
Abstract
A large renal mass was identified by ultrasound during a regular health check on an intact adult female chimpanzee (Pan troglodytes). Cytology revealed a neoplastic population of clusters of polygonal cells with distinctive pink, granular cytoplasm. The primary differentials were oncocytoma and renal chromophobe cell carcinoma. The mass was surgically resected and grossly it effaced >75% of the right kidney and had a central scar. Histology confirmed an oncocytoma based on characteristic morphology, diffuse expression of cKIT (CD117), and limited expression of CK7, both assessed via immunohistochemistry. Transmission electron microscopy identified the granular component of the cytoplasm as mitochondria. Renal oncocytoma has not been reported previously in a great ape, to our knowledge. Our case appears nearly identical to the frequently reported and well-characterized human counterpart.
During a routine health check of a 47-kg, intact adult female chimpanzee (Pan troglodytes), a large, right renal mass was incidentally documented on both ultrasound and palpation. A percutaneous, ultrasound-guided fine-needle aspirate of the mass performed during the health check was very cellular, consisting of numerous large polygonal cells present singly and in variably sized cohesive clusters (Fig. 1A). Cells had low nuclear:cytoplasmic ratios and round nuclei with finely stippled chromatin and sometimes single, small, inconspicuous nucleoli. Anisokaryosis was mild to moderate with occasional karyomegalic variants. Cells had moderate-to-large volumes of pale-blue to gray cytoplasm, with a subpopulation with distinctive pink, granular cytoplasm, and with rare round pink inclusions (Fig. 1B). Mitotic figures were rare. The primary differentials were renal oncocytoma and renal chromophobe cell carcinoma.
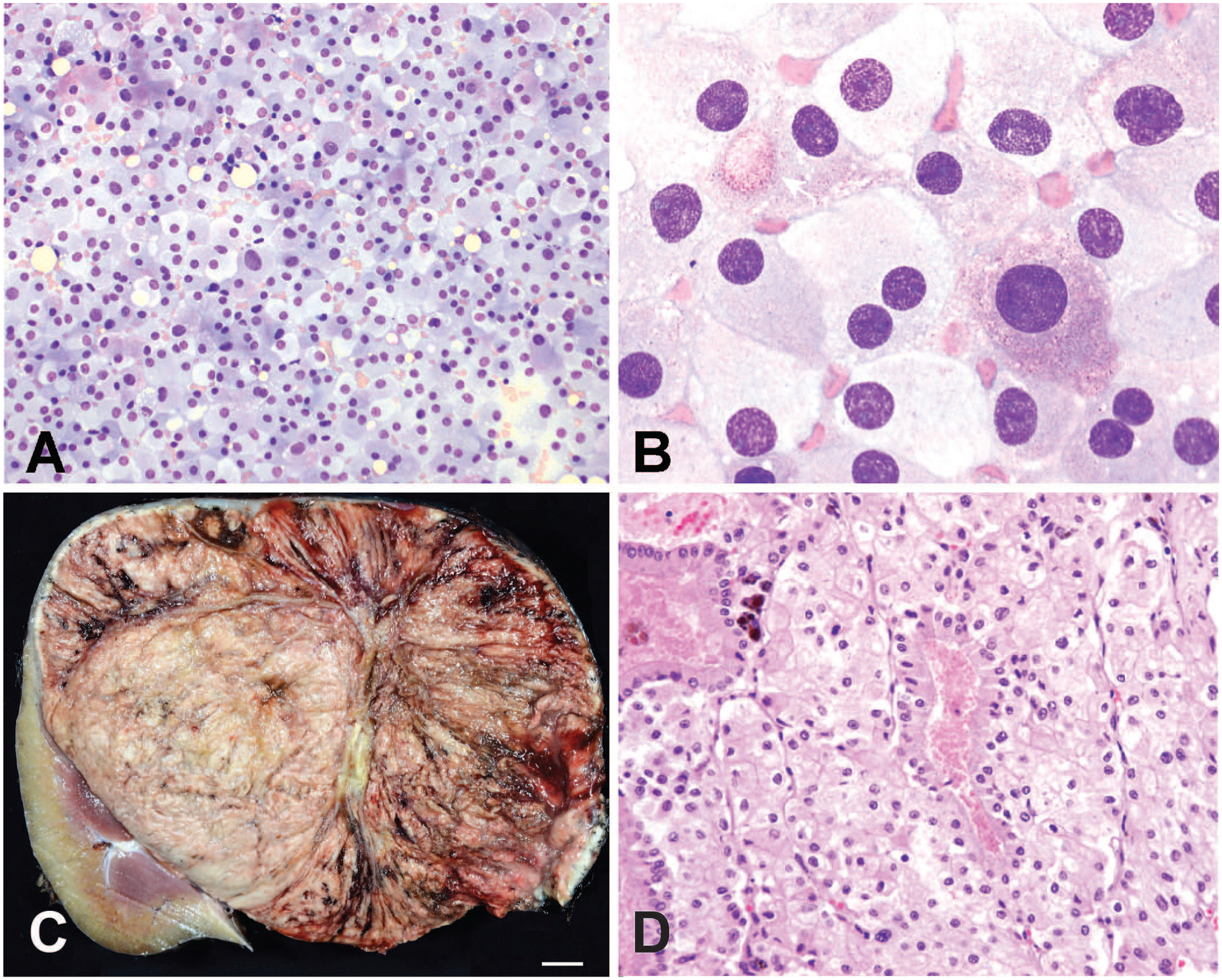
Cytology, gross, and histopathology of a renal oncocytoma in a chimpanzee.
The right kidney and mass (14.8 × 11.8 × 11.4 cm; 1.22 kg) were surgically removed by total nephrectomy (Fig. 1C). The mass was completely encapsulated and contained within the renal capsule. On section, the mass nearly extended to the periphery of the kidney, effacing and replacing up to 80% of the normal renal parenchyma, and sparing a small portion of normal kidney at one pole. On section, a central band of fibrous tissue, interpreted as a scar, separated neoplastic lobules with variable appearance. A single, bulging, tan, relatively homogeneous nodule comprising one-third of the mass was located eccentrically between the scar and normal renal parenchyma. The remaining two-thirds of the neoplasm was composed of tan tissue with red tracts of blood and vessels radiating from the central scar (Fig. 1C). Although not specific for oncocytomas, a central scar has been well-documented as a consistent gross feature of oncocytomas.4,13,15
Histologically, the encapsulated, nodular, expansile, densely cellular, homogeneous mass was comprised of neoplastic cells organized in variably sized lobules, nests, and tubules, delineated by a delicate fibrovascular network (Fig. 1D), irrespective of the gross sampling location. Rare tubules lined by columnar epithelium with a brush border were interspersed throughout the neoplasm. Neoplastic cells were polygonal with distinct cell borders, and abundant, eosinophilic granular cytoplasm forming a chicken-wire appearance (Fig. 1D). Nuclei were round with peripheralized chromatin and generally indistinct nucleoli. There were occasional multinucleate cells with up to 4 nuclei. Anisocytosis was mild, and anisokaryosis was mild to moderate. There was 1 mitotic figure in 2.37 mm2. The mass was regionally interrupted by vessels and linear tracts of hemorrhage that were visible grossly. Hemosiderophages were scattered throughout the mass. Tubules in the normal kidney immediately surrounding the mass were compressed and replaced by fibrous connective tissue. Glomerular changes were inconsistent and ranged from segmentally thickened glomerular capsules and sclerosis to complete obsolescence. The mass extended to the 7.5-µm thick renal capsule. Differential diagnoses included an oncocytoma and renal chromophobe cell carcinoma.
The immunohistochemical (IHC) profile assisted diagnosis of an oncocytoma, while ruling out a renal chromophobe cell carcinoma. Neoplastic cells had moderate-to-strong, cytoplasmic and membranous cKIT (CD117) immunoreactivity throughout the mass (Fig. 2A). Fewer than 1% of the neoplastic cells had moderate cytoplasmic CK7 immunoreactivity (Fig. 2B). Collecting ducts in non-neoplastic renal tissue had strong cytoplasmic immunoreactivity to CK7 (data not shown). In humans, malignant transformation of an oncocytoma to a renal chromophobe cell carcinoma is generally coupled with the acquisition of marked CK7 expression.15,16 Although complete lack of CK7 expression is regarded to be less supportive of an oncocytoma, rare (<5%), random neoplastic cell CK7 immunoreactivity is considered typical for oncocytoma. 14
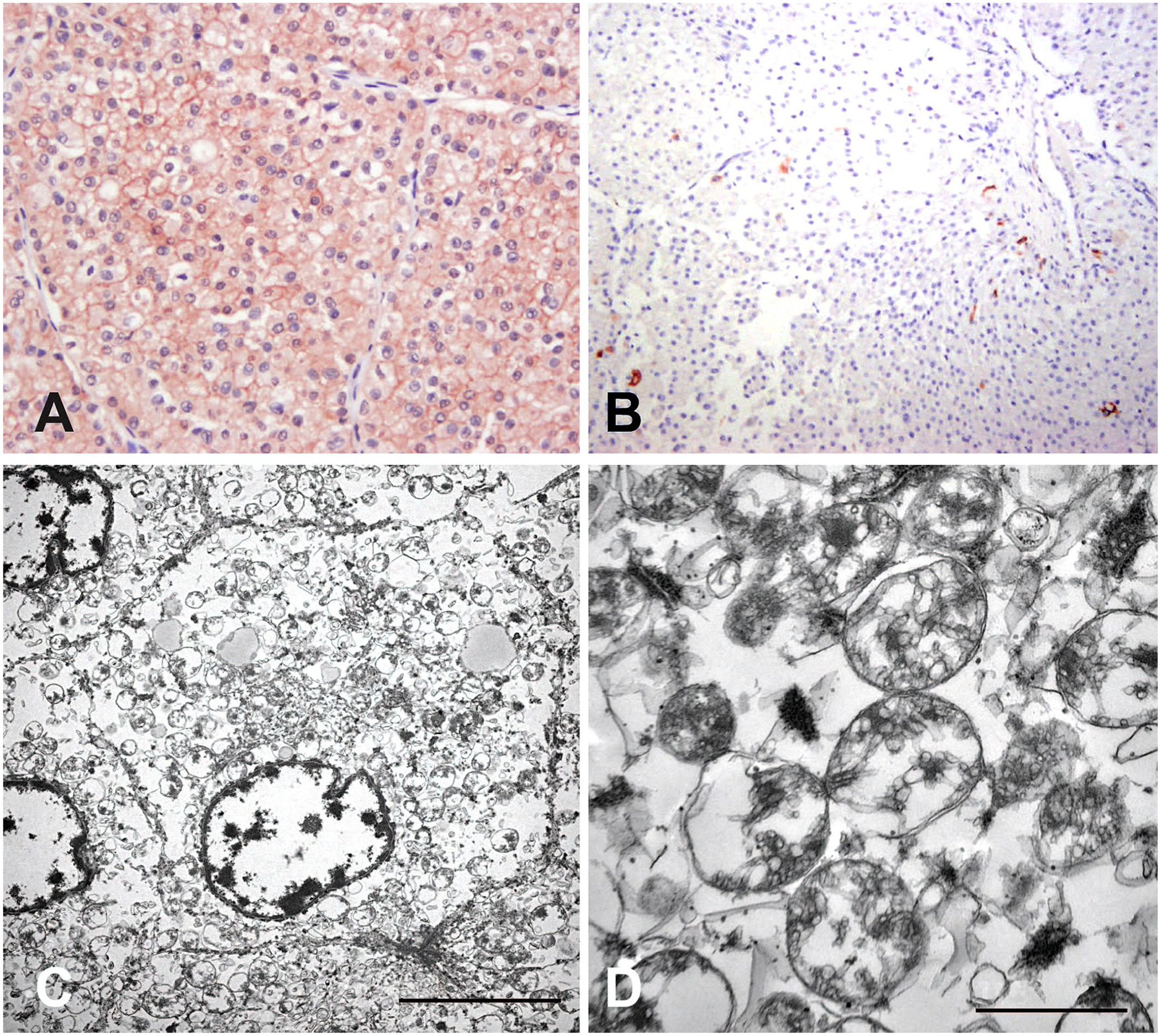
Ancillary testing of a renal oncocytoma in a chimpanzee.
Other markers, including DOG1, cyclin D1, vimentin, and special stains, including colloidal iron, succinic acid dehydrogenase (SDH), and periodic acid–Schiff (PAS) have been used in human medicine.14,16 PAS staining revealed variable numbers of PAS-positive cytoplasmic granules, and vimentin IHC was negative (data not shown); other IHC markers were deemed unnecessary in this case due to CD117 and CK7 IHC and TEM results (described below). DOG1 is uniformly expressed in chromophobe renal cell carcinoma and oncocytomas, but absent in renal clear cell carcinomas. Cyclin D1 is variably expressed in oncocytomas, but not expressed in either carcinoma. Vimentin is variably expressed in oncocytomas and renal clear cell carcinoma, but negative in chromophobe renal cell carcinomas. 16 SDH is used as a marker of differentiation between oncocytomas and renal chromophobe cell carcinomas in cases in which morphologic distinction is not clear, although it is not used as a screening marker. 14
Transmission electron microscopy identified eosinophilic granules within the cytoplasm as mitochondria. In a 70-nm tissue section, the cytoplasm of neoplastic cells contained 50–100, round-to-oval, irregular, 500-nm to 1-µm diameter, occasionally fractured, double membrane–bound mitochondria with tubular, haphazardly arranged cristae surrounded by variable amounts of clear space (Fig. 2C, 2D). No other organelles were identified. The nuclei were round to indented, with a few crenated and convoluted nuclei with mixed euchromatin and heterochromatin, and lacked a nucleolus. The cell membrane was generally smooth with small pockets of microvilli at the intersection between neighboring cells. The cell of origin of renal oncocytomas is believed to be intercalated epithelial cells of the cortical collecting duct. 11
Oncocytes do not necessarily have a single cell of origin or histogenesis. The term is a morphologic cellular description of a histologic change that can occur in cells in any organ. 12 Oncocytic change or transformation is seen as cytomegaly coupled with abundant eosinophilic granular cytoplasm due to the accumulation of altered mitochondria making up 30–60% of the cytoplasmic volume, presumably the result of metabolic or cellular stress.1,12 Some cells may normally have increased numbers of mitochondria; hence, evaluation must also include the cellular origin.
Renal tumors in chimpanzees are rare. In a 2009 survey of 2 chimpanzee facilities, including reports of 117 chimpanzee neoplasms before 2009, only 4 (3.4%) renal tumors were identified, including a primary renal carcinoma, 5 an ectopic adrenal cortical carcinoma, 8 and 2 benign hemangiomas. 2 We retrieved no cases of renal oncocytomas, or their malignant counterpart renal chromophobe cell carcinoma, using the search terms “renal oncocytoma” or “renal chromophobe cell carcinoma” and “chimpanzee” in PubMed and Web of Science, suggesting that this condition has not been reported previously in chimpanzees.
Renal oncocytomas have been documented as rare tumors in veterinary species, including the dog, 3 cat, 7 and rat, 9 but not non-human primates. In humans, oncocytomas are 3–7% of all primary renal tumors. 10 Beyond their characteristic gross, histologic, immunohistochemical, and ultrastructural features, human oncocytomas have been further evaluated karyotypically or by fluorescence in situ hybridization. Findings include a loss of chromosome 1, loss of the Y chromosome, or rearrangement of 11q13. 6 Despite the myriad changes that can be present, a diploid karyotype or loss of chromosome 1 with consistent histology and IHC is considered supportive of an oncocytoma diagnosis in equivocal cases. 15 Concern for potential infectious biological agents prevented archiving of any fresh tissue in our case; all tissue was formalin-fixed.
Our finding of an oncocytoma in a chimpanzee is almost identical to the well-defined entity documented in humans. Fortunately, surgical excision in those cases is usually curative.
Footnotes
Acknowledgements
We thank Dr. Jenessa Gjeltema (UC Davis), who managed the case. Dr. Bill Culp (UC Davis) performed the surgery and mass removal. Dr. Tess Rooney (UC Davis) collected the aspirate. Christina Heard (CAHFS) prepared sample sections for electron microscopy. This case was presented at the 2023 American College of Veterinary Pathologists Meeting Primate Pathology Workshop.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.