
Abstract
Introduction
This paper describes the development, implementation, and preliminary findings of the Ironbark Program, a group-based intervention delivered in a residential psychiatry facility. The Ironbark Program uses a common treatment factor approach to support people with a range of mental health challenges, including borderline personality disorder (BPD), BPD traits, or emotion dysregulation.
Method
The rationale, development, goals, and session outline of the Ironbark Program are described. The preliminary evaluation of the program examined feasibility and acceptability from a staff perspective using pre- and post-training implementation surveys, and from a consumer perspective, using session ratings collected after each Ironbark module.
Results
The Ironbark Program has been an effective way to utilise existing resources despite initial implementation challenges. The Ironbark Program has resulted in greater cohesiveness, confidence, and a broad improvement in staff attitudes regarding consumers diagnosed with BPD. Consumers consistently rated Ironbark modules as ‘very good’ and ‘excellent’.
Conclusions
Preliminary findings suggest Ironbark represents an effective collaboration between a non-government organisation and mainstream public psychiatry. The program can be delivered cost-effectively by non-clinical and support staff. Ironbark was designed to be specific enough to be effective for consumers with BPD or BPD traits, while being sufficiently generic to benefit all PARC consumers.
Keywords
Background
Borderline personality disorder (BPD) is characterised by persistent identity disturbance, challenges with interpersonal functioning, impulsivity, and emotional instability. 1 Although evidence-based psychotherapies have been developed for BPD, they are not readily accessible for people seeking treatment. 2 The development of a modular, group-based psychotherapy program based on a ‘common treatment factors’ approach provides an opportunity for effective treatment delivery within residential community mental health services.
The Austin Prevention and Recovery Care service
The Austin Prevention and Recovery Care (Austin PARC) service is a publicly funded mental health facility operating under a step-up/step-down model. It offers consumers short-term residential care for up to 28 days (average 17 days) as an alternative to an inpatient admission (step-up), as well as providing transitional support following discharge from acute inpatient care (step-down). Consumers with various diagnoses and mental health difficulties seek support from PARC, some of whom have BPD, BPD traits, or emotion dysregulation. The service is operated by Austin Health in partnership with a non-government organisation, Mind Australia Ltd, and is staffed by mental health practitioners and a lived experience peer worker on a 24-h basis. A senior clinician is available 7 days per week during business hours. A part-time consultant psychiatrist and part-time psychiatry registrar are available Monday to Friday during business hours; PARC staff may escalate clinical concerns to on-call medical staff outside of business hours. Consumers can participate in group and individual recovery-focused sessions throughout their admission.
Pre-Ironbark Program PARC group module topic options.
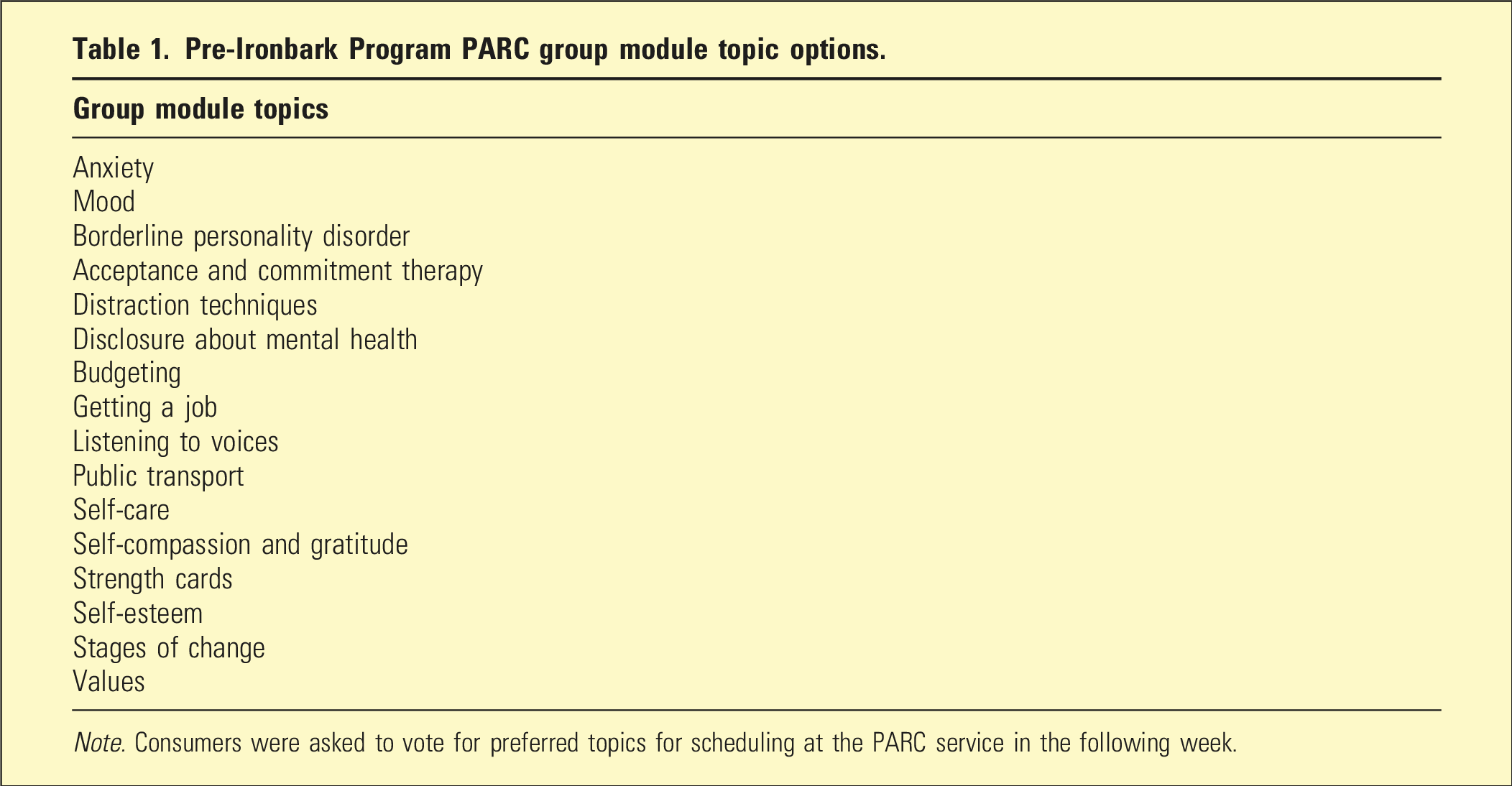
Note. Consumers were asked to vote for preferred topics for scheduling at the PARC service in the following week.
Rationale for collaboration with Spectrum Personality Disorder and Complex Trauma Service
In 2018, operational leaders from Mind and Austin PARC contacted Spectrum Personality Disorder and Complex Trauma Service (Spectrum) to request support for improving practice when working with consumers with BPD. Spectrum is a specialist mental health service funded by the state government, with a state-wide remit. The decision to approach Spectrum followed recognition among PARC staff that a primary diagnosis or traits of BPD impacted significantly on consumers’ ability to effectively engage with the existing PARC program. Furthermore, there were no evidence-based interventions for BPD suited to a short duration PARC (or equivalent community residential service) setting. A previous study found that significantly fewer consumers with BPD or BPD traits were admitted to inpatient units following their discharge from a Northwest PARC service, 3 suggesting long-term benefits of PARC services for people experiencing BPD-related challenges. However, this previous study did not describe the structure and content of the program nor the changes in BPD symptoms reported by their participants.
In the current PARC study setting, group and individual keywork sessions are facilitated by non-clinical staff. By contrast, research on brief interventions and stepped-care for BPD-related challenges tends to involve individual therapy facilitated by specialised therapists in combination with intensive group therapy programs.4,5 There is little research about brief interventions for BPD symptoms in community settings such as PARC services, which have limited access to regular supervision from psychologists and consultant psychiatrists compared to inpatient, outpatient, and public mental health services.
To better understand the scope of this problem, we informally tracked program engagement and outcomes for Austin PARC consumers with BPD and BPD traits over 4 months. Consumer engagement was indicated by attendance of consumers at group sessions, keywork sessions, community meetings, family and carer support intervention sessions, and participation in cooking and chores. The following themes were identified: • These consumers tended towards the lowest levels of engagement with PARC program activities. • Staff frequently disagreed about the most effective ways of engaging these consumers, with sometimes dramatic changes in approach between admissions. • It was unclear whether staff were using evidence-based approaches and resources during individual sessions with these consumers due to a lack of consistency and transparency. • Although these consumers frequently formulated their treatment goals around increasing distress tolerance and regulating emotions, they were often unable to make progress towards these goals. • When offered shorter stay durations (less than the maximum 28 days), consumers with BPD often became focused on advocating for an extension of their stay rather than engaging and focussing on their goals. • Positive outcomes for these consumers were often limited to simple tasks, such as building a routine around sleep, daily activities, and meditation.
To address these challenges, Mind, Austin PARC, and Spectrum partnered to create the Ironbark Program.
Method
This section describes the development and implementation of the Ironbark Program, in addition to the processes for evaluating the program from staff and consumer perspectives.
The Ironbark Program
A brief group-based intervention was designed with content specific to consumers experiencing BPD-related difficulties including emotion dysregulation and interpersonal challenges, but sufficiently generic to meet the needs of all PARC consumers. The program is named after a native tree species called ‘Ironbark’ that features in Indigenous Australian culture. Its bark resembles iron and can protect the tree from the hottest fire. While the markings of the fire remain, the buds beneath, protected by the bark, can regrow. This image of resilience and recovery symbolises the aims of the Ironbark Program.
Key considerations in the design1 of the program included (i) making content relevant to all PARC consumers regardless of their diagnoses; (ii) group module duration up to 90 min; (iii) program duration consistent with PARC admission (up to 4 weeks); (iv) stand-alone modules to accommodate consumers being admitted and discharged at different times; (v) amenable to facilitation by non-clinical staff (with training and supervision provided by Spectrum); (vi) no requirement for additional resources, and (vii) creation of a Facilitator’s Manual to ensure consistency.
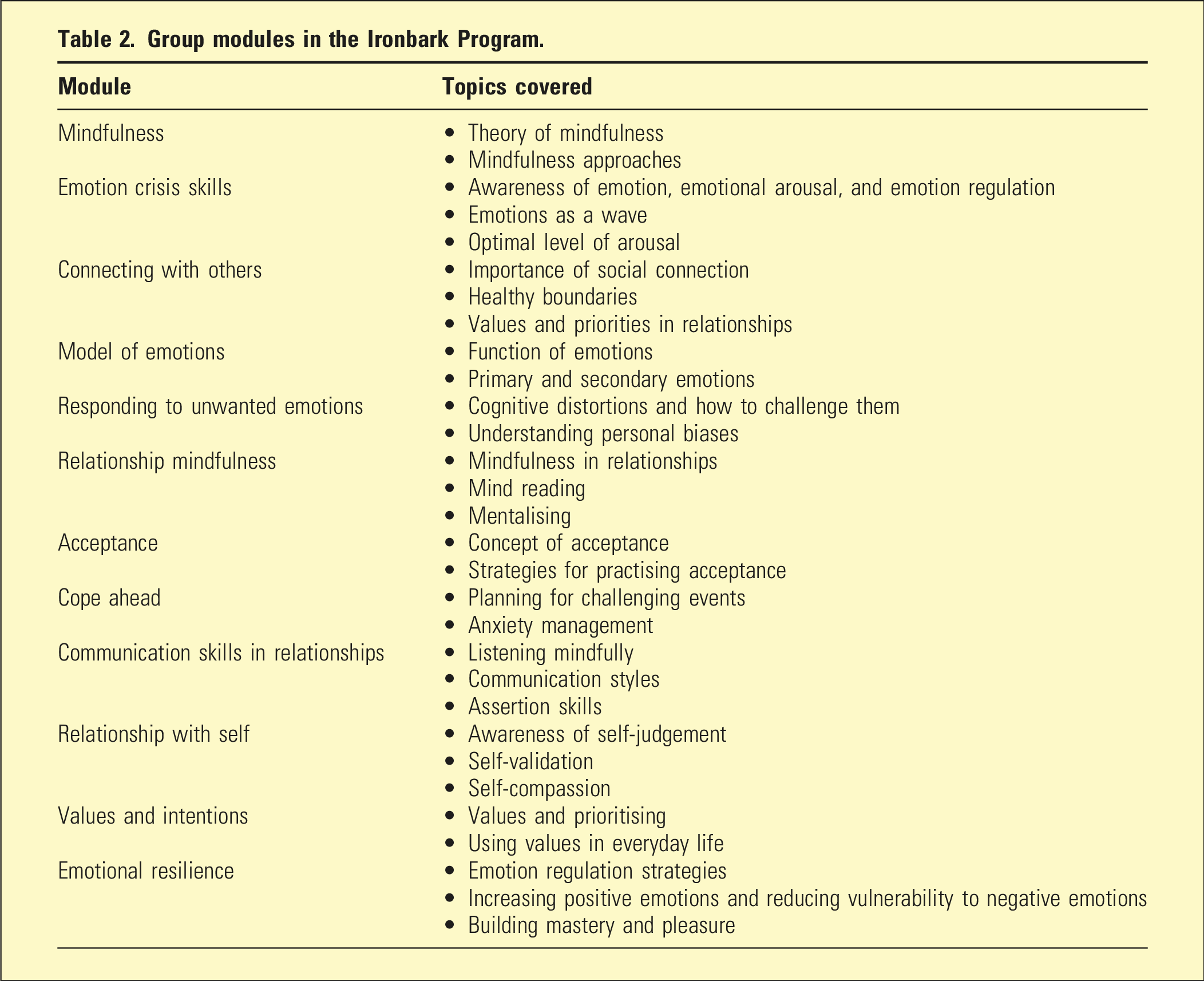
Group modules in the Ironbark Program.
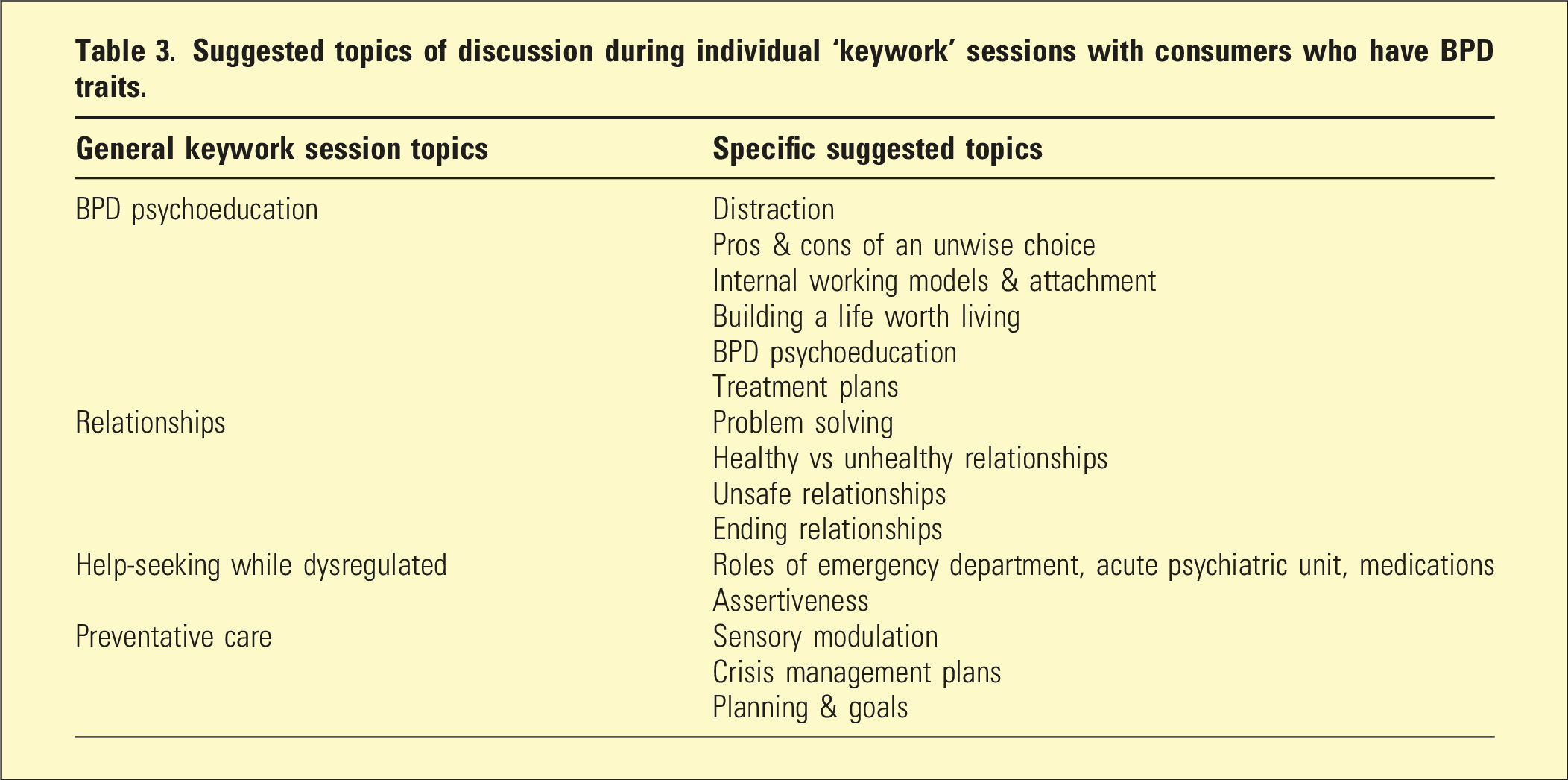
Suggested topics of discussion during individual ‘keywork’ sessions with consumers who have BPD traits.
The Ironbark modules cover broad themes relevant to most diagnoses, including how to recognise and respond to emotions, and build mindfulness and interpersonal skills, as informed by the clinician researchers’ experiences working with people with BPD (Table 2). The skills-based modules were agreed to be universally useful, especially for consumers struggling with low self-esteem, emotion regulation, relationship difficulties, and who had experienced early childhood adversities with associated attachment difficulties. The modules are scheduled three times per week. Consumers can commence the program with any module; consumers completing a 28-day admission can access all modules.
Each 90 min module is co-facilitated by two mental health support workers from Mind or Austin Health. These staff received training and supervision from Spectrum, attending two full-day workshops which covered general principles when working with consumers with BPD, including strategies for validating and navigating their distress. The training also reviewed the Facilitator’s Manual content to ensure consistency of the program’s delivery.
During the pilot study, PARC staff received supervision from Spectrum once every 2 months for 12 months, focussing on issues relevant to specific module content and adapting the content delivery to accommodate the diverse needs of consumers. Facilitators were taught how to respond to consumer distress and support consumers if they become activated by Ironbark content. Ironbark facilitators were also encouraged to be flexible, offering consumers the opportunity to unpack challenging aspects of a previous module before returning to the standard program. This was intended to enhance consumer agency in how they engage with the content and work through distress. Facilitators were advised to flag potentially activating content at the beginning of group modules and explain benefits of participation despite its challenges.
Consumers receive an Ironbark workbook containing resources and activity sheets that support learning and sharing. Consumers with a diagnosis or traits of BPD are provided with additional tailored resources that complement the material covered in the group-based modules. These focus on BPD-related challenges and topics that consumers may want to cover (e.g. Unsafe Relationships) and can be utilised during bi-weekly individual ‘keywork’ sessions (see suggested keywork topics in Table 3) with a Mind support worker.
Evaluation of the Ironbark Program received institutional ethics approval (HREC/52977/Austin-2019). Consumers and staff who contributed to the evaluation provided written informed consent.
Consumer feedback post-session
Session ratings were routinely and anonymously collected from all consumers to obtain a preliminary sense of their perceptions of the Ironbark Program. The survey asked a single question ‘How would you score this group out of 5?’ using a five-point Likert scale, with 1 = Poor and 5 = Excellent.
Staff and consumer evaluation, pre- and post-program implementation
Staff participants completed 10 min online surveys prior to training and 6 months after program implementation, responding to questions concerning their perceptions of the PARC organisation, team cohesion, and the impact of the program on consumer participation. The survey included a modified version of the personality disorder attitude and knowledge survey, otherwise known as ‘eKALM’, 7 which assesses empathy, attitudes, knowledge, and management. 4 Staff also rated how successful their clients were in learning and implementing new skills presented in Ironbark Program modules. For staff joining PARC following the program’s implementation, the pre-training survey was administered upon commencement and the post-implementation survey once they had facilitated the program for 6 months.
The program evaluation is ongoing, with comprehensive data collected from consumer participants with a diagnosis of BPD, BPD traits, or emotion dysregulation and a PARC admission of at least 2 weeks. Measures are completed at admission, discharge, and 3- and 6-months’ post-discharge, assessing borderline symptom severity, emotion dysregulation, depressive symptoms, daily functioning, and quality of life. The effectiveness of the Ironbark Program for improving staff confidence and attitudes, as well as outcomes for adult consumers with BPD, BPD traits, or emotion dysregulation, will be reported in future publications.
Preliminary results
Preliminary staff and consumer outcomes are briefly described here.
Primary mental health diagnoses of Austin PARC consumers between March 2021 and April 2022.
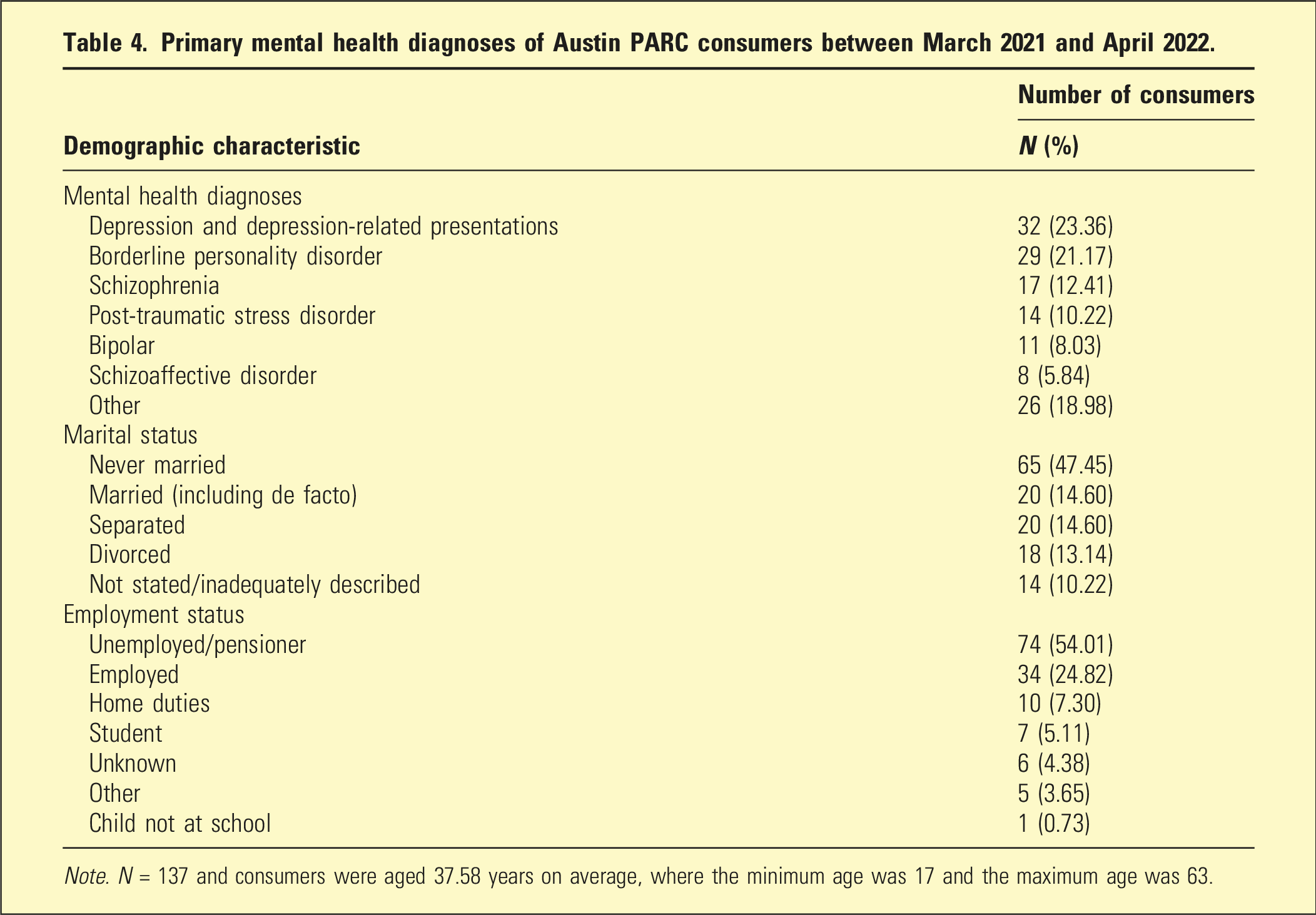
Note. N = 137 and consumers were aged 37.58 years on average, where the minimum age was 17 and the maximum age was 63.
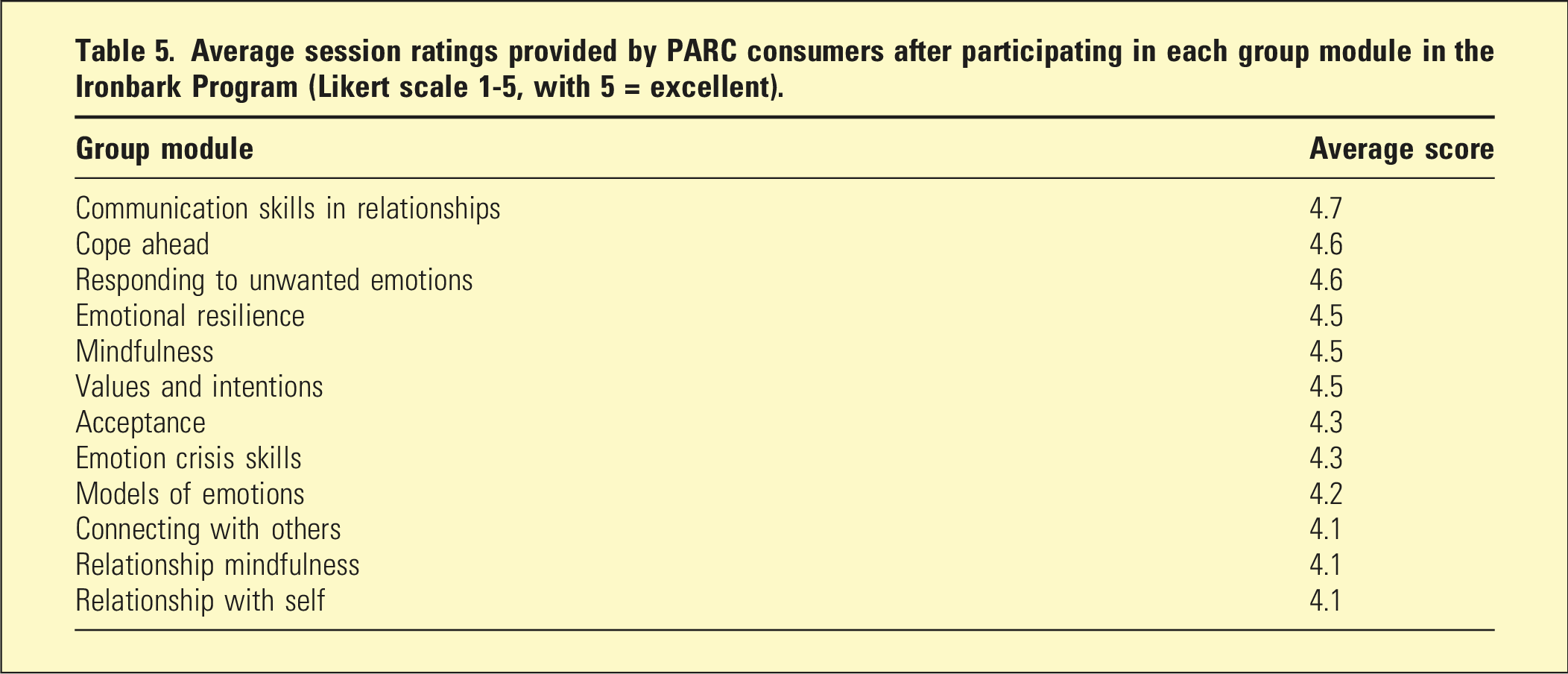
Average session ratings provided by PARC consumers after participating in each group module in the Ironbark Program (Likert scale 1-5, with 5 = excellent).
Twenty-two staff contributed data to the pre-training survey, and thirteen staff to the post-implementation survey. The data reported here reflect eKALM outcomes. When asked whether the service is meeting the needs of consumers with BPD, staff ratings of ‘good’ or ‘very good’ increased from 45% pre- to 85% post-Ironbark. eKALM scores showed increased positive and reduced negative attitudes experienced by staff towards consumers. Due to the small sample sizes, there was insufficient statistical power to conduct significance testing. Forthcoming papers regarding staff and consumer outcomes will report on a larger sample to facilitate these analyses.
The staff surveys asked staff about team cohesion and consumer skill acquisition. For the former, ratings of ‘very cohesive’ increased from 23% to 61% post-Ironbark. Similarly, improvements in consumers’ ability to implement new skills averaged 2.6 pre-implementation and 3.5 post-implementation (where 1 = unable and 5 = very successful). The program is encouraging collaboration among the service’s Mind practitioners, who are collating and sharing additional resources consistent with the Ironbark framework to promote consistent, effective care.
Ironbark facilitators and lived experience staff noted anecdotally that some Ironbark content can be activating for some consumers. For example, the Acceptance module includes mindfulness exercises and discusses alleviating suffering via acceptance. This module asks consumers to sit with and work towards accepting distressing thoughts and memories, which facilitators reflected may heighten emotional distress in consumers who have trauma backgrounds. This is a challenging task for most people; hence elevated distress is understandable. Notably, feedback from consumers who engaged in the process of challenging long-standing patterns of thoughts and behaviours, identified the Acceptance module content as the most empowering of all the Ironbark modules.
Discussion
Preliminary evaluation of staff feedback pre- and post-implementation suggests that problems identified during the pre-Ironbark scoping exercise are being addressed through the Ironbark Program, although we await confirmation following completion of the staff and consumer outcome analysis. Word of the benefits of the program is spreading, with Austin PARC already receiving referrals from internal and external organisations seeking access to the Ironbark Program. While encouraging, this likely reflects the lack of brief, BPD-appropriate care options available in the broader public mental health sector.
Our preliminary results suggest a positive shift in staff attitudes towards consumers with BPD, improved staff cohesion and consistency, and favourable consumer feedback for the Ironbark modules. Previous research reported that staff attending a 2-day BPD-specific professional development workshop reported positive improvements in their attitudes towards working with clients with personality disorders, 8 with improvement sustained 3- and 6-months post-training. Kramer et al. 4 speculated that the concise, structured nature of brief intervention training provides clinicians with clear principles and guidance when working with people with BPD. In the present study, the reported improvement in staff cohesion and motivation to implement the Ironbark Program infers that its structure and content support non-clinical staff to work with consumers with BPD-traits and emotion-dysregulation. The Ironbark Program has fundamentally changed the framework and model of care in which the Austin PARC staff practise. Hence it is difficult to ascertain whether these positive changes are due to Spectrum’s training, the new model of care, the practical experiences gained while delivering the Ironbark Program, or a combination of these factors.
The Ironbark Program modules are delivered on a rolling basis; consumers admitted for a maximum of 28 days can access all 12 modules during their stay. The authors speculate that consumers feel ‘held’ and contained by the consistent structure offered by the Ironbark Program. Staff are better equipped and more confident when assisting consumers to identify their emotions and support them through distress associated with the discharge process, which is particularly advantageous for PARC consumers completing a shorter duration of stay. Favourable feedback regarding the Ironbark Program modules was provided by PARC consumers with and without BPD diagnoses or traits, suggesting most consumers perceived benefit and relevance of the content regardless of their diagnosis.
Encouragingly, 99% of consumers reported they would recommend the Ironbark modules to others, with average session ratings between 4 and 5 (where a score of 5 indicates ‘excellent’).
A potential contributing factor to the program’s success and consumers’ satisfaction is that Austin PARC is based in the community and during their stay, consumers are encouraged to take leave and spend time in their usual community settings (e.g. home with family, workplace, and university). This structure provides a unique opportunity for consumers to participate in a relatively intensive group program and then feel empowered to practice their skills in the context of their regular lives. This structure promotes consumer agency during the treatment process, which is widely recognised as an important feature in the recovery process.9,10
Challenges and limitations
Despite the broad success of the Ironbark Program, there were some challenges during implementation, particularly regarding the reorganisation of staff responsibilities and responding to consumer distress. At 90 min, Ironbark group modules are up to 30 min longer than the previous PARC program, requiring two facilitators rather than just one. However, the additional group session time meant that Mind support workers, who would usually be providing one on one keywork support during this time, were available to facilitate the Ironbark group sessions instead. Tasks previously allocated for day-shift staff (e.g. preparing dinner) were re-allocated to evening staff so that day-staff could facilitate group sessions. Furthermore, prior to the Ironbark Program, a second staff member - if available - would often co-facilitate group sessions. Hence, there was no requirement to increase the number of staff at PARC to support the Ironbark Program.
Understandably, the first time Ironbark was offered, staff required additional time to familiarise themselves with the program content to deliver the modules effectively. While acknowledging these challenges, staff overwhelmingly endorsed the Ironbark Program as it enhanced their ability to provide consistent care to consumers with BPD traits. Staff support for the Ironbark Program is clearly indicated by their willingness to continue delivering the program, despite activity scheduling alterations. Ironbark facilitators and lived-experience workers anecdotally reported some consumer distress, primarily with the Acceptance module, although this module is not consistently activating. Learning to accept challenging emotions and experiences in a supportive context is helpful for improving distress tolerance and emotion regulation 11 and is an important aspect of recovery. Hence, Spectrum advised Austin PARC staff to continue delivering this module and manage any changes in risk as appropriate. In the event of distress, consumers are supported by one of the module facilitators and later, by their Mind support worker during individual sessions.
The Ironbark Program was developed to specifically address challenges experienced by people with BPD, while remaining relevant and beneficial for all PARC consumers regardless of diagnosis. Consistently positive consumer feedback regarding group module content supports this, although as post-session feedback was requested by the group facilitators after the group session rather than by a third party, it is possible this may have influenced participants’ anonymous feedback. Forthcoming research will describe the effectiveness of the Ironbark Program for improving symptoms of BPD, depressive symptoms, general wellbeing, functioning, and quality of life in addition to changes in service usage. It will also describe the acceptability and feasibility of the Ironbark Program in greater detail from the perspective of the staff delivering the service.
Conclusions
Since its implementation at Austin PARC, the Ironbark Program has generated considerable interest among other PARC and similar services across Australia. The advantages of the Ironbark Program include its relevance to all PARC consumers regardless of their diagnoses, while also targeting specific traits of BPD. The program can be facilitated by staff who are not clinically trained (e.g. support workers) and delivered using available resources. The preliminary results of this pilot study are encouraging, and we await the final client outcome and staff survey data to understand more about the efficacy of the Ironbark Program. In the longer term, we anticipate that Ironbark will be rolled out more broadly to provide relevant, accessible, and cost-effective support as part of a stepped care approach for people with BPD-related difficulties who access public mental health services. This will help fulfil the wider goal of offering effective, accessible, short-term support to people with BPD traits and reducing demand for crisis interventions.
Footnotes
Acknowledgements
The authors gratefully acknowledge the expertise and contributions of Dr Laura Hayes, Dr Zoe Gibbs, Corrine Murphy, Prof. Richard Kanaan, and Sam Crowley.
Ethical considerations
The reported data were collected with institutional ethics approval (HREC/52977/Austin-2019).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.