
Abstract
Objective
Post-traumatic nightmares (PTNs) are a debilitating symptom of post-traumatic stress disorder (PTSD), yet evidence for pharmacological treatment remains inconsistent. This audit examined the effectiveness and tolerability of prazosin for PTNs in an Australian inpatient psychiatric population.
Method
A clinical audit with pre-test post-test analysis was conducted using records from Monash Health wards. Adult patients (n = 50) prescribed prazosin for PTNs for ≥7 days were included. Symptom severity was measured using the Clinical Global Impression-Severity (CGI-S) scale at treatment initiation and discharge, and clinical response using the Clinical Global Impression-Improvement (CGI-I) scale. Demographics, trauma histories, comorbidities, dosing, and adverse effects were also recorded.
Results
Participants were predominantly female (74%) and aged 18–34 years. The median CGI-S improved from 5 (“markedly ill”) to 2 (“borderline mentally ill”), representing a 3-point reduction (p < .01). CGI-I ratings indicated patients were “much improved” (median = 2). Prazosin was discontinued in 12 of 114 patients, most commonly due to dizziness or hypotension.
Conclusions
Prazosin was associated with clinically and statistically significant improvements in PTNs in this cohort, noting confounding variables and subjective assessment with no control group. Findings support clinical use while underscoring the need for larger, prospective Australian trials.
Background
Post-traumatic stress disorder (PTSD) affects 11% of Australians. 1 Post-traumatic nightmares (PTNs) occur in up to 90% of individuals with PTSD and trauma-related disorders. 2 Treatments for PTNs remain off-label due to limited evidence. 3 Prazosin, an α1-adrenergic antagonist traditionally prescribed for hypertension and prostatic hyperplasia, has emerged as a treatment for PTNs, though clear guidelines have not yet been established. 4 Despite this lack of evidence, 86% of Australian and New Zealand psychiatrists report having prescribed prazosin in their careers. 5
PTSD
As described in Appendix A, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) defines PTSD as requiring direct, witnessed, or indirect exposure to actual or threatened death, serious injury, or sexual violence. 6 A diagnosis also requires the presence of symptoms across four domains: intrusion (e.g. distressing dreams), avoidance, negative alterations in cognition and mood, and hyperarousal (e.g. sleep disturbances).
PTNs
PTNs are not clearly defined in the literature. For this audit, the definition is based on the DSM-5-TR description as recurrent distressing dreams in which the content and/or affect is related to the traumatic event(s). 6 These nightmares are thought to be driven by sympathetic noradrenergic drive. 7
Prazosin
Prazosin, an α1-adrenergic antagonist, is utilised for hypertension and prostatic hyperplasia. 4 Patented in 1965, prazosin lowers blood pressure by relaxing smooth muscle and reducing vascular resistance, while also crossing the blood–brain barrier.4,8 PTSD is characterised by sympathetic arousal and hyperadrenergic activity, 9 suggesting that α1-adrenergic blockade may have therapeutic benefits. 10 By blocking α1-adrenergic receptors, prazosin reduces noradrenaline activity in brain regions including the amygdala and locus coeruleus. 4 This mechanism is thought to underlie effects in decreasing hyperarousal, improving sleep, and reducing PTNs. Prazosin is also widely accessible and affordable in Australia.
Current guidelines
Current Australian guidelines (Phoenix Australia) dictate first-line medications for PTNs and PTSD are antidepressants (selective serotonin inhibitors or venlafaxine). 11 While prazosin is not included in these guidelines, Phoenix Australia published a document that outlines titration guidelines adapted from Cardiff University School of Medicine. 11
Literature review
A literature review was conducted for this audit using the Cochrane, PubMed, and Ovid MEDLINE databases. A summary of the current literature is provided in Appendix B, while a synthesis of findings is presented here.
Prazosin was first reported to have therapeutic effects in PTSD by Raskind in a case series involving four Vietnam War veterans prescribed prazosin for PTSD. 12 Two participants achieved elimination of PTNs after reaching a dose of 5 mg, while the other two, prescribed 2 mg, experienced a 50% reduction in PTN severity. This landmark study initiated investigations into the efficacy of prazosin for PTSD and PTNs. These included an open-label trial and a chart review conducted by Raskind and colleagues in 2002, both of which demonstrated significant efficacy.13,14
Following this, the first placebo-controlled trial was conducted by Peskind in 2003, where nine Holocaust survivors received 2–4 mg of prazosin. 15 Participants experienced reductions in PTNs and a decrease in PTSD severity. Over the following decade, multiple controlled trials were undertaken by Raskind, Taylor, and others. These studies reported significant reductions in PTNs across populations including veterans, civilians, and refugees.16–25
However, in 2018, Raskind et al. published the largest RCT, involving 152 veterans, which found no significant differences between prazosin and placebo for PTNs. 26 This was the first trial to contradict earlier findings and had considerable implications for practice. Following its publication, the American Academy of Sleep Medicine downgraded guidelines regarding prazosin as a treatment for PTSD and PTNs. 27 The perception of prazosin shifted, with hesitancy in prescribers due to conflicting evidence.
Rationale
Recommendations in Australia and globally do not strongly support the use of prazosin. However, this position is based on one RCT, despite a broader body of supportive evidence. The rationale for this audit is to improve the limited evidence base, enabling the development of a larger dataset for analysis. Data on an Australian population and their characteristics will provide evidence specific to this context, informing local guidelines.
This audit also informs future research by applying a systematic approach to chart reviews of nightmares in patients with PTNs in inpatient settings. Although nursing/medical documentation is limited by variability, this audit seeks to demonstrate feasibility of such an approach for research in the future.
The choice of a retrospective chart review audit is justified by both the accessibility of existing data and the feasibility within available resources.
Research aims
The primary aim of this audit is to determine the safety and efficacy of prazosin for treatment of PTNs as currently prescribed. Establishing whether prazosin has a significant effect will help guide future research and contribute to the broader evidence base needed for higher-level analyses.
A secondary aim is to document tolerability among individuals treated with prazosin. Identifying patients who cannot tolerate the medication due to side effects will inform the practicality of its use and inform education of patient expectations.
Dosages and participant characteristics will be recorded to provide insights into the effective dose range of prazosin for PTNs. Although these data will not be analysed, they will be presented to highlight patterns.
Hypothesis
For those experiencing PTNs in inpatient adult psychiatric wards under Monash Health, those who receive prazosin for at least 7 days will have a significant improvement in the severity of their PTNs.
Method
Audit design
This is a clinical audit of inpatients experiencing PTNs, with data collected before and after use of prazosin. Pre-post analysis was conducted on the same sample of patients.
Sampling
Utilising Monash Health pharmacy dispensation data across seven inpatient wards (four adult, one young adult, one mother-baby unit, and one geriatric ward), 316 patient files were assessed as individuals who were dispensed prazosin on adult mental health wards. The data ranged from 2nd of September 2019 (beginning of electronic records at Monash Health) to collection date of 23rd of July 2025. Of these records, inclusion/exclusion criteria were applied. Inclusion criteria were 18-years-old or older; commenced on prazosin as an inpatient for the treatment of PTNs. Exclusion criteria were continued home medication, indication other than PTNs, ceased prior to discharge, inadequate documentation, and less than a 7-day course.
Data collection
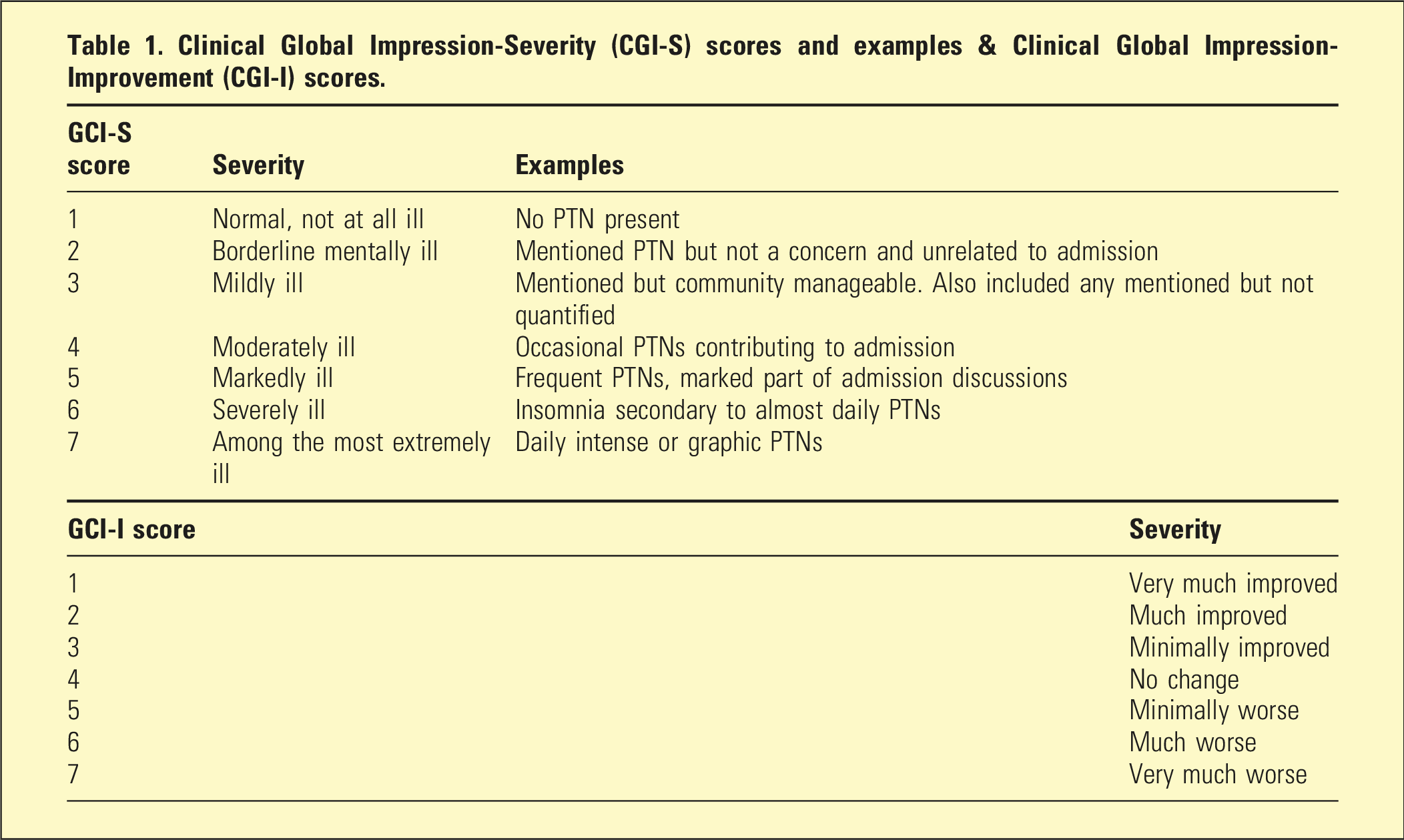
Clinical Global Impression-Severity (CGI-S) scores and examples & Clinical Global Impression-Improvement (CGI-I) scores.
Demographics for the selected patients were also noted to support insights gained from analysis while avoiding identifiability. This included age group (18–24, 25–34, 35–44, 45–54, 55–64, 65+), birth country, type of trauma (as described in reviews), and additional diagnoses (all diagnoses listed on discharge summary as contributing to admission). These characteristics were left broad to ensure privacy of patients.
Additional outcomes include reason for cessation prior to discharge to assess significantly adverse reactions, and the doses of prazosin on commencement and discharge guiding physicians in prescribing target doses.
CGI-S and CGI-I were formed by author CH using clinical experience to guide the exact scores following data collection, and a random selection of 10% (using Microsoft Excel random number generator) CGI scores were reviewed by another psychiatric registrar, ensuring inter-rater reliability.
Data analysis
The CGI-S (commencement of prazosin, and discharge from acute or subacute ward) and CGI-I (on discharge from inpatient ward) data analysis was completed in Microsoft Excel (median, interquartile range, percentage change) and SPSS (Wilcoxon signed-rank test for statistical significance with a p value of <0.05; effect size calculated as rank-biserial correlation with r = 0.10, 0.30, and 0.50 representing small, medium, and large effects, respectively).
Tolerability was assessed descriptively using discontinuation rates and frequency of adverse effects as a proportion of all patients commenced on prazosin for the first time, for any duration.
Results
316 patients were assessed with 50 included for analysis, as described in Figure 1. This spanned from 2nd of September 2019 to 23rd of July 2025. Inclusion and exclusion of participants.
Participant age group, sex, birth country, type of trauma, and additional diagnoses.
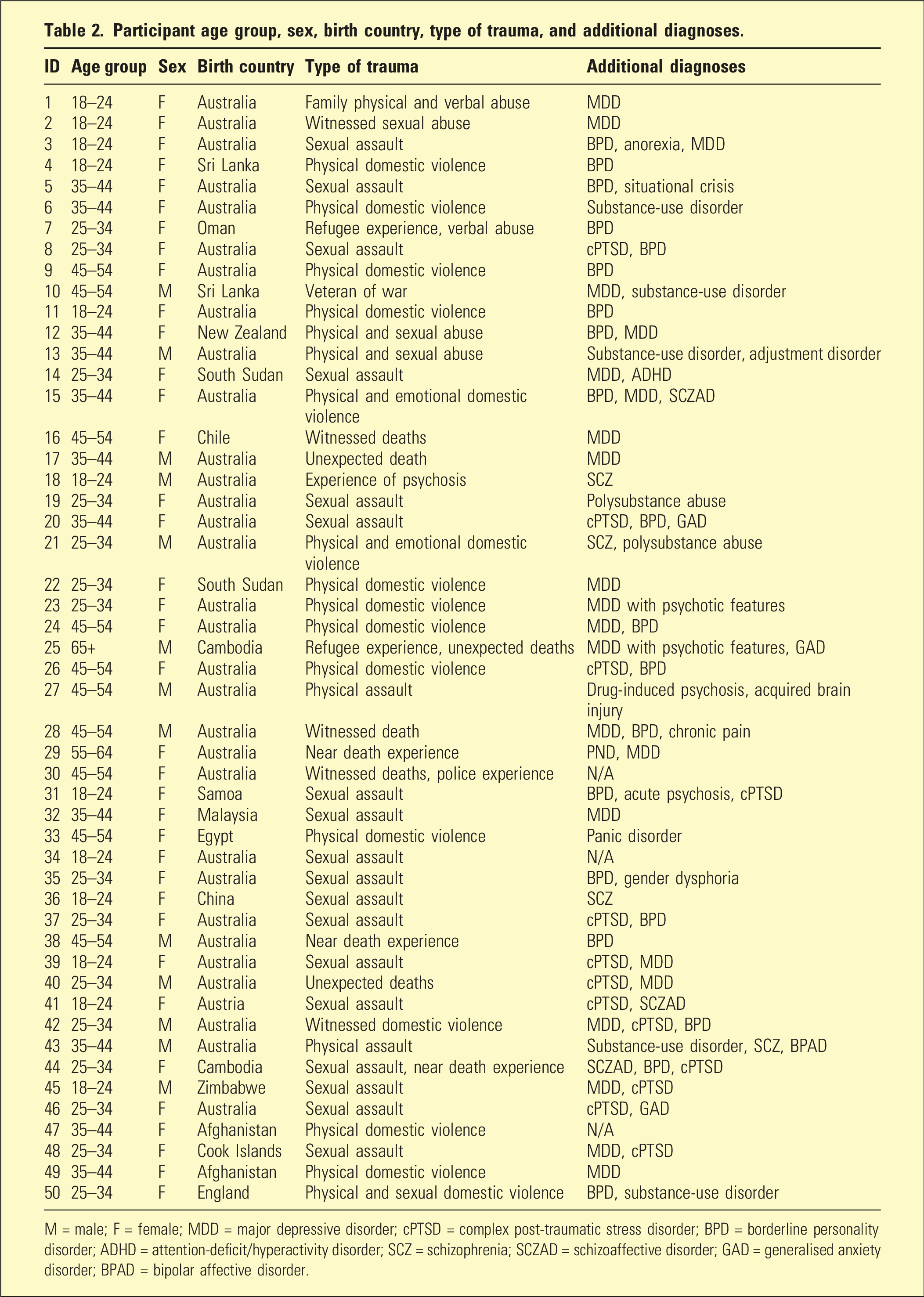
M = male; F = female; MDD = major depressive disorder; cPTSD = complex post-traumatic stress disorder; BPD = borderline personality disorder; ADHD = attention-deficit/hyperactivity disorder; SCZ = schizophrenia; SCZAD = schizoaffective disorder; GAD = generalised anxiety disorder; BPAD = bipolar affective disorder.
Types of traumas are described in Table 2, noting several had multiple forms of trauma. The most prevalent themes were sexual (n = 21), physical (n = 19), domestic violence (n = 15), with other less prevalent being near death experience (n = 3), witnessed death (n = 3), unexpected death (n = 3), emotional abuse (n = 2), refugee trauma (n = 2), verbal abuse (n = 2), police experiences (n = 1), psychosis (n = 1), war experiences (n = 1), witnessed domestic violence (n = 1), and witnessed sexual abuse (n = 1).
Additional diagnoses were assessed from discharge summary diagnoses as contributing to the admission reviewed (which do not necessarily meet diagnostic manual diagnoses but may be more descriptive terms). These diagnoses are listed in Table 2, where many had multiple comorbidities. It is noted that all patients met the criteria for PTSD. The most common comorbidities were major depressive disorder (MDD; n = 23), borderline personality disorder (BPD; n = 19), and complex post-traumatic stress disorder (cPTSD; n = 13).
Prazosin doses individually are displayed in Graph 1. Dosages for patients on commencement ranged from 0.5 mg to 2 mg, with an average of 1.01 mg. Doses on discharge ranged from 0.5 mg to 10 mg, with an average of 2.44 mg. Prazosin doses on admission and discharge.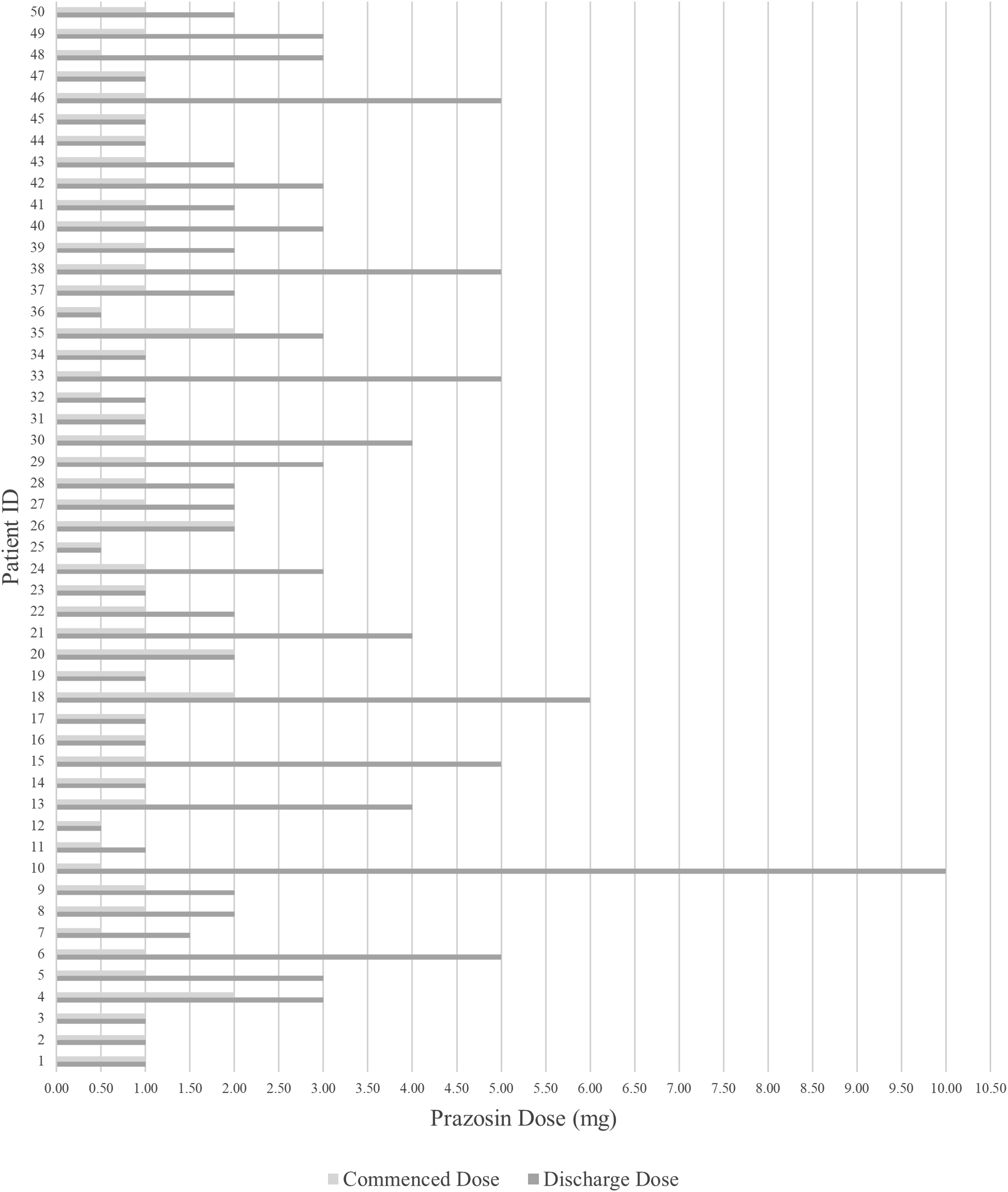
Total days on prazosin ranged from 7 to 253 days (interquartile range [IQR] 8 to 22), with an average of 26.08.
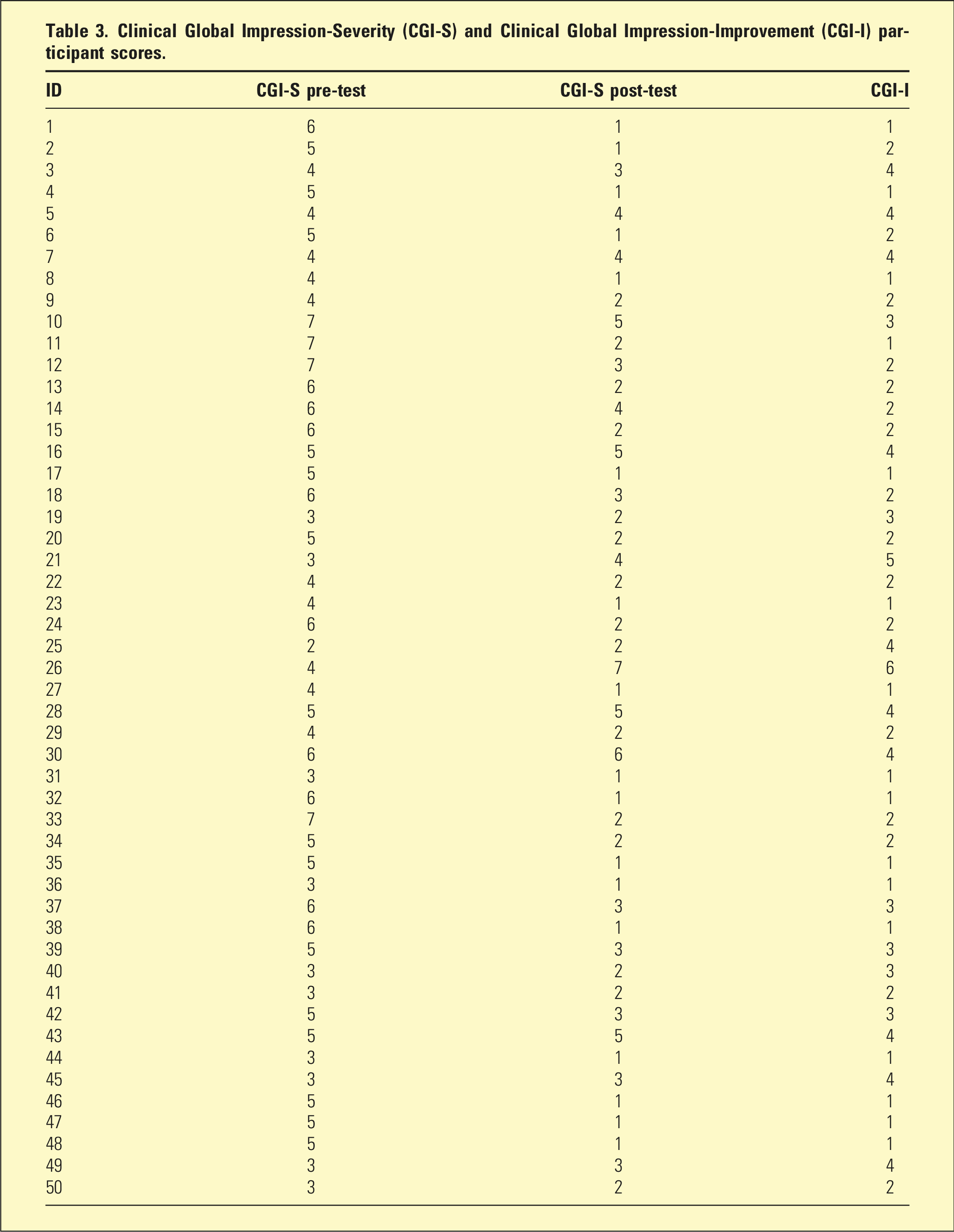
Clinical Global Impression-Severity (CGI-S) and Clinical Global Impression-Improvement (CGI-I) participant scores.
Excluding those with inadequate documentation, of all adult patients commenced on prazosin for PTNs with any duration given (n = 114), the adverse effect discontinuation rate was 7.9% (9/114), with an overall discontinuation rate (including self-cessation) of 10.5% (12/114). The reasons included adverse effects thought to be due to prazosin: lack of efficacy (n = 3), dizziness (n = 2), postural hypotension (n = 2), nocturnal enuresis (n = 1), worsened hyperarousal (n = 1), and syncope (n = 1). Two also self-ceased with no adverse effects.
Discussion
This audit reviewed 50 adult inpatients prescribed prazosin for a minimum of 7 days for PTNs as an adjunct to inpatient treatment. The findings demonstrated a significant reduction in PTN severity between treatment initiation (CGI-S median = 5; IQR = 4 to 6) and follow-up (CGI-S median = 2; IQR = 1 to 3), with statistical significance (Z = −5.300, p < .01, r = 0.750), indicating a large treatment effect. CGI-I further reflected a median rating of “much improved” (median = 2; IQR = 1 to 3). As these patients received concurrent treatments in an acute ward environment, findings should not be attributed solely to prazosin and must be interpreted with caution. Nevertheless, these results support the hypothesis that adjunct prazosin use for at least 7 days is associated with PTN improvement in inpatients.
These findings align with the earlier positive prazosin literature but diverge from Raskind’s 2018 RCT, which reported no significant benefit over placebo in 152 US veterans. 26 Several population differences may account for this divergence. Raskind’s cohort consisted exclusively of male US veterans with combat-related PTSD, whereas this cohort was predominantly female (74%) with trauma arising largely from sexual and physical violence – a profile more representative of the broader Australian PTSD population, where approximately 77% of cases occur in females. 1 Importantly, this cohort was also acutely unwell inpatients, compared with Raskind’s stable outpatient veterans, and symptom severity at baseline was high (CGI-S median = 5), leaving substantial room for measurable improvement. These factors, combined with the adjunctive inpatient treatment environment, may explain the more pronounced response observed here. To the authors’ knowledge, this is the largest audit examining prazosin for PTNs in an Australian cohort, contributing important – though observational – evidence to the literature dominated by US veteran studies of limited generalisability to Australian practice. 5
The sample characteristics of this cohort have practical implications for Australian psychiatrists. The prevalence of sexual and physical trauma, including domestic violence, as the predominant trauma types mirrors the presentations seen in Australian acute psychiatric settings and suggests prazosin may be particularly relevant in this population. The sex distribution (74% female) closely reflects PTSD prevalence in Australia, 1 and the high rates of comorbid MDD and BPD reflect the complex presentations typical of Australian inpatient populations. 29 Regarding trauma type, the underrepresentation of witnessed trauma may reflect a tendency in clinical assessment to emphasise personally experienced events, warranting greater clinician awareness.
The mean commencement dose of 1.01 mg was consistent with Australian guidelines, 11 though the mean discharge dose of 2.44 mg fell well below the recommended target of up to 10 mg nightly – yet significant improvement was still observed. This suggests that even conservative dosing within inpatient admission timeframes may be clinically meaningful, which is a practical consideration given the brevity of acute admissions. While dose-response relationships could not be assessed, improvement was observed across this range, underscoring the need to re-examine current titration guidelines in the context of inpatient settings. Given the affordability and accessibility of prazosin in Australia, these findings support its continued use as an adjunct treatment while awaiting more definitive trial evidence.
Limitations
This audit has several important limitations. As a retrospective chart review, it is subject to inherent constraints, including documentation bias and uncontrolled confounding variables. The absence of a control group prevents attribution of improvements in PTN severity to prazosin alone, as concurrent medications, psychotherapy, or the therapeutic milieu likely contributed. While not examined, the authors noted several other medications (including antipsychotics and antidepressants) were prescribed that would impact PTNs. These patients were also presenting with psychiatric issues that have been treated and improved through various interventions and respite. Nevertheless, the indication of possible improvements from prazosin shows need for future research with control groups.
The outcome measures used rely on subjective assessments and do not fully capture the complexity of PTN symptoms. This limitation was mitigated to some extent through inter-rater comparisons. The single-centre design at Monash Health may restrict generalisability; however, the inclusion of patients across seven inpatient units with varied specialisations enhances representativeness within the setting.
The brief audit period limited follow-up duration compared with previous research, although this was limited by resources. In addition, excluding patients who discontinued prazosin within 7 days may have introduced selection bias, potentially overestimating tolerability and effectiveness. To address this, patients who ceased treatment were still documented to maintain clarity and transparency, though cautious interpretation of results is needed.
Overall, these limitations highlight the need for cautious interpretation and underscore the importance of prospective, controlled studies with larger populations.
Conclusions
This audit highlights the clinical and statistical association between prazosin use and improved outcomes for PTNs, alongside acceptable tolerability, in an Australian inpatient population, noting the limitations of confounding variables and subjective assessments. The lack of control group must be noted, meaning the effects observed cannot be interpreted as evidence of prazosin’s independent efficacy. These findings contribute to the limited existing literature and help to contextualise current prescribing by documenting effects observed in practice. Future research should focus on large-scale randomised controlled trials in this population and dose-response analysis to establish efficacy and to strengthen the evidence base needed to inform clinical guidelines.
Supplemental material
Supplemental material - Prazosin for post-traumatic nightmares: A clinical audit in acute public psychiatric unit patients
Supplemental material for Prazosin for post-traumatic nightmares: A clinical audit in acute public psychiatric unit patients by Conor Heeney, Samuel Rainbow, Anton Neville Isaacs, and Nicholas A Keks in Australasian Psychiatry.
Footnotes
Acknowledgements
Dr Anton Isaacs and Prof. Nicholas A Keks AM as supervisors for this research project.
Ethical Considerations
Ethical approval was not required for this audit. All patient data were fully anonymised, de-identified, and handled in accordance with the Declaration of Helsinki. The data used in this evaluation were collected for quality improvement purposes only Quality Assurance VIC Project ID 112631.
Author contributions
C.H. conceived idea and completed data collection, analysis, and full article. S.R. collected/analysed data for inter-rater reliability. N.K. performed project supervision and manuscript review. A.I. performed project supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the nature of the research, supporting data is not available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.