
Abstract
This research analyses the role of accounting in British disablement pensions awarded to men who sustained shell shock during their Army service in the First World War. In this context, “accounting” refers to the classification of medical conditions when determining pension eligibility and awards. Pension classifications were prejudiced towards men with physical disabilities and against men with shell shock. Accounting classification’s ability to make a medical condition invisible is central to this research. The invisibility of shell shock as a medical condition in the pension classification system led to financial discrimination against men with shell shock. The immorality of this discrimination was hidden by a system of accounting classification that distanced decision-makers from the ramifications of their decisions. In addition, the Minister of Pensions adopted blame avoidance techniques to protect his Ministry and the British government from criticism occasioned by the discriminatory treatment of men with shell shock.
Introduction
Who are these? Why sit they here in twilight?
Wherefore rock they, purgatorial shadows …
Treading blood from lungs that had loved laughter.
Always they must see these things and hear them,
Batter of guns and shatter of flying muscles,
Carnage incomparable, and human squander
Rucked too thick for these men’s extrication.
1
Hines (1988) recognized that reporting choices made in accounting have the power to create reality. Our research supports this theme, examining classification of medical conditions for the purpose of awarding disablement pensions to men who had served in the front line of battle for the British Army during the First World War. We focus on the classification for disablement pension purposes of shell shock sustained through military service. Classification schemes for illness and disability are described in the health care literature as an accounting for illness (Barnes and Mercer, 1996; Bowker and Star, 2000; Davison et al., 1992; Meltzer, 1997). We view pension entitlement classification as accounting for illness. But the pension classification is more than an accounting for illness; it also placed a financial value on the sacrifice of men disabled while serving their country. Extant accounting literature on pension entitlements has focused on areas other than classification, including the emancipatory potential of the Internet in pension accounting (Gallhofer et al., 2006), accounting practices associated with pension entitlements (Kiosse and Peasnell, 2009; Napier, 2009) and the relationship between pensions and capital markets (Glaum, 2009). Our research brings the notion of pension classification as accounting for illness to the example of pension determinations for men disabled through shell shock to illustrate the power of accounting to make a medical condition invisible, leading to discrimination against those suffering from that condition. It is easy to dismiss historical research as an anachronism which only has relevance for a particular time and place, offering no lessons for contemporary society. However, illness classification systems continue to determine both medical and cost management of illness, hospital funding and treatment, and access to disability services, which indicates that accounting for medical conditions continues to be problematic (Friedman et al., 2006; Rapoport et al., 1990; van Tulder et al., 1995). We use a historical example to make visible accounting issues which may not be viewed as clearly through a contemporary lens because they might become enmeshed in political debate (Bonoli, 2000; Breyer, 1994; Crawford, 1977).
There is a contradictory irony in the British government expressing concern that its pension management of men disabled by shell shock was overly politicized and the subject of excessive public debate (Reid, 2010) when its classification system for pension entitlements increased Parliamentary and public debate by financially disadvantaging men with shell shock (Babington, 1997; Parry and Codrington, 1918). We have focused exclusively on shell shock as a disabling condition because there was disagreement in the British medical community and British Army on whether it was a legitimate medical condition, both on its cause and treatment. This impacted on pension entitlement decisions for men with shell shock. Table 1 provides the medical classifications used for determining pension entitlements from 1917, when they were at their most detailed, and illustrates that despite the prevalence of shell shock among returning soldiers, the focus of the classification schema was on physical wounds so shell shock did not feature as a discrete medical condition.
Extract from Ministry of Pensions’ classification for military disablement pensions (Ministry of Pensions, 1919).
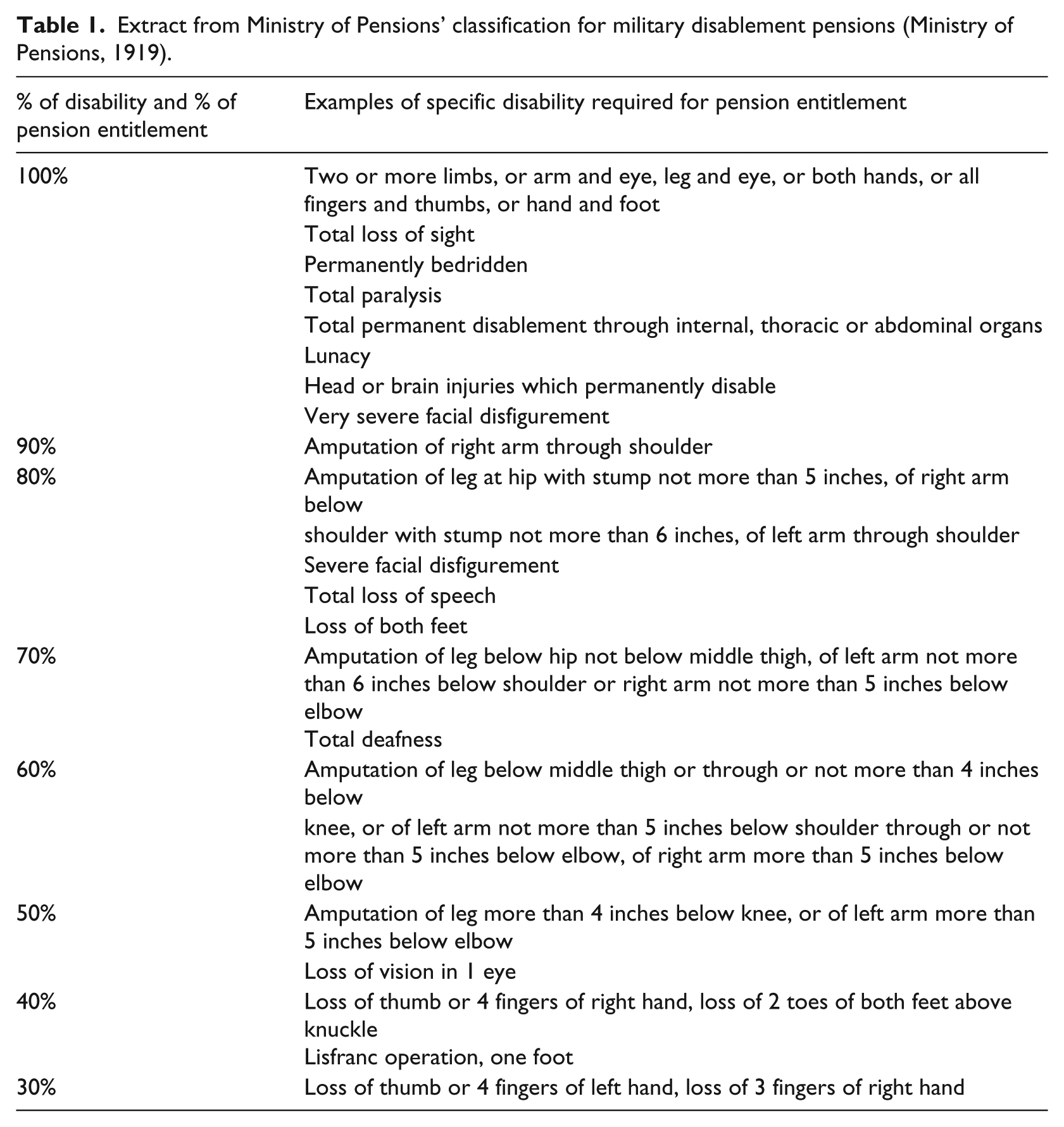
The categories shown Table 1 are given in full. Pension awards below 20 per cent have been excluded because each category includes an extensive list of medical disabilities. However, shell shock, other terms commonly used for shell shock and references to other related psychological conditions are not included in these categories.
The First World War was the first time the term “shell shock” had been used, although symptoms consistent with shell shock had been identified since ancient times (Babington, 1997). Shell shock refers to a set of symptoms which can include loss of hearing, speech, sight, movement control or cognitive abilities, an appearance of concussion without a head trauma injury, or fear ranging from a desire to flee the battle area to a catatonic state. During the First World War, desire to flee a battle area was a particularly contentious symptom; the British Army viewed it as cowardice rather than the symptom of a legitimate medical condition (Head, 1916). Hence, men with shell shock may have been executed as cowards for failing to obey orders to fight (British Expeditionary Force, 1922). The term “shell shock” was both used in medical diagnosis and common parlance during the period covered by our research, so we have used this term. However, other medical nomenclature of the period included nervous disorder, neurasthenia, commotion, hysteria, weak heart, nervous disorder of the heart and insanity (Babington, 1997). Contemporary nomenclature for this medical condition is post-traumatic stress syndrome. Although our example is limited by time and context, equitable pension determinations for those disabled by war whose medical condition may not manifest in clearly definable symptoms, which is the case with post-traumatic stress syndrome, continues to be problematic and contentious (Forbes et al., 2001; McDonald and Calhoun, 2010). Our historical example was selected because it reflects contemporary debate on pension entitlements for those with post-traumatic stress syndrome, highlighting issues of accounting classification while avoiding the politicization and emotion surrounding the entitlement debate (Bichescu et al., 2007; Stubbs and Soroya, 1996; Wessely and Deahl, 2003).
The period covered by our research was one of major cultural change in Britain (Eksteins, 2000). Accounting processes were changing in an effort to introduce scientific approaches to cost calculation (Boyns and Edwards, 2007). The Institute of Cost and Management Accountants was established during this period (Loft, 1986), and although the British government used accounting information primarily for expenditure control (Funnell, 2006; Miley and Read, 2014), it actively encouraged its private sector suppliers to implement scientific management practices that would enable them to use accounting information for costing decisions. This was done to ensure the British government was not overcharged for resources acquired from the private sector as part of the war effort (Boyns and Edwards, 2007; Brown, 1998).
Our research uses primary resources when available, including official transcripts of Parliamentary debates, reports by the Ministry of Pensions, a post-war inquiry by the War Office into the management of shell shock (War Office Committee of Inquiry into Shell Shock, 1922), a report on war pensions by two members who served on the Ministry of Pensions Appeal Tribunal throughout the war (Parry and Codrington, 1918) and the case histories of British Army doctors who specialized in the treatment of shell shock cases (Mott, 1919; Myers, 1916; Rivers, 1918a; Salmon, 1917; Smith and Fear, 1917). Throughout the period covered by this research, the Minister of Pensions was required by legislation to ensure that the Ministry and its Medical Pensions Boards “kept proper and sufficient accounts” of all their deliberations (for example, War Pensions Act, 1920: section 5). The Minister was also responsible for appointing a finance officer to keep accounting records of all payments. However, this was not done for the purpose of internal or external reporting but to ensure payments from public money complied in amount with pension determinations (War Pensions Act, 1920). The Ministry of Pensions maintained detailed accounting records of pension applications, pension entitlement decisions and the amounts paid to each pensioner. Annual pension statistics of the total cost of disablement pensions and the cost per pension classification category were also maintained, although this information was not publicly disclosed during the war (Ministry of Pensions, 1919). Although mere speculation, disclosing the number of men disabled during their military service may have deterred men from enlisting, been considered bad for public morale and caused public debate on the value of ongoing war participation. The Ministry of Pensions did not keep statistics on the number of pension applications rejected or downgraded. However, Parliamentary debates, a post-war British government report by the War Office and records of the Ministry of Pensions’ Appeal Tribunal, all of which use the term “shell shock” in preference to other medical terms, refer to the frequency with which the Ministry of Pensions rejected or downgraded the pensions of men with shell shock, and state that the majority of complaints with pension determinations are from men with shell shock (Committee of Public Accounts, 1918; Parry and Codrington, 1918; War Office Committee of Inquiry into Shell Shock, 1922). It is from the detailed examination of individual pension and hospital records by medical historians that statistics are available showing which pensions were awarded to men with shell shock (Jones, 2007; Jones et al., 2002). Their analyses are based on symptoms consistent with shell shock disclosed in individual pension files. Without this research contribution it would not be possible to identify which men suffered from shell shock. In addition, hospital records are available for the number of men treated at hospitals established exclusively for the treatment of severe shock, and public hospital records for men treated as in-patients or out-patients, although this understates the number of men with shell shock by excluding those treated by private doctors and men who did not receive treatment (Jones, 2007).
The next section provides further background on shell shock and the moral dilemma it presented to the British Government. This is followed by a description of the application of the disablement pension system and discussion of the contribution of this example to enhancing our understanding of accounting. The analysis draws on extant research on blaming, distancing and scapegoating to highlight how the accounting classifications used by the Ministry of Pensions discriminated against men with shell shock. The pension classification system purported to cover all examples of war disablement (British Expeditionary Force, 1922) but the reality was financial inequity for men with shell shock vis-à-vis other forms of disablement so that men who were victims of shell shock then became victims in a pension system with discriminatory accounting classifications.
Background
In this section, we introduce factors that impacted on disablement pensions entitlements for men with shell shock. First, it was poorly understood as a medical condition. There was neither an accepted definition nor accepted medical protocol for diagnosis and treatment (Webb, 2006), which led to considerable doubt about the genuineness of those claiming battle trauma. Second, the lack of consistent and readily determinable symptoms that could always be described as shell shock contradicted prevailing medical understanding of illness and confounded pension decision-makers. The image of the shell shocked soldier has become synonymous with the First World War (MacLeod, 2004). The high incidence of shell shock diagnoses among officers and enlisted men in the British Army impacted on Britain’s ability to maintain an adequate fighting force during the war and on pension and medical costs both during and after the cessation of hostilities (Babington, 1997). It challenged British notions of masculinity and had significant economic implications when formerly able-bodied men were unable to return to civilian employment following their war service and sought pension entitlements for disablement that did not include a physical battle wound (Holden, 1998). Britain borrowed heavily to finance participation in the First World War (Mitchell, 2011), so its burgeoning debt problem was compounded by the financial demand from the large number of pension claims. In this section, we also address the uncertainty concerning the number of men with shell shock, which was a consequence of the lack of medical protocol and an imprecise understanding of the condition, but which means that it is not possible to be precise about the magnitude of the pension problem described in this research. We can only present estimates of the magnitude of the problem, so although we refer in our research to sources such as Parliamentary debate records where pensions for men with shell shock were frequently discussed, quantitative data must necessarily be replaced by inferential qualitative data in this area of research.
An issue for the British medical profession was whether shell shock could exist without obvious physiological injury such as a battle wound. When first identified in 1914, shell shock was considered a physical trauma to colloidal tissue of the spinal column or brain caused by the force of exploding shells from heavy artillery, which is why it was termed “shell shock” (Myers, 1916). However, when casualties with similar symptoms but who had not been near exploding shells began to present in large numbers, doctors sought other explanations and antipathy towards a diagnosis of shell shock commenced (Smith and Fear, 1917). Although psychological battle trauma was suggested, physiological explanations for shell shock prevailed. This reflected medical knowledge of the time, the British medical profession’s distrust of psychiatric methods and the British medical profession’s lack of professional recognition for psychiatry. Psychiatric illness, the diagnosis and treatment of which were in their infancy, was maligned in Britain in the nineteenth century, when the pejorative term “railway spine” became popular to describe people who claimed spinal pain following involvement in a railway accident when there was no sign of physical illness. Shell shock patients were often said to have railway spine. It was only following successful post-war treatment of shell shock as a psychiatric illness that attitudes towards the condition and psychiatry gradually improved and the British medical profession started to review its attitude towards men with shell shock (Rivers, 1917, 1918a, 1918b).
Although the British medical profession was divided on whether shell shock was a genuine medical condition, the British Army did not accept shell shock as a legitimate condition. The British Army’s official position was that shell shock symptoms were either cowardice or the exacerbation of a pre-existing nervous disposition (War Office Committee of Inquiry into Shell Shock, 1922). Mental illnesses, at this time, were considered to be hereditary (Freeman, 2010), so if someone was exhibiting symptoms it must have come from a previously undiagnosed inherited mental illness, not from war service. The Army did not consider prior medical histories when recruiting men, except in cases of a prior hospitalization for insanity which disqualified a man from Army service. The Army view that shell shock was the aggravation of a pre-existing condition was not based on empirical evidence (War Office Committee of Inquiry into Shell Shock, 1922). The Army contended that the shorter training period for recruits necessitated by war prevented Army officers identifying men of nervous disposition who in normal circumstances would not get through recruit training, and hence men of a nervous disposition were being sent into battle (War Office Committee of Inquiry into Shell Shock, 1922). Moreover, the Army’s position was that a nervous disposition was a self-inflicted phenomenon for which a man should not receive sympathetic treatment. Otherwise, other men would be encouraged to feign similar symptoms to avoid front-line fighting.
In 1916 the Army forbade use of the term “shell shock” in medical diagnosis (British Expeditionary Force, 1922), although some Army doctors ignored this command. Army diagnoses were often hastily made as doctors attempted to classify all men wounded in battle by their medical condition. The primary role of this classification was to identify men who could be treated and returned to front-line fighting (War Office, 1911). Once the use of the term “shell shock” was banned, Army diagnoses for men with shell shock could be purposely vague because what mattered was not the medical diagnosis but a recommendation that a man receive further treatment away from the front line (van Bergen, 2009). Hence, a medical diagnosis might only state one debilitating symptom, such as blindness or deafness (War Office Committee of Inquiry into Shell Shock, 1922) or be intentionally misleading. Medical records for Craiglockhart, a hospital in Scotland that only treated men with severe shell shock, indicate that rather than a diagnosis of shell shock, Army patient records sent with a patient due for hospital admission could contain imaginative diagnoses to overcome the Army’s ban, including migraine, gas poisoning, glycosuria, a compound fracture of the toe and haemorrhoids (Webb, 2006). These records were used by the Ministry of Pensions when making pension determinations. The diagnostic word games to get round the Army ban could leave men with shell shock unable to provide evidence of any symptom that fell within the compensation classifications. Other medical evidence could be admitted, but a Ministry of Pensions Medical Review Board was under no obligation to consider it, leading to inconsistency both in terms of the medical evidence considered in making a pension determination and in the pension award itself (Parry and Codrington, 1918). The Ministry of Pensions did not keep accounting records of rejected applications so there is no way to ascertain whether imaginative diagnoses prevented men receiving pensions, although men with shell shock whose pension applications had been rejected were the largest group of appellants seeking review of their pension determination and the review panel has indicated that the imaginative diagnoses by Army doctors plus the reluctance of Pension Medical Boards to admit other medical evidence led to most pension application rejections (Parry and Codrington, 1918). The attitudes towards shell shock of both the British Army and British medical profession are important because both groups could provide information upon which pension entitlement claims were assessed and both groups were directly involved with determining entitlement awards. Their involvement is discussed in the following section.
The number of men with shell shock seeking medical attention or pensions, and the number and amount of pensions awarded to men with shell shock are not known precisely because of the imprecision of medical and pension record-keeping. The British Army kept detailed records of all men who received medical treatment at its various medical aid posts but its records do not help determine the number of men with shell shock likely to seek pensions because of the Army ban on the term “shell shock”. No statistics on men seeking pensions or the number of pensions awarded were published during or immediately after the war; it may have been considered bad for morale to reveal this information, if it was kept. The total amount allocated to pensions was reported to Parliament, as were amounts allocated to defence and total budget allocations because this spending required Parliamentary approval. The amount allocated to defence, as expected, increased during the war years (Figure 1), which necessitated substantial borrowing (Figure 2), primarily from the United States. Post war, pension expenditure increased (Figure 1), contributing to budgetary pressures impairing Britain’s ability to repay this debt.

Comparison of amounts spent on pensions and defence for the years 1914 to 1923 (millions) (Mitchell, 2011)

British government debt for the years 1914 to 1923 (millions) (Mitchell, 2011)
Being able to avoid or limit pension spending on men disabled by shell shock would have helped the government reduce its expenditure, mitigating to an extent the budgetary pressures imposed by servicing and, potentially, reducing the wartime debt.
Complicating factors in researching this area are record-keeping imprecision and/or a lack of record-keeping. With neither an established medical diagnosis for shell shock nor an agreed medical nomenclature for the condition, it is difficult to estimate the number of men with shell shock, and so this cannot be used as a proxy indicator of the number of disablement pensions. For instance, in December 1914, when the British Army was using inter alia the term “shell shock” to describe battle trauma symptoms, 7 to 10 per cent of British officers and 3 to 4 per cent of non-officers were diagnosed with shell shock (MacLeod, 2004). Between July and December 1916, although the British Army had banned the use of the term “shell shock” in an attempt to hide the magnitude of the problem (Miley and Read, 2015; War Office Committee of Inquiry into Shell Shock, 1922), over 16,000 new diagnoses of shell shock were made plus an unspecified number of diagnoses not labelled “shell shock” but which encompassed shell-shock-like conditions (MacLeod, 2004). Extant research using officer diaries and army reports indicates that approximately 40 per cent of battle casualties and over 30 per cent of cases of men discharged from the Army during that period suffered from shell shock (Merksey, 1979). Mott (1919), a doctor who worked exclusively in the treatment of shell shock casualties, estimated that one seventh of all men discharged as medically unfit from the Army suffered from shell shock. In October 1917 Salmon (1917), a doctor working exclusively in shell shock rehabilitation, determined that if all men with wounds were excluded, shell shock accounted for one third of the men discharged from the British Army and that between 80,000 to 100,000 men suffered shell shock symptoms severe enough to require discharge and ongoing medical treatment. Although the figures are imprecise, all suggest shell shock was a significant cause of battle disablement, and so it is not a large leap to posit that many of these men sought pensions for their disablement. Since the Ministry of Pensions did not recognize shell shock as a medical condition for disablement pension purposes, figures for shell shock pensions are unavailable. However, Britain’s official war history indicates that in 1921 65,000 men received pensions for symptoms consistent with shell shock (Cruttwell, 1934; Johnson and Rows, 1923) out of a total of 1.3 million pensions awarded (Reid, 2010). Despite not recognizing shell shock as a medical condition, in 1939 the Ministry of Pensions stated that more than 120,000 men were receiving pensions as a result of shell shock, although contemporary analysis of the Ministry of Pensions’ documents suggests that this may have been an overstatement (Jones et al., 2002). Despite the uncertainty concerning the statistics, the amount paid in pension entitlements to men suffering from shell shock, and which could have been paid by a more sympathetic pension regime, would seem substantial. This caused consternation to a government attempting to manage escalating debt by decreased spending (Mitchell, 2011) and led to pension entitlements for shell shock becoming a target for cost cutting (Parry and Codrington, 1918). This is discussed in the following section.
Accounting for disablement pensions
Prior to the First World War, military pensions had been a discretionary grant from the British monarch, on whose behalf the Army Council handled the practical administration of Army pensions, devolving this responsibility to the Central Army Pensions Issue Office and the Chelsea Hospital Commissioners (Parry and Codrington, 1918). The overriding consideration in pension determinations by the Crown was that soldiers did not suffer any loss of their former living standard due to disablement. The Army Council ensured accounting records could demonstrate this; the overriding purpose of accounting records was to demonstrate financial equity between a soldier’s living standard before and after any event that precluded the soldier from continuing his military service (Parry and Codrington, 1918). At the outbreak of hostilities in 1914, the monarch handed all pension control to the British Government, thus the First World War marked the first time the British government had undertaken the determination and management of Army pensions or needed to consider the impact of military pensions on public finance. In this section we describe the period between the outbreak of war and 1923, which can be viewed as four distinct periods in terms of the approach used by the British Government towards disablement pension classification. Throughout this period, the focus in pension record-keeping was on financial efficiency; records were kept to demonstrate to the government the amount spent on pensions and that no money over the amount authorized by a pension determination was paid out of public money to a pensioner (War Pensions Act, 1920; Parry and Codrington, 1918).
Period 1: 1914–August 1916
This period was marked by a lack of policy and confusion concerning disablement pension management. The British Government did not have a process for determining disablement pensions and shared responsibility among the Chancellor of the Exchequer; the Secretary of War; the Treasury; the Admiralty (only for Navy pensions); the War Office, whose delegation was exercised by the Army Council with assistance from the Central Army Pensions Issue Office; the Chelsea Hospital Commissioners; and the Royal Patriotic Fund Corporation, a fund established pre-war to receive private donations given to the Crown to supplement Royal pension grants. Without clear lines of responsibility, the British Government’s response was to continue paying pensions awarded by the Crown without making any new determinations (Parry and Codrington, 1918).
In November 1914, Opposition politician Hayes Fisher proposed a unified pension system, arguing men from all levels of society were foregoing current employment to fight as private soldiers so should know they would receive ongoing pension entitlement if unable to resume employment through wartime disablement. This proposal was rejected by the British Government as revolutionary and unnecessarily drastic (United Kingdom, 1914). By May 1915 it became evident to the War Office that to encourage large numbers of men to support the war effort by leaving civilian employment for temporary wartime military service, the British Government must provide disablement pension entitlements equivalent to civilian workers’ compensation (Reid, 2010). While a process was being developed, all pension payments were stopped, creating hardship for many veterans and their families (United Kingdom, 1915: cc2106–16).
The British Government gave the Royal Patriotic Fund Corporation statutory responsibility to determine the pension scheme. It was assisted by local and district committees established in each borough. Committee members were recompensed for administrative expenses from the private donations previously received by the Royal Patriotic Fund Corporation to supplement Crown pension payments (Parry and Codrington, 1918). Donors were not notified that their donations had been applied to this purpose and there was no publicly available accounting record of this expenditure (Parry and Codrington, 1918). The Royal Patriotic Fund Corporation proposed a pension of 25 shillings per week for total disablement and the difference between the pensioner’s income from other sources and 25 shillings per week for partial disablement. There was concern that the pension entitlement might be insufficient, requiring local government supplementation (Parry and Codrington, 1918), but due to disagreement among the local committees, this scheme was not implemented so the issue of a sufficient entitlement was not resolved.
Period 2: 1916
This period was marked by the introduction of a government pension scheme applicable to all men disabled through war service and is the first time that the classification of pension entitlements led to discrimination against men with shell shock. In September 1916, politician Hayes Fisher’s political party had joined the government and he introduced a standard disablement pension scheme. The Ministry of Pensions was established to determine and control Army pensions (Ministry of Pensions, 1919). A pension determination was made following medical discharge from the Army and there was no provision to review decisions. To allay concerns that physically unfit men would undertake military service for a few months, be discharged as unfit and be awarded a pension for life, the scheme provided that disablement caused by military service gave a pension for life whereas disablement due to a pre-existing condition aggravated by military service gave a pension until a Pension Medical Board comprising three doctors determined the medical condition had returned to its pre-war state. This distinction between disablement caused by or aggravated by war service was not applied to physical wounds since it was easy to establish whether they had occurred during military service, so it was only applied to pension determinations for men with non-physical conditions, which included shell shock (Ministry of Pensions, 1919: 152).
In accordance with its official position, shell shock was described in British Army discharge reports using a range of other terminology and was always stated to be an exacerbation of pre-existing condition. Pension determinations were usually based on British Army discharge medical records, though other medical evidence could be referenced (Jones, 2007). Evidence from the Pensions Appeals Tribunal indicates that outcomes of pension determinations for men with shell shock were predictable and did not favour the claimant (Parry and Codrington, 1918). The apparent prejudice in pension determinations against shell shock was exacerbated by the antipathy in the British medical profession towards recognizing shell shock as a legitimate medical condition (War Office Committee of Inquiry into Shell Shock, 1922).
As part of the 1916 pension scheme, the Ministry of Pensions established a system based on assessed level of disability. All existing pension holders were re-assessed and re-classified, receiving 100, 75, 50, 25 or 0 per cent of the total disablement pension. The percentage entitlement was determined using detailed descriptors of the type of disablement at each pension payment level. These descriptors, which were later broken into additional categories, are listed in Table 1.
The 1916 scheme led to significant cost savings for the British Government since previously all pensioners had received a full pension entitlement for life (Jones et al., 2002). The Financial Secretary to the War Office expressed concern in Parliament that because pension reviews were based on case notes rather than new medical examinations, men with shell shock might be treated too generously under the pension scheme and proposed that their pensions should be reviewed regularly to take into account improvements in their condition; there was no suggestion that this should also happen with physical wounds (Parry and Codrington, 1918). A result of the prejudice against shell shock in Army medical records and among doctors making pension determinations was that many men with shell shock lost pensions awarded prior to 1916. Termination of a pension made a man ineligible for publicly funded medical treatment and eligible for re-enlistment in the Army. This led to some men with shell shock being returned to front-line fighting (War Office Committee of Inquiry into Shell Shock, 1922).
Only men in receipt of full pensions were entitled to medical care funded at public expense. Public concern about the number of men with shell shock no longer eligible for publicly funded medical care and with insufficient means to afford private care led to private money-raising campaigns to fund free private hospitals for men with shell shock, decreasing the total cost of public health care as the number of men treated at public expense decreased and providing an additional cost saving to government (Holden, 1998) while shifting part of the medical cost burden to the private sector. However, this improved government health statistics, which were based on the number of public patients, allowing the government to use the statistics to suggest that public health treatment was curing men with shell shock (Reid, 2010).
Period 3: 1917–18
This period was marked by express attempts to cut pensions as a mechanism for government cost saving. As with all changes to the pension scheme, men with shell shock were not the only group to be financially disadvantaged by the changes. However, it is this group that is the exclusive focus of our research because their disadvantage was greater than that of men with physical medical conditions, whose pensions could be reduced as part of a pension reform agenda but were rarely terminated or disallowed, as happened to the majority of men with shell shock (Holden, 1998). In 1917, £40,000,000 pounds was spent on disablement pensions (Ministry of Pensions, 1919; Mitchell, 2011). A more detailed breakdown of pension expenditure is unavailable. The Minister of Pensions announced that changes to the pension scheme were expressly intended to control escalating disablement pension costs, lessen the number of men on pensions and make more men eligible for recruitment to boost the Army (Parry and Codrington, 1918). All pensions were reviewed using a new scale that set awards at increments of 10 per cent. Hence the level of disability was assessed to be 100, 90, 80, 70, 60, 50, 40, 30, 20, 10 or 0 per cent. Table 1 provides further detail on this classification scheme. Under the new scheme, those found to have disablement of less than 10 per cent were ineligible for a pension. The British Government stated this was an administrative efficiency and cost saving to prevent men claiming excessive amounts for their disablement, even though claimants had no part in their own pension determination (Parry and Codrington, 1918). All pensions were reviewed and pensions for non-physical conditions such as shell shock were lowered or revoked (Ministry of Pensions, 1919). The Ministry of Pensions cited this as evidence of previous pension overpayment, blaming men with shell shock for taking pension overpayments (Minister of Pensions, 1917), even though pension payments were the sole responsibility of the Ministry of Pensions.
At the same time, the British Government attempted to defray the escalating cost of war pensions by shifting the burden back onto the public. The Naval and Military War Pensions, &c. (Administrative Expenses) Act 1917 c. 14 gave the Minister of Pensions power to accept and administer private donations towards war pensions. These funds were outside Parliament’s legal control, making the Minister a private almoner. This money was not kept separate from government money and no publicly available accounting for its use was provided (Parry and Codrington, 1918: 116). To lower the cost of Pension Medical Boards, board membership became voluntary and boards were established in any regional town that could furnish volunteers to staff a local board (Parry and Codrington, 1918). Previously, a measure of consistency in decision-making occurred because a small pool of doctors staffed a central Pension Medical Board but the plethora of decentralized boards operated independently. A change was made to the composition of the local boards. Whereas three doctors had staffed the central board, local boards comprised two doctors and an Army officer with a casting vote who chaired all the meetings. This was problematic for men with shell shock who sought a pension using criteria such as deafness or blindness, which can be symptoms of shell shock, because the Army’s stated position was that there was no such thing as shell shock (Holden, 1998).
Under the classification scheme introduced in 1917, pension entitlements were based on the most debilitating medical condition in the classification schema at the time of a pension determination. Shell shock symptoms could change or fluctuate in severity over time, further disadvantaging men in a system where there was no opportunity for a pension review if a condition worsened and where the pension descriptors favoured those with physical injuries. Under the scheme, if the most debilitating medical condition as determined by a Pension Medical Board was not covered by the descriptors, a pension entitlement was revoked irrespective of other symptoms (Parry and Codrington, 1918) adding to the inequity towards men whose most debilitating symptom was rarely a physical one found in the classification descriptors.
In 1917, the Minister of Pensions stated that any pensions awarded to men with shell shock would be reviewed because shell shock was a psychological condition that men could control in all but the most severe cases (Babington, 1997). This was consistent with the Army’s view (British Expeditionary Force, 1922). It is not clear whether the presence of Army officers on local boards influenced this view, whether it was a consequence of a similar view held by the Minister of Pensions or whether the coincidence of views was coincidental. However by 1917, this view contradicted prevailing medical opinion which was shifting to recognize shell shock as a legitimate medical condition occasioned by battle trauma, although the extent to which it was physiological or psychological remained subject to dispute (Mott, 1919). The Minister for Pensions also stated that pensions for shell shock would be its main target area to achieve cost savings (Parry and Codrington, 1918). In subsequent appeals against decisions that cut or revoked pensions, the Pensions Appeals Tribunal stated it could not consider assertions of inequity in the policy that drove pension changes but could only determine whether the pension rules as they stood had been applied (Parry and Codrington, 1918). Although Parliament and the Pensions Appeals Tribunal stated that many pensions were revoked as a consequence of this review, exact numbers were not provided. Whether this is because numbers were unavailable or secret is unknown. Similarly, the number of men returned to Army service was not disclosed. The intention and impact of these pension changes was to simultaneously lower pension payments while increasing the Army’s fighting strength (Committee of Public Accounts, 1918; Parry and Codrington, 1918). The morality of sending men with shell shock back to the situation that caused their shell shock is beyond our comprehension, but it is also beyond the scope of this research. There is no doubt that men with shell shock were targeted; the Minister of Pensions stated this in Parliament. The Chancellor of the Exchequer, Financial Secretary of the War Office and politicians from all parties spoke in Parliament against both targeting men with shell shock for pension reduction or revocation to save costs and re-enlisting men with shell shock. Concern was also expressed in Parliament about Army chairmen of local boards being under Army direction to destroy medical information on shell shock and to override any decisions by medical members of a Pension Medial Board that treated men with shell shock sympathetically (United Kingdom, 1917: cc1996–2114).
We note that even a full pension could cause financial hardship, so it was not only men with shell shock who suffered financially under the pension system. A full disablement pension of 40 shillings per week was less than what was earned by an unskilled builder (84 shillings and 6 pence per week), a coal mining labourer (99 shillings and 3 pence per week) or a skilled coal getter (135 shillings and 6 pence per week). Pensions did not increase for dependents and there was no government plan to re-train ex-servicemen or help them return to employment (van Bergen, 2009). The Minister of Pensions refused to review cases raised in Parliament that involved financial hardship or gross inequity, stating that Pension Medical Board decisions were final. This forced many men to seek local government relief for financial hardship, shifting the cost burden from national government to local boroughs, which varied in their financial capacity and the level of support they could offer (United Kingdom, 1923b: cc2573–7). There are instances of the Minister supporting pension boards despite the hardship or unfairness caused by pension decisions, including cases where men hospitalized with shell shock had their pensions revoked and therefore lost their eligibility for public health care and became eligible for re-enlistment into the Army (see examples in Parliamentary reports at HC Deb 19 February 1918 vol. 103 cc589–90 and HC Deb 11 April 1922 vol. 153 cc335–81). The Pensions Appeals Tribunal was only available to those who could afford legal representation, but legislation gave the Minister of Pensions an overriding discretion to change decisions although there are no records of the exercise of this discretion in pension cases concerning men with shell shock. If such discretion was ever exercised, the records, if made, have been destroyed or lost. We do not suggest evil intent; many public records were destroyed in the bombing of London during the Second World War.
Period 4: 1919–23
This was the immediate post-war period when Britain sought to cut government spending to manage the national debt, which rose from £754 million in 1913 to £7,414 million in 1919 (Mitchell, 2011), and disablement pensions were viewed as a lucrative source of funds, rather than just recompense for men disabled in the service of their country (Eksteins, 2000; Jones et al., 2002). In 1919 British Government policy was to return the currency to a pre-war gold standard, which required reversal of its deficit, and so post-war fiscal policy was aimed at debt reduction through reduced government spending (Aldcroft, 1973). In this economic climate and with high post-war unemployment, the Minister of Pensions targeted shell shock again, expressly stating that all pensions for men with shell shock would be reviewed as a contribution to fiscal austerity and leading to these pensions again being lowered (Jones et al., 2002) and subsequently revoked by the Treasury, Auditor-General or Committee of Public Affairs, even though they did not have legal jurisdiction over pensions (Parry and Codrington, 1918). The British Government supported the revocations as consistent with the need for cost-saving and as evidence that Pension Medical Boards had been too lenient in the past with pension determinations for men with shell shock (Committee of Public Accounts, 1918: para. 10; Parry and Codrington, 1918).
Additional cost savings were achieved through administrative and accounting measures. Pensions commenced from the date of a pension determination, not the date of discharge, even though it could take months for a pension deliberation to be made (Parry and Codrington, 1918). Whenever pensions were reviewed, all pensions were stopped but when payments recommenced, there was no money for missed pension periods (United Kingdom, 1918: cc1839–43). The Minister of Pensions refused to re-open cases that had been subject to appeal, even when inaccurate pension accounting records caused injustice. For instance, on 8 September 1919 H.G. Norton was discharged from the Army with shell shock described as neurasthenia, was totally immobile and so determined permanently unfit and awarded a 100 per cent pension entitlement. Two months later, the pension was cancelled. Under the pension rules, a successful appeal gave a right to have the pension reviewed. It did not give the right to have a pension reinstated. After successfully appealing through the Pensions Appeals Tribunal, Norton’s case was reviewed by a Pension Medical Board on 29 January 1920, which, on the same medical evidence, determined his disability to be 30 per cent. The reviewing board held that on enlistment, his disability was 20 per cent, even though his enlistment records showed no evidence of a disability, he had been found fit for military service without medical impediment by the British Army and there was no pre-war medical evidence of a disability. Evidence of his fitness on Army recruitment was dismissed by the Army chairman of the reviewing board because he determined that Army tests of medical fitness differed from pension tests of medical fitness. No justification for this was provided. The Ministry of Pensions determined that Army service had therefore caused a 10 per cent disability which was too small for a pension but Norton would receive a gratuity of £5. The pension ceased but the gratuity was never paid. When this matter was raised in Parliament as a case of improper Ministry of Pensions’ accounting, the Minister of Pensions refused to investigate it, arguing it had been reviewed and there was no requirement for the Minister to re-open cases of accounting irregularities (United Kingdom, 1922a). Extant research indicates that all injustices from inaccurate accounting records that were mentioned in Parliament or raised in a formal appeal pertain to pension entitlements for men with shell shock (Holden, 1998; Parry and Codrington, 1918).
The Minister of Pensions did not believe accounting practices needed to be reviewed despite evidence of their inadequacy (United Kingdom, 1922b). For instance, Lieutenant Verity was discharged from military service as an invalid suffering from tuberculosis. He was awarded a full 100 per cent pension by the Army. However, the Ministry of Pensions paid a 30 per cent disability pension for shell shock. During Parliamentary questioning, the Minister of Pensions refused to review the case because Ministry of Pensions’ accounting records stated that Verity had shell shock, despite medical evidence that he had never had shell shock and was still being treated for tuberculosis. On further questioning, the Minister of Pensions reiterated his decision but admitted the Ministry had no record of Verity’s disability and that its accounting records were insufficient to determine whether other classification errors had occurred (United Kingdom, 1922b: cc1423-4).
Accounting issues worsened in 1921, when the pension process was split: despite its stated antipathy towards men with shell shock, the Army was made responsible for Army pension determinations while the Ministry of Pensions managed pension payments (Babington, 1997). Simultaneously, the British Government determined that only medical conditions evident within seven years of the date of discharge were eligible for pension entitlement (United Kingdom, 1923a: cc1548–9). This disadvantaged men with shell shock since it was the only known medical condition at the time where symptoms could manifest many years later (Johnson and Rows, 1923; Reid, 2010). In the post-war period, the Ministry of Pensions started reporting pensions awarded to men with shell shock, although shell shock was still not recognized as a discrete pension descriptor. In 1920, 3,700 pensions were awarded to men with shell shock (United Kingdom, 1920: cc241-242), rising to 6,900 in 1923 (United Kingdom, 1923a). These figures may be inaccurate since they are based on the Ministry of Pensions’ view of which applicants had shell shock, but they also suggest a softening in the position on shell shock and pension entitlement. Whether this represents a change in position or rhetoric is unknown. In 1923 the War Pensions Acts 1915 to 1921 Amendment Bill 1923 changed the onus of proof in disablement pension cases from the claimant to the Minister of Pensions. At the time, over 250,000 applications by men seeking pensions exclusively attributable to shell shock had been rejected (United Kingdom, 1923b: cc2573–7). Statistics are unavailable for men who paid for private health care or who received inadequate or no health care because adverse pension determinations prevented their accessing public health care.
In post-war Britain the cost and quality of publicly funded medical care to men with shell shock was a political issue (Aldcroft, 1973). The Minister of Pensions turned it into an administrative issue by stating that the administrative costs of British public health care were four pence per British pound spent on health care, and that these were lower than any other country. He also stated that Britain had been able to keep the cost of public health care for men with shell shock to an average of £20 per man because of the efficiency of the pension entitlement system. The Minister did not respond to Opposition questions about whether avoiding the payment of pensions to men with shell shock was a strategy to minimize health care spending (United Kingdom, 1940: cc317–424).
Although our research focuses on men with shell shock, British Parliamentary debates and Pension Tribunals Appeals show issues pertaining to pensions for other medical conditions, although they are much less frequent than issues pertaining to pensions for shell shock disablement. In the following section, our discussion of the implications for accounting of the disablement pension scheme focuses exclusively on the pension scheme as it applied to men with shell shock.
Discussion
In every War Pension history there comes a time within a few years of war when the new generation desires to get rid of its liabilities. (Parry and Codrington, 1918: 51)
In this section we discuss how accounting for illness for the purpose of determining disablement pensions allowed men with shell shock to be made scapegoats of British government cost-cutting measures. The rigid classification of illness allowed pension decision-makers to distance themselves from the moral consequences of pension determinations that financially disadvantaged men with shell shock. When the Minister of Pensions was criticized for targeting men with shell shock, he relied on other aspects of accounting connected with the pension system to avoid blame. The unfair treatment of men with shell shock was achieved because the classification of illness made shell shock invisible for the purposes of pension determination, indicating that what accounting fails to reveal can be as important as what it reveals. However, it can be far harder to see what is missing from an accounting system than what is visible (Choudhury, 1988), and therefore to rectify the deficit of a system.
Scapegoating
Pensions for men with shell shock were a target of Ministry of Pensions’ cost savings during and subsequent to the First World War. Revoked pensions provided additional savings; men became unable to access public hospital care, so were no longer a financial drain on the public health system, providing additional cost savings to the British government. In addition, during the war, men whose pensions were revoked were eligible for recall into the British Army, which helped maintain its fighting strength. Maintaining fighting capability was critical to the British Government, which accepted the British Army’s view that the military force with the most men standing after decisive battles would be the ultimate victor (Brown, 1998; van Bergen, 2009).
Pension determinations for shell shock were particularly problematic because shell shock symptoms seldom remained stable, and so medical assessments made at one point in time might not accord with those made at another time. If medical conditions changed, pension payments might be expected to change. This may explain why the pensions of men with shell shock were targeted for more frequent review than pensions for other medical conditions, but it fails to explain why so many pensions for men with shell shock were denied or awarded then reduced or revoked even though medical evidence showed no improvement in their condition. It does not explain why the Minister of Pensions refused to consider cases of injustice towards men with shell shock, why there were more appeals about pensions for shell shock than any other medical condition or why so many applications for pensions from men with shell shock were rejected (Ministry of Pensions, 1919; Parry and Codrington, 1918). It also fails to explain why the descriptors used to account for illness eligible for a disablement pension failed to include shell shock or the many euphemisms commonly used for the condition by the British Army. This is even though shell shock was determined by the Appeals Review Tribunal of the Ministry of Pensions to be the second most frequent cause of war service disablement (Parry and Codrington, 1918) and even though the pension descriptors were stated by the Ministry of Pensions to cover all reasons for medical discharge (Ministry of Pensions, 1919). There is only one way that the descriptors can be viewed as comprehensive and this is if the British Army view that shell shock did not exist was adopted. In its descriptive choices for medical conditions that would be compensated by a pension award, the Ministry of Pensions was doing what the Army had done: it was attempting to make shell shock invisible. The Army did this by banning use of the term “shell shock”. The Ministry of Pensions did it by excluding shell shock from its list of medical conditions so that in accounting for illness, it excluded shell shock from its definition of illness.
Men with pensions for shell shock conditions became scapegoats for the British Government. Physical conditions were clear-cut; the notion of men sustaining a physical injury in battle had long been understood so the issue for these men revolved around the appropriate pension amount. Shell shock raised other issues. It had not been diagnosed prior to the First World War so was not well understood as an illness; it could exist in men with no sign of physical injury, which challenged the concept of “wounded in battle”; its treatment involved psychiatrists at a time when the medical profession considered them charlatans (Freeman, 2010); it did not involve one clearly defined set of symptoms; and the British Army, which through its experience with battle might be expected to understand its results on the health of the fighting soldier, thought it was feigned to avoid fighting. As a poorly understood illness whose existence was the subject of dispute by the British medical profession and Army, it is unsurprising that shell shock did not feature in the Ministry of Pensions’ classification of medical conditions sustained in battle. Men with shell shock did not view their right to a disablement pension as less than that of men with physical wounds, but the uncertainty and debate surrounding so many aspects of this condition meant that men with shell shock came under more scrutiny than other men when pension entitlements were being assessed (Holden, 1998; United Kingdom, 1918). Whenever pensions became a target of government cost-cutting, the grey area of pensions for men with shell shock was reviewed because even though pension awards had been made on the basis of a physical condition such as blindness or deafness rather than for shell shock per se, the scepticism about shell shock as an illness threw doubt on the veracity of all men compensated for a physical symptom of shell shock. The classification of physical conditions for which a pension award would be made served to make shell shock invisible by excluding it. The reviews which led to the revocation of pensions awarded to men with shell shock served to make men with shell shock invisible by excluding them from public hospital treatment and removing them from public care in hospitals or through pension entitlement.
It may be coincidence that when the British medical profession doubted the legitimacy of shell shock, Pension Medical Boards were staffed by doctors. However when medical opinion started to shift so that doctors were beginning to recognize shell shock as a legitimate illness, the composition of Pension Medical Boards was changed by legislation so an officer of the British Army, which had a standing policy of not recognizing shell shock as a legitimate medical condition, chaired each board and had a casting vote on all pension determinations. It may also be coincidence that at this time, the British Government was concerned about increasing Army recruitment levels to maintain its fighting strength (Brown, 1998). There is no direct evidence to indicate that this was planned to ensure men with shell shock continued to be disadvantaged by the pension system. It may have been the result of unfortunate coincidence, but this seems unlikely since members of the Pension Appeals Tribunal identified the increased number of appeals from men with shell shock whose pensions were revoked or whose applications were rejected after the Army gained control of all pension boards (Parry and Codrington, 1918).
There are always scapegoats in society and they are treated with violence. Violence does not need to be physical; it can take many forms, including discriminatory treatment if those scapegoated are viewed as accessing resources that others want or need to access (Fleming, 2004; Girard, 1986). Girard observed that in punishing the scapegoats in society, others avoid punishment. In the context of disablement pensions, targeting men with shell shock for pension reduction more than any other groups of pensioners is consistent with the definition of scapegoating posited by Girard (1986).
Girard (1987) examined religious and historical examples of scapegoating to conclude that scapegoats, regardless of their guilt or innocence, are treated with violence so that society as a whole may escape such treatment. During the British Government’s post-war fiscal tightening, reducing pensions for men with shell shock made the Ministry of Pensions a team player that was meeting government cost-cutting objectives. When the Treasury, Auditor-General and Committee of Public Affairs revoked pensions for men with shell shock they acted outside their jurisdiction yet the decisions were not challenged, suggesting that greater cost-savings from revoked pensions for shell shock would save the British Government money and lessen the severity of other cost-saving measures imposed as the Government sought to lower debt. Savings achieved through cutting pensions awarded to men with shell shock were savings the British government did not need to find from stringency in areas of spending that might impact on the general population. Pension revocations that forced men with shell shock back into the British Army contributed to saving the British public from the fate of losing the First World War, giving a different meaning to the age-old rhetoric of battle as the sacrifice of a few for the many.
Despite legislative control by the Minister of Pensions over the classification of medical conditions, there is no evidence of debate to consider a less ambiguous inclusion of shell shock so that men with shell shock would have a clear entitlement to a disablement pension. The ongoing exclusion of shell shock from the Ministry of Pensions’ accounting classifications kept shell shock invisible; in doing so it made men with shell shock scapegoats of a pension system that espoused a rhetoric of compensating those who had been disabled in the service of their country, but maintained inbuilt discrimination through a selective definition of disablement.
Distancing
Accounting classifications that distance government decision-makers from making moral judgments and turn their decisions into administrative efficiencies can lessen the visibility of inequities that might be apparent if the moral consequences of decision-making were visible. In extant literature on scapegoating, processes or rules that governments use to distance their decisions or actions from moral consequences have been described as a type of violence perpetrated against those whom a civilizing society is supposed to protect (Giroux, 2010; Sumner, 1996). Men suffering from shell shock deserved the protection of a society they had fought to protect, yet this society accepted discriminatory pension disablement descriptors that made one group of its protectors, men with shell shock, financially vulnerable.
The violence perpetrated against men with shell shock by the Ministry of Pensions was moral rather than physical, but moral violence is harder to fight because the process of instigating rules and processes to support government decision-making can create an illusion of equity and fairness in that the same rules and processes appear to be applied to all decisions in the same way. The use of rules, processes and tools of accounting classification to enable decisions that distance decision-makers from the moral consequences of their decisions has been termed “adiaphorization” (Bauman, 1988). Bauman (1996) adopts the term adiaphorization to describe distancing mechanisms that lead to actions or objects being treated as morally neutral so they can be carried out or perceived without moral evaluation. The term “adiaphorism” is taken from Judeo-Christian religion, where it refers to things that are neither forbidden nor mandated by religious scriptures and are therefore of indifference to the institution of the church. Bauman (1988) uses the Nazi construction of the Holocaust as an administrative efficiency as an example of adiaphorization that allowed Nazi decision-makers to distance themselves from the morality of decisions and eradicate populations. The Holocaust example shows that even the most extreme actions are rendered neither morally good nor bad by rules or processes that distance decision-makers from the moral consequences of their decisions. In separating decision-makers from the moral consequences of their decisions, it is easier for a government to control outcomes in society by implementation of unfavourable or unpopular decisions (Bauman, 1988).
Bauman (1988) describes moral judgements as disruptions that interfere with the smooth running of government. Hence, government wants processes and rules that separate decisions from their moral consequences so that it runs smoothly (Poder and Jacobsen, 2012). Since society want a smooth-running government, adiaphorizing processes are unlikely to be challenged. This does not negate the possibility of dissent within society. Rather, it refers to the widespread disagreement of society.
Bauman recognizes three aspects to distancing. First, there must be a system that stretches the relationship between an action and its consequences. The Ministry of Pensions stretched the relationship between action and consequences by requiring Medical Pension Boards to make pension determinations without examining or interviewing the men whose cases they were considering and by limiting pension determinations to a closed set of results so that decisions were constrained by accounting classifications of medical conditions. Pension Medical Boards decided which evidence they would consider in making their determinations, and since the reasons for their decisions were not disclosed, appeals decisions were rare (Parry and Codrington, 1918). Second, the system must be applied to some people, but not others, in a way that avoids moral impulse. Men with amputations and wounds were easy to classify under the pension entitlement system. The location of the primary wound or level of amputation determined the pension entitlement. For instance, men with the loss of two limbs received different accounting classifications depending on whether their amputations included an arm amputated below the elbow, an arm amputated above the elbow with a stump of more than six inches or an arm amputated within six inches of the shoulder. Men whose shell shock made symptom identification problematic and who had a number of symptoms, which is the norm with shell shock (Babington, 1997), were at the mercy of those applying the rigid classification system that, at best, would lead to a pension award based on the most debilitating symptom covered by the accounting classifications (van Bergen, 2009). Third, the system must identify specific traits that are used for classification and are separate from moral judgement (Bauman and Donskis, 2013). Since men with shell shock were awarded pensions based on a Pension Medical Board assessment of their most debilitating symptom within the pension accounting classification, decision-makers were selecting one symptom based on an incomplete list of shell shock symptoms and using that symptom to determine a pension entitlement. Ministry of Pension decisions were defensible by reference to the accounting classifications but not if pension determinations are considered a moral judgement. The Minister of Pensions defended even the most blatantly unfair pension decisions by stating they were in accordance with the accounting classifications; at no time did he recognize that the classifications might need to be expanded, which would have involved moral choices about the validity of shell shock as a medical condition.
Accounting classification provided the tool of adiaphorization that allowed pension decision-makers to remove moral judgement from pension determination. By rigid application of the accounting classifications, pension decisions appeared morally neutral despite their bias against men with shell shock. This made it easier for pension decision-makers to reduce pensions, even though it would cause financial hardship, or revoke pensions despite the financial hardship, loss of access to public health care and the likelihood that a man would be returned to Army service and the conditions that had caused the shell shock. Since accounting classification had turned pension determinations into morally neutral decisions, adiaphorization of pension processes meant there was no outcry when the Treasurer and Auditor-General reduced and revoked pensions to lower government spending, even though both acted ultra vires (Parry and Codrington, 1918).
When disablement pensions were introduced, they were compensation to men disabled in the service of their country and a system predicated on ensuring men who left civilian employment were afforded compensation equivalent to compensation available for similar disablement in that employment. In practice, accounting classification made pension determinations an administratively efficient way of managing the ongoing cost to the British government of men’s wartime disablement. Thus, when the Minister of Pensions announced in Parliament that the British government’s pension administrative costs were lower than those of other countries, this was accepted as signalling the Ministry of Pensions was financially efficient and effective. The Minister also claimed administrative costs were lower than those of private charitable institutions, even though those institutions were established to provide medical care to men with shell shock who were refused pensions by the British government and hence were unable to receive public medical care.
Accounting classification enabled decision-makers to distance themselves from the moral consequences of adverse decisions concerning pensions for men with shell shock. The Ministry of Pensions needed to use a distancing mechanism such as accounting because it provided a method of blame avoidance for its decisions, particularly the many decisions that were financially deleterious to men with shell shock.
Blaming
Hood (2002) has identified that public office-holders seek to deflect or reduce blame resulting from unpopular or adverse decisions. Extant literature recognizes the need for blame avoidance by government to avoid financial risks (Black, 2006). In the regulation of health, blame avoidance has been linked to preservation of the careers of politicians and public servants (Hood et al., 2001). The success of campaigns to raise private donations and the opening of private medical facilitates for men with shell shock who had been refused pensions or whose pensions had been revoked indicates that there was a substantial level of public sympathy for these men and the likelihood of public resentment towards the British government for the financial treatment of men with shell shock (Babington, 1997).
Three main strategies have been identified for deflecting or avoiding blame. First, presentational strategies involve argument, spin or stage management and other techniques to shape public impressions (Hood, 2007). The Minister of Pensions appeared to be careful in his responses to Parliamentary questions, referring always to Pension Medical Board responsibility rather than the Ministry of Pensions in issues concerning pension determinations. Thus, he is seen to be supporting the opinions of medical experts. Second, agency strategies use the complexity of government agency relationships and agency structures to draw complex lines of responsibility so that it is unclear where a decision was made, and rotate staff who may be blamed for a decision to obscure the identity of the decision-maker (Hood et al., 2009). Although from a legislative perspective, the Minister of Pensions was responsible for pension determination, he saw the decision of Pension Medical Boards as final (Minister of Pensions, 1917; Ministry of Pensions, 1919). However, Board members came from the medical profession so their adverse pension determinations could be constructed as emanating from the medical profession rather than the Ministry of Pensions (Holden, 1998). Third, policy strategies involve implementing routines and processes that minimize individual or institutional liability or blame (Weaver, 1986). The stringent accounting classification of medical conditions used by the Ministry of Pensions provided a Nuremberg defence; when pension decisions were challenged in Parliament, the Minister of Pension’s invariable response was that pension decision-makers were merely following the rules. Following the accounting classifications was so strongly enculturated that when the records of the Ministry of Pension were shown to be incorrect in the case of Lieutenant Verity, they were not corrected. Instead the Minister of Pensions deflected criticism by asserting that the records had been accurately used to make a pension determination consistent with accounting classifications. The strategies for blame avoidance are not necessarily discrete. Hood (2002) would categorize the type of policy automaticity enabled by the accounting classifications as a hybrid between agency and policy strategies, and maintaining accounting classifications that facilitated discriminatory scapegoating of men with shell shock as a hybrid of presentational and policy strategies.
Blame avoidance is also avoidance of responsibility (Hood, 2002). Once decision-makers can avoid responsibility for their decisions, distancing mechanisms are more likely to succeed (Folger and Skarlicki, 1998) and so is scapegoating (Douglas, 1995). In the case of pensions for men with shell shock, accounting classification that kept shell shock invisible as a medical condition facilitated the distancing of pension decision-makers from the morality of making men with shell shock scapegoats of government cost-cutting and provided a tool that supported blame avoidance by the Minister of Pensions for pension determinations made by the Ministry of Pensions.
Conclusion
During and subsequent to the First World War entitlement to a disability pension for military service in the British Army was based primarily on medical records compiled by the British Army on discharge of a soldier as being medically unfit for service, using a system developed by the Ministry of Pensions to classify medical conditions that would receive a pension entitlement. The system used by the Ministry of Pensions classified medical conditions by their type and severity. We describe this classification schema as an accounting for illness.
The schema purported to classify all disabling medical conditions sustained during war service, but its focus was on physical wounds, meaning that the Ministry failed in its classification scheme to account appropriately for shell shock. Battle trauma was not well understood at the time. As the number of men suffering this trauma increased, the British medical profession started to recognize shell shock as a legitimate medical condition occasioned by war service. However, neither the British Army nor the Ministry of Pensions accepted this changed view towards shell shock.
Our research has focused on the ramifications of the Ministry of Pensions’ failure to account for shell shock in the same clearly definable way that it accounted for physical wounds leading to disablement. It describes the financial disadvantage sustained by men with shell shock compared to men with physical wounds and the ongoing scrutiny to which men with shell shock were subjected, even when they had physical symptoms that brought them within the descriptors listed in the Ministry of Pensions’ classification schema. From an accounting perspective, an approach to accounting for illness that focused on physical conditions and excluded mental trauma unless accompanied by a physical condition, was an incomplete system and therefore a failure if a holistic coverage of medical conditions occasioning disablement was its intended aim.
There are indicators that it served the British government to leave shell shock as a grey area not adequately covered by the Ministry of Pensions’ schema. For instance, it allowed the Ministry to target this group when seeking cost savings through pension reduction, and men with shell shock who were not awarded a pension or whose pension was revoked during a pension review by the Ministry of Pensions became eligible for Army re-enlistment, boosting Britain’s fighting capability. Thus, men with shell shock became scapegoats of a government seeking to make cost savings and ensure its supply of soldiers to fight for their country on the battlefields of the First World War.
By excluding shell shock in a clearly definable way from its schema to account for disabling medical conditions leading to a pension entitlement, the Ministry of Pensions made shell shock an invisible illness for pension purposes. The classification schema was viewed by the British government as an equitable approach to disablement pension determinations because the inequity concerning men with shell shock was hidden.
Determining the level of pension men deserve for disablement sustained in service of their country is always a moral decision by government. It was also a moral decision to maintain a pension classification schema that excluded shell shock even after the British medical profession started acknowledging shell shock as a legitimate medical condition. By turning pension determinations into a matching of what was stated in Army discharge records with the Ministry of Pensions’ classification schema, the Ministry of Pensions distanced pension decision-makers from the morality of their decision, though this did not alter the underlying morality of the choices being made. Once government decision-makers can make immoral decisions, governments must engage in blame avoidance to deflect censure from the consequences of their actions. Our research gives examples of the blame avoidance strategies used by the Ministry of Pensions.
Contemporary investigation of disablement pensions has been problematic. Records were either not kept or have been lost or subsequently destroyed, meaning that there are important gaps, including lack of knowledge about the number of men with shell shock who sought disability pensions, the outcome of each case and the amount of pensions awarded to men with shell shock who were able to demonstrate physical symptoms that fell within the classification schema. However, we would contend that exact numbers are unimportant. To disadvantage only one man disabled while serving his country would be an injustice; it is not necessary for the number to be significant for the injustice to exist. While contemporary pension management has not been a subject of extant research, research into medical and disability management indicates that the problem of classifying illnesses to make them invisible for the purposes of decision-making, funding or access to disability services continues to be problematic.
Our use of an historical example removes the politicization of contemporary debate on health care and disability but leaves untouched the accounting issue, which is that it is not only what is included that is important to accounting; what is left out of any classification for accounting purposes is equally important and it is by examining the negative space of what has been left out that injustices which might otherwise remain hidden and invisible are likely to be revealed so that corrective action can be taken. It is our view that there is considerable opportunity for accounting research to throw light onto the injustices hidden in the dark corners of incomplete, selective or exclusive classification schemes and that historical approaches to research can play an important role by removing the noise of political debate while preserving the issues that should be explored.
Footnotes
Acknowledgements
For John Owen Rees, invalided by his Army service in the First World War and then disadvantaged by a disablement pension scheme that sought to make his illness invisible. We wish to thank our anonymous referees for their helpful comments on this submission and an earlier draft submitted to the eighth Accounting History International Conference held in Ballarat. We would also like to thank participants at the eighth Accounting History International Conference for their comments on an earlier draft.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.