
Abstract
Objectives:
We aimed to evaluate the feasibility of performing gynecological laparoscopic surgeries under spinal anesthesia (SA) and compare the anesthetic parameters and patient satisfaction between SA and general anesthesia (GA) in gynecological laparoscopic surgeries.
Methods:
This prospective, single-blinded, randomized clinical trial included 80 women indicated for laparoscopic surgery. Participants were randomly assigned to two groups of 40 each, SA and GA, and outcomes were compared between them.
Results:
Respiratory rate and mean arterial blood pressure were generally lower in the GA group than in the SA group (p > 0.05). During surgery, the SA group experienced more complications than the GA group (p < 0.05). There was no significant difference between the two groups in the incidence of hypertension, bradycardia, restlessness, dyspnea, abdominal pain, respiratory depression, and chills during surgery (p > 0.05). Post-Anesthesia Care Unit (PACU) recovery time was significantly longer in the GA group (p = 0.001). The prevalence of chills and restlessness as PACU complications was significantly higher in the GA group than in the SA group (p = 0.001). Surgeons’ satisfaction levels were significantly higher with GA (p < 0.05).
Conclusion:
Although SA and GA showed no significant differences, SA appears more satisfactory for gynecological surgeons performing laparoscopic procedures. However, the best anesthesia choice depends largely on the type of surgery and the patient’s condition.
Keywords
Introduction
Laparoscopic surgery has the benefit of causing less surgical stress than open surgery, which causes less discomfort and less postoperative respiratory function impairment. 1 General anesthesia (GA) with controlled ventilation has traditionally been regarded as the safest technique for laparoscopic procedures because it maintains end-tidal carbon dioxide (ETCO2) within a normal range, which may be disturbed by abdominal insufflation; regional anesthesia is generally not recommended because the Trendelenburg position and pneumoperitoneum are two established factors that adversely affect cardiovascular and respiratory function.2–5
Although spinal anesthesia (SA) is followed by some neurological deficits such as cauda equina syndrome, decreased heart rate, low blood pressure, back and shoulder pain, and headaches, it also has many advantages like the convenience of the procedure, patient consciousness, the reduced necessity of sedatives or narcotics, avoidance of possible consequences of GA and intubation, early discharge, and low failure probability.3,6 Due to the contraindications of GA in some illnesses and situations like chronic obstructive pulmonary disease, musculoskeletal disorders, muscular disorders, pulmonary diseases, and asthma, SA has been considered to be a potential replacement for GA in recent years. 7
Recent evidence from general surgeons suggests that the advantages of laparoscopic surgery may increase when regional anesthesia is combined with minimally invasive surgery.8,9 This prospective and randomized study aimed to compare SA and GA in advanced gynecological laparoscopic surgery regarding safety and patient tolerance.
Methods
This prospective, single-blinded, randomized clinical trial study was conducted at Al-Zahra Hospital in Tabriz. This study was conducted in the interval of March 2022 to Sep 2022. This study has been registered in the Iranian Registry of Clinical Trials (IRCT20211103052950N1, 27/01/2022) and approved by the Ethics Committee of the Tabriz University of Medical Sciences, Tabriz, Iran (Code Number: IR.TBZMED.REC.1400.690, 25/10/2021).
Each participant gave their informed consent after the faculty ethics council at Tabriz University of Medical Sciences authorized the research. The participants in this study were 80 patients aged between 18 and 60 with American Society of Anesthesiology (ASA) I-II physical status who were scheduled for grade I, II gynecological laparoscopic surgeries.
To determine the sample size, a similar study by Das (2015) was used with the help of the sample volume determination software to check quantitative programs in independent groups using the formula. The sample size includes an alpha error (significance level) of 5%, an optimal p-value of 0.5, an error rate of 0.13, and a power of 80%.
The number 80 was obtained from patients using the easy sequential sampling (consecutive) method. They randomly divided them into two equal groups of 40 people using randomized software (Rand list online) and entered them into the study. The study was blind to whom were responsible for data analysis. The period of recruitment and follow-up was approximately 1 year.
All these patients were randomly allocated into two groups, group A (40 patients undergoing GA) and group B (40 patients undergoing SA), using the random number table under the direct supervision of the corresponding author. The exclusion criteria were coagulation disturbances requiring blood transfusion, hypersensitivity to SA, any contraindication for SA, body mass index >30 kg/m2, history of more than two surgeries, grade III, IV gynecological surgeries, and any systemic diseases.
Before the procedure, patients in both groups underwent standard monitoring every 5 minutes—heart rate, respiratory rate, SpO2, ECG, and noninvasive blood pressure—and monitoring continued throughout the surgery until the patient was transferred to the postanesthesia care unit (PACU). In addition, end-tidal CO2 pressure was monitored only in group B patients. After venous cannulation with an 18 G catheter, preload infusion was started with Ringer solution 10 ml/kg initially, followed by Ringer solution at 4 ml/kg/h throughout the surgery.
In Group A, midazolam 0.03 mg/kg and fentanyl 1 μg/kg were infused IV as premedication. Induction was performed with lidocaine 1 mg/kg, propofol 2 mg/kg, and atracurium 0.5 mg/kg; maintenance was achieved with remifentanil and propofol. The patient was intubated with an endotracheal tube size 7.5, and ventilation was controlled mechanically with a tidal volume of 8–10 mL/kg and a respiratory rate of 12 breaths per minute.
In group B, patients in thiSA group experienced SA, considering sterility, performed in L3 to L4 by a 25-G Quincke spinal needle while they were sitting.
A total of 10 mg of bupivacaine 0.5% and 10 µg of fentanyl were injected into the subarachnoid space, after which the patient was immediately positioned supine. The level of sensory blockade was measured and recorded using a pinprick test. If the sensory blockade reached the T4 level, surgery was commenced. An oxygen mask at 4 to 5 L/min was used for the patients. Midazolam 0.03 mg/kg was administered to reduce patients’ anxiety. Additional intravenous doses of fentanyl 2 µg/kg were given to patients with shoulder pain, abdominal pain, or restlessness. Patients with agitation and persistent pain despite medical therapy were converted to GA and replaced with a new patient.
Both groups’ adverse events, including inability to perform surgery, change to laparotomy, conversion of SA to GA, hypotension (a decrease of more than 20% in systolic blood pressure), hypertension (an increase of more than 20% in systolic blood pressure), bradycardia (heart rate less than 50), respiratory depression and dyspnea (respiratory rate less than 12 and O2 saturation less than 95%), headache, nausea, vomiting, chill, and itching, were noted and appropriately managed when they occurred. Also, additional dosages of fentanyl or conversion to GA were recorded in group B. SA or GA and laparoscopic surgery were all carried out by the same anesthesia and surgical teams.
Patients were observed in the PACU; any complications were recorded and treated. Pain severity and sedation level were assessed every 15 minutes using the visual analog scale (VAS) and the Ramsay sedation score, respectively. The VAS categorizes pain into four levels: no pain (0/10), mild pain (≤3/10), moderate pain (4–7/10), and severe pain (≥8/10). Both surgeons and patients reported their satisfaction with the procedure at three levels: fully satisfied, comparatively satisfied, and not satisfied. The position for surgeries was lithotomy, and a 15°–25° Trendelenburg position was used in both groups. One liter/min of CO2 was chosen to provide proper pneumoperitoneum. Intra-abdominal pressure (IAP) was maintained in the 12–14 mmHg range using low-pressure CO2 when possible. All patients in both groups received 4 mg of ondansetron during the surgery.
Statistical analysis
The SPSS software (version 21.0, Chicago, IL, USA) was used for data analysis. Qualitative data are presented as frequencies (percentages). Quantitative data are displayed as mean ± standard deviation according to their normal distribution. The Shapiro–Wilk test was used to assess data normality. p-value was obtained for qualitative data via Fisher’s exact test and chi-squared test and for quantitative data via independent T-test (if parametric) and Mann–Whitney U test (for nonparametric variables).
Results
A total of 80 patients were enrolled in this study, divided into two groups: 40 patients in the GA group and 40 patients in the SA group. Patients had a mean age of 35.15 ± 9.60 years. The youngest patient was 18 years old, and the oldest was 60 years old. The mean weight was 70.40 ± 12.36 kg. The lowest weight was 64 kg, and the highest weight was 108 kg. A total of 62 patients (77.5%) had ASA I physical status, and 18 (22.5%) had ASA II physical status.
Patients underwent gynecological laparoscopic surgery for different reasons in this manner: cystectomy (47 patients, 58.75%), EP (20 patients, 25%), infertility (tubal evaluation) (4 patients, 5%), hysterectomy (2 patients, 2.5%), ovarian torsion (2 patients, 2.5%), resection of the secondary horn of the uterus (1 patient, 1.25%), endometriosis (1 patient, 1.25%), myomectomy (1 patient, 1.25%), laparoscopic IUD removal (1 patient, 1.25%), and oophorectomy (1 patient, 1.25%). The mean duration of surgery for all studied patients was 53.86 ± 17.09 minutes. The minimum surgery time was 25 minutes, and the maximum was 145 minutes. The mean duration of anesthesia for all studied patients was 63.99 ± 18.19 minutes. The minimum anesthesia duration was 35 minutes, and the maximum was 150 minutes. Comparison of demographic variables—including age, weight, ASA class, reason for surgery, duration of surgery, and duration of anesthesia—between the GA and SA groups revealed no statistically significant differences (p > 0.05).
Hemodynamic changes
The comparison of mean arterial blood pressure (MAP), heart rate, arterial oxygen saturation (O2 Sat), respiratory rate, and EtCO2 changes during the study period between the two groups is shown in Figures 1, 2, and Supplementary Appendixes S1–S3, respectively. The results showed that MAP was consistently lower in the SA group than in the GA group throughout the investigation (Supplementary Appendix S1). However, a statistically significant difference between the groups was observed only at the 5-minute time point (p = 0.001).

Comparison of arterial oxygen saturation during the study period between groups.

Comparison of the number of breaths during the study between groups (p < 0.05).
Heart rate
The results showed that there was no statistically significant difference between the two groups (Supplementary Appendix S2).
Arterial oxygen saturation
The obtained results showed that the arterial blood oxygen saturation values in the GA group were higher than in the SA group at all times. However, there was no statistically significant difference between the two groups (Fig. 1).
Respiratory rate
The obtained results showed that, except for the baseline and PACU time, the respiratory rates in the GA group were significantly lower than in the SA group (Fig. 2).
End-tidal carbon dioxide
It was shown that there was no difference between the two groups in EtCO2 values during the investigation (p > 0.05) (Supplementary Appendix S3).
Intra-abdominal pressure
IAP was maintained between 8 and 12 in all patients. There was no significant difference between the groups in IAP except at the 55th and 60th minutes and at the end of the operation, at which IAP was significantly lower in the SA group (p < 0.05).
At first glance, the SA group experienced more complications and consequently more medication during surgery than the GA group (Table 1). Hypotension was recorded in 14 patients in the SA group and one in the GA group (p = 0.001). Shortness of breath was observed only in the GA group (three patients) and not in the SA group. By contrast, nausea and/or vomiting occurred only in the SA group (3 vs. 0). A total of 29 patients in the SA group and 3 in the GA group experienced shoulder pain (p < 0.001). Results showed that 32 patients in the SA group experienced notable shoulder pain during surgery (p < 0.001). Mild shoulder pain with the severity of less than 4/10 was reported in four patients in the SA group. Two patients in the SA group experienced severe shoulder pain with a severity of 8/10 and 10/10, respectively. Two patients in the SA group had no shoulder pain. The results showed that the frequency of use of ephedrine, fentanyl, midazolam, propofol, and ondansetron in the SA group was significantly higher than in the GA group (Table 2).
Frequency of Complications During Surgery and Its Comparison Between Two Anesthesia Techniques
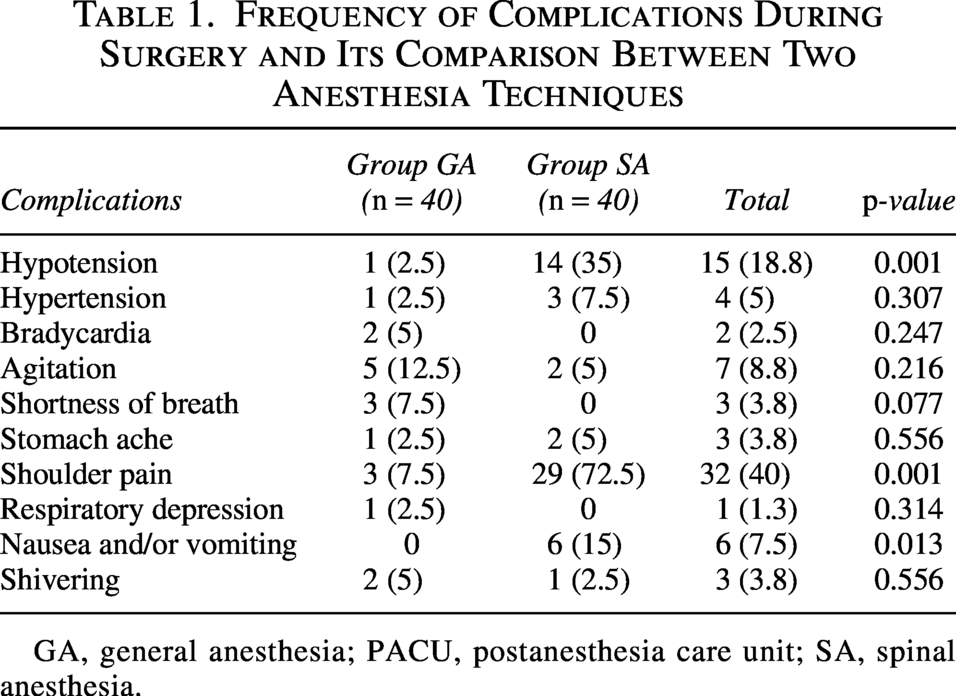
GA, general anesthesia; PACU, postanesthesia care unit; SA, spinal anesthesia.
Comparison of PACU Complications Between Two Anesthesia Techniques

There were no shortness of breath and hypertension in both groups.
GA, general anesthesia; PACU, postanesthesia care unit; SA, spinal anesthesia.
There was no significant difference between the groups in some complications such as hypertension, bradycardia, restlessness, dyspnea, abdominal pain, respiratory depression, and chills.
Variables related to the PACU were also recorded from the G and SA groups (Table 2). The frequency of complications during PACU, including agitation and shivering, was significantly higher in GA group patients than in SA group (p = 0.001, p = 0.004, respectively). The severity of abdominal pain based on the VAS scale in the GA group was also significantly higher than in the SA group (p = 0.001). Therefore, there was a significant difference in the medications used in PACU between the two groups (p < 0.001). The SA group patients did not use any medications, but most of the GA group patients used drugs in this manner: 18 patients used pethidine, 12 patients used fentanyl, and three patients used fentanyl and ondansetron. This conversely correlates with the drug consumption during surgery shown in Table 1. Restlessness was another common complication that was recorded only in 15 patients of the GA group (p = 0.001). The full recovery time in PACU was also significantly (p = 0.001) higher in GA group patients than in SA group (Supplementary Appendix S4). The other PACU-related variable is the Ramsay scale, which significantly differs between the groups (p < 0.001). In the GA group, 16 patients were in grade 1, and the 24 other patients were in grade 2, while all 40 patients in the SA group were assessed in grade 1 of the Ramsay scale. The other measured variable is the degree of sedation, a five-level variable from 0 to 4, which differs significantly between the groups (p < 0.001). The group G patients were distributed across all five levels in this manner: 5 patients in level 0, 5 patients in level 1, 12 patients in level 2, 9 patients in level 3, and 9 patients in level 4. There were no patients in level 3 and level 4 in the SA group, while we had 9 patients in level 0, 29 in level 1, and 2 in level 2. Hypertension and vomiting were also documented as complications in PACU, but there was no significant difference between the two groups.
The satisfaction status of the surgeon and the patient after surgery is shown in (Table 3). The complete satisfaction of the surgeon was significantly higher in the GA group than in the SA group (p = 0.001), but no difference was observed between the two groups in terms of patient satisfaction.
Satisfaction Status of Surgeon and Patient after Surgery and Its Comparison between Two Groups

GA, general anesthesia; SA, spinal anesthesia.
Discussion
Laparoscopy is a surgical technique that is characterized by its minimally invasive nature. This procedure has been shown to provide several postoperative advantages, such as reduced surgical trauma, decreased pain, improved pulmonary function, faster recovery, and shorter hospitalization periods. 10 Laparoscopic treatments are increasingly preferred over laparotomies in clinical practice. 11 Laparoscopic surgeries are often carried out under GA. In this new age of minimally invasive surgery, regional anesthesia had not yet acquired popularity and was not favored as the first option in gynecological laparoscopic operations.
According to the literature, regional anesthesia is seen as a more acceptable alternative to GA in diagnostic laparoscopic general surgery and laparoscopic cholecystectomies. 2 Most research on SA in laparoscopic surgery focuses on laparoscopic cholecystectomy, with rare appendectomy and hysterectomy occurrences.12,13 Pneumoperitoneum, which is thought to be poorly tolerated by patients who are awake throughout the surgery, and the Trendelenburg position may be the primary causes of this withdrawal, respectively. Gynecological laparoscopic surgeries differ from laparoscopic cholecystectomy because it necessitate a reverse Trendelenburg posture, which results in better pulmonary dynamics.
On the other hand, the Trendelenburg position raises issues with pulmonary compliance, making it more difficult to control the ensuing hypercarbia.14,15 An ideal anesthetic technique would provide the best possible surgical circumstances without endangering the body’s physiology or metabolism, maintain hemodynamic equilibrium, and ensure a speedy and safe recovery after surgery.16,17 As a result, a technique that offers comparable hemodynamic parameters is considered advantageous. Consistent with the findings of the present study, a retrospective cohort study was conducted among 82 women divided into two groups (SA and GA). Patients underwent elective or emergency laparoscopic salpingectomy for ectopic tubal and/or ovarian pregnancy. Findings of this study indicated that patients who underwent SA had a faster resumption of bowel motility and earlier mobilization, shorter hospitalization, and greater satisfaction compared with GA. 18 There is disagreement on the respiratory criteria for SA and GA during laparoscopic surgery. It has been shown that spontaneous physiological respiration during SA performs better than aided respiration during GA. 19 Numerous studies have indicated that mid-thoracic levels of SA result in either small or minor changes in respiratory function, with clinically significant alterations being minimal. 20 In addition, the study observed minimal alterations in respiratory rate and tidal volume despite a significant degree of blockage with SA. In addition, a slight reduction in vital capacity was noted. 19 Furthermore, it has been observed that pulmonary functions tend to return to their baseline levels within a period of approximately 24 hours following laparoscopic procedures conducted under GA. 21 Our study showed no significant difference in RR between the S and GA groups at the baseline and the recovery stage. However, in other minutes, RR was significantly lower in the GA group.
While hypotension has been observed as an adverse effect in SA, it is a physiological consequence of sympathetic blockage. Furthermore, apart from the hypotension associated with SA, the elevation of IAP caused by the pneumoperitoneum may also contribute to the continuation of hypotension. SA-related hypotension is believed to have greater significance in medical procedures such as laparoscopic cholecystectomy, mainly when performed with the patient in the Fowler position. 22 Sinha et al. conducted a study on a cohort of 4645 patients. 21 A total of 2.992 individuals underwent laparoscopic cholecystectomy, wherein systemic anesthesia (SA) was administered to all patients. Notably, 846 patients (18.21%) exhibited hypotension during the procedure. The decreased incidence of hypotension observed in this study may be attributed to the comparatively low intraperitoneal insufflation pressure, which was maintained within a range of 10–12 mmHg.
In this study, the MAP in the SA group was lower than in the GA group at all times. However, no statistically significant difference was observed between the two groups regarding systolic and diastolic blood pressure. The presence of alert and compliant patients during laparoscopic procedures may be deemed a favorable circumstance intraoperatively, as it facilitates effective communication and expedites the recovery process. Paradoxically, a widespread desire exists to avoid using SA for laparoscopic surgeries. The primary rationale for this withdrawal concerns the potential negative consequences associated with pneumoperitoneum, which may not be well-tolerated by an awake patient undergoing the procedure. Using the Trendelenburg position during gynecological laparoscopy has resulted in an elevation of infra-diaphragmatic pressure, potentially resulting in decreased arterial blood oxygenation (O2 Sat), increased EtCO2 pressure and pain perception. 22
This study showed that 32 patients in the SA group experienced shoulder pain during surgery (p < 0.001). Mild shoulder pain, with a severity of less than 4/10, was reported in four patients in the SA group. Two patients in the SA group experienced severe shoulder pain, with severities of 8/10 and 10/10, respectively. Regarding arterial O2 saturation and end-tidal CO2 pressure, there were no statistically significant differences between the two.
A significant constraint restricting SA adoption in laparoscopic surgery pertains to patient comfort and satisfaction. Most studies in the literature solely assessed subjective assessment (SA), and patients were predominantly reported to have expressed satisfaction.21,23,24 In our study, all patients in the GA group were highly satisfied, but the satisfaction rate was “High” in 21 patients in the SA group. Theoretically, no patient can compare both anesthetic techniques because no one ever steps in the same river twice.
One of the significant challenges encountered during laparoscopic surgery under SA is insufficient relaxation of the abdominal muscles. One of the foremost issues surgeons encounter in all abdominal surgical procedures is the discussed problem. In a study, surgeons who conducted laparoscopic cholecystectomies using SA were surveyed for their views. The results indicated that all surgeons were in agreement that this anesthetic technique was satisfactory, providing adequate abdominal relaxation for surgery, and that they did not encounter any issues related to the anesthetic technique. 23 Nonetheless, the occurrence of right shoulder pain was identified as a drawback of SA administration, leading to elevated IAP that restricted laparoscopic examination.13,23 However, the laparoscopic surgery was executed without any complications after alleviating shoulder pain during the operation. 25
The results of the present study demonstrated that in laparoscopic surgery with GA, the satisfaction level of surgeons was evaluated as “High” for 35 patients and as “Low” for 5 patients, while in the operations with the other method, laparoscopic surgery with SA, the surgeons’ satisfaction level was “High” for 36 patients and “Low” for only four patients after alleviating shoulder pain. In the current epoch of minimally invasive surgical procedures, it is imperative that anesthetic methodologies mitigate the deleterious effects of surgical stress on organisms, minimize the incidence of postoperative complications arising from anesthesia and surgery, and enhance the comfort levels of both patients and surgeons. Furthermore, in this “new normal” age after the 2019 coronavirus epidemic, one may provide their opinion on the preventive benefits of SA compared with GA for all operating room personnel, including surgeons, anesthetists, and others. The utilization of SA in gynecological laparoscopy may present itself as a viable and less intrusive substitute for GA, provided that comparable or superior attributes in relation to hemodynamic and respiratory parameters, contentment of both patient and surgeon, and overall levels of oxidants, antioxidants, and oxidative stress indices are taken into account. It is apparent that additional randomized prospective studies on a large scale are necessary to establish conclusive evidence supporting the customary utilization of this technique, which is both safe and accommodating to patients.
One of the strong points of this research has been conducting and investigating this method in women’s laparoscopic surgery. Unfortunately, this research could not be generalized to major surgeries, including patients with extensive endometriosis. It is suggested to conduct another similar study with a larger sample size and on patients who need major surgeries, including endometriosis.
Limitations
This trial compared two anesthesia methods, including SA and GA. However, our study had some limitations. The “regional anesthesia” arm may be described as SA combined with sedation, given the substantial use of opioids and sedatives. Although SA is distinct from regional anesthesia, these similarities should be considered for accurate interpretation and comparison. We also sought to mitigate this issue; participants in both groups were comparable in demographic characteristics, medical and surgical history, and grade, and we used a random assignment method to ensure that the groups were randomly allocated.
Conclusion
Although SA and GA showed no significant differences, SA appears more satisfactory for gynecological surgeons performing laparoscopic procedures. However, the best anesthesia choice depends largely on the type of surgery and the patient’s condition.
Authors confirm that our research is supported by an institution that is primarily involved in education or research. The authors are exclusively involved in research and educational activities.
Authors’ Contributions
F.T. registered, collected, and analyzed the data and wrote the main article text. H.A. and S.T.N. collected data, analyzed, interpreted, contributed to the protocol development. H.A., F.T., S.T.-N.H., and R.V. helped with the study design, and edited the article. F.T., R.V., and S.T.-N.H. supervised the study, revised the article critically. All authors read and approved the final article.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude for the statistical support provided by the “Clinical Research Development Unit of Al-Zahra Hospital” at Tabriz University of Medical Sciences.
Author Disclosure Statement
The authors declare that there is no conflict of interests.
Funding Information
Tabriz University of Medical Sciences has financially supported this study.
Ethics Approval and Consent to Participate
This study has been registered in Iranian Registry of Clinical Trials (IRCT20211103052950N1, 30/01/2022) and approved by the Ethics Committee and Institutional Review Board of the Tabriz University of Medical Sciences, Tabriz, Iran (Code Number: IR.TBZMED.REC.1400.690, 25/10/2021). Each participant gave their informed consent after the faculty ethics council at Tabriz University of Medical Sciences authorized the research.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.