
Abstract
Objectives
This study aimed to analyse trends in youth mental health service utilisation across hospital and community settings by integrating incidence, prevalence, and DALY estimates from the Global Burden of Disease (GBD-2023) to account for changes in underlying population burden.
Methods
We used a triangulation approach, comparing trends in hospital separations and community contacts with independent indicators of underlying occurrence and burden from GBD-2023 to contextualise changes over time. A retrospective analysis of national data for individuals aged 0–25 years (2013–14 to 2023–24) examined hospital separations and community contacts for substance-use, mood, neurotic/stress-related, and behavioural/emotional disorders. Diagnoses were mapped to GBD categories. Age-standardised and age-specific rates were calculated, and temporal trends were assessed using Joinpoint regression.
Results
Hospitalisation rates for depressive, anxiety, bipolar, and substance-use disorders rose until 2021 and then declined. Community service use strongly correlated with hospital trends, particularly for mood and anxiety disorders. GBD data showed sustained increases in anxiety (6.5%), modest growth in depression (1.7%), and slight decline in substance-use disorders (−0.5%).
Conclusion
Youth mental health care in Australia is shifting toward community-based services, with reduced hospital reliance. Rising internalising disorders, especially anxiety, reflect the need for sustained, system-wide strategies that address clinical care and underlying determinants.
Mental health (MH) challenges among children and young people represent a significant public health concern in Australia, 1 as early MH difficulties can have long-term impacts on overall wellbeing. 2 National data (2013–14) indicate that approximately 14% of children aged 4–17 years experience a mental disorder in any given year. 3 The Australian Bureau of Statistics’ National Study of MH and Wellbeing (2020–22) reports that nearly 39% of young people aged 16–24 years experience a mental disorder annually. 4 Globally, research shows that around three-quarters of all mental illnesses emerge before the age of 25, highlighting the critical importance of early detection and intervention. 5
Despite the expansion of MH services specifically for young individuals in Australia – including Primary Health network, commissioned youth services, headspace centres, and state/territory programs 6 – and substantial increases in expenditure, 7 hospitalisations for MH conditions among people under 25 remain significant. 8 Such admissions often indicate severe or complex presentations, inadequate response to community-based care, or delays in accessing early intervention. 9 While national reports provide descriptive statistics on hospital activity, 1 they lack integrated analyses combining hospital trends, community use, and population-level indicators of disorder occurrence and burden, limiting the ability to assess whether current service configurations meet youth MH needs. To provide a more comprehensive understanding of youth MH care, the present study adopts a triangulated approach by integrating hospitalisation data, community contacts, and recently released population-level Global Burden of Diseases (GBD) estimates 10 of incidence, prevalence, and disability-adjusted life years (DALYs). In this study, ‘triangulation’ refers to the comparison of trends in hospitalisations and community contacts with independent estimates from the GBD indicators to help distinguish changes in service utilisation from changes in underlying disorder occurrence, rather than relying on a single data source.
Service demand is closely linked to the diagnostic profile of young people accessing care. Meta-analyses indicate high comorbidity among key MH conditions, particularly mood, anxiety, and substance-use disorders.11,12 Studies of young people with substance-use disorders report comorbidity rates as high as 50–90% with other psychiatric conditions.13,14 Evidence also indicated childhood-onset disorders such as conduct-disorder substantially elevate the risk of later substance-use and mood disorders.15,16 These overlapping trajectories contribute to functional impairment, complex care needs, and long-term illness burden. Therefore, this study focuses on diagnostic groups that are both prevalent and highly burdensome in youth–substance-use, mood, anxiety, and childhood-onset behavioural disorders – reflecting their major contribution to service demand and population health burden. Accordingly, this study aims to (i) analyse trends in hospitalisations among young people (under 25 years) from 2013–14 to 2023–24; (ii) compare these trends with population-level GBD incidence, prevalence, and DALY estimates for key youth diagnostic groups; and (iii) explore the relationship between hospital and community service utilisation; to identify patterns that can inform evidence-based policy, resource allocation, and the design of youth-focused MH services.
Methods
Study design and data sources
We conducted a retrospective, population-based study using administratively collected hospital separations (HS) and community-MH service (CMH) data among young people in Australia from 2013–2014 to 2023–2024 financial years. To contextualise service utilisation within the broader epidemiological burden, we also incorporated estimates from the GBD-2023 study. 10
Admitted patient mental health-related care
Hospital data were sourced from the Australian Institute of Health and Welfare (AIHW) National Hospital Morbidity Database, 1 which compiles episode-level records of admitted patient care from all public and private hospitals in Australia. MH-related HS were identified when the care type was recorded as MH, the principal diagnosis was a mental or behavioural disorder, or a relevant MH-related procedure was recorded. Activity was reported as separations (completed episodes of care), including both overnight and same-day admissions.
Community MH care
CMH data were obtained from the AIHW National CMH-Care Database, derived from the CMH Care National Minimum Data Set. 1 This dataset includes service contacts from state and territory specialised public ambulatory MH services. A service contact is any recorded interaction between a specialised MH service provider and a consumer, individually or in a group, via face-to-face, telephone, or telehealth. CMH contact rates reflect recorded contacts within the included CMH and care delivered in other settings like services from private psychiatrists, GPs, and NGOs are excluded.
Global burden of disease data
Estimates of incidence, prevalence, and DALYs for Australia were obtained from the GBD-2023, coordinated by the Institute for Health Metrics and Evaluation (IHME). The GBD provides harmonised estimates across locations and years, reporting both crude and age-standardised rates per 100,000 population, stratified by age, sex, and calendar year. 10 The related Australian data has been extracted from IHME visual hub (https://vizhub.healthdata.org/gbd-results/).
Study population
The study population comprised individuals aged 0–25 years, consistent with Australian definitions of child and youth MH services. For hospital data, we extracted records with a principal diagnosis within selected ICD-10-AM categories (F10-F19, F30-F39, F40-F48, F90-F98), which represent the most common and clinically significant mental and behavioural disorders in young people. These groups were chosen based on their high rates of HS in our data exploration across all MH disorders (F00-F99) (Table-S-1), and strong evidence from studies emphasising their prevalence, frequent comorbidity, and links during childhood and adolescence.11,12,17–19
To enable meaningful comparison with the GBD-estimates, hospital diagnoses were further grouped to match GBD mental and substance-use categories. Specifically, depressive-disorders included F32-F33.9 and F34.1; bipolar-disorder included F30-F31.9 and F34.0; anxiety-disorders included F40-F44.9 and F93-F93.2; conduct-disorder included F91-F92.9; and alcohol/drug-use disorders included F10-F19.99. Records with non-MH codes or external cause codes (e.g. E24.4, G31.2, G62.1, R78.0, X65-X65.9, Y15-Y15.9, P96.1, and R78.1-R78.9) were excluded. 20 ADHD (F90) was not included due to its classification as a neurodevelopmental disorder and its limited representation in hospital admission data.
CMH data were analysed using the original ICD-10-AM F00-F99 framework, as reported in the national dataset, because these records are coded at the broader chapter level and cannot be reliably disaggregated into GBD categories. Consequently, while CMH data provide important context on service utilisation, the primary comparative analyses focus on HS and GBD-estimates, which share a harmonised classification structure.
Measures
• Principal diagnosis: The condition primarily responsible for the contact or admission episode. • Service utilisation: Number of recorded contacts (community-based) or separations (hospital-based). • Population rates: Age-standardised rates/100,000 population, using the 2001 Australian standard population as the reference (current recommended Australian standard population); and age-specific rate/100,000 population. • GBD metrics: ○ Incidence: New cases emerging annually. ○ Prevalence: Total number of people living with the condition. ○ DALYs: Combined measure of years of life lost and years lived with disability.
Statistical analysis
We calculated age-standardised and age-specific rates of HS and CMH utilisation by diagnostic group, sex, and year. Temporal trends were assessed using Joinpoint regression analysis (Joinpoint Trend Analysis Software, NCI), which fits segmented log-linear models to identify statistically significant changes in trend. Model specifications followed the Joinpoint analysis guidelines. We allowed a maximum of one joinpoint to detect a single significant change in trend. Model selection was based on the Weighted Bayesian Information Criterion (BIC) to ensure the best fit with parsimony. To account for serial correlation, an autocorrelated errors model was applied, and confidence intervals for the Annual Percent Change (APC) and Average Annual Percent Change (AAPC) were estimated using 5001 resamples with the empirical quantile method.
To explore the relationship between hospital and community service utilisation, we summarised CMH activity by calculating the number of contacts and the corresponding age-specific rates for each diagnostic category. These measures were compared with HS rates using scatter plots with fitted linear regression lines (95% CI) in Jamovi (version 2.6.17) to visually assess correlations between inpatient and community-based service use across diagnostic groups.
Results
Overall trends in hospital separations and community contact rates
Figure 1(a) shows HS rates/100,000 population, and Table 1 presents annual APC estimated using Joinpoint regression. HS for key diagnostic groups, substance-use, mood, neurotic/stress-related, and behavioural/emotional disorders, rose steadily between 2013 and up to 2021 before declining sharply thereafter. Mood-disorders increased by 3.9% per year until 2021 and then dropped by 19.3%, while stress-related disorders followed a similar pattern (APC +3.9%, then −10.4%). Behavioural/emotional disorders rose fastest (+4.8%) before declining (−24.5%), whereas substance-use peaked in 2019 (+2.7%) and subsequently fell by 7.3%. Hospital separation rate/100,000 population (a); community contact rate/100,000 population (b). Trend in mental health hospitalisation rate in Australian youth (≤25 years) in related diagnosis aAAPC: Average annual percentage change. bAPC: Annual percentage change.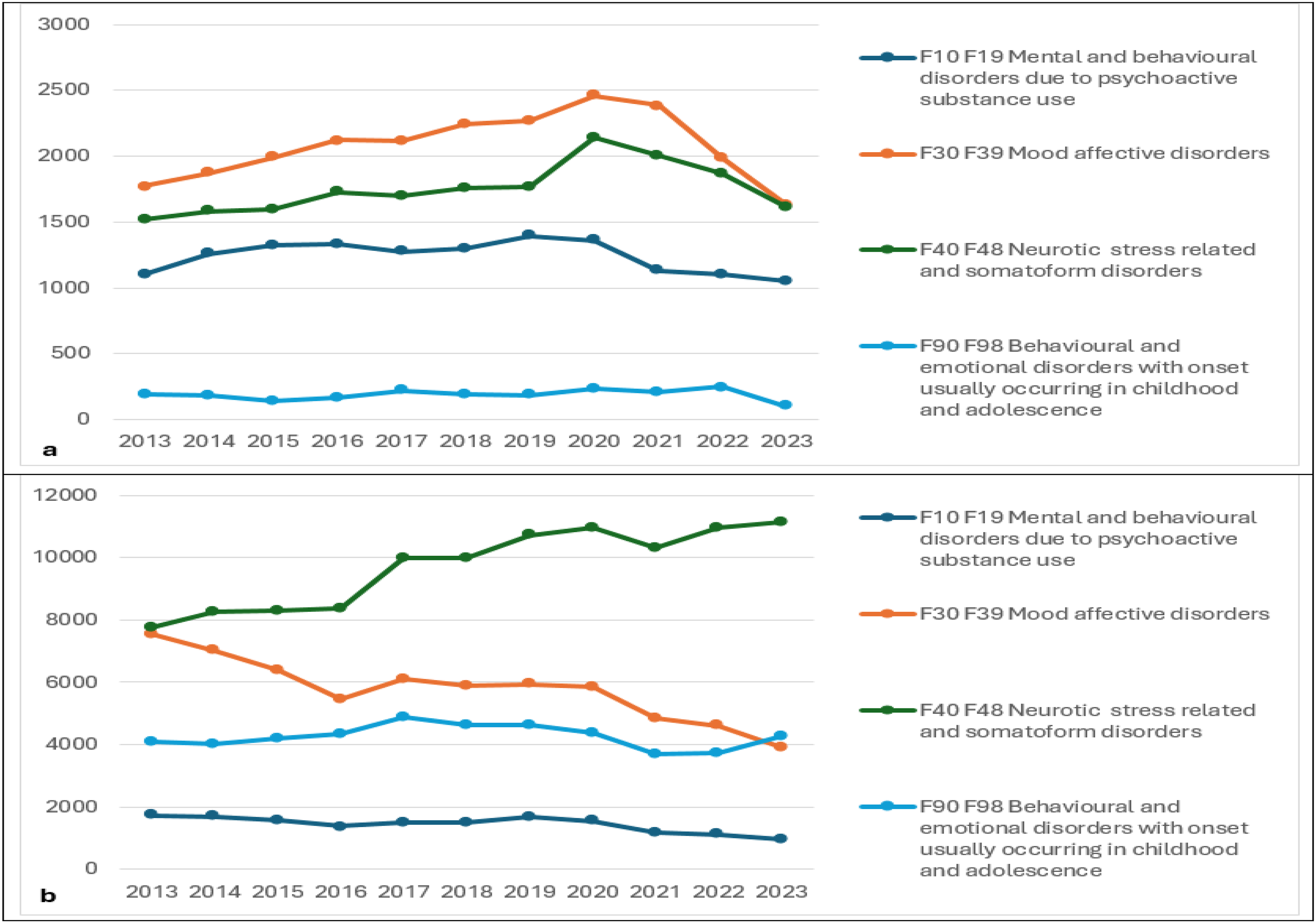
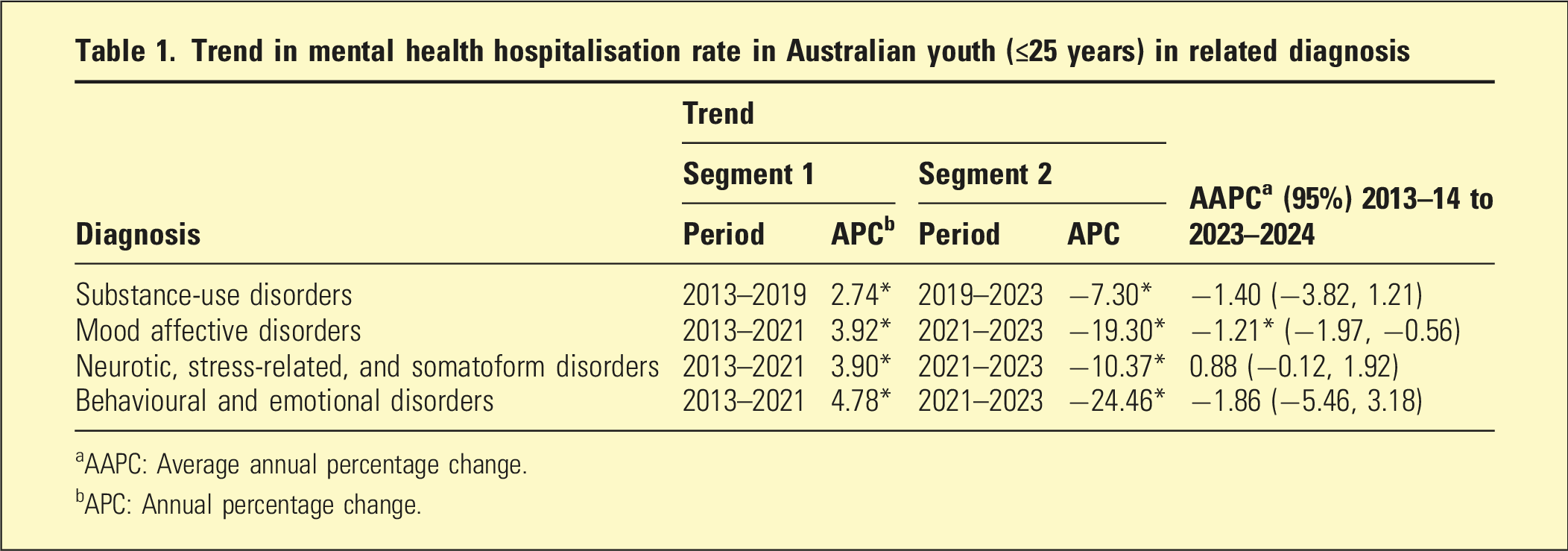
Figure 1(b) shows CMH contact rates increased throughout the same period, surpassing HS by 2023 for stress-related conditions. Trends presented here reflect service utilisation within the included CMH, not the underlying community prevalence.
Figure-S-1 further supports these findings, showing strong positive correlations between CMH contact and HS across diagnostic categories. This was strongest for mood and neurotic/stress-related disorders, moderate for substance-use, and weakest for behavioural/emotional disorders.
Diagnosis and gender-related trends with disease burden
Trend in mental health prevalence, incidence, DALY, and hospitalisation rate in Australian youth (≤25 years) in related diagnosis
aAAPC: Average annual percentage change.
bAPC: Annual percentage change.
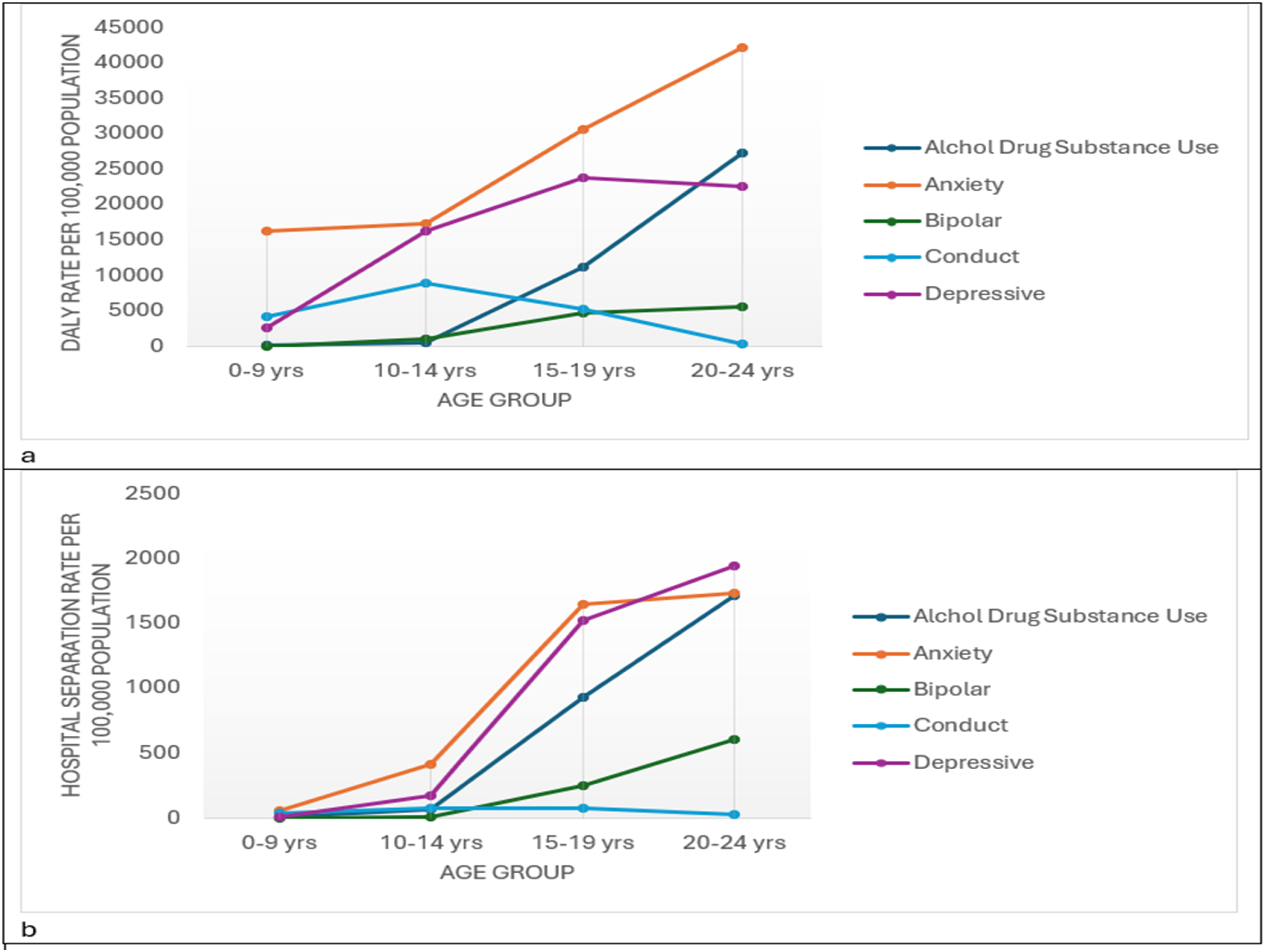
The mental disorder DALYs (a) and hospital separation (b) rate per 100,000 population in Australian youth (≤25) by different age groups 2013–2023.
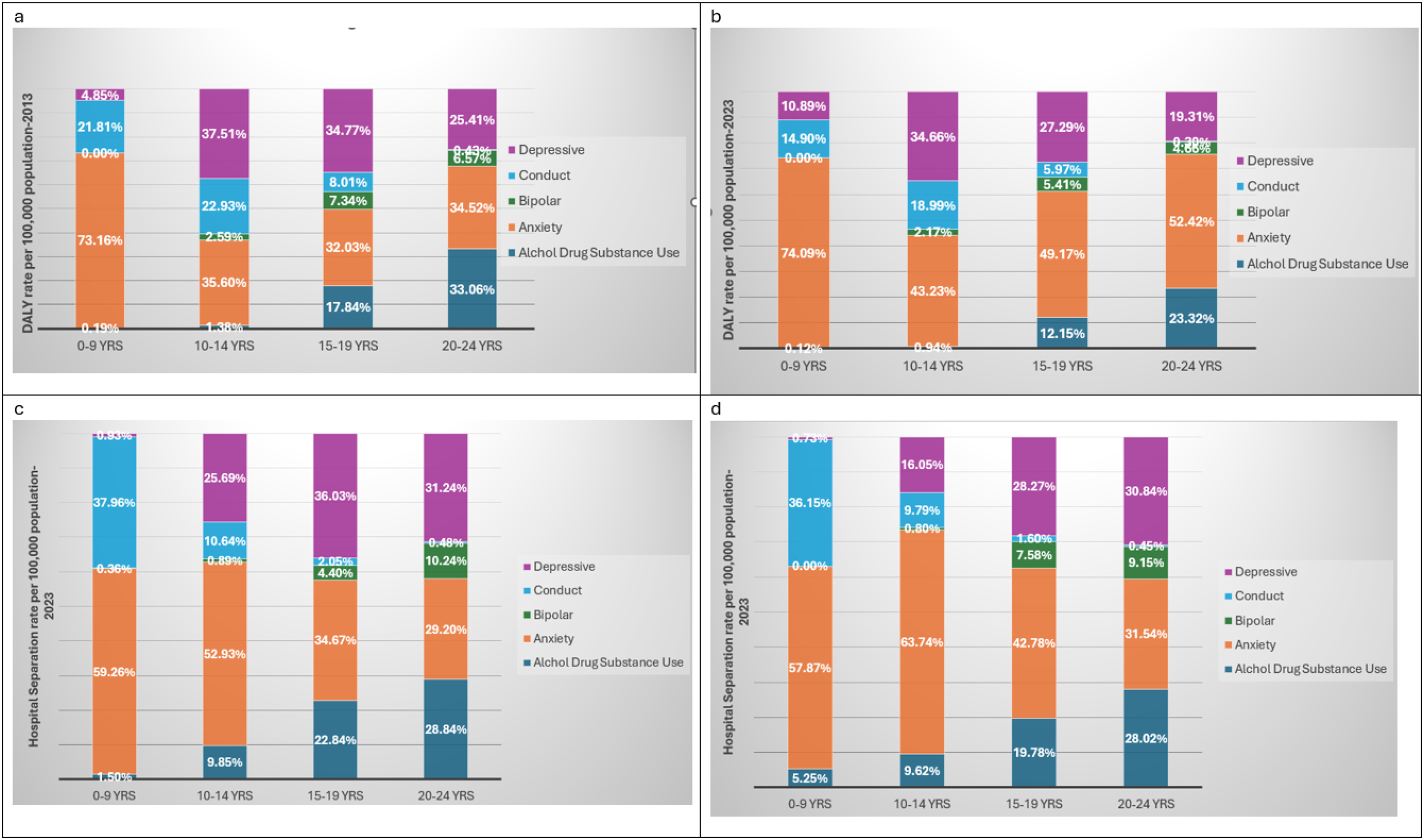
Proportional distribution of age-standardised DALY rates for mental disorders by cause within each age group in 2013 (a) and 2023 (b); proportional distribution of age-standardised mental disorder–related hospital separation rates by cause within each age group in 2013 (c) and 2023 (d).
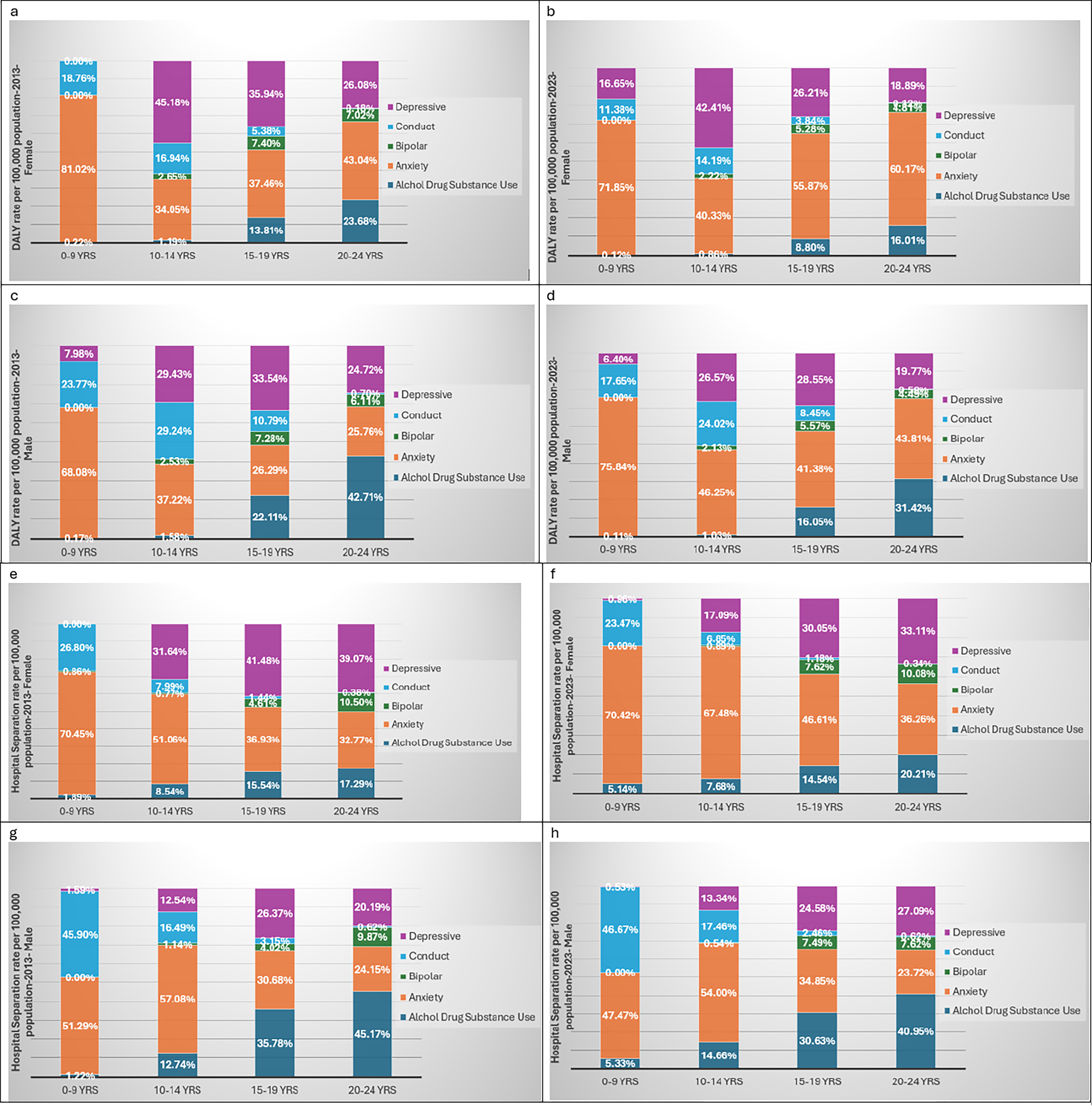
Proportional distribution of age-standardised DALY rates for mental disorders by cause within each age group, females 2013 (a), and females 2023 (b); males 2013 (c), and males 2023 (d); proportional distribution of age-standardised mental disorder–related hospital separation rates by cause within each age group, females 2013 (e), and females 2023 (f); males 2013 (g), and males 2023 (h).
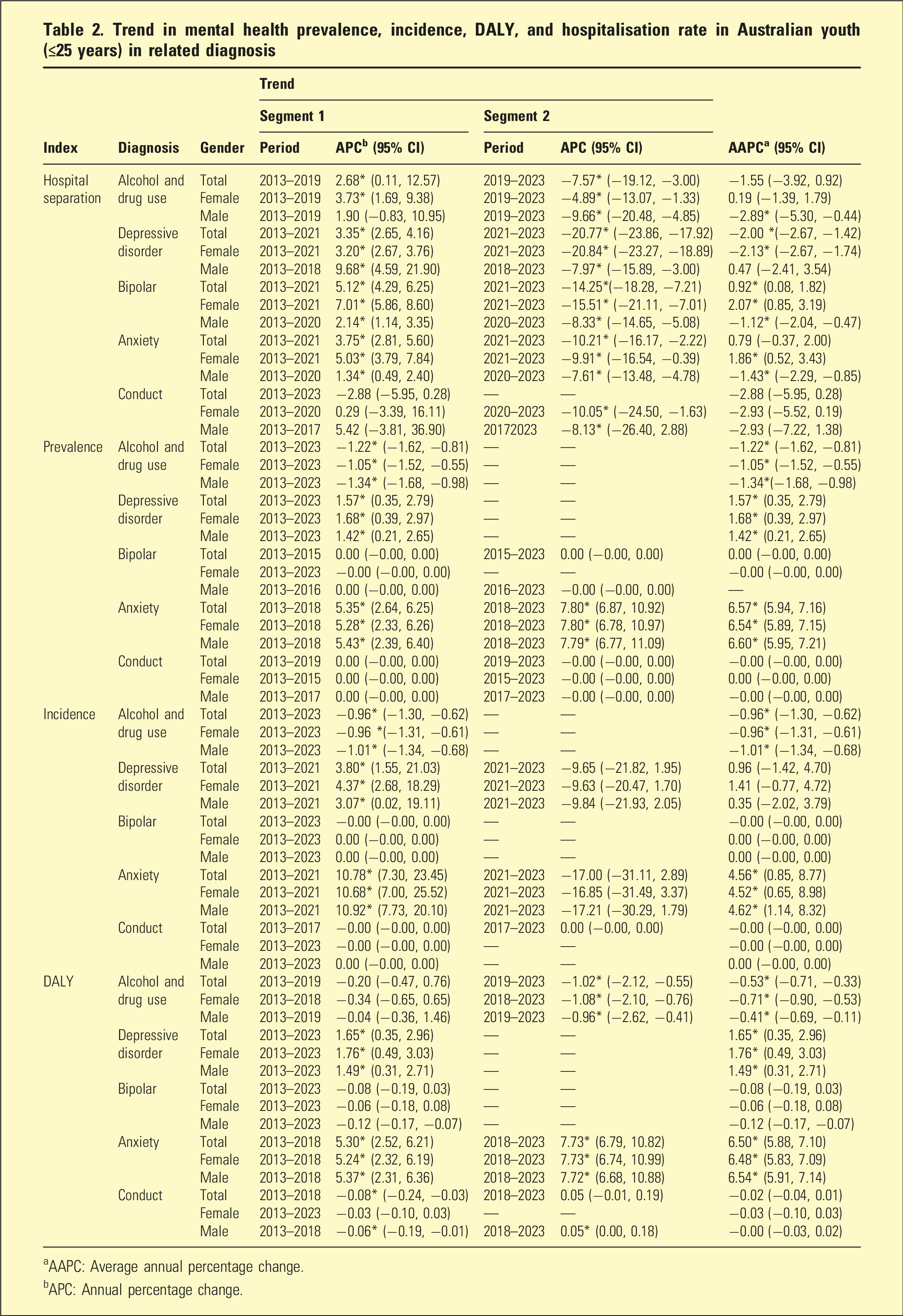
As shown in Table 2 HS for depressive disorders increased steadily until 2021 (+3.4%) before a marked decline (−20.8%), giving an overall AAPC of −2.0% (p < .05). However, Figure 3(b) shows that depression continued to account for a large share of total DALYs in 2023, even though its DALY’s proportion declined. Anxiety-disorders (F40-F48) followed a similar pattern, rising by 3.8% APC of HS per year until 2021 before declining by 10.2%, while AAPC DALYs increased by 6.5% annually (Table 2). Figure 2(a) show anxiety remaining the leading cause of DALYs in younger adolescents, and Figure 3(a)–(b) shows its proportion increasing in 2023 compared with 2013.
Bipolar disorder trends (Table 2; Figure 1(a)) show HS rising by 5.1% until 2021 and then decreasing by 14.3%, with a small net increase overall (+0.9%). DALY rates were stable during the study period.
Substance-use separations peaked in 2019 (+2.7%) and declined thereafter (−7.6%), producing an overall AAPC of −1.6%. DALYs also decreased slightly (Table 2). Figure 3(b) highlights that substance-related burden remains high among older youth (15–24 years). Similarly, conduct disorders showed proportional declines in both DALYs and separations (Table 2; Figure 1(a), F90-F98).
Across all diagnostic groups during 2013–2023 (Table 2), sex differences were most evident in HS: females showed net increases for bipolar (AAPC + 2.1%) and anxiety (+1.9%), in contrast to net declines in males. Males declined significantly for substance-use disorder (−2.9%), whereas separations increased slightly in females. Post-2019/2021 declines in HS were generally steeper in females (depressive-disorder, bipolar, anxiety, conduct). Trends in prevalence, incidence, and DALYs were broadly similar by sex. These gender differences are consistent with the overall diagnostic distribution shown in Figure 3(b)–(d) and Figure 4(b)–(d), where emotional conditions such as depression and anxiety make up a larger share of total burden in females, and behaviour-related and substance-use disorders contribute more among males’ youth.
Composition of burden and hospitalisation data
Figure 3 shows a gradual change in the composition of youth mental-health burden and hospitalisation between 2013 and 2023. In 2013 (Figure 3(a)), anxiety-disorders accounted for the largest share of total DALYs among young people, while depressive and substance-use disorders contributed moderately, and conduct disorders made up a smaller proportion. By 2023 (Figure 3(b)), anxiety remained the leading cause of DALYs, and its relative share increased compared with 2013, while the proportions for depressive and substance-use disorders declined slightly. These changes suggest that anxiety has become the most persistent and widespread source of MH burden among young Australians, particularly in mid-to-late adolescence.
Discussion
Main findings
The results provide evidence that, over the past decade, youth MH care in Australia has increasingly shifted toward community-based management. This shift reflects a broader move from hospital-based to community-based care, consistent with the 2015 National MH Commission’s advice to redirect resources from inpatient to community settings. 21 However, this change occurred amid limited inpatient growth, as new acute beds were offset by reductions in non-acute capacity and shorter lengths of stay. 22 AIHW specialised facilities data 23 show that child and adolescent MH hospital beds were broadly stable at around 5–6 beds per 100,000 population from 2013–14 to 2022–23, while ‘youth’ beds slightly increased from 1 (2014–15) to 3 per 100,000 (2022–23). During the period, although hospital capacity remained stable, service demand rose due to increased psychological distress and emergency department presentations following the COVID-19 pandemic.24–26 Broader social issues such as financial hardship, housing insecurity, and cost-of-living pressures likely intensified the severity of presentations. 21 On the other hand, the pronounced change in hospitalisations around 2020–21 may also reflect reduced access to (or avoidance of) hospitals during COVID-19 lockdown periods, with greater reliance on community-based care; whether this is a sustained shift or partly a pandemic-related effect should be monitored in post-pandemic data.
The strong positive correlations between CMH contact and HS suggest a response relationship, where expanded community services may initially increase hospitalisations through improved detection and referral, followed by stabilisation or decline as outpatient capacity strengthens. The weaker relationship for behavioural/emotional disorders may emphasise continuing challenges in early detection and access among younger groups. However, these are descriptive and not causal correlation.
Although depressive-disorder separations declined after 2021, depression remained a major contributor to DALYs in 2023, suggesting sustained burden despite fewer hospitalisations and likely reflecting improved community management rather than reduced prevalence. Higher APC values among females are consistent with global findings that adolescent girls experience greater increases in depressive symptoms due to biological and social factors. 27
For anxiety-disorders, DALYs increased steadily while HS declined after 2021. Anxiety remained the leading cause of DALYs in younger adolescents, consistent with findings by Watkeys et-al 28 in NSW. Greater screening and the availability of digital and community programs such as headspace and Better Access have likely improved early detection and outpatient management. 29
Bipolar-disorder trends showed HS rising until 2021 and then decreasing, while DALY rates were stable, indicating effective long-term care rather than recovery. Higher APC values of HS among females may reflect improved recognition of depressive-dominant or mixed episodes. 30 For substance-use disorders, separations peaked in 2019 and declined thereafter, with a modest decline in DALYs. These results mirror national trends showing reduced youth smoking and alcohol consumption but increased e-cigarette and illicit-drug use, particularly among young women. 31 Conduct disorders also showed proportional declines in both DALYs and separations, reflecting reductions in externalising behaviours and improvement in early-intervention access. 28
The observed gender differences are consistent with findings from the literature27,28 showing that females are more affected by emotional disorders and males by behaviour-related conditions.
The composition of burden and hospitalisation data showed an increasing share of anxiety burden, consistent with global evidence of rising anxiety among youth 27 driven by social and environmental stressors. Modest decline in depressive and substance-use burden may indicate benefits from early intervention and harm-reduction programs, and improved community-care. Yet persistently high anxiety and mood-related burden likely reflect ongoing social, digital, and socioeconomic pressure, and post-pandemic uncertainty.21,32
Triangulation of findings
In line with the study objectives, we applied a triangulation approach to integrate inpatient and CMH data (Figures 1–3; Tables 1–2) with population-level burden and system indicators (Figure 4 and Figures S-2). This method examined whether changes in hospital use reflected actual variation in youth mental illness or were influenced by service capacity, access, and shifts toward community care. By combining service data with DALYs from the GBD framework, the analysis provides a clearer understanding of how youth MH needs and service responses have changed in Australia from 2013 to 2023.
The integrated evidence shows a strong positive relationship between DALYs and hospitalisation rates (Spearman’s r = 0.77, p < .001; Figure S-2), suggesting that hospital use generally reflects population illness levels. Overall, the findings indicate continuing increases in DALYs of depression and anxiety, even with the expansion of government-supported community programs such as Better Access, which funds Medicare-subsidised MH care, and headspace, a national network of youth-MH centres.27,29 Conduct and substance-use disorders have decreased, likely due to public-health and harm-reduction efforts 31 ; however, this may be accompanied by emerging or less visible forms of psychological distress associated with online and social media exposure as shown in previous studies. 32 Strong positive relationship between HS and CMH contact rates indicated that changes in one part of the system are closely linked to the other. Together with the time-series trends, this suggests a gradual move toward greater community-based care, although limited bed capacity and workforce pressures may still conceal unmet demand. 21 The highest burden remains among older adolescents aged 15–24 years with girls more affected by mood and anxiety problems and boys by substance-use.25,27,28 Evidence suggests that around two in five young people receiving care have multiple diagnosis,28,30 showing the growing complexity of youth MH care and the need for stronger coordination between services.
Limitation
A key limitation is reliance on retrospectively collected administrative datasets where diagnoses may be incomplete or inconsistently coded. The dataset captures contacts only within included services, potentially underestimating care delivered elsewhere, particularly in periods or subgroups with greater uncaptured services. Finally, limited detail on potential confounders (e.g. severity and social factors) means residual confounding is possible, and missing data or linkage error may reduce precision and attenuate associations.
Implications of the study
Findings revealed that Australia’s youth MH system is undergoing structural consolidation but also facing increasing clinical complexity. HS have declined, and CMH has expanded, yet the burden continues to grow. This pattern reflects international trends where service expansion improves access but not always outcomes.27,29
Contributing factors include socioeconomic pressures, digital exposure, and post-pandemic effects, adding vulnerability among socially disadvantaged youth.21,32 The sustained increase in DALYs rates for depression and anxiety signals a key policy implication: reduced hospitalisation does not equate to improved population outcomes. While community and primary care have alleviated acute demand, they have yet to produce measurable declines in total disease burden. This finding points to the need for continued emphasis on prevention, resilience building, and long-term recovery strategies across educational, occupational, and digital settings. However, reductions in population-level burden may be modest unless upstream determinants are addressed in parallel. This highlights the importance of cross-sector approaches that combine MH strategies with wider social and environmental policy action.
Future priorities should include maintaining community-care capacity while addressing hidden demand, improving early identification and continuity of care, and strengthening coordination across service sectors to better manage complex and comorbid cases. Prevention, early support, and long-term recovery strategies are essential to turn access gains into measurable improvements in health outcomes.22,29
Supplemental material
Supplemental Material - Hospitalisation and burden of major psychiatric and behavioural disorders among young populations in Australia: Trends and epidemiological insights (2013–2023)
Supplemental Material for Hospitalisation and burden of major psychiatric and behavioural disorders among young populations in Australia: Trends and epidemiological insights (2013–2023) by Somayyeh Azimi, Nasir Uddin, Kirsty Snelgrove, and Ettore Guaia in Australasian Psychiatry
Footnotes
Acknowledgements
Microsoft Copilot was used to assist with English-language editing (grammar and clarity). All scientific content, interpretations, and conclusions are those of the authors.
Ethical considerations
This study analysed publicly available, anonymised data from the Australian Institute of Health and Welfare and Institute for Health Metrics and Evaluation. No new data were collected from human participants by the authors. Therefore, formal ethics approval and informed consent were not required. The research was conducted in accordance with the principles of the Declaration of Helsinki, the National Statement on Ethical Conduct in Human Research (National Health and Medical Research Council), and relevant privacy legislation.
Funding
The authors received no external financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support this study are freely available online Australian Institute of Health and Welfare and Institute for Health Metrics and Evaluation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.