
Abstract
Objective:
Evaluate patient-reported symptoms and quality of life (QOL) before and after female sterilization device (Essure) removal.
Design:
Multicenter prospective study.
Setting:
Three academic institutions.
Population or Sample:
Patients with device-attributed symptoms undergoing Essure removal.
Methods:
Symptoms were measured using a study-specific questionnaire and Short Form-8 (divided into Physical and Mental Component Scores). Scores at 4 months postoperative were compared to baseline using a mixed effects logistic regression and linear mixed model. Subgroup analysis was performed for hysterectomy and uterine-preserving groups.
Main Outcome Measures:
Patient-reported symptoms and Short Form-8 4 months after Essure removal compared to baseline.
Results:
A total of 80 patients enrolled in the study and underwent Essure removal: 53 (66.3%) with laparoscopic hysterectomy and 27 (33.8%) with laparoscopic bilateral salpingectomy or bilateral cornuectomy. Fifty-one participants (63.8%) completed the 4-month postoperative questionnaire. Of the 17 device-attributed symptoms evaluated, participants reported clinically important improvement in 16 of the symptoms postoperatively. QOL improved significantly following device removal, with the Physical Component Score improving by 9.9 points (95% CI: 7.0–12.9) and the Mental Component Score by 13.8 points (95% CI: 10.4–17.2). QOL improved in both physical and mental score domains after device removal with no difference between hysterectomy and uterine-preserving groups (p = 0.83 and p = 0.06, respectively). Of the entire cohort, 92.2% (n = 47) were satisfied with their surgical results.
Conclusions:
Patients undergoing Essure removal for device-attributed symptoms report improved symptoms and QOL following surgery. Device removal may benefit those experiencing device-attributed symptoms and is associated with high patient satisfaction.
Keywords
Introduction
Essure (Bayer AG, Leverkusen, Germany) is a hysteroscopic sterilization device that was introduced in 2002 and gained popularity world-wide.1–3 It consists of an expanding nickel-titanium micro-insert placed in each proximal fallopian tube to induce tissue ingrowth and tubal occlusion. 4 The device was effective in preventing pregnancy, with an age-adjusted effectiveness of 99.7% at 5 years.2,5,6 However, given device malposition, chronic pelvic pain, abnormal bleeding, allergic reaction, and numerous other device-attributed symptoms affecting 1.1%–4.2% of recipients, Bayer AG voluntarily withdrew Essure from the United States market in 2019.1,7–10
Surgical removal of the Essure device became common practice for patients experiencing device-attributed symptoms.11,12 Removal is typically performed via bilateral salpingectomy, as the micro-inserts permanently adhere to the fallopian tubes.13,14 Salpingectomy may be performed together with a bilateral cornuectomy or hysterectomy to ensure the device is entirely removed. Several retrospective studies have described the outcomes of patients undergoing Essure removal with a focus on pelvic pain.15–18 Pelvic pain has been shown to improve in up to 88.5% of patients who undergo Essure removal; however, less is known about other device-attributed symptoms.11,12 Quality of life (QOL) seems to improve after Essure removal; however, this has only been explored in single-institution and retrospective studies.18,19 To address this gap, we conducted a prospective, multi-center study to evaluate common device-attributed symptoms and QOL after Essure removal surgery. Our primary objective was to determine change in symptoms and QOL from baseline to 4 months postoperative. A secondary objective was to compare symptom and QOL outcomes between patients undergoing hysterectomy and uterine-preserving surgeries. We hypothesize that symptoms and QOL would improve following Essure removal and would be most improved after hysterectomy.
Materials and Methods
This multicenter, prospective study was performed at three academic institutions between 2017 and 2020 in collaboration with the Society of Gynecologic Surgeons Fellows’ Pelvic Research Network (FPRN®). It was stopped after the target sample of 80 patients was reached. Sample size was determined based on the volume of procedures anticipated at the participating institutions over a 3-year time frame.
Patients ≥18 years scheduled for Essure removal were recruited. Patients were eligible if they/their surgeon suspected the device to be causing symptoms and informed consent could be given in English. Surgical approach and concomitant procedures were at the discretion of the patient and surgeon. All surgeons were high-volume, fellowship-trained minimally invasive gynecological surgeons.
Eligible patients were given a recruitment letter explaining the study and surveys. Participants indicated consent to participate by completion of the preoperative survey. Data were abstracted from the medical record and intraoperative data collected in a surgeon-completed form (Table 1). Surveys were administered on paper by mail, electronically through a web link, or verbally by phone, according to participant preference (Supplementary Data S1: Preoperative questionnaire). Symptoms were assessed using a study-specific questionnaire (see below for survey development). QOL was measured using the validated Short Form-8 (SF-8), which is divided into physical and mental component scores. Higher scores indicate better health status.
Patient and Procedure Characteristics
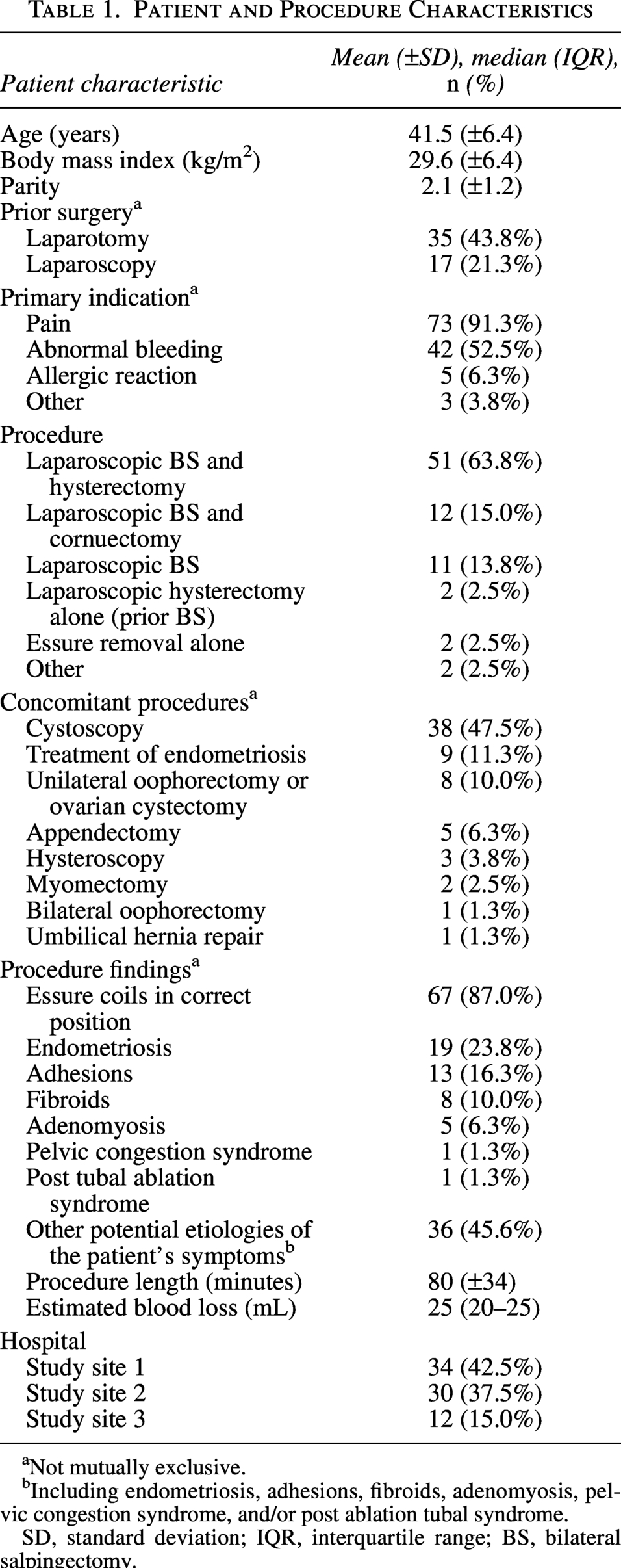
Not mutually exclusive.
Including endometriosis, adhesions, fibroids, adenomyosis, pelvic congestion syndrome, and/or post ablation tubal syndrome.
SD, standard deviation; IQR, interquartile range; BS, bilateral salpingectomy.
Follow-up surveys were administered 4 months postoperative (Supplementary Data S2: Postoperative questionnaire). This end-point allows the preceding 4-weeks assessed in SF-8 to occur after complete surgical recovery. A $25.00 gift card was included as an incentive to complete the postoperative survey. All data were stored in REDCap (Vanderbilt University, 2021). Institutional review board approval was obtained at each site before initiating recruitment.
Device-attributed survey development
The investigator team sought input from clinicians and research experts on symptoms experienced by people with Essure and, through an iterative process, developed a survey draft. A female research assistant with training in recruitment and qualitative interviewing recruited patients in clinic. She had no prior relationship with participants and introduced herself as a research assistant working on the study. She informed participants that the study objective was to better understand the symptoms experienced by people with Essure and develop a condition-specific survey. Patients agreeing to participate completed an interview in person at a clinic visit or by phone at a time of their choosing. A convenience sample of 11 patients with Essure-attributed symptoms receiving care at one of the study sites was recruited, 4 patients at a consult visit to review the baseline survey and seven patients at a postoperative visit to review the postoperative survey. Participants were provided the survey draft and were asked to provide feedback on survey readability, applicability, symptom completeness, symptom accuracy, and postoperative survey delivery timing. Field notes were made during the interviews and curated afterwards. Four study team members reviewed the field notes and identified three emerging themes: (1) Revise for clarity, (2) add questions/symptoms, and (3) follow-up survey should be >3 months postoperative. Patient feedback was incorporated using a consensus approach, the surveys were revised for clarity, and the symptom of hair loss was added. Additionally, postoperative survey timing was delayed to 4-months.
Analysis
Patient and procedure characteristics were analyzed using descriptive and inferential statistics. Patients who completed the postoperative questionnaire were compared to those who did not to assess for responder bias. A subgroup analysis was performed comparing patients who underwent a hysterectomy versus a uterine-preserving procedure. Data were analyzed using two-sample t-tests for normally distributed continuous data, Wilcoxon rank sum tests for nonnormally distributed continuous data, and Fisher’s exact tests for categorical data. Mixed-effects logistic regression was used to assess change in symptoms before versus after Essure removal. Linear mixed models were used to assess change in SF-8 scores before versus after Essure removal. Statistical analysis was performed using SAS software, version 9.4.
Effect size is reported as odds ratio with 95% confidence intervals. The minimal clinically important difference (MCID) is the smallest difference in an outcome measure that patients perceive as beneficial and that warrants the cost and risk of an intervention. 20 The MCID is condition and intervention specific; however, a description of postsurgical MCID for SF-8 is absent in the gynecologic and general surgery literature. In the absence of data from a similar population, we include MCID following spinal stenosis decompression as a reference. In this population, an improvement of 5–6 points on the Physical Component Scale and 2–6 points on the Mental Component Scale was found to be clinically important. 21
Results
Eighty eligible patients were recruited, completed the preoperative questionnaire, and underwent Essure removal at the three sites between 2018 and 2020 (Table 1). The most common indications for surgery were pelvic pain (n = 73, 91.3%) and abnormal bleeding (n = 42, 52.5%). Before Essure placement, 65.0% (n = 52) of patients reported using hormonal contraception, with 94.2% (n = 49) reporting hormone discontinuation after Essure placement. At baseline, 75.0% (n = 60) reported following social media groups to discuss Essure-associated problems.
Participants underwent laparoscopic hysterectomy with bilateral salpingectomy (n = 51, 63.8%), laparoscopic bilateral salpingectomy with cornuectomy (n = 12, 15.0%), laparoscopic bilateral salpingectomy alone (11/80, 13.8%), laparoscopic Essure removal alone (n = 2, 2.5%), and laparoscopic hysterectomy alone in patients who had previously undergone a bilateral salpingectomy (n = 2, 2.5%). All patients who completed the baseline survey underwent the planned procedure. The 57 patients who elected to undergo a hysterectomy reported doing so to ensure the entire Essure coil was removed (87.0%, n = 47), to treat their pain (66.7%, n = 36), and to stop their periods (37.0%, n = 20).
Intraoperative findings identified proper Essure coil placement in 87.0% of patients (n = 67) and other potential etiologies of symptoms in 45.6% (n = 36). Eight participants (10%) experienced a postoperative complication within 30 days of surgery, which included: minor infection (N = 5 post-hysterectomy), allergic dermatitis (n = 2, 1 post-hysterectomy and 1 post-cornuectomy), and 1 reoperation (post-hysterectomy).
Fifty-one patients (63.8%) completed the 4-month follow-up. Of the 17 device-attributed symptoms, significant improvement occurred in 16 of 17 symptoms (Table 2). Following Essure removal, SF-8 physical component summary scores showed a 9.9-point increase (95% confidence interval [CI]: 7.0–12.9) and mental scores a 13.8-point increase (95% CI: 10.4–17.2). Patients who completed the postoperative questionnaire (n = 51) were slightly older in age, of lower parity, and more likely to be of White race than those who did not respond (n = 29) (data not shown). Responders were otherwise similar to nonresponders, with similar hysterectomy rates between groups. Patients who underwent hysterectomy (n = 53, 66.3%) were similar to those who underwent a uterine-preserving procedure (n = 27, 33.8%), except that they were more likely to have a primary surgical indication of pelvic pain or abnormal uterine bleeding (data not shown).
Symptom and Quality of Life Outcomes at 4-Months Postoperative as Compared to Baseline
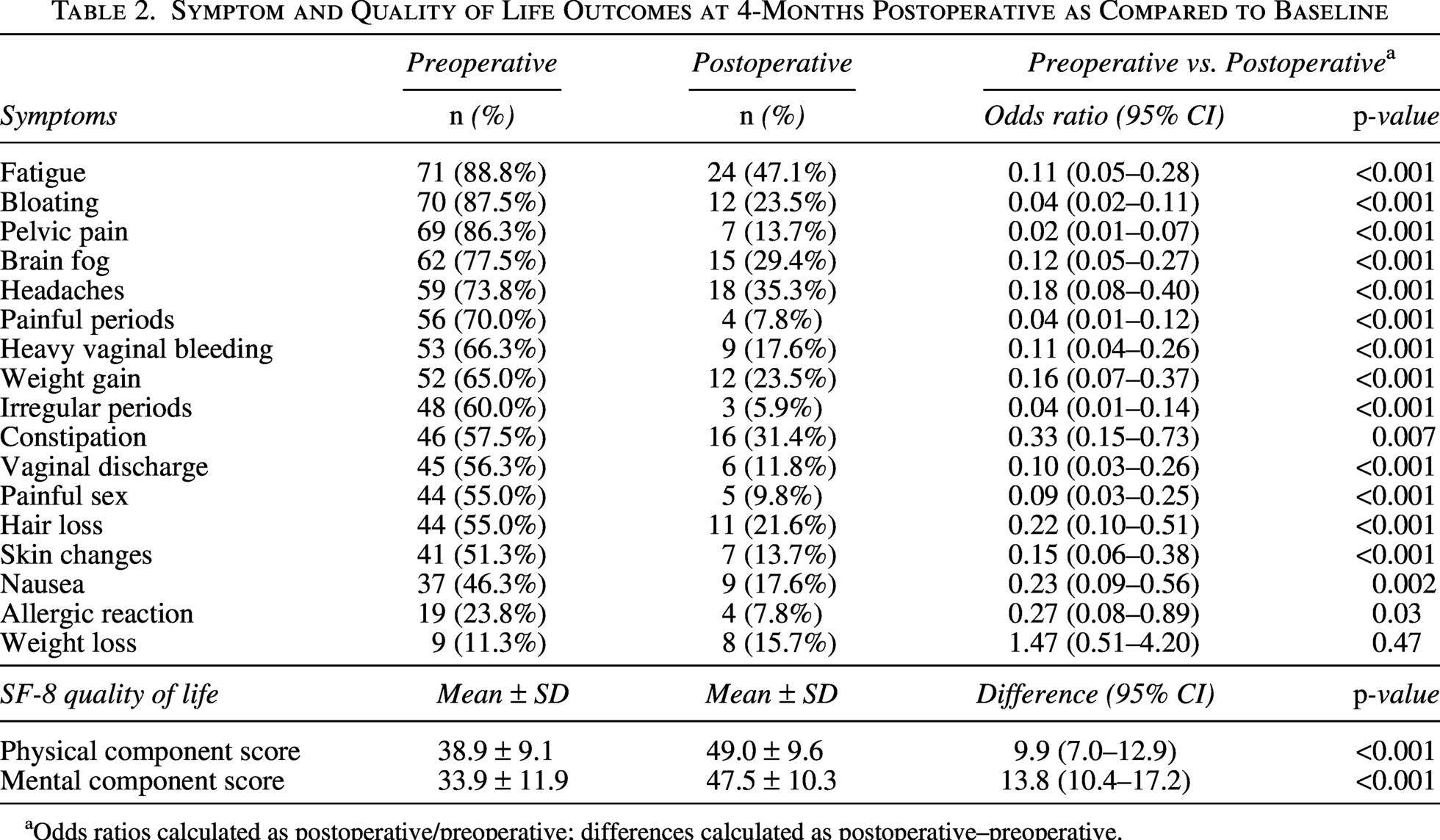
aOdds ratios calculated as postoperative/preoperative; differences calculated as postoperative–preoperative.
Symptom change and QOL outcomes between hysterectomy and uterine-preserving groups are shown in Table 3. Pelvic pain and vaginal discharge were more likely to resolve following hysterectomy (OR 13.2 [95% CI: 1.44–121] and OR 10.3 [95% CI: 1.17–89.9], respectively), while changes in the other symptoms were similar in both groups. Patients who underwent a hysterectomy had greater improvement in their mental component score compared to those who underwent a uterine-preserving procedure; however, this did not reach statistical significance (6.8 point greater improvement [95% CI: −0.2 to 13.8]). Physical component score changes were similar for both groups.
Symptom and Quality of Life Outcomes at 4-Months Postoperative for Hysterectomy Versus Uterine Preservation (No Hysterectomy) Sub-Groups
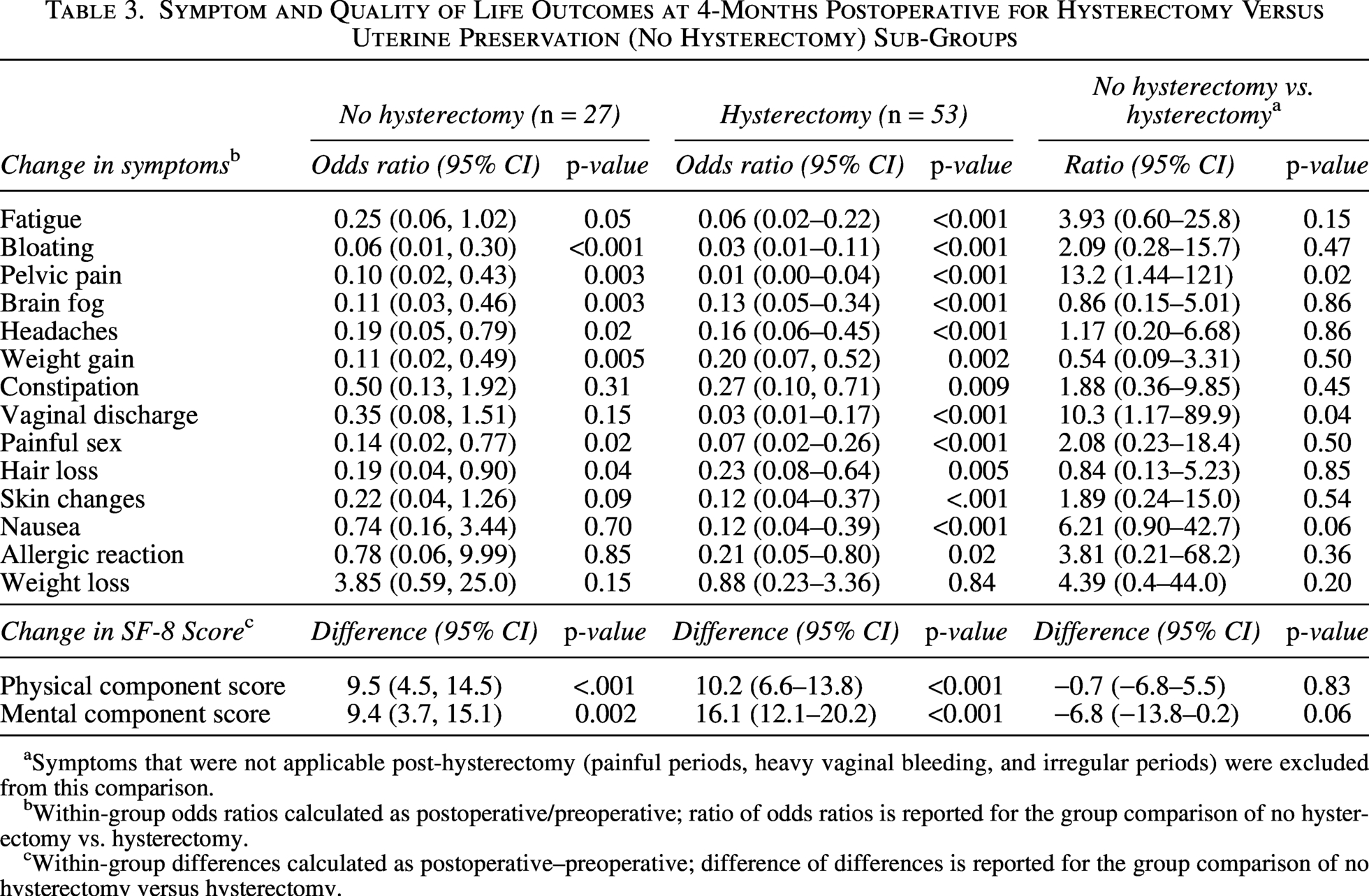
Symptoms that were not applicable post-hysterectomy (painful periods, heavy vaginal bleeding, and irregular periods) were excluded from this comparison.
Within-group odds ratios calculated as postoperative/preoperative; ratio of odds ratios is reported for the group comparison of no hysterectomy vs. hysterectomy.
Within-group differences calculated as postoperative–preoperative; difference of differences is reported for the group comparison of no hysterectomy versus hysterectomy.
Of the 51 patients who completed the postoperative survey, 92.1% (n = 47) reported they were satisfied with the results of surgery. Eight patients (15.7%) reported new onset symptoms, two after salpingectomy with cornuectomy (vasomotor symptoms [n = 1] and abdominal pain [n = 1]) and six after hysterectomy (pelvic pain [n = 1], dyspareunia [n = 1], post-coital bleeding [n = 2], and urinary or bowel symptoms [n = 2]). Ultimately, 49 (96.1%) patients felt that the symptoms they had before surgery were related to Essure.
Discussion
Main findings
We found that 16 of 17 device-attributed symptoms and both mental and physical QOL scores improved following Essure removal. Pelvic pain was the most common indication for surgery and was most likely to improve after a hysterectomy. While some patients experienced new symptoms following surgery, 92.1% of patients were satisfied with their procedure.
Results in the context of previous studies
Prior studies examining Essure removal reported 39.8%–88.5% of patients experienced complete or partial symptom improvement postoperative.11,12,15,18,19 Limitations of these studies are a dependence on retrospective and single-institution study design and limited assessment of QOL (with only two studies using validated measures). These studies demonstrated an improvement in symptoms after surgery; however, study design limitations decrease their utility in clinical practice.
In our prospective multicenter study, we found a strong association between Essure removal and resolution of pelvic pain, which supports prior findings (OR: 0.02, 95% CI: 0.01–0.07). When comparing hysterectomy to uterine preservation, we found similar improvements in non-menstrual symptoms, with greater improvement in pelvic pain and vaginal discharge after hysterectomy. One prior study compared outcomes between patients who underwent a laparoscopic bilateral salpingectomy with cornuectomy versus a vaginal hysterectomy and found no difference in symptom improvement between groups. 16 All hysterectomies in our study were performed laparoscopically, and 45.6% of patients had other potential symptom etiologies, which were identified and treated during surgery. This may explain why pelvic pain showed greater improvement after laparoscopic hysterectomy in our study but no difference after vaginal hysterectomy.
Prior to our work, the most robust data on QOL post-Essure removal was from a French single-institution study. 17 The QOL of 80 patients was evaluated using SF-12, the Visual Analog Scale, and the McGill pain score. Forty-seven patients underwent device removal alone with or without cornuectomy, and 33 had a concomitant uterine procedure (23 endometrial ablation, 5 myomectomy, and 5 hysterectomy). They found significant improvement in both mental and physical health domains at 1-month postoperative, which was sustained at 3- and 6 months postoperatively. Similar to these findings, participants in our study demonstrated improvement in both mental and physical health domains that was sustained beyond 3 months postoperative.
A key consideration for patients seeking Essure removal is determining the optimal removal approach. Findings from our study provide data to assist with informed decision-making. While patients showed high satisfaction and improvement in symptoms and QOL after both hysterectomy and uterine-preserving surgeries, for patients with abnormal bleeding, pelvic pain, and/or vaginal discharge, hysterectomy may carry additional benefit.
Our study is novel, as we employed patient-engaged methods to understand and evaluate the device-attributed symptoms important to patients. Our findings highlight the benefit of Essure removal for multiple symptoms, including those that are identified by patients as important but not previously described. While this study cannot determine if Essure is the direct cause of symptoms, the results may be used to better counsel patients considering Essure removal.
While the Essure product is no longer available in the United States, important lessons about patient-health care relationships can be learned and integrated into future research and development endeavors. The term “health-care gaslighting” has been widely used to describe the patient experience of having Essures placed and then having symptoms dismissed as not being from the device. 22 Women and other historically marginalized groups are often targets of gaslighting. 23 Patient connectivity through social media and advocacy through large Facebook groups like “Essure Problems” were key in giving women a voice and directing the Essure narrative. 24 Over the past decades, gynecology has been plagued by prominent device lawsuits and products being removed from the market.25,26 These device-related complications are crucial barriers to patients trusting clinicians and the health care system as a whole. This may have negative implications for patient acceptance of future devices. Continued innovation in gynecology, especially with a focus on decreased invasiveness, is desperately needed. However, for future innovation and medical devices to succeed, we must learn from Essure: (1) the importance of comprehensive patient counseling on the risks of engineered products, with focus on the risks specific to implantable devices; (2) the voices and experiences of patients are valid; (3) industry must be transparent and timely in adverse event reporting; and (4) social media platforms can be strong drivers of health care, research, and development.24,27
Strengths and limitations
This study represents one of the largest cohorts of patients undergoing Essure removal and the only one to employ a multicenter prospective study design. Additionally, we used patient-engaged methods, validated measures, and robust data collection methods to reach patients of different backgrounds. Study limitations include responder bias, as patients who completed the postoperative questionnaire had some characteristics that were different than those who did not complete the questionnaire, and confirmation bias, in which patients undergoing Essure removal may tend to report results that support their decision for surgery. Given the novel Essure-specific patient-reported outcomes assessed, a sample size calculation was not feasible, and recruitment size was determined based on clinical volume. Additional work is needed to evaluate long-term impacts of Essure removal, with a focus on symptom evolution over a longer period of time and longitudinal satisfaction with hysterectomy as compared to uterine preservation. Patients presenting for Essure removal had a high incidence of other pathology likely contributing to symptoms. It is possible that the symptom improvement identified in this study was due to treatment of the underlying conditions and not due to Essure removal specifically.
Conclusion
Patients undergoing Essure removal for device-attributed symptoms report improved symptoms and QOL following the surgery. This prospective cohort study found that Essure removal led to significant improvement in 16 of 17 device-attributed symptoms and improved mental and physical QOL scores on SF-8. While some patients experienced new symptoms following surgery, 92.1% of patients were satisfied with their procedure choice.
Authors’ Contributions
CRediT author statement: W.T.R. was involved in the investigation, project administration, writing- original draft. C.M.H. involved in the investigation, writing—review and editing. C.A. was involved in investigation, writing—review and editing. P.M. was involved in project administration, writing—review and editing. C.M.S. was involved in formal analysis, data curation, writing—review and editing. A.R.K. was involved in formal analysis, data curation, writing—review and editing. T.A.D. was involved in resources, writing—review and editing. A.C.Y. was involved in conceptualization, funding acquisition, writing—review and editing. M.O.A was involved in investigation, writing—review and editing. J.I.E. was involved in investigation, supervision, writing—review and editing. S.L.R. was involved in conceptualization, methodology, investigation, writing—review and editing, funding acquisition. N.V.C. was involved in conceptualization, methodology, investigation, project administration, writing—original draft, funding acquisition.
Footnotes
Acknowledgments
The authors thank Elise Requadt for her assistance with article editing and Alexis Lindsey for her assistance with qualitative interviews and survey development.
Author Disclosure Statement
C.M.H., C.A., P.M., C.M.S., T.A.D., A.C.Y., S.L.R., and N.V.C. have no financial relationships to disclose. W.T.R. is funded through National Institute of Health K23 HD110710 and R21 HD115568, ARPA-H Sprint for Women’s Health ICHUB-24–101-1392/SWH-24, Washington University Institute of Clinical and Translational Sciences KL2 (2022–2024) and Doris Duke Fund to Retain Clinical Scientists (2024). A.R.K. owns stock in Merck Pharmaceutical. J.I.E. is a consultant for Arthrex.
Funding Information
This study was performed in collaboration with the Society of Gynecologic Surgeons Fellows’ Pelvic Research Network (FPRN®). The FPRN® provided advisory support for the overall study design and site collaboration. The FPRN® provided financial support for subject reimbursement and statistical analysis. The FPRN® had no role in final study methodology, data collection, analysis, or interpretation of data; writing of the report; or in the decision to submit the article for publication.
Prior Presentation
This study was presented at the 48th Annual Scientific Meeting of the Society of Gynecologic Surgeons in San Antonio, TX from March 27-30, 2022.
IRB Approval
This study received Institutional Review Board approval from (1) Partners Human Research Committee at Brigham and Women’s Hospital and Massachusetts General Hospital, protocol ID 2017P000375/PHS, first approved 28 April 2017, (2) Vanderbilt Institutional Review Board, protocol ID 180380, first approved 15 March 2018, (3) Human Subjects Protection Office at Penn State College of Medicine, protocol ID STUDY00011383, first approved 30 January 2019.