
Abstract
A retrospective study was performed to compare the treatment regimens in feedlot cattle that died with bovine respiratory disease (BRD) to the antimicrobial susceptibility patterns of the microorganisms isolated from lungs. Forty-three cattle submitted by the Willard Sparks Beef Research Center (WSBRC) to the Oklahoma Animal Disease Diagnostic Laboratory for postmortem examination during 2007 had bronchopneumonia (acute = 16, subacute = 5, or chronic = 22). Lungs from cattle were cultured aerobically (40 cattle) and for Mycoplasma spp. (34 cattle). Susceptibility panels were performed. At least 1 BRD pathogen (Mannheimia haemolytica, Pasteurella multocida, Histophilus somni, Mycoplasma bovis, or Arcanobacterium pyogenes) was isolated from 39 cattle, and 77% (30/39) had multiple organisms recovered. Mycoplasmal infections were common (25/34) and a major component of mixed infections (24/25). The majority (60%) of the M. haemolytica, P. multocida, and H. somni isolates were resistant to tetracycline. Most of the H. somni isolates (67%) were susceptible to tilmicosin (Ti), enrofloxacin (En), ceftiofur (Ce), and florfenicol, despite extensive treatment with Ti, En, and Ce (75% of isolates were from cattle that received each antimicrobial once). Most of the M. haemolytica (65%) and P. multocida (79%) isolates were susceptible to En and Ce, despite antemortem treatment of cattle with these antimicrobials. Hence, the current study reports a discrepancy between the antemortem treatment of clinical BRD and the susceptibility patterns of the bacteria isolated from lungs postmortem. Based on these findings, factors other than antimicrobial resistance are playing a role in the death of feedlot cattle with BRD.
Introduction
Bovine respiratory disease (BRD) is the most economically important disease of beef cattle, 12 and accounts for 75% of the morbidity and over 50% of the mortality in feedlot cattle. 12 In feedlots with high morbidity and mortality due to BRD, prevention and treatment of animals can cost over $3 billion annually. 20 Additionally, economic losses are incurred due to reduced animal performance, increased days on feed, lower carcass weights, lower quality grades, and increased human labor.2,4,17
Bovine respiratory disease in feedlot cattle is characterized by severe bronchopneumonia and/or pleuropneumonia, 13 and is considered a multifactorial disease in which at least 1 bacterial organism is typically cultured from affected animals.3,11,18 Risk factors for the development of BRD include previous or concurrent respiratory viral infection, poor nutrition, and poor management factors, which can lead to immune suppression. Poor management factors include overcrowding, poorly timed weaning, poor shipping conditions, and exposure to harsh environmental conditions.9,10,16,19
The most common bacteria isolated from the lungs of animals diagnosed with BRD are Mannheimia haemolytica, Pasteurella multocida, Histophilus somni, Mycoplasma bovis, and Arcanobacterium pyogenes.5,8,15,19,21 There are many different viruses that may contribute to the development of bacterial bronchopneumonia, including Bovine herpesvirus 1 and 4, Bovine parainfluenza virus 3, Bovine respiratory syncytial virus, and Bovine viral diarrhea virus.1,14
Antimicrobial treatment to reduce mortality associated with BRD can be challenging. In a previous study of bacteria cultured at the Oklahoma Animal Disease Diagnostic Laboratory, the percentage of M. haemolytica isolates susceptible to tilmicosin and florfenicol significantly declined between 1994 and 2002, while the percentage susceptible to ceftiofur, enrofloxacin, and trimethoprim–sulfamethoxazole remained stable. 21 The percentage of P. multocida isolates susceptible to tilmicosin, florfenicol, trimethoprim–sulfamethoxazole, and tetracycline also declined significantly, while the percentage susceptible to ceftiofur and enrofloxacin remained stable. In that previous study, H. somni isolates remained susceptible to all antimicrobials tested. 21 The findings suggested that several of the currently available treatments should be effective in treating the bacterial component of BRD; however, the clinical impression of feedlot managers and veterinarians is that feedlot cattle continue to experience high mortality despite treatment.
Many studies have looked at the efficacy of different treatments and treatment protocols.8,13,21 The purpose of the current study was to determine which organisms were isolated from the lungs of cattle in a feedlot in Oklahoma, to determine the susceptibility patterns of these organisms, and to compare these patterns to the medicinal treatments given prior to death.
Materials and methods
Cases
The UVIS database at the Oklahoma Animal Disease Diagnostic Laboratory (OADDL) was searched for animals that died at the Oklahoma State University Willard Sparks Beef Research Center (WSBRC) in 2007. The final reports from each animal were reviewed, and the following information was recorded: final pathologic diagnosis, chronicity of the pathologic lesions, bacterial organisms isolated, and susceptibility patterns of the bacterial organisms.
Briefly, representative sections of lung were collected on the postmortem floor, aseptically sampled, and routinely streaked on 5% sheep blood agar and MacConkey agar plates. The plates were incubated at 37ºC and 5% CO2 for 12–24 hr. Isolated bacteria were identified using standard techniques, including Gram stains, cytochrome oxidase tests, catalase tests, and Gram-negative/positive identification panels. a At the discretion of the pathologist, a proportion of cases were also cultured for Mycoplasma spp. as previously described. 22 Susceptibility of the bacterial isolates was determined using susceptibility plates b according to guidelines outlined by the Clinical and Laboratory Standards Institute (CLSI). 7 The plate included the following antimicrobials: ceftiofur, tiamulin, chlortetracycline, gentamicin, florfenicol, oxytetracycline, penicillin, ampicillin, danofloxacin, sulfadimethoxine, neomycin, trimethoprim–sulfamethoxazole, spectinomycin, tylosin tartrate, tulathromycin, tilmicosin, clindamycin, and enrofloxacin. Mycoplasma bovis and A. pyogenes isolates were not susceptibility tested due to lack of standardized methods and CLSI recommendations at the time of the present study. 7
For each case, the live animal records at the WSBRC were reviewed, and all the antimicrobial treatment information prior to death was recorded. Cattle were selected for treatment based on clinical signs of BRD. At the first sign of clinical BRD, cattle were given 10 mg/kg body weight (BW) of tilmicosin c subcutaneously (Tx1). If clinical signs continued, the initial treatment of tilmicosin was followed by 10 mg/kg BW of enrofloxacin d given subcutaneously (Tx2). Upon progression of clinical signs over time, affected cattle were given an additional 2.2 mg/kg BW of ceftiofur e subcutaneously (Tx3). Statistical analysis was performed using EpiCalc, f using a 95% confidence interval. A p-value of less than 0.01 was considered significant.
Results
A total of 49 cattle were submitted by WSBRC for necropsy, of which 43 had pneumonia. Cattle received antemortem treatments as follows: no treatment = 4, Tx1 = 7, Tx2 = 5, and Tx3 = 27. The chronicity of the bronchopneumonia was categorized as follows: acute = 16, subacute = 5, and chronic = 22 cattle. The number of treatments given compared to the chronicity of the bronchopneumonia is presented in Table 1. Cattle with subacute or chronic bronchopneumonia were more likely to have received 3 treatments than cattle with acute pneumonia (χ 2 = 8.81, p = 0.003). A fraction (5/16, 31%) of cattle with acute bronchopneumonia were treated 3 times.
The number of cattle with acute, subacute, or chronic bronchopneumonia by pathology compared to the number of antemortem treatments given.*
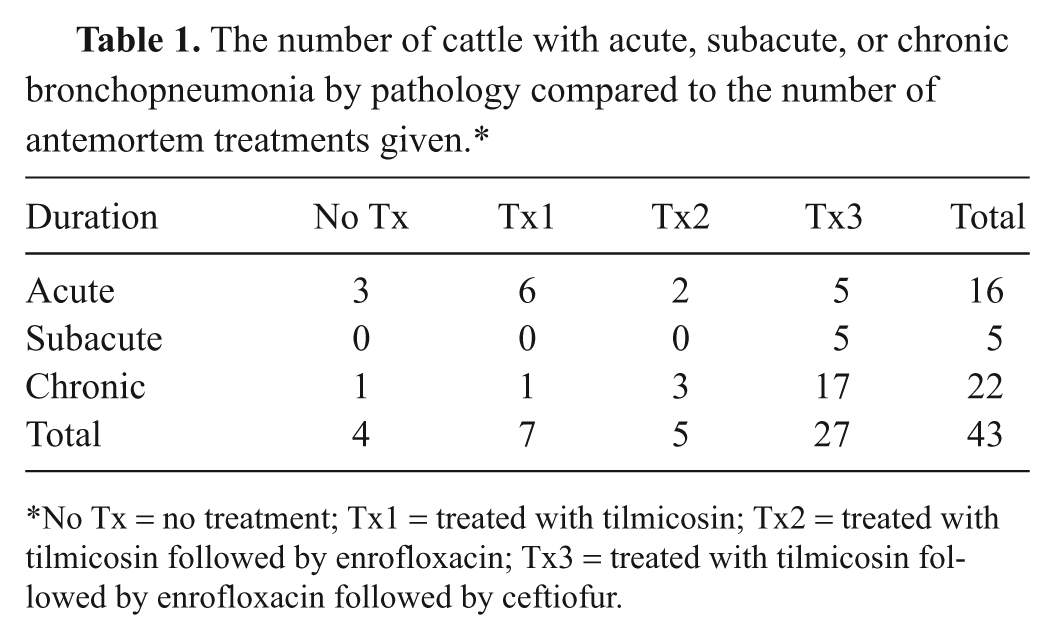
No Tx = no treatment; Tx1 = treated with tilmicosin; Tx2 = treated with tilmicosin followed by enrofloxacin; Tx3 = treated with tilmicosin followed by enrofloxacin followed by ceftiofur.
The lungs from 40 cattle were cultured aerobically with 34 of these lungs also cultured for Mycoplasma spp. The organisms isolated are listed in Table 2 and presented graphically in Figure 1. Mixed infections were the most common (30/40, 75%), and M. haemolytica was the most likely organism to be cultured in mixed infections (18/30, 60%). Mycoplasma bovis was cultured in a high proportion of cases (25/34, 74%) and was often cultured as a component of a mixed infection (24/25, 96%).
Organisms cultured from 40 cattle with bronchopneumonia during 2007.*
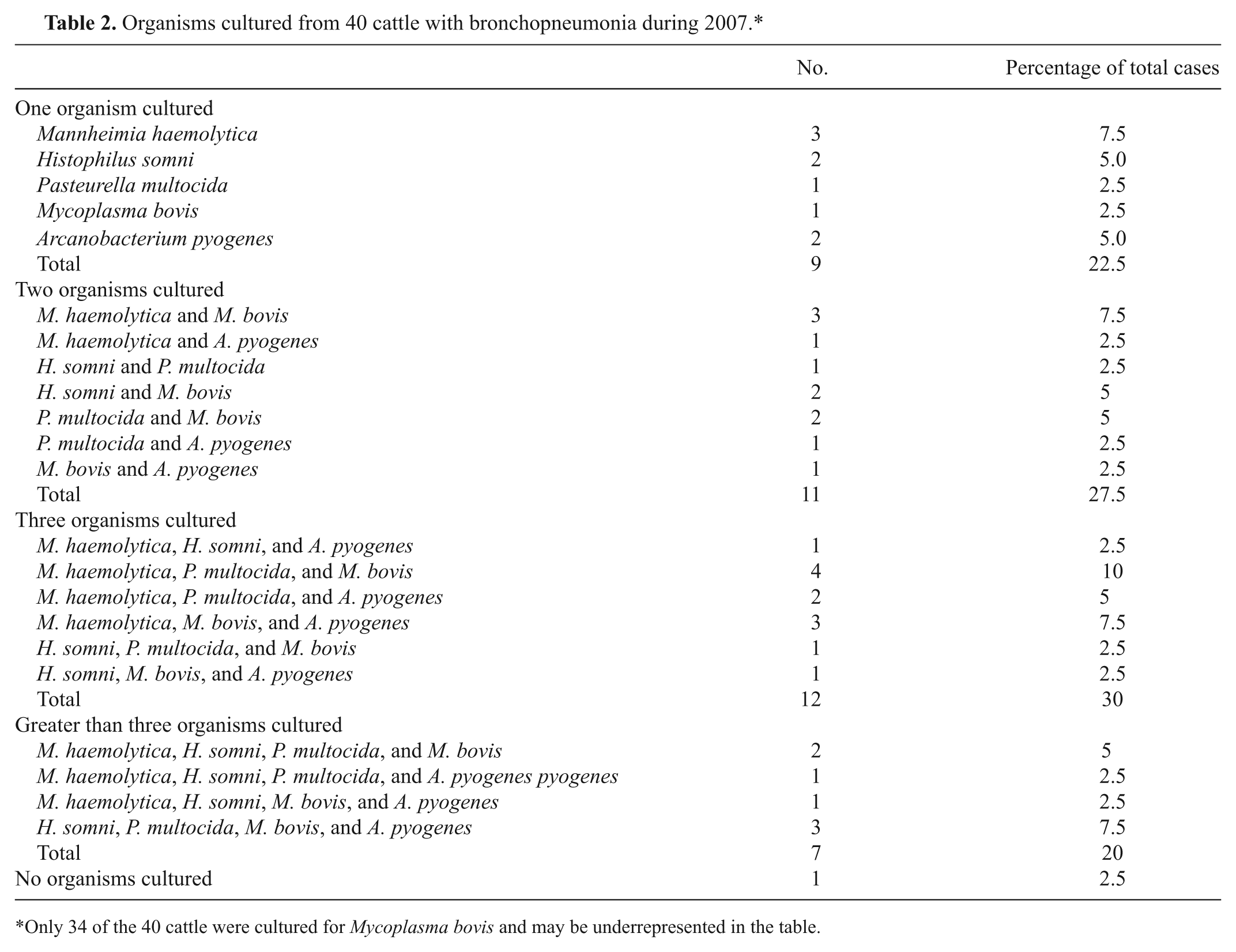
Only 34 of the 40 cattle were cultured for Mycoplasma bovis and may be underrepresented in the table.

Number of bacterial isolates from the lungs of feedlot cattle with bronchopneumonia cultured aerobically on blood agar plates (40) and for Mycoplasma spp. (34).
Susceptibility patterns were performed on 43 bacterial isolates (M. haemolytica = 14, H. somni = 12, P. multocida = 14), and the susceptibility patterns of the organisms for tilmicosin, enrofloxacin, ceftiofur, tetracycline, and florfenicol are presented in Table 3. One H. somni isolate was not tested for susceptibility to ceftiofur and tetracycline. The proportion of isolates susceptible to the antimicrobials tested is presented in Figure 2.
Susceptibility patterns for 43 bacterial organisms isolated from 40 feedlot cattle with bronchopneumonia during 2007.*

S = susceptible; I = intermediate; R = resistant. Susceptibility of 1 H. somni isolate to ceftiofur and tetracycline was not performed.
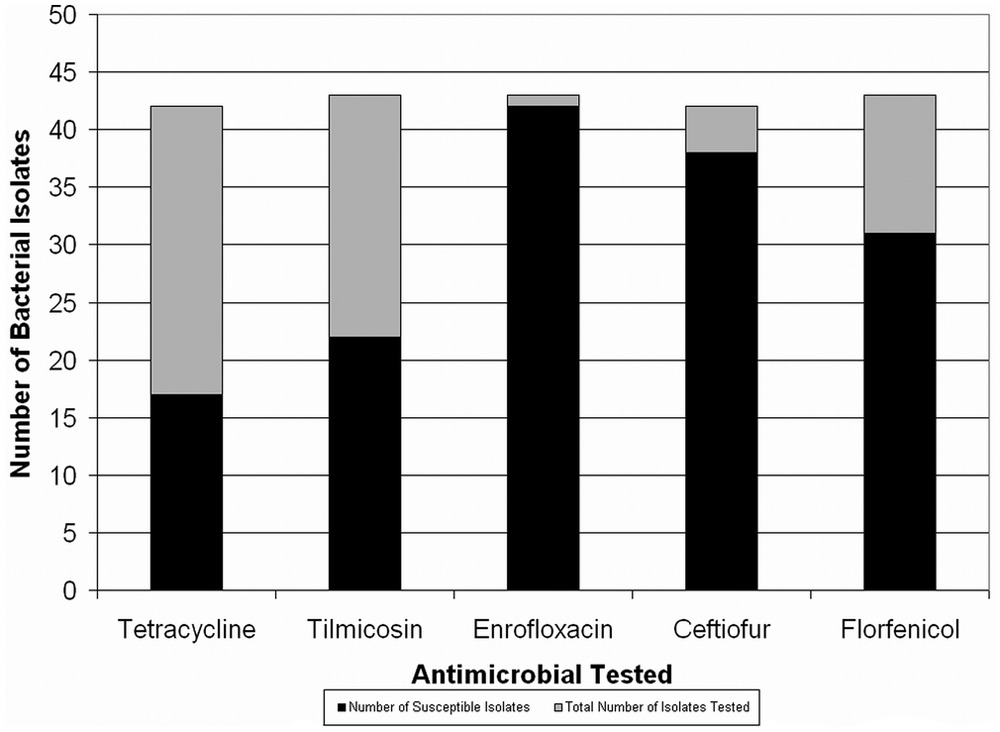
Number of 43 bacterial isolates (Mannheimia haemolytica [17], Histophilus somni [14], and Pasteurella multocida [12]) susceptible to the 5 antimicrobials tested. Results on susceptibility testing for tetracycline or ceftiofur for 1 H. somni isolate were not available.
Only a small proportion of isolates were susceptible to tetracycline (17/42, 40%). Just over half of the isolates were sensitive to tilmicosin (22/43, 51%). A large number of isolates were susceptible to enrofloxacin (42/43, 98%), ceftiofur (38/42, 90%), and florfenicol (31/43, 72%).
The susceptibility patterns are compared to the number of treatments by bacterial organism isolated in Table 4. Most of the H. somni isolates were susceptible to the antemortem treatments given. Most of the M. haemolytica and P. multocida isolates were susceptible to enrofloxacin and ceftiofur, both of which were given antemortem to cattle that died from these infections.
Comparison of antemortem treatments with antibiotic sensitivities for Mannheimia haemolytica (M), Histophilus somni (H), and Pasteurella multocida (P) isolates from the lungs of 17 feedlot cattle with bronchopneumonia during 2007.*
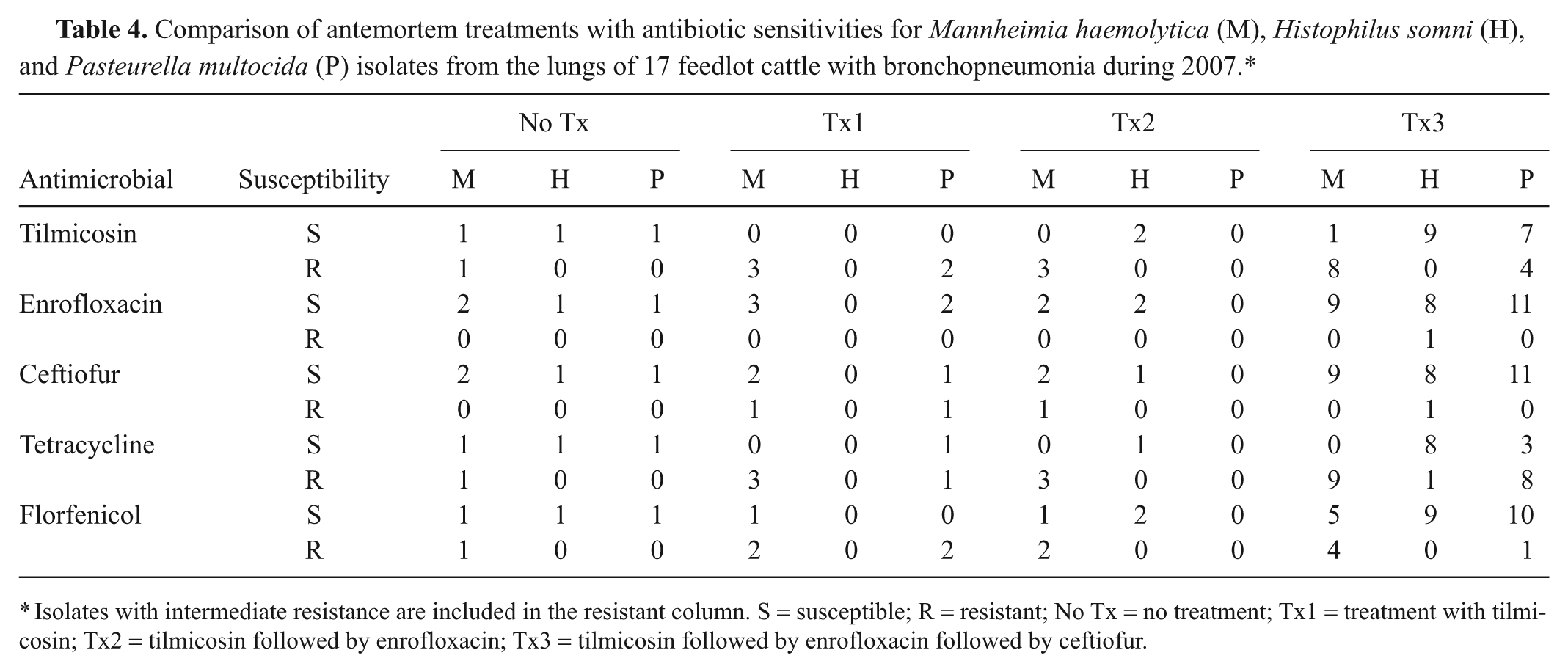
Isolates with intermediate resistance are included in the resistant column. S = susceptible; R = resistant; No Tx = no treatment; Tx1 = treatment with tilmicosin; Tx2 = tilmicosin followed by enrofloxacin; Tx3 = tilmicosin followed by enrofloxacin followed by ceftiofur.
Discussion
Chronic bronchopneumonia was common in the cattle in the current study and reinforces earlier findings. 14 In the present study, cattle with chronic bronchopneumonia were more likely to have received multiple treatments, suggesting a lack of response to initial antimicrobial therapy. Previous studies have suggested that antibacterial resistance plays a strong role in the development of terminal bronchopneumonia in cattle.3,6,21 However, the results of the present study suggest that other factors, in addition to antimicrobial resistance, play a role in the development of antimicrobial unresponsive, terminal bronchopneumonia in cattle.
Interestingly, some of the cattle with acute bronchopneumonia had been treated several times. It is possible that the pathologic categorization of the bronchopneumonia was incorrect. It is also possible that during the initial treatment, the cattle had respiratory disease unrelated to bacterial infection but then developed secondary bacterial infections later.
The organisms isolated from the cattle in the current study included M. haemolytica, P. multocida, H. somni, M. bovis, and A. pyogenes. Mixed infections, often M. haemolytica and/ or M. bovis, were the most common. The findings are similar to previous reports of BRD in feedlot cattle. 21 Not surprisingly, 60% of the bacterial isolates were resistant to tetracycline, which is comparable to the 56% resistance rate reported in 2002. 21
The resistance to tilmicosin was widely variable among the different species of bacterial isolates tested. Of the M. haemolytica isolates tested, 88% showed intermediate resistance or resistance to tilmicosin. This is considerably higher than the 21% of M. haemolytica isolates reported resistant to tilmicosin in 2002. 21 Conversely, none of the H. somni isolates were resistant to tilmicosin. This is similar to a previous report, which found only 4% of H. somni isolates resistant to tilmicosin in 2002. 21 Of the P. multocida isolates, 43% were resistant to tilmicosin, which was slightly higher than the 27% of isolates reported resistant in 2002. 21
Seventy-two percent of bacterial isolates in the current study were susceptible to florfenicol, which is considerably lower than the 90% of isolates susceptible reported in 2002, in which a decline in susceptibility was already noted. 21 Most of the bacterial isolates were susceptible to enrofloxacin (98%) and ceftiofur (90%), which is comparable to reports in 2002 (enrofloxacin = 98%, ceftiofur = 97%). 21
Based on the antimicrobial susceptibility tests alone, most of the cattle with H. somni should have responded to antemortem treatments given. Similarly, most of the cattle with M. haemolytica and P. multocida isolates should have responded to antemortem treatments of enrofloxacin and ceftiofur. The isolation of organisms that were susceptible to the antimicrobials given to cattle with severe terminal bronchopneumonia is perplexing.
Several factors may play a role in the inefficacy of antimicrobials in the present study. It is possible that the antimicrobial may not have reached the site of infection. It is also possible that the antimicrobial reached the site of infection but was either inactivated or otherwise ineffective once at the site. Timing of antimicrobial therapy is also likely critical. It is possible that the cattle that were more severely affected at the time of first treatment were less likely to respond to treatment despite susceptibility of the organism to the antimicrobial given or that the treatment was not given long enough. Additional studies exploring the concentrations and activity of antimicrobials at different sites within pneumonic lungs of cattle are required to explore these possibilities.
Overall, the current study shows that susceptibility patterns of the bacterial organisms isolated from the lungs of feedlot cattle that died with bronchopneumonia may not always relate to the antimicrobial treatments administered prior to death. Based on the findings, factors other than antimicrobial resistance may be influencing the death of feedlot cattle with clinical BRD.
Footnotes
Acknowledgements
The authors would like to thank Ben Holland, staff at the Oklahoma State University Willard Sparks Beef Research Center, and the staff at the Oklahoma Animal Disease Diagnostic Laboratory.
a.
bioMérieux, St. Louis, MO.
b.
Bovine/Porcine TREK Sensititre Plate BOPO6F, TREK Diagnostic Systems Inc., Cleveland, OH.
c.
Micotil® 300, Elanco Animal Health, Indianapolis, IN.
d.
Baytril® 100, Bayer Healthcare LLC, Animal Health Division, Shawnee Mission, KS.
e.
Excenel®, Pfizer Inc., New York, NY.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
This study was completed through the Oklahoma State University’s Veterinary Research Scholars Program. This program is supported by competitive grants from the National Institutes of Health, the Merck-Merial Veterinary Scholars Program, the Morris Animal Foundation, and by the Center for Veterinary Health Sciences at Oklahoma State University.