
Abstract
We investigated a case of severe Serratia odorifera infection in a racehorse. The horse had developed progressive lameness associated with swelling of the left tarsal region, which progressed to ulcerative dermatitis, tendinitis, tenosynovitis, and desmitis. The plantar side of the superficial digital flexor (SDF) tendon was visible through the skin ulcer, and coalescing nodules were present in the dermis. The horse was euthanized and an autopsy was performed. Grossly, in addition to the changes described above, severe edema of the soft tissues was associated with the ulcer. Microscopically, necrotizing and ulcerative, chronic-active dermatitis with granulation tissue was noted, along with lymphoplasmacytic and suppurative tendinitis (SDF), tenosynovitis (SDF and lateral digital flexor), and desmitis (long plantar ligament and flexor retinaculum [FR]), with collagen degradation and intralesional gram-negative bacteria. Serratia odorifera was isolated in pure culture from the ulcerated skin, SDF tendon, FR, and synovial fluid of the tarsus joint. To our knowledge, soft-tissue inflammation caused by S. odorifera has not been described in horses previously.
Serratia odorifera, S. marcescens, and S. plymuthica are gram-negative rods in the Enterobacteriaceae family. 7 These Serratia spp. are opportunistic agents found in nosocomial infections of immunocompromised human patients.7,15 In humans, they have been associated with sepsis (S. odorifera, S. marcescens),7,9,15 endocarditis (S. odorifera),11,14 liver and lung abscesses (S. odorifera, S. marcescens, S. plymuthica), 8 infection of the urinary tract (S. marcescens), 7 meningitis, encephalitis (S. marcescens), 7 endophthalmitis (S. marcescens), 7 osteomyelitis (S. marcescens, S. plymuthica),3,7 arthritis (S. marcescens), 7 and skin ulcers (S. marcescens). 17
In domestic animals, only infections with S. marcescens have been reported. Affected species include cattle (mastitis, early abortions),5,6 horses (septicemia in a foal), 18 dogs (skin ulceration and abscess), 13 and cats (endophthalmitis). 10 A review of PubMed, CAB abstracts, and Google Scholar did not yield any reference to infection by S. odorifera in horses. Here, we describe a case of ulcerative dermatitis, tendinitis, tenosynovitis, and desmitis associated with S. odorifera infection in a racehorse.
A 5-y-old Thoroughbred racehorse mare with a history of chronic ulcerative dermatitis on the plantar side of the left tarsal and metatarsal region was submitted for autopsy to the California Animal Health Food Safety Laboratory (San Bernardino Branch, San Bernardino, CA, USA). The skin ulcer had grown and failed to heal for ~24 d. The lesion was painful and the mare had hyperesthesia and swelling of the affected area. The horse was treated with enrofloxacin, procaine penicillin G, rifampin, minocycline, flunixin meglumine, hydrocortisone, and phenylbutazone, but given lack of improvement and poor prognosis, she was euthanized.
An autopsy was performed. The left tarsal region was swollen, and a 13.0 × 7.0-cm, deep ulcer was present ~4.0 cm distal to the calcaneal tuber (
Fig. 1A
,
1B
). The ulcer had hemorrhagic edges, and the abundant granulation tissue in the ulcer bed was covered by purulent exudate and occasional crusts. The subcutaneous tissue was firm, yellow, and multinodular. The plantar surface of the superficial digital flexor (
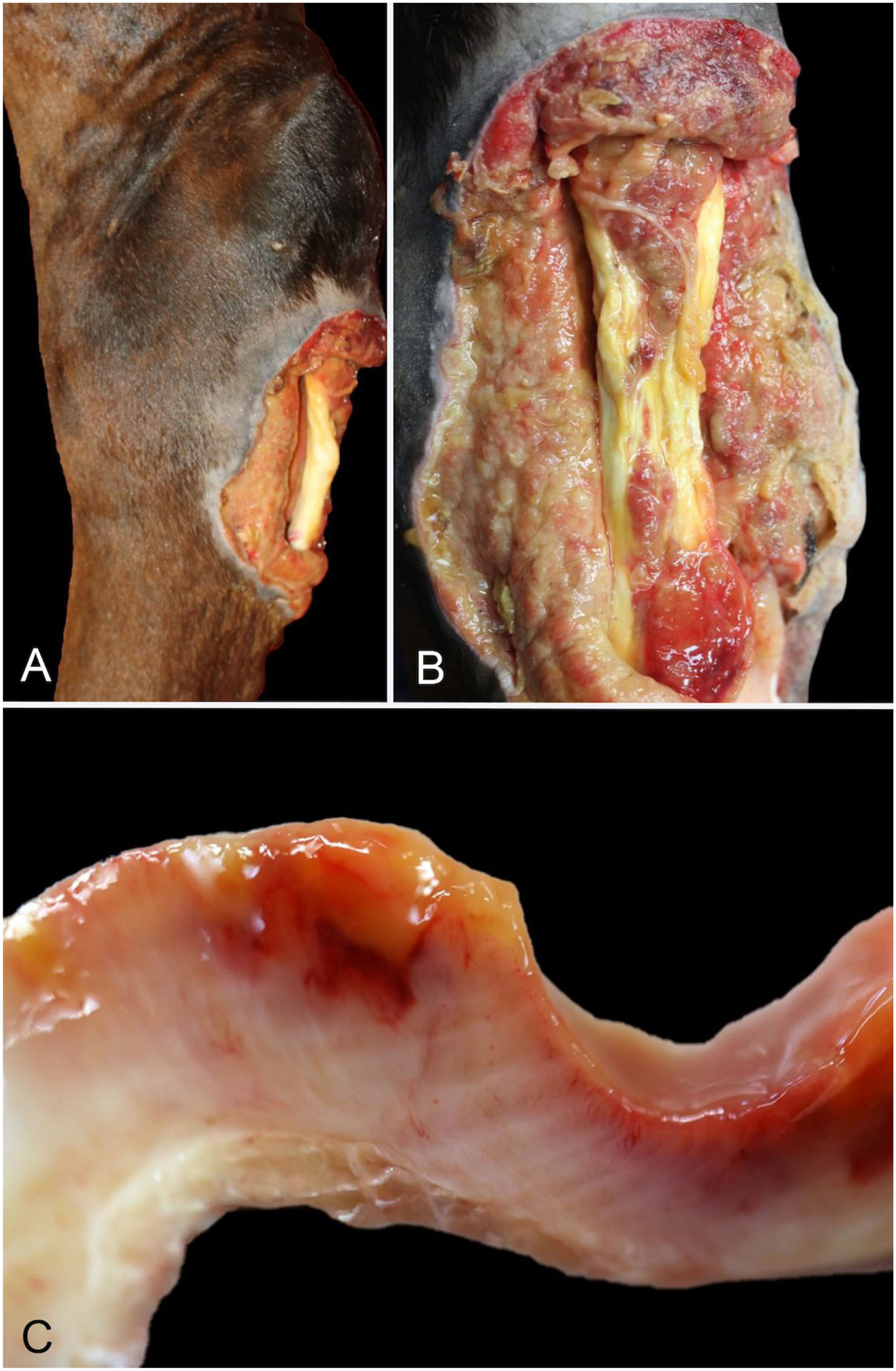
Gross lesions in the left tarsus of a horse with ulcerative dermatitis caused by Serratia odorifera.
Samples of skin, tendons, ligaments, joint capsule, brain, heart, lungs, liver, kidney, spleen, stomach, and intestines were collected, fixed in 10% neutral-buffered formalin, processed routinely, and 4-µm thick sections were stained with H&E, Gram, and period acid–Schiff/alcian blue (PAS/AB) stains.
Swabs were collected from the skin ulcer, SDF tendon, FR, and synovial fluid of the tarsus joint and inoculated onto trypticase soy agar (TSA) with 5% blood agar, chocolate agar, and MacConkey agar, and incubated aerobically at 37°C for 48 h. Bacterial colonies were identified using MALDI-TOF mass spectrometry (Sirius One; Bruker). S. odorifera in pure culture was isolated from the ulcerated skin, SDF tendon, FR, and joint fluid of the tarsus.
Microscopically, the epidermis and dermis of the affected region were ulcerated. The ulcer bed was covered by a layer of viable and degenerate neutrophils, hemorrhage, and bacterial colonies, with an underlying layer of granulation tissue infiltrated by macrophages, lymphocytes, and fewer plasma cells. In the SDF tendon, LPL, and FR, well-demarcated areas of granulation tissue compressed the epi- and endotendon and ligament, and effaced and replaced the fibrils of the collagen bundles ( Fig. 2A ). The granulation tissue was surrounded by a layer of macrophages and neutrophils admixed with immature collagen, fibrin, hemorrhage, karyorrhectic debris, and mixed gram-negative bacteria, which replaced and effaced the lining of the synovial sheath of the SDF tendon (distally) and the subtendinous calcaneal bursa of the SDF tendon (proximally). In less-affected areas, some collagen bundles had lost the normal parallel arrangement of the fibers. Tenocytes and ligamentocytes were absent, accompanied by mild-to-moderate infiltrates of viable and degenerate neutrophils, hemorrhage, and karyorrhectic debris ( Fig. 2B ). The synovial sheath of the SDF and lateral digital flexor tendons had few villi, with the intima thickened by 5–9 layers of synoviocytes admixed with lymphocytes, plasma cells, histocytes, and occasional neutrophils ( Fig. 2C , 2D ). No significant microscopic lesions were observed in any other tissue.
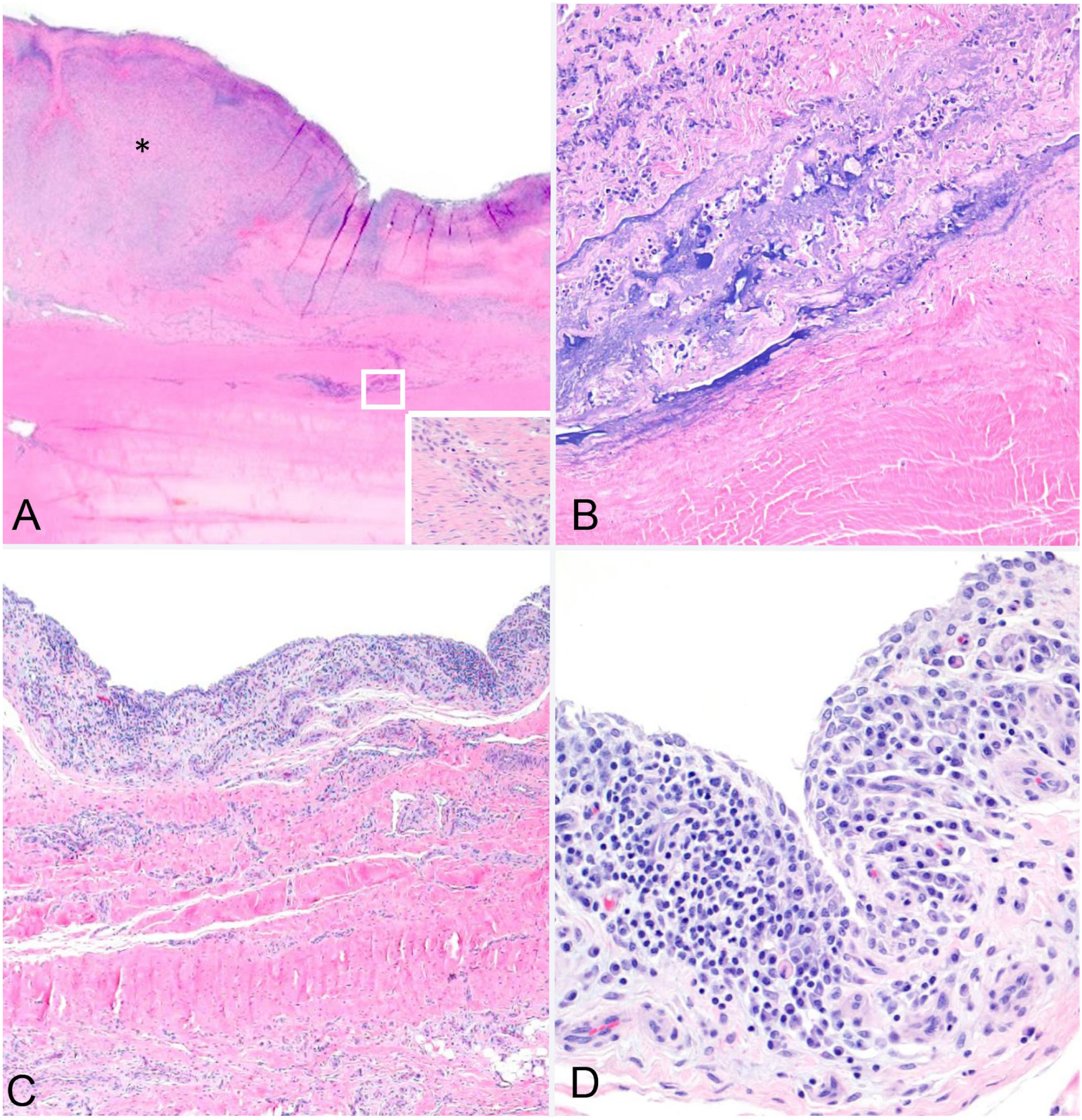
Microscopic lesions in a horse with ulcerative dermatitis, tendinitis, tenosynovitis, and desmitis caused by Serratia odorifera. H&E.
The most important findings in our case were ulcerative dermatitis with inflammation of the underlying tendons and other soft tissues, and isolation of S. odorifera in pure culture. The lesion in the skin of this horse was similar to those caused by S. marcescens in dogs and humans,13,17 but to our knowledge, lesions in tendons of horses or other animals associated with S. odorifera infections have not been reported previously. Septic tendinitis, tenosynovitis, and/or desmitis associated with Staphylococcus spp., Streptococcus spp., Escherichia coli, and Enterobacter spp. have been described in horses, often following a traumatic event and penetrating injury.2,4,16,20
Serratia spp. are opportunistic bacteria that typically cause infection via the respiratory or urinary tracts. In hospital-acquired systemic infection in humans, the use of contaminated catheters is another important portal of entry.9,11,14 Several of these human patients had preexisting conditions or risk factors that contributed to the opportunistic infection of Serratia spp., including hematologic disorders, and liver and/or kidney failure.9,11 In our case, no evidence of preexisting heart, liver, or kidney failure was evident in the clinical history or during the autopsy, and the portal of entry of S. odorifera was not determined. Possible portals of entry include wounds or injection sites. Although this mare had no history of local wounds or injections, we cannot rule out these possibilities.
As in humans, chlorhexidine and benzalkonium-resistant S. marcescens can be multidrug resistant and cause opportunistic infections.1,12 Virulence factors of S. marcescens involved in opportunistic infections include hemolysins, cytotoxic factors such as phospholipase A, and the ability to form biofilms. Antimicrobial resistance (
S. odorifera should be considered as a potential cause of soft-tissue infections in horses that may be refractory to routine antimicrobial therapy. Culture and AMS testing to direct appropriate therapy may result in a better outcome and would decrease the potential for development of additional AMR in opportunistic bacteria.
Footnotes
Acknowledgements
We thank Juliann Beingesser and Jose Constante for their excellent technical assistance.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was funded by the California Animal Health and Food Safety Laboratory, School of Veterinary Medicine, University of California–Davis.