
Abstract
Objective
Older adults living with mental illness experience significant physical health inequities and premature mortality. The Equally Well (EW) framework promotes integrated, person-centred care to address these disparities, yet its application in older adult mental health services remains underexplored.
Method
Using a phenomenological approach, focus groups with nine allied health clinicians working in a community-based older adult mental health service explored understanding and implementation of EW. Data were thematically analysed using the Theoretical Domains Framework.
Results
Clinicians endorsed EW’s holistic intent but reported variable understanding, discipline-specific role ambiguity, administrative burden, and fragmented primary care as barriers, particularly in the context of frailty and multimorbidity. Facilitators included documentation prompts, multidisciplinary collaboration, and targeted training.
Conclusions
Allied health clinicians support EW principles but emphasise the need for organisational investment, practical training, streamlined documentation, and stronger primary-care links. Findings highlight the importance of age-sensitive adaptation of EW to ensure equitable physical health care for older adults with MI.
Older adults living with mental illness (MI) experience a disproportionate burden of physical health problems and premature mortality compared to the general ageing population.1,2 These inequities are driven not only by age-related physiological changes but also by systemic factors such as diagnostic overshadowing, fragmented care, and the under-recognition of physical health needs in mental health settings. 3 In Australia, the Equally Well (EW) Consensus Statement was introduced by the Australian Government in 2017 to address these longstanding disparities by promoting integrated, person-centred care that targets the physical health of people living with MI of all ages. 4
Although the EW framework shares features with broader physical health promotion and integrated care initiatives, it is conceptually distinct in its explicit focus on health equity for people living with mental illness. EW is a nationally endorsed framework that emphasises parity of physical health outcomes, shared accountability between mental health and primary care systems, and structural supports to embed physical health monitoring and follow-up within routine mental health care. In doing so, it moves beyond individual clinician goodwill toward a coordinated, system-level response to longstanding physical health inequities.
Despite its policy significance, implementation of EW in routine practice—particularly within older adult mental health services—remains underexplored. Older adults experience specific challenges, including ageism, multimorbidity, cognitive decline, reduced mobility, frailty, and complex transitions between health and aged-care systems, all of which may complicate the delivery of integrated physical health initiatives. 5 While mental health services are central to EW delivery, there is limited empirical understanding of how clinicians interpret and enact EW principles in day-to-day practice with older adults, whose needs often sit at the intersection of mental health and geriatric care. 6
Within this Victorian public older adult mental health service (OAMHT), allied health clinicians (AHC) commonly undertook routine physical health screening, documentation, health promotion, and liaison with primary care, while medical input was accessed as required. In the present study setting, AHC were primarily responsible for routine physical health processes, with medical input accessed as required. Accordingly, this study conceptualises EW implementation at the level of routine clinical practice, defined as how AHC interpret, operationalise, and enact EW principles in assessment, care planning, documentation, referral processes, and collaboration with primary care. This practice-focused approach aligns with EW’s emphasis on embedding physical health considerations within existing service structures and centres clinicians’ lived experiences of implementation.
Consequently, this study sought to explore how AHC in Victoria understand and implement the EW framework in their work with older adults with the intent of informing health equity strategies for older Australians with MI.
Despite growing attention to physical health promotion in mental health services, relatively few studies have examined how initiatives such as EW are implemented in older adult mental health settings (see Appendix A for literature search). This limited focus has important implications for service delivery and policy, as frameworks developed primarily for working-age populations may be applied without sufficient adaptation to later-life contexts.
Methodological rationale
Given this paucity of information, a qualitative design with a phenomenological lens was selected to explore clinicians’ lived experiences and meaning-making, and may improve clarity. This approach enabled an in-depth understanding of the contextual and behavioural factors influencing EW implementation, which are not easily captured through quantitative methods.
Aims/Objectives
The study aimed to explore how AHC understand and integrate EW principles into their work with older adults living with mental illness. Specific objectives were to: 1. Assess clinician awareness and understanding of EW; 2. Identify barriers to and facilitators of implementation; and 3. Generate clinician-informed recommendations for improving EW integration in practice.
Methods
Study design
This qualitative study employed a semi structured thematic approach, guided by phenomenological theory. Interview prompt questions were formulated to align with the study objectives and help focus participant responses (see Appendix). Ethical approval was obtained (LR24-062-113529).
Setting, participants and recruitment
The study was conducted in a community-based OAMHT. Within this service, AHC were primarily responsible for routine physical health screening, documentation, and liaison with primary care, with medical input accessed episodically or via external providers. In practice, this involved risk identification, health promotion, and coordination of investigations and treatment through general practitioners (GPs), with most ongoing management occurring in primary care.
The service operated under a brief intervention model (BIM), defined as time-limited, goal-directed episodes of specialist care focused on assessment, stabilisation, and care planning rather than ongoing case management. This model applies to the majority of cases, where time-limited multidisciplinary care is delivered with structured liaison to GPs. Patient care is then coordinated through GPs and, where relevant, private psychiatrist or psychologist. A smaller subset of patients receive longer-term care, typically those requiring ongoing treatment under the Mental Health Act or maintenance interventions such as ECT.
Continuity of care was supported through discharge planning, liaison with GPs and aged care services, and established re-referral pathways. This model reflects broader Australian public mental health service design, where specialist services operate alongside primary care and aged care to provide longitudinal support.
Consistent with this model, clinicians did not routinely accompany consumers to primary care appointments, instead relying on referral, documentation, and inter-service communication.
Interviews were conducted with small groups of AHCs; medical staff, psychiatrists, GP, and consumers were not included. The study intentionally focused on AHCs because they hold primary responsibility for routine physical health screening, documentation, and coordination of EW–related activities within community-based older adult mental health teams. Participants were registered allied health clinicians recruited using purposive and snowball sampling to ensure disciplinary representation. Eligibility criteria included current employment within the OAMHT and availability for face-to-face participation.
Data collection
Three semi-structured small-group interviews were conducted at participants’ workplace between January and February 2025. Interview questions were informed by the Theoretical Domains Framework (TDF) to explore implementation-relevant domains, including knowledge, professional identity, and environmental context. 7 Interviews were audio-recorded, transcribed verbatim, de-identified, and ranged from 30 to 44 min (mean 38 min), with transcripts returned to participants for verification.
Data analysis and reflexivity
Framework-based thematic analysis was used, guided by the TDF domains. Coding was completed using qualitative data analysis software Taguette. 8 Themes were developed independently and iteratively by two researchers. Reflexivity was maintained through journaling and peer debriefing to minimise bias. The study adhered to COREQ guidelines to ensure transparency and rigour. 9
A third researcher was available to resolve conflicts but was not required. No new themes emerged after the transcripts from three focus groups were analysed, suggesting thematic saturation and interviews ceased.
Results
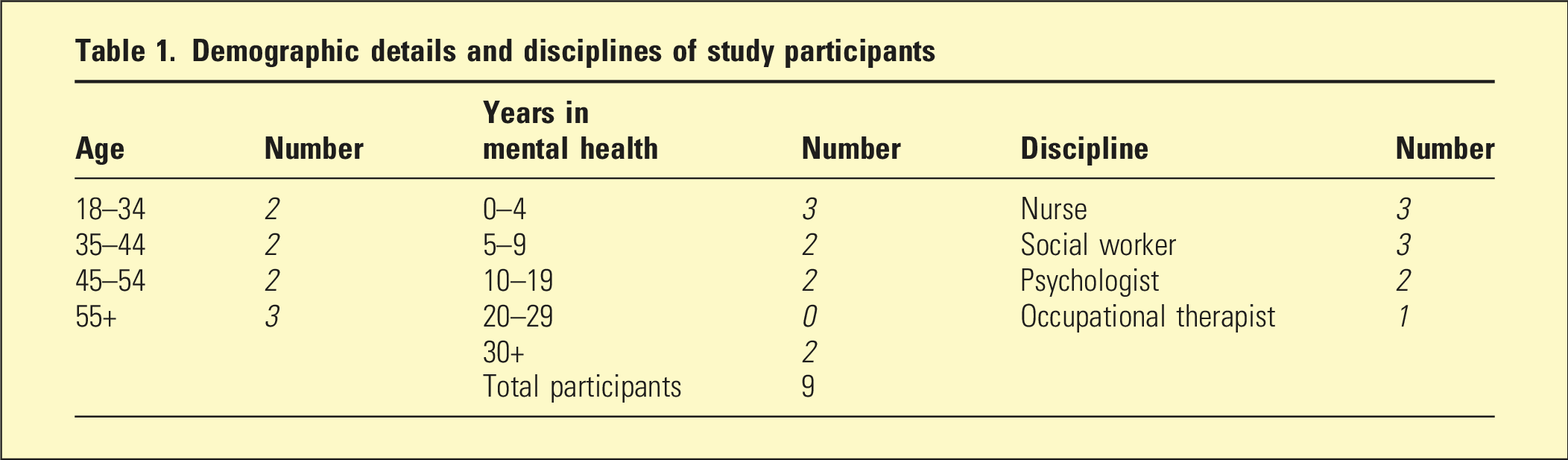
Participants
Demographic details and disciplines of study participants
Question 1: Understanding of the EW framework
Clinicians demonstrated a broad awareness of EW as a framework promoting holistic care but varied in their confidence and depth of understanding.
Holistic care: This was evidenced by views embracing the notion that mental health care necessarily encompasses both the physical and the mental: “I think to me, it would be along with their mental health, also considering what’s happening around in their physical status as well.” (RN)
This was seen as an important, intricate, and bidirectional relationship with consequences for overall health outcomes: “Physical health interacts with people’s mental health. So if you’re physically well, you’re more likely to be mentally well.” (SW)
Respondents recognised that physical needs were central to the EW framework, important, but often neglected in clinical care: “I think it’s…about trying to get people with mental illness to access the same level or quality of care that somebody else without mental illness would receive.” (CP)
Varied confidence in understanding EW: While most participants were aware of the overarching EW goal of improving physical health many reported only a superficial grasp of its specific principles, priority areas, or practical applications. “I really don’t know the depths of that EW project. I [only] know on a superficial level. None of us could really articulate what the priorities are.” (OT)
Discipline background influenced confidence and engagement. Nurses felt more comfortable monitoring physical health, while psychologists and social workers perceived it as outside their scope. “I think it depends on what discipline you come from. . . .for example Social Workers don’t get that same training as others, so it may not necessarily be as much on the radar to monitor physical health.” (SW)
There was uncertainty on how to operationalise the EW framework when collaborating with external services, particularly GPs and this hindered implementation. “It’s very hard to get that through to GP . . . . it’s still in the initial steps where we are navigating how to get the reports etc.” (RN)
Question 2: Challenges or barriers to implementation
Clinicians identified patient disengagement, clinician reluctance, and systemic constraints as key barriers. Older adults’ frailty, cognitive decline, and limited mobility often impeded participation in physical health promotion
Patient disengagement: This was seen as a major barrier. This was attributed to a range of factors, including the acuity of MI, competing psychosocial priorities, community access issues, and longstanding health behaviours and frailty. Respondents reported that many consumers simply did not perceive physical health as a priority, nor did they want to change. “A lot of our clients have depression and they can’t be bothered. They just want to lie in bed all day long and they don’t care whether they’re eating enough, whether they’re exercising.” (SW)
Some respondents felt EW was not appropriate to offer in all situations, for example, in palliative care. “How does it impact on their care when dementia’s virtually a palliative illness anyway? At what point does this stuff stop or is it meant to be in a tapered fashion, or is it everything or none?” (OT)
Finally, clinicians identified the social isolation, leading to a lack of follow up on screening outcomes or suggested interventions as opportunities lost. “I have a client base where because of their age, or because of less support around, they are not in connection with their GP. So they are doing telehealth and just going once.” (RN)
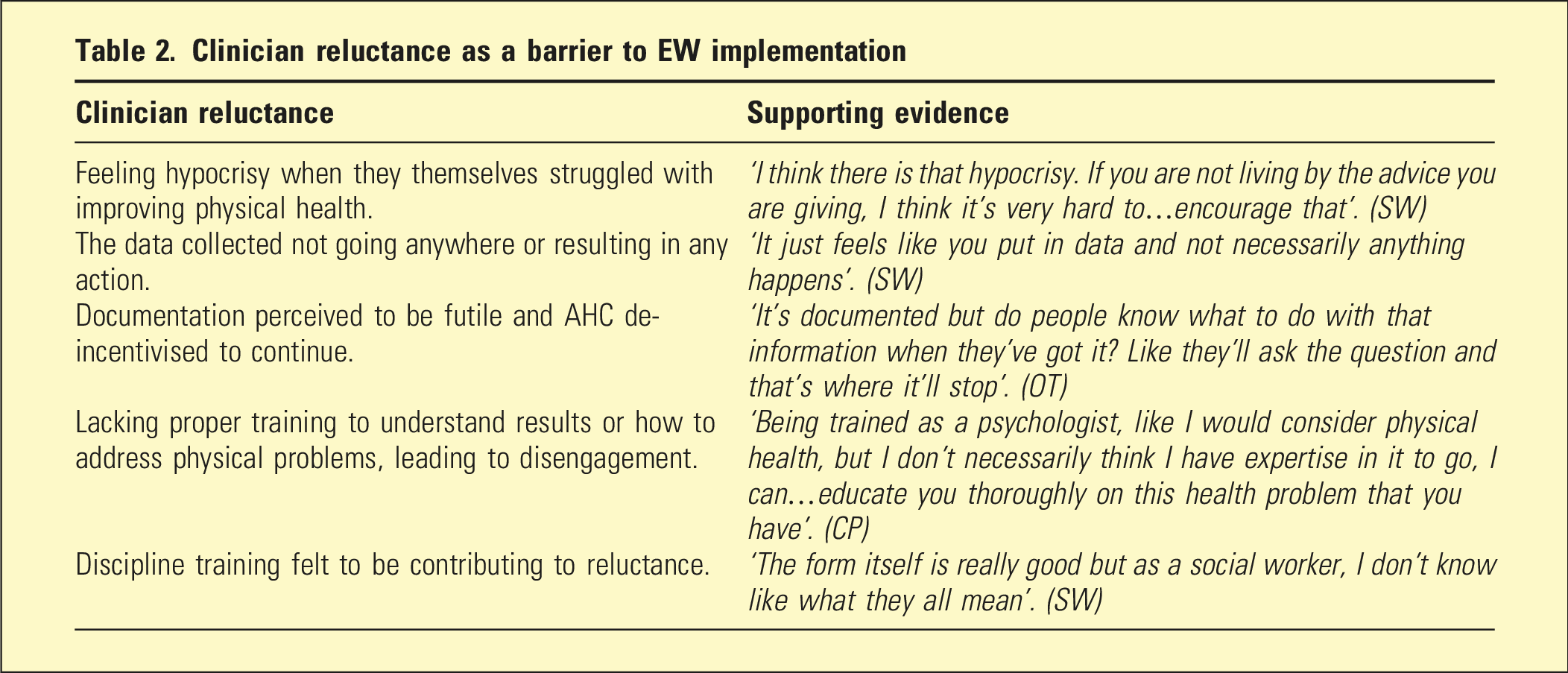
Clinician reluctance as a barrier to EW implementation
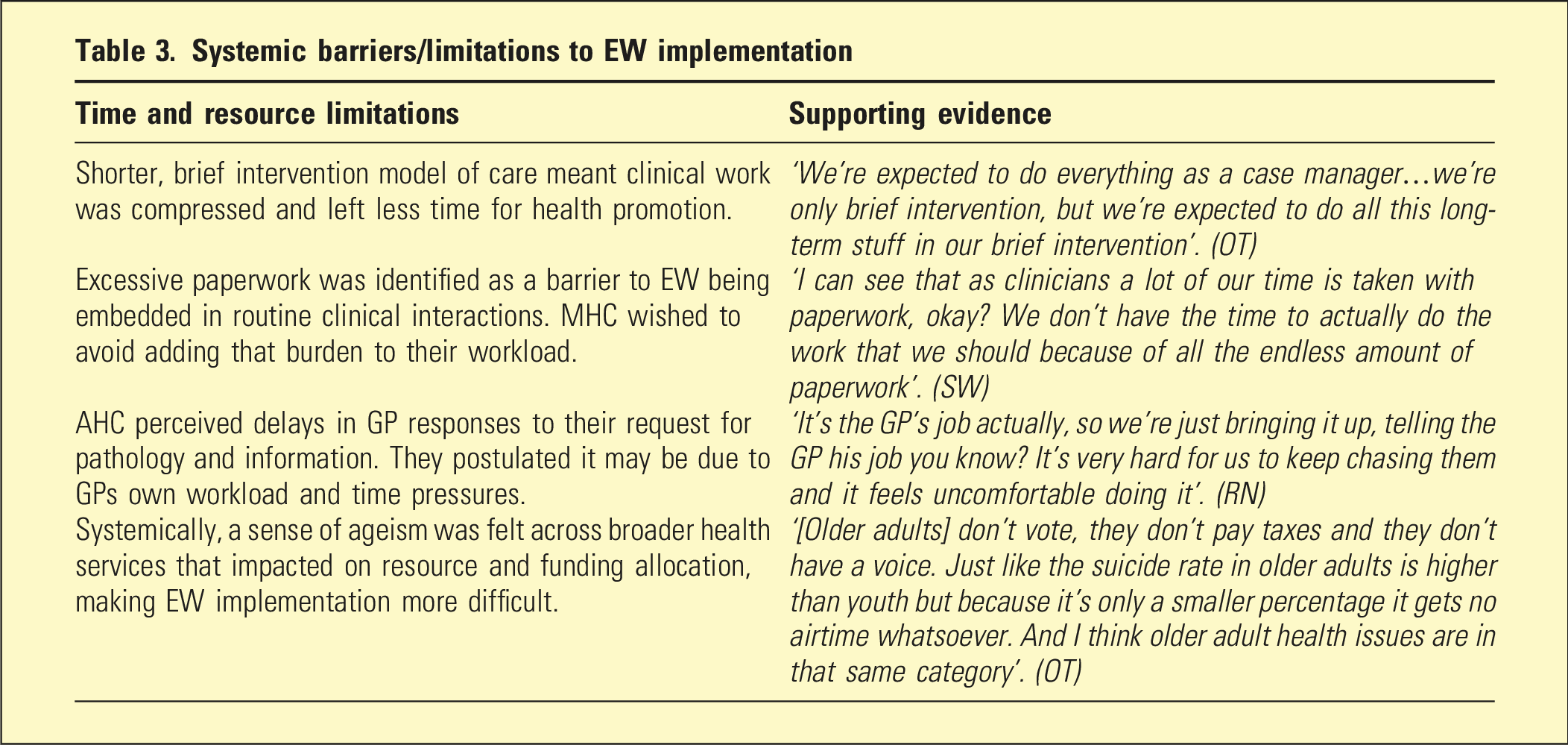
Systemic barriers/limitations to EW implementation
Question 3: Facilitators of implementation
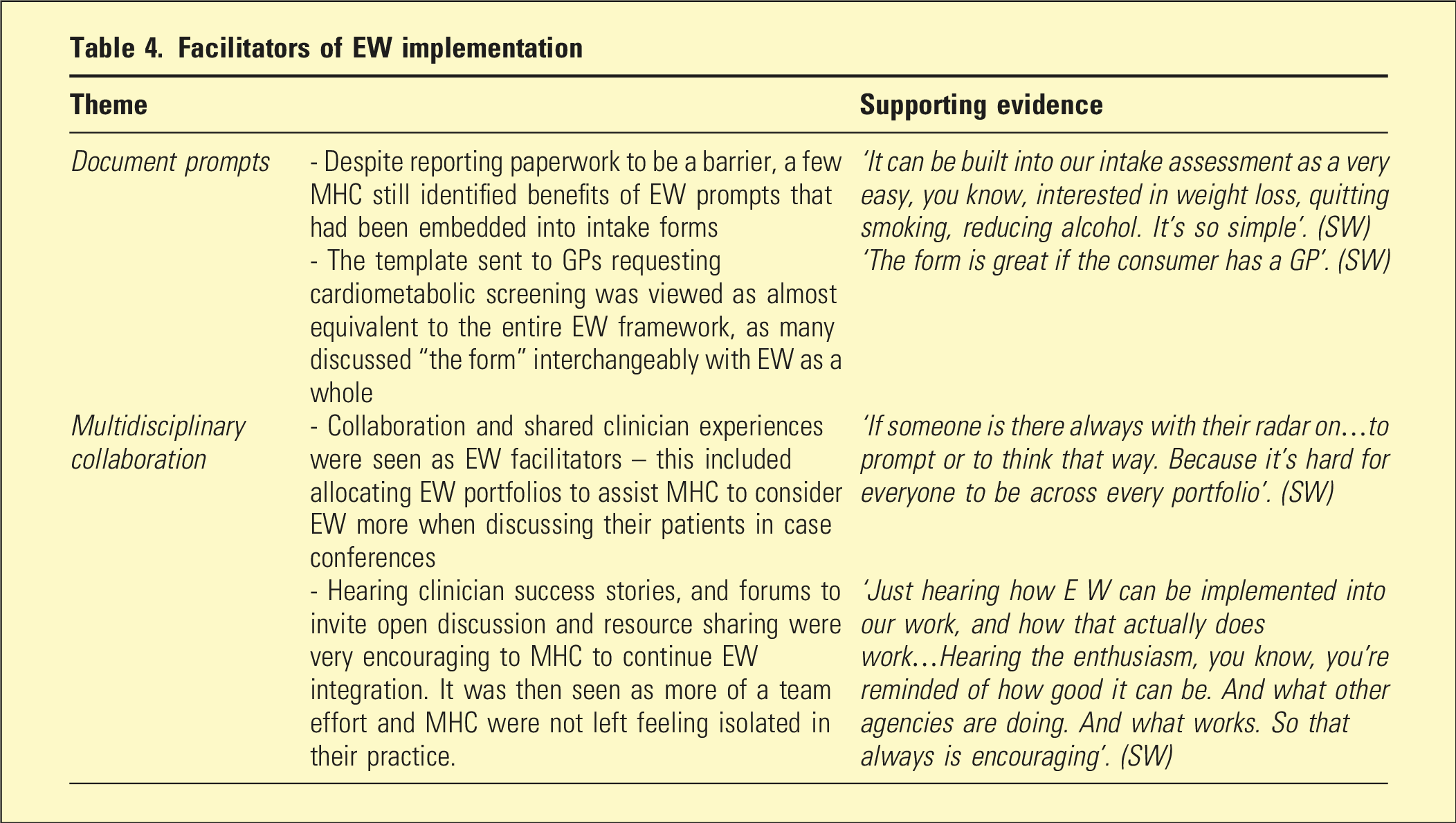
Facilitators of EW implementation
Question 4: Recommendations for improving implementation
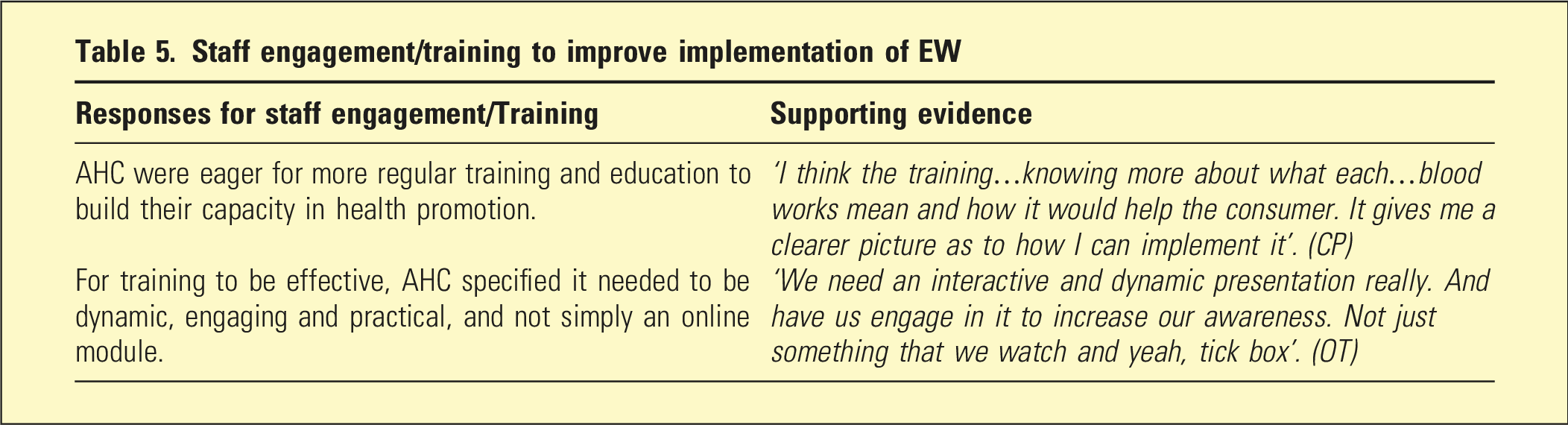
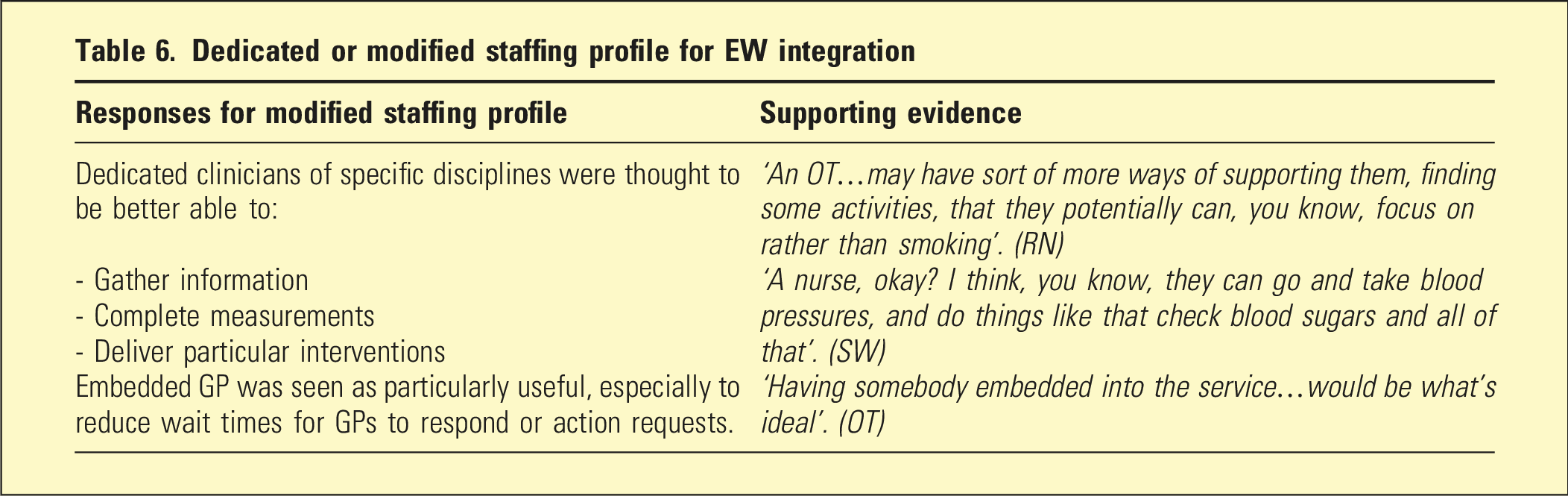
Clinicians proposed simplifying documentation, embedding clear referral pathways, and introducing regular, interactive staff training to strengthen capacity and confidence. Third, dedicated roles, such as embedded nurses or GP to support ongoing physical health interventions for older adults.
Simplifying documentation: Some AHC still described embedding of EW into mandatory simple paperwork as it was thought likely to benefit and assist patient engagement. “Keep it as simple as possible okay? We don’t need numerical figures …someone might say I might want to get my blood pressure under control. Then we talk about that. What are you doing? Okay, you’re on medication. What else can you do? You know, it’s not so much the figures.” (SW)
Clear and easy access to referral pathways and solutions following identification of issues was seen as crucial to successful EW integration and improved health promotion. “What would make it easier is…tick the box exercise of the person’s identifying needing this…having a very clear and easy pathway to the remedy.” (SW)
Staff engagement/training to improve implementation of EW
Dedicated or modified staffing profile for EW integration
Discussion
This study explored AHC perspectives on the EW initiative within community-based OAMHS. Key findings included variable clinician understanding of EW, perceived barriers to patient engagement in physical health promotion, discipline-based differences in confidence and role clarity, and system-level obstacles such as documentation burden and fragmented care pathways. Importantly, the BIM should not be interpreted as an absence of holistic or continuous care, but as a service configuration in which specialist input is time-limited and embedded within broader ongoing care delivered through primary care and aged care services. AHC also described age-related factors such as frailty, cognitive impairment, and multimorbidity that shaped the feasibility and perceived appropriateness of physical health promotion.
Understanding of EW framework
Clinicians showed variable understanding of the EW framework but generally recognised its focus on holistic, person-centred care and the impact of psychotropic medications on physical health. Inconsistent understanding contributed to uncertainty about professional responsibility for follow-up of physical health concerns—some viewed this as the GP’s role, while others saw it as a shared OAMHS responsibility. This ambiguity has been shown to weaken care coordination and hindered engagement with EW activities. 10
That medical leadership and articulation with geriatric services did not feature prominently in participants’ accounts should not be read as an absence of these practices, but as an indication that they were not experienced as central or visible components of EW implementation from the perspective of AHCs.
For some clinicians, exposure to EW occurred via local documents or (pre-EW ‘forms’) rather than through formal engagement with the framework, potentially contributing to an inadequate understanding of EW in practice.
Clinicians’ interpretations partly aligned with the EW ‘essential elements’ of person-centred care and progress monitoring, 4 yet the concept of integrated care and strong GP–MHS partnerships was less familiar.
Barriers, facilitators & suggested changes to EW
Allied health clinicians described EW implementation as shaped by interacting clinician, patient, and system-level factors that both constrained and enabled practice. Patient disengagement was commonly identified as a barrier, particularly in the context of frailty, cognitive impairment, reduced mobility, and social isolation. However, what clinicians perceived as disinterest often reflected structural barriers to participation rather than lack of motivation, 11 highlighting the need for age-sensitive, person-centred approaches that account for later-life complexity. 12
Clinician-level barriers included uncertainty regarding role boundaries, limited training in physical health, and discomfort initiating conversations perceived to fall outside disciplinary scope.13–15 These challenges were particularly evident among non-nursing disciplines and contributed to inconsistent engagement with EW activities. System-level constraints, including brief intervention models, time pressures, administrative burden, and fragmented communication with primary care further limited implementation.16,17 Challenges in communication were attributed to structural and funding arrangements rather than individual practitioner willingness. Documentation was frequently experienced as burdensome and of limited utility when not linked to clear follow-up pathways, reinforcing perceptions of futility. Within this model, implementation of the EW framework is dependent on effective coordination across service boundaries, particularly with GPs who play a central role in ongoing physical health care. As such, EW enactment in brief intervention settings relies less on direct provision and more on identification, referral, and follow-up within integrated care pathways.
At the same time, clinicians identified several enablers that mitigated these challenges. Embedded documentation prompts were viewed as useful when they normalised physical health conversations and provided structure, even though paperwork was generally regarded as onerous.18,19 Multidisciplinary collaboration, including shared discussion of cases and allocation of EW-related portfolios, supported collective responsibility and reduced individual clinician burden.20,21 Informal peer learning and exposure to successful examples of EW implementation increased confidence and sustained engagement.
Participants emphasised that effective implementation depended less on individual clinician motivation and more on practical system-level supports. 22 Suggested improvements included simplifying documentation, embedding clear referral pathways following screening, and providing interactive, discipline-relevant training rather than generic education. 23 Dedicated or embedded roles – such as nurses or GP – were viewed as particularly valuable for strengthening coordination, ensuring follow-up, and reducing reliance on individual clinician initiative.24–26 Together, these findings indicate that EW implementation in older adult mental health services is contingent on aligning workforce roles, documentation processes, and primary care partnerships to the realities of ageing-related complexity.
Age-related considerations shaping EW implementation
Clinicians identified frailty, cognitive impairment, multimorbidity, and reduced mobility as central to EW enactment. Unlike working-age contexts, where EW often emphasises lifestyle modification and long-term risk reduction, participants described the need to recalibrate goals toward maintenance, comfort, and harm minimisation. This was particularly evident in dementia, advanced functional decline, and palliative trajectories, where clinicians questioned whether standard EW expectations aligned with consumers’ goals of care.
Social isolation and limited informal supports further constrained implementation, as follow-up of identified physical health needs was often impeded by reduced access to primary care, transport limitations, and fragmented aged-care pathways. These findings indicate that EW implementation in older adult services requires explicit age-sensitive adaptation, rather than direct transfer of models developed for working-age populations.
Clinical and workforce implications for EW implementation
While clinicians across disciplines supported EW’s intent, confidence in addressing physical health varied according to professional training and perceived scope of practice. Role ambiguity regarding responsibility for physical health follow-up remained a key barrier, with uncertainty over shared accountability between mental health services and primary care.
Participants emphasised that effective implementation depended on organisational, rather than individual, solutions. Streamlined documentation, integrated EMRS, clear referral pathways, practical discipline-relevant training, and access to dedicated or embedded physical health roles, particularly nurses or GPs, were viewed as critical to supporting consistent EW implementation within brief intervention models.
Strengths and limitations
Interviews were conducted by the principal investigator, a senior clinician known to participants. While this familiarity may have facilitated openness, it also introduced potential social desirability and investigator bias. Reflexive journaling and peer debriefing were used to mitigate these influences, though they cannot be fully eliminated.
The small, all-female, single-site sample was appropriate for in-depth qualitative inquiry but limits transferability to other settings or clinician groups. Perspectives may differ in services with greater gender, cultural, or professional diversity. Medical staff were not included, and their perspectives on medication management and cross-sector collaboration may complement these findings. Also, AHC personal health experiences, which may vary with age, were not explicitly explored and may represent an additional influence that warrants further investigation. Future research incorporating GPs could provide a more comprehensive understanding of multidisciplinary implementation of EW. The findings should also be interpreted in the context of a brief intervention service model, which may shape clinician experiences of continuity, coordination, and role responsibility compared with long-term case management services.
Conclusion
This study provides insight into AHC perspectives on implementing the EW framework within community-based OAMHS. While clinicians supported the principles of holistic, person-centred care, inconsistent understanding of EW and role ambiguity limited confidence in addressing physical health needs. Implementation was further constrained by limited training, administrative burden, and the complexities associated with frailty, multimorbidity, and cognitive impairment.
Importantly, EW implementation in OAMHS differed from that described in working-age populations, requiring adaptation to ageing-related contexts and shifting goals of care rather than a primary focus on lifestyle modification and long-term risk reduction. These findings highlight a range of approaches needed for age-sensitive implementation.
Supplemental material
Supplemental material - Understanding the Equally Well Framework in Older Adult Community Mental Health Services: A Qualitative Study of Allied Health Clinician Perspectives
Supplemental material for Understanding the Equally Well Framework in Older Adult Community Mental Health Services: A Qualitative Study of Allied Health Clinician Perspectives by E Wong, S Aradhye, S Innes in Australasian Psychiatry
Footnotes
Acknowledgements
We would like to thank the participants who generously gave of their time and made this project possible.
Ethical considerations
Ethics approval was obtained from the local health service research committee prior to commencing (reference number LR24-062-113529).
Author contributions
EW: design, method, search, data extraction and analysis, writeup.
SA: concept, design, methodology, analysis, write-up.
SI: data analysis, write-up.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.