4–20 for ES items. Gullone and Taffe (2012) reported good internal consistency for the ERQ-CA strategies, such that, alpha coefficients ranged from .82 to .86 for the CR scale and from .69 to .79 for the ES scale. They also reported sound convergent and construct validity for the ERQ-CA. The Persian version of the ERQ-CA, which has acceptable psychometric properties with Cronbach’s alpha coefficients of 0.81 for all items and 0.79 and 0.68 for reappraisal and suppression, respectively (Lotfi et al., 2019), was used in the present study. Lotfi et al. (2019) also reported sound convergent and construct validity for the Persian version of the ERQ-CA.
Statistical analysis
Data were graphed and inspected visually in accordance with analytic guidelines for single-case experimental designs (Barlow et al., 2009; Kazdin, 2011). We identified significant changes attributable to the treatment using percentages and the reliable change index (RCI) (Jacobson & Truax, 1992). RCI was calculated to determine whether change reflected more than just measurement using the formula RCI = X2–X1/Sdiff in which X1 = pre-score, X2 = post-score, Sdiff =
Results
Attendance and adherence
Participants completed 85 of the 96 sessions (88.54%). Participants’ adherence to homework completion was excellent (M = 1.47; SD = 0.72).
Visual inspection
To track changes, each parent and adolescent’s scores on the CPRS-RS and ERQ-CA, respectively, were assessed during the baseline phase (B1–B3), in the treatment phase (T1–T4–T8–T12), and in the follow-up phase. The data were represented graphically and inspected visually. Figures 1 (a) to (d) and 2 (a) and (b) show the eight participants’ scores at all stages, indicating changes in all outcomes except one (scores on the oppositional CPRS-RS subscale) for two participants, P6 and P7.

Scores on the Conners’Parent Rating Scale-Revised (CPRS-R) across baseline (B1-B3), intervention (T1-T4-T8-T12), and follow-up (FLU) phases for all eight participants (P1-P8): (a) Attention deficit; (b) Hyperactivity; (c) Oppositional; (d) ADHD index.
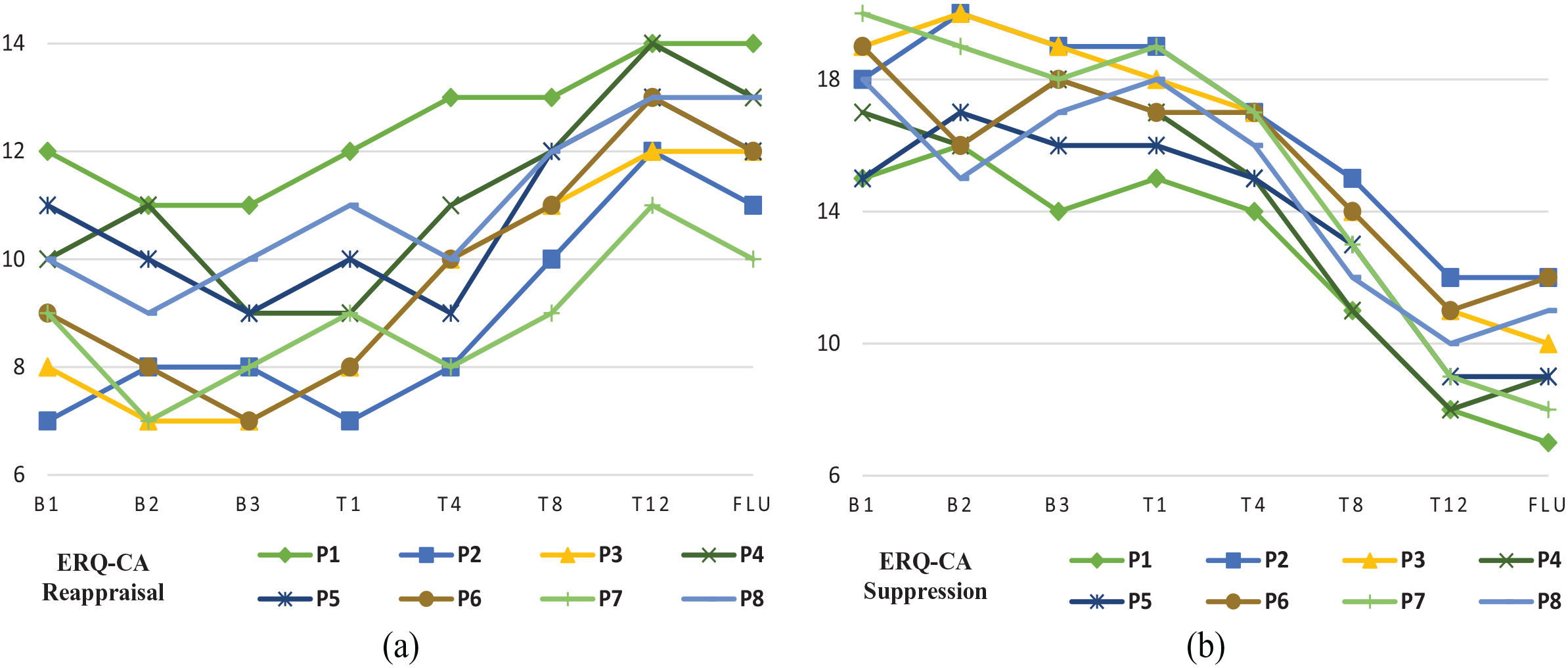
Scores on the emotion regulation questionnaire for children and adolescents (ERQ-CA) across baseline (B1-B3), intervention (T1-T4-T8-T12), and follow-up (FLU) phases for all eight participants (P1-P8): (a) Reappraisal; (b) Suppression.
Reliable change index
Table 2 presents three change scores for each participant: baseline change (B1 to the last baseline assessment before treatment), pre–post change (last baseline assessment to T12), post-follow-up change (T12 to follow-up), and pre-follow-up change (last baseline assessment to follow-up). The RCI scores suggest that, for all the participants other than P6 and P7, the intervention produced a significant and reliable change in the targeted domain (see Table 2). Analyses of the changes in CPRS-RS across the baseline, intervention, and follow-up phases support the hypothesis that CBT and adjunctive music-based emotion-regulation skills would lead to a significant decrease in the severity of ADHD symptoms. Again, according to the RCI scores, all the participants other than P6 and P7 achieved significant improvements at post-treatment and maintained a substantial proportion of their gains at follow-up.
Reliable change index (RCI) scores.
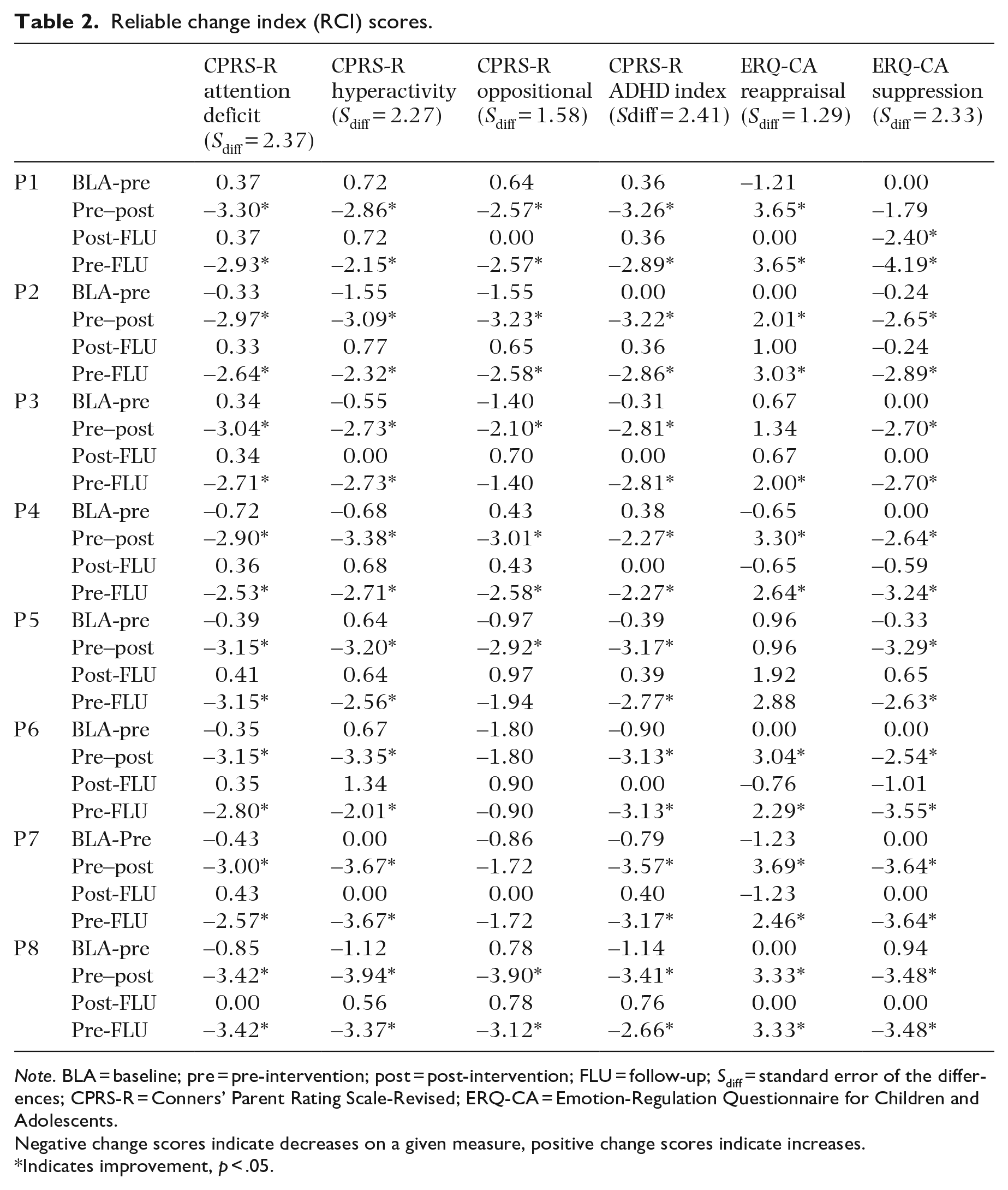
Note. BLA = baseline; pre = pre-intervention; post = post-intervention; FLU = follow-up; Sdiff = standard error of the differences; CPRS-R = Conners’ Parent Rating Scale-Revised; ERQ-CA = Emotion-Regulation Questionnaire for Children and Adolescents.
Negative change scores indicate decreases on a given measure, positive change scores indicate increases.
Indicates improvement, p ˂ .05.
Moreover, participants who improved their scores on the CPRS-RS, representing the severity of ADHD, during the intervention phase generally also improved their scores on the CR subscale of the ERQ-CA, representing the use of adaptive emotion-regulation strategies, and the emotional suppression subscale of ERQ-CA, representing the use of maladaptive emotion-regulation strategies. For all eight participants, changes (increases in CR and decreases in emotional suppression) during the intervention phase met the RCI threshold. Again, according to the RCI scores, all but one of the participants achieved significant improvements from the intervention to follow-up and maintained a substantial proportion of their gains at follow-up. The exception was P6 who scored slightly lower on measures of CR during the 12th session. She reported to the therapist that the emergence of a stressful family situation toward the end of treatment phase was having a negative effect on her ratings in the study measures. However, after two 45-min booster sessions that focused on adaptive coping, adaptive thinking, and restructuring her belief that stressful life events are crucial in the development of personality and can be modified by adaptive coping and cognitive styles, her use of adaptive emotion regulation improved.
Effect sizes
Table 3 presents an overview of the means (SD) and effect sizes (Cohen’s d) for outcome measures for all participants at all stages. Effect sizes (Cohen’s d) suggest that all participants showed improved outcomes in the treatment phase and at follow-up. Medium to large effect sizes suggest improvements in ADHD symptoms and use of emotion-regulation strategies from baseline to follow-up.
Means, standard deviations, and effect sizes of outcome measures.
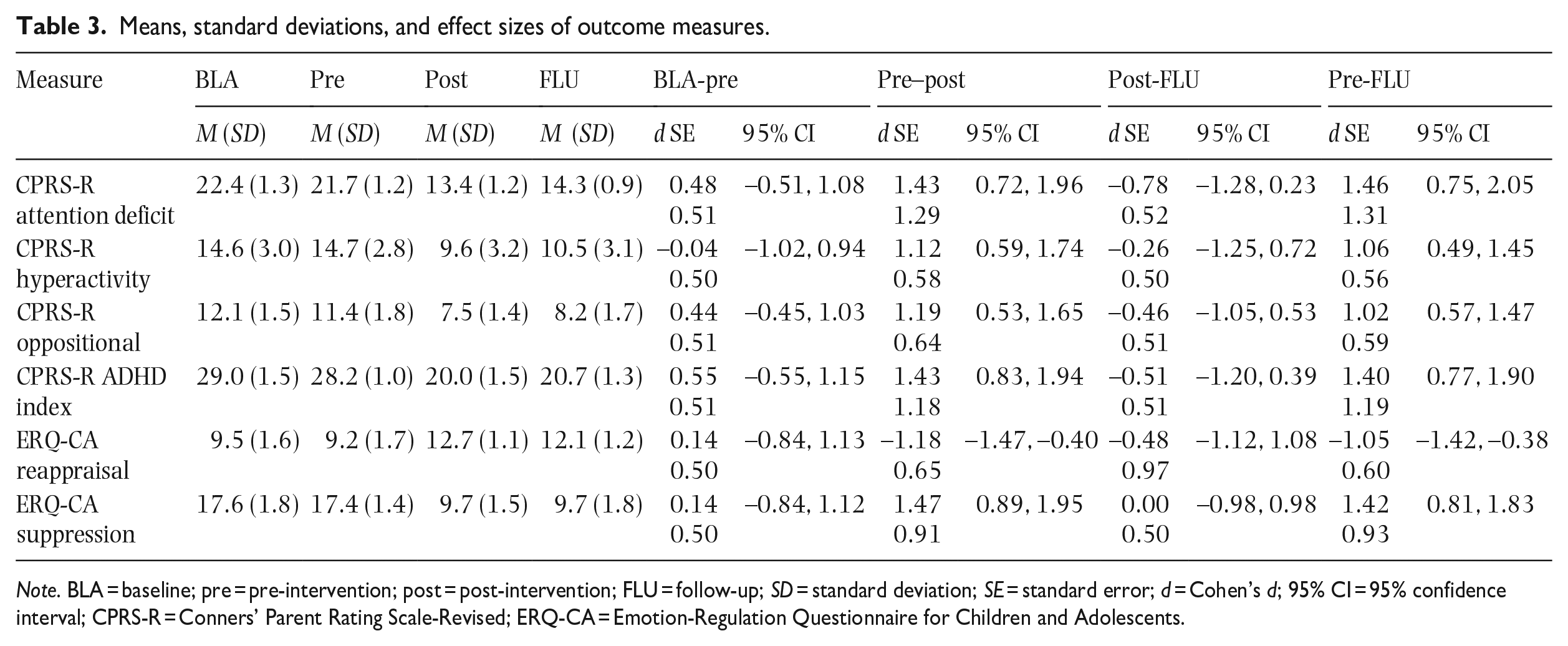
Note. BLA = baseline; pre = pre-intervention; post = post-intervention; FLU = follow-up; SD = standard deviation; SE = standard error; d = Cohen’s d; 95% CI = 95% confidence interval; CPRS-R = Conners’ Parent Rating Scale-Revised; ERQ-CA = Emotion-Regulation Questionnaire for Children and Adolescents.
Discussion
The aim of this single-case experimental study was to examine the effects of CBT with adjunctive music-based emotion-regulation skills training with eight adolescents with ADHD. The results demonstrate that the intervention was effective in treating the core symptoms of adolescent ADHD—cognitive (i.e., attention), behavioral (i.e., hyperactivity/impulsivity), and overall. Participants also showed decreased use of maladaptive and increased use of adaptive emotion-regulation strategies. The medium to large effects on the outcome variables are notable considering the relatively brief treatment duration.
Although the combination of CBT and adjunctive music-based emotion-regulation skills training has not been studied previously, our findings are consistent with those of previous reports that music-based interventions are effective for core ADHD symptoms and comorbid emotional–behavioral problems (Antonietti et al., 2018; Dursun et al., 2021; Maloy & Peterson, 2014; Zhang et al., 2017). Contemporary cognitive and behavioral models of ADHD (Antshel et al., 2014; Graziano & Garcia, 2016; Sprich et al., 2015; Sprich & Safren, 2020; Steinberg & Drabick, 2015) posit that many of the consequences of the core symptoms of this disorder are maintained or exacerbated by dysfunction in the self-regulatory system and lack of adequate emotion-regulation skills. Treatment that combines compensatory adaptive emotion-regulation skills training with the standard CBT protocol for ADHD may reduce the cognitive-emotional and cognitive-behavioral problems of people with ADHD (Rosen et al., 2019). Given that contemporary CBT is modifiable and flexible, it can be adapted to the specific needs of adolescents. The addition of adjunctive skills, such as the use of music-based emotion-regulation strategies, may augment the therapeutic benefits of CBT and be a cost-effective way of addressing not only the core symptoms of ADHD and also the self- and emotion-regulating processes that underlie them. Our findings suggest that this approach can be used to address the core symptoms of ADHD and improve the use of emotion-regulation strategies in adolescents. In future it may therefore play a role in the treatment of this population.
In the cognitive-behavioral approach, music is the mechanism for changes in cognitive-emotional and cognitive-behavioral components (M. M. Chan & Han, 2021). Although these data are preliminary, it may suggest that adding music to standard psychological treatments can play a role in the treatment of young people with ADHD since it provides them with a self-regulatory system (Antonietti et al., 2018). Many music therapists consider emotion regulation to be a potential benefit of music-based skills training and use music in therapeutic relationships to improve adolescents’ ability to manage/regulate their own emotions and use adaptive cognitive-emotional strategies (Aalbers et al., 2021; Marik & Stegemann, 2016). Since emotion regulation considered as an essential component of broader self-regulation system (Diamond & Aspinwall, 2003; Geva & Feldman, 2008), promotion of self-regulation competence through music helps them in the top-down and effortful executive control and enables them to manage/regulate the emotions and impulsive tendencies. The use of music to increase adolescents’ competence for regulating themselves helps them in their efforts to exert executive control, and manage their emotions and impulsive tendencies. If they can do this, they are better able to plan their behavior so as to meet the goals they have set for themselves (Antonietti et al., 2018). Because music-based emotion-regulation skills training works on the mechanisms underlying ADHD, it can improve the attention and cognitive performance of adolescents with ADHD and decrease their levels of hyperactivity and impulsivity. Although it is premature to make direct clinically based generalizations until future research have been conducted, these results provide evidence to support the use of music listening to facilitate emotion regulation and improve the core symptoms of ADHD in adolescents.
To understand and explain the reasons behind the augmenting effects of adding music-based emotion-regulation skills training to standard CBT for ADHD, it is important to understand the effects of music on the brain. Much of the literature is in the field of neuroscience and focuses on the neural mechanisms underlying music-based interventions. Music listening engages multiple areas of the brain, both cortical, such as the left and right primary auditory cortex and cortical motor area, and subcortical, including the medial geniculate body in the thalamus and the amygdala (M. M. Chan & Han, 2021; Thaut et al., 2015). Functional magnetic resonance imaging (fMRI) studies of music-based interventions have generally indicated that music listening induces widespread coactivations across various functional networks (Dursun et al., 2021; Maloy & Peterson, 2014). Music may indirectly influence the emotional, cognitive, and behavioral processing systems in such a way as to reduce the symptoms of ADHD.
When individuals listen to calming music, their emotions are regulated to a greater extent by top-down and effortful executive control that may result in the modification of the related features of ADHD, including negative affectively driven impulsive behaviors and emotional–behavioral dysfunctions. Music has long been thought to influence emotions and emotion-regulation processing (Marik & Stegemann, 2016; Moore, 2013). In general, emotion regulation is characterized by increased activation in the cognitive control and monitoring areas—the anterior cingulate cortex, orbitofrontal cortex, and lateral prefrontal cortex—which leads to decreased activation in the amygdala (Etkin et al., 2015; Gyurak et al., 2011; McRae et al., 2010; Ochsner & Gross, 2005). The neural correlates of emotion regulation suggest an interplay between the frontal lobe areas involved in cognitive control and the areas involved in emotional reactivity (Gyurak et al., 2011). The amygdala is the primary structure implicated in emotional reactivity (Etkin et al., 2015; McRae et al., 2010; Ochsner & Gross, 2005). Listening to relaxing music tends to reduce the activation of the amygdala, regulate emotions, decrease the secretion of stress hormones, and reduce fluctuations in mood (Antonietti et al., 2018; De Witte et al., 2020; İçel & Başoğul, 2021). When individuals listen to calming music, the amygdala registers the sensory input, processing tempo, rhythm, and notes to determine the emotional response and stimulate behavior accordingly (M. M. Chan & Han, 2021; Marik & Stegemann, 2016). Indeed, related studies have also shown that the theory-of-mind network (Koelsch, 2009), which is considered a higher order cognitive-emotional process and comprises frontotemporal regions, including the medial and superior temporal gyri (Whitehead & Armony, 2018) and the frontal brain regions (i.e., inferior frontal gyrus, orbital fronto-lateral cortex, and the anterior insula; Koelsch, 2005), is activated during music-based interventions. These findings regarding the neural mechanisms underlying music-based interventions provide a neurological foundation for the well-known effect that music can be used to regulate emotions, enhance cognitive performance, and control impulsive behaviors (Dursun et al., 2021; Hakvoort et al., 2013). From the neurological perspective, such findings may explain why music may contribute to reduced core symptoms of ADHD.
Moreover, neuroimaging studies have also shed light on the activation of the reward circuit in the brain when implementing music-based skills and the role that dopamine plays in this regard. Research shows that music increases dopamine levels in the brain (Maloy & Peterson, 2014; Yinger & Gooding, 2014). It has been reported that listening to music increases the activation of the vertical striatum, which includes the nucleus accumbens or “human reward system” (Blood & Zatorre, 2001, pp. 11819–11820). It has also been suggested that music might stimulate the production of certain dopamine receptors for people who are deficient in these receptors (Blum et al., 2010). Deficiency in dopamine receptor D2 is implicated in ADHD pathogenesis (Mariggiò et al., 2021; Wu et al., 2012). According to the optimal-stimulation theory and moderate brain-arousal (MBA) model for ADHD, optimal and moderate environmental noise allows for reduced neural background activity and a hypo-functional dopamine system in children with ADHD, and could improve cognitive functioning (Baijot et al., 2016; Söderlund et al., 2007). The MBA model for ADHD predicts that calming music may trigger the brain’s reward system and increase dopamine levels in the brain, and therefore help to regulate the emotions of and improve cognitive function in young people with ADHD (Baijot et al., 2016).
If music by its nature triggers the brain’s reward system, it is no wonder it often works as a strong motivator for patients who are generally not motivated to engage in therapy and have low adherence to treatment (Hakvoort et al., 2013; Maloy & Peterson, 2014). Since resistance to treatment, dropout, and withdrawal is common among ADHD adolescents receiving psychiatric care, it has been argued that treatment satisfaction and treatment adherence are important criteria in addition to treatment effectiveness (Bukstein, 2004; Evans et al., 2019; Lachaine et al., 2012). Consistent with these suggestions, our results show that adolescents reported high adherence to treatment, as they continued with it and carried out their homework diligently. This is particularly interesting given that other samples of young people with ADHD have exhibited low treatment adherence (Sibley et al., 2017). The importance of involving adolescents in treatment is well known and increases as they get older (Evans et al., 2019). Thus, adding favorable adjunctive treatment strategies adapted to the developmental needs and preferences of adolescents with ADHD may motivate them to engage in therapy and augment the therapeutic benefits of standard CBT. Although participants in the present study benefited from the intervention, more work needs to be done before definitive conclusions about efficacy can be drawn.
The results of this study should be interpreted in the context of its limitations. The measures included self-reported symptoms, so that, the effects of demand characteristics cannot be ruled out. It is difficult to generalize from the results of single-case designs, such as the one used in the study. The statistical analyses that could be performed were limited because of the small size of the sample of adolescents who took part. Another potential limitation is that the music and CBT interventions were combined; it was not possible to determine which of the two components was (more) effective or if they were effective because they were combined. Despite these limitations, the results suggest that it is worth continuing to evaluate combined CBT for ADHD augmented by music medicine, with larger samples, using a randomized controlled design sufficiently powered to detect outcome moderators and treatment mechanisms. Future research could also consider a three-armed design to distinguish between the effects of different treatments (i.e., a CBT-only condition, a music-only condition, and a combined CBT-music treatment).
The clinical implications of this study are that, as music has become increasingly accessible in individuals’ daily lives through online streaming services and portable music devices (Greenberg et al., 2020), it may be used to augment standard CBT for ADHD and increase its therapeutic benefits with minimal cost. Calming music, in particular, can be used to regulate the emotions indirectly. However, results are preliminary and the mechanisms through which music may affect ADHD symptoms and/or interact with psychotherapy remain unclear.
Footnotes
Acknowledgements
The authors are grateful to all participants in the research and all those who facilitated the implementation of the research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the University of Kurdistan Research Ethics Committee (IR.UOK.REC.1400.001), which follows the Declaration of Helsinki for the ethical principles of medical research involving humans.
Informed consent
Written informed consent was obtained from all parents and assent was obtained from all the adolescent participants.