
Abstract
Study Objective:
This study aims to determine if the presence of endometriosis decreases the probability of adnexal torsion. We hypothesize that the presence of endometriosis is associated with a lower risk of ovarian torsion.
Methods:
A retrospective case–control study was performed. Study population included patients who underwent emergent surgery for suspected adnexal torsion from January 2014 to August 2023. The medical record was reviewed to obtain demographic information, preoperative symptoms, patient history, and intraoperative findings. Pathology results were reviewed when applicable. A convenience sample was utilized due to limited number of cases. A post hoc power analysis was calculated.
Results:
A total of 160 patients underwent surgery for suspected adnexal torsion, with 118 (73.8%) found to have torsion, while 42 (26.2%) did not. Preoperative history of endometriosis was associated with lower torsion risk (odds ratio [OR] = 0.30, 95% confidence interval [CI]: 0.11–0.77). Endometriomas were not found in any of the torsion cases compared with 5 (11.9%) of the nontorsion cases (p = 0.001). Intraoperative findings suggestive of endometriosis in the torsion group were superficial without ovarian involvement. Adhesions between the adnexa and the pelvic side wall were linked to lower torsion risk (OR = 0.06, 95% CI: 0.02–0.17).
Conclusion:
A preoperative diagnosis of endometriosis was associated with lower odds of having adnexal torsion. Furthermore, five (3%) endometriomas were found in total, all in nontorsion patients. Our data show that patients with endometriosis have a lower risk of adnexal torsion, particularly if they have ovarian involvement. The presence of pelvic adhesions between the adnexa and pelvic side wall was also associated with a lower risk of adnexal torsion.
Introduction
Adnexal torsion is a surgical emergency that occurs when the ovary or fallopian tube twists around its vascular supply, limiting appropriate blood flow to the organ. The true incidence of adnexal torsion is unknown, as it is a surgical diagnosis; however, recent emergency department data estimates the incidence of ovarian torsion in the United States to be 157.4 per 100,000 women. 1 Additional population-level data indicate increasing rates of annual emergency department visits for adnexal torsion in women aged 18–65, which rose from 2791 in 2006 to 5243 in 2018. 2 In a cohort study performed with 291 children and adolescents who underwent surgery for suspected adnexal torsion, torsion was confirmed in 57.7% cases. 3 Clinical presentations and recognized risk factors are similar between both pediatric and adult patients and include ovulation induction, history of previous torsion, pregnancy, and ovarian cyst.4,5 Although the literature reports features for radiological identification, including asymmetrical ovarian enlargement, peripheralized follicles, free fluid, the “whirlpool sign”—or a twisted vascular pedicle, abnormal ovarian location, and uterine tilting, preoperative diagnosis of torsion is consistently challenging because ultrasound with Doppler is unreliable and symptoms are nonspecific.6,7 As a result, a low threshold for diagnostic laparoscopy is essential to prevent possible ovarian loss in premenopausal patients desiring future fertility.
Endometriosis is a common cause of severe abdominal and pelvic pain in reproductive-age females. The incidence of endometriosis is estimated to be up to 10% of all females and 50%–60% of those with pelvic pain. 8 Acute onset of lower abdominal pain caused by endometriosis can mimic the symptomatology of adnexal torsion. 9 However, endometriosis is known to cause pelvic adhesions between the adnexa, pelvic side walls, and/or uterus. 10 The revised American Society of Reproductive Medicine Classification highlights the critical role of adhesions in endometriosis as they strongly influence the score. 11 As a result, patients with endometriosis may be at lower risk of torsion and therefore not require emergent surgical intervention. A retrospective cohort study in 2019 reported on intraoperative findings during surgery for pelvic pain in patients with confirmed endometriomas, with 23% of the cases performed emergently due to concern for torsion. 12 None of these cases had findings consistent with torsion, and all had pathology-confirmed endometriosis. 13
More studies are necessary to better understand the connection between acute lower abdominal pain, endometriosis, and the subsequent intraoperative findings. We aim to fill this gap so providers can optimize surgical planning in these patients. The primary objective of this study is to determine if there is an association between endometriosis and ovarian torsion. Secondary objectives include determining if prior surgery, prior pelvic disorders, and intraoperative findings such as pelvic adhesions also impacted torsion risk. We hypothesize that the presence of endometriosis is associated with a lower risk of ovarian torsion.
Methods
This was a retrospective case–control study on patients who underwent emergent surgery for suspected adnexal torsion. The patients with torsion were defined as cases. The patients without torsion were defined as controls. All surgical cases took place at an academic tertiary care hospital and two affiliated community hospitals between January 2014 and August 2023. A convenience sample was used due to the limited number of cases available. A post hoc power calculation was performed.
Informatics for integrating biology and the bedside (i2B2), a program that organizes data from the electronic medical record (EMR), was used to identify potential patients using age, date range, visit context, and International Classification of Diseases (ICD) 9 and 10 codes were selected as conditions to generate a list. ICD-9 and ICD-10 codes for torsion of ovary, ovarian pedicle, or fallopian tube were selected. Inclusion criteria were patients 18 years of age and older who underwent surgical exploration for suspected adnexal torsion performed either directly from the emergency department or directly from the clinic by any gynecological surgeon during the included timeframe. Exclusion criteria included any patient who underwent urgent surgical exploration for another suspected cause, such as ectopic pregnancy, ruptured ovarian cyst, or any other diagnosis not consistent with adnexal torsion. Patients who were found to have adnexal torsion during a scheduled or emergent surgery for indications other than suspicion of ovarian torsion were also excluded.
Clinical characteristics gathered included self-reported demographic information, body mass index, tobacco use, preoperative diagnoses, pain quality, nausea/emesis, laterality of pain, length of pain, location of pain, and surgical history. Patients were considered to have preoperative endometriosis if patient self-reported it during the emergency room visit, if it was reported in a prior gynecological or primary care appointment, or if the patient had a prior laparoscopy with documented signs of endometriosis. Prior pelvic surgeries included hysterectomy, appendectomy, cystectomy, tubal ligation, salpingectomy, oophorectomy, excision of endometriosis, detorsion, and oophoropexy.
Intraoperative findings were broken down into broad categories based on operative reports. These categories included fallopian tube torsion, endometriosis, adhesions to the abdominal wall, endometrioma, dermoid cyst, hemorrhagic cyst, other types of cysts, ruptured cysts, hemoperitoneum, adhesions to pelvic side wall, tuboovarian abscess, and appendicitis. Patients were considered to have intraoperative endometriosis if they had intraoperative findings consistent with endometriosis based on operative report or a histological diagnosis, if present. We could not depend on pathology for the diagnosis of cysts and/or endometriosis because not every case excised a specimen for pathological confirmation.
Data were presented as n (%) and odds ratios (OR) with a 95% confidence interval (CI). Chi-square or Fisher’s exact tests were performed to compare categorical variables as appropriate, and nonparametric rank sum tests were used to compare continuous variables. A post hoc power analysis was calculated. Statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC). This study was approved by the Medical College of Wisconsin institutional review board, and all policies were followed.
Results
Our data collection identified 378 possible patients, and after application of inclusion and exclusion criteria, a total of 160 patients underwent urgent surgical exploration for suspected adnexal torsion and were included in this study. Of these, 118 (73.8%) were confirmed to have torsion, while 42 (26.2%) did not. Demographics, presenting symptoms, and surgical history are shown in Table 1. The baseline characteristics between the two groups were largely similar except for a higher current smoking rate (n = 11 [26.2%] vs. n = 12 [10.2%], p < .001) in the group without torsion. There was no difference in prior hysterectomy or prior pelvic surgery between the two groups. When comparing the type of hysterectomy, more patients in the no torsion group underwent an abdominal hysterectomy (n = 4 [9.5%]) compared with the torsion group (n = 1 [0.8%]), which had more minimally invasive routes, including laparoscopic and vaginal. There was no difference in the length of pain prior to presentation between the two groups. Significantly more patients in the torsion group reported nausea with emesis (n = 84 [71.2%] vs. n = 18 [42.9%], p = 0.002).
Patient Characteristics
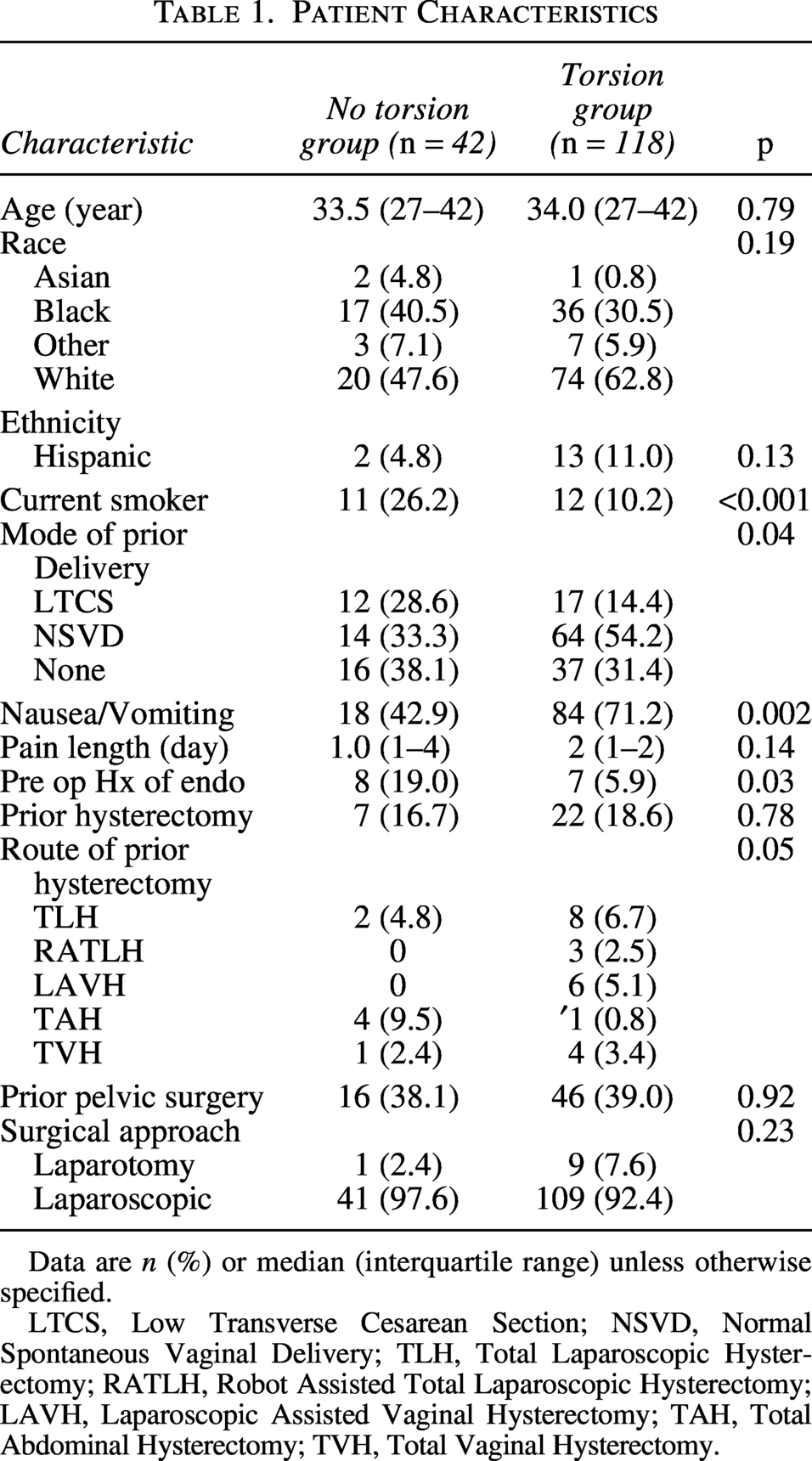
Data are n (%) or median (interquartile range) unless otherwise specified.
LTCS, Low Transverse Cesarean Section; NSVD, Normal Spontaneous Vaginal Delivery; TLH, Total Laparoscopic Hysterectomy; RATLH, Robot Assisted Total Laparoscopic Hysterectomy; LAVH, Laparoscopic Assisted Vaginal Hysterectomy; TAH, Total Abdominal Hysterectomy; TVH, Total Vaginal Hysterectomy.
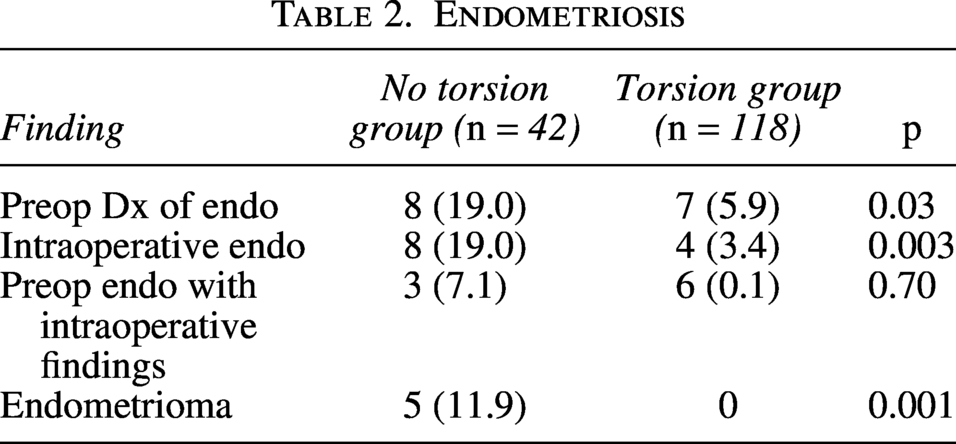
As seen in Table 2, preoperative history of endometriosis was associated with lower torsion risk (OR = 0.30, 95% CI: 0.11–0.77). There were no endometriomas found on pathology in the torsion group compared with five in the no torsion group (OR = 0.30, 95% CI: 0.01–0.53). These two findings support our hypothesis that patients with endometriosis are less likely to have surgically confirmed adnexal torsion. A post hoc power analysis was performed based on the observed effect size and sample size of our primary outcome. For an alpha of 0.05, the study has a power of 67%. Although our study did not have adequate power due to the limited sample available, it is an important preliminary step to guide further research.
Endometriosis
Intraoperative findings suggestive of endometriosis occurred more in the no torsion group (n = 8 [19.0%] vs. n = 4 [3.4%], p = 0.003). The intraoperative findings are shown in Table 3. Adhesions to the pelvic side wall were found in half of the cases without torsion (n = 21 [50.0%] vs. n = 7 [5.9%], p = 0.001) and were linked to a lower risk of torsion as well (OR = 0.06, 95% CI: 0.02–0.17). Seven out of the 21 patients with pelvic adhesions were reported to be due to endometriosis in the no torsion group compared with 1 out of 7 in the torsion group (OR = 0.04, 95% CI: 0.01–0.36). The remaining cases of pelvic adhesions without a diagnosis of endometriosis were still linked to a lower risk of torsion (OR = 0.12, 95% CI: 0.04–0.30).
Intraoperative Findings
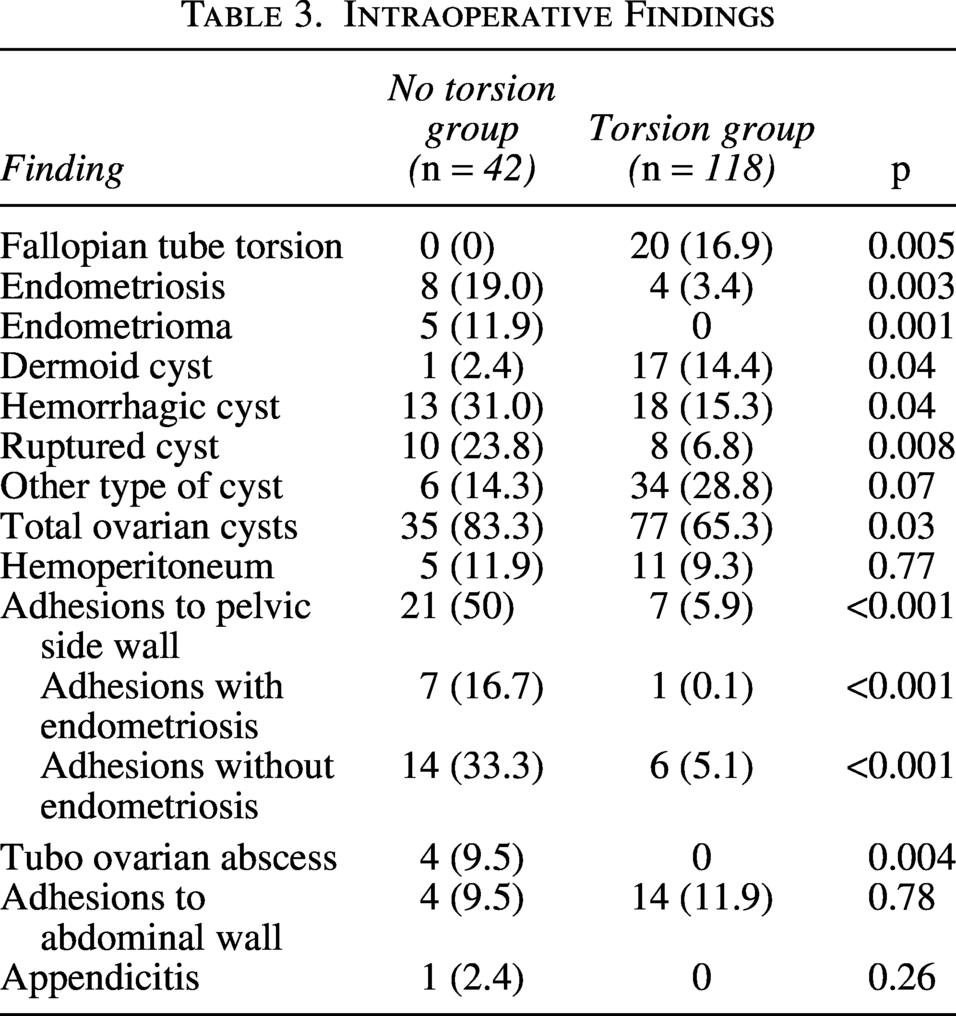
Ovarian cysts were reported more in the no torsion group (n = 35 [83.3%] vs. n = 77 [65.3%], p = 0.03). When cysts were broken down according to type, dermoid cysts (n = 17 [14.4%] vs. n = 1 [2.4%], p = 0.04) were reported more in the torsion group, while hemorrhagic cysts (n = 18 [15.3%] vs. n = 13 [31.0%], p = .04), ruptured cysts (n = 8 [6.8%] vs. n = 10 [23.8%], p = .008), and tuboovarian abscesses (n = 0 [0%] vs. n = 4 [9.5%], p = 0.004) were found more often in the no torsion group. The torsion cases had a higher rate of both cystectomy (n = 64 [54.2%] vs. n = 18 [42.9%]) and oophorectomy (n = 32 [27.1%] vs. n = 6 [14.3%]).
Discussion
We present a retrospective case–control study on rates of adnexal torsion and endometriosis in patients who underwent urgent surgical exploration for suspected adnexal torsion in both academic and community-based hospitals. A preoperative diagnosis of endometriosis was associated with a lower risk of intraoperative adnexal torsion. Furthermore, no cases of adnexal torsion were found to have an endometrioma. This supports our hypothesis that patients with endometriosis are less likely to have surgically confirmed adnexal torsion.
Endometriosis was more likely to be found intraoperatively and on pathology in patients without torsion. In patients who had both endometriosis and torsion, the endometriosis was identified as superficial implants. It is important to recognize that endometriosis may have been missed in patients with torsion if the surgeon did not survey the entire pelvis for additional causes of pain. Ovarian involvement with endometriosis may be required to reduce torsion risk since the ovaries often become densely adherent to the pelvic side wall and ultimately immobile. Our findings are congruent with a group study from 2019 that showed zero cases of histologically confirmed endometrioma in patients found to have adnexal torsion during emergency surgery. 13
Half of the cases without torsion were found to have adhesions between the ovaries and the pelvic side wall. These cases were separated out between those with adhesions and endometriosis versus those with adhesions of unclear etiology. No matter the etiology, pelvic adhesions were still associated with a statistically significantly lower risk of adnexal torsion. This is also consistent with the same study from 2019 that showed adhesions present in 56% of patients with known endometriosis and no evidence of torsion who underwent emergency surgery due to pain. 13 In our study, these adhesions could be secondary to prior hysterectomy, pelvic surgery, history of pelvic inflammatory disease, or other pelvic infection. Although none of the above were found to be protective of torsion in this study, it is important to take a focused history that incorporates all possible causes of pelvic adhesions.
Characterization of the ovarian cyst is also an important clinical factor when considering a diagnosis of adnexal torsion. Studies have previously shown that teratomas, follicular cysts, paratubal cysts, and serous cysts are known risk factors for ovarian torsion. 14 Findings associated with these cysts would raise a provider’s clinical suspicion. On the other hand, findings on ultrasound consistent with an endometrioma, such as unilocular or multilocular cysts with ground glass opacities or low-level echoes, should cause a provider to consider the possibility of the presence of endometriosis. 15 Based on the findings of our study and previous studies, if a patient has acute pelvic pain with an ultrasound finding favoring an endometrioma, urgent surgery may not be necessary. A referral to an endometriosis specialist should be provided to allow for specialized care and improved surgical planning based on the patient’s goals. If endometriosis is found during an emergent case and torsion has been ruled out, it may be in the patient’s best interest to end the case to allow for referral and optimal surgical results in the future.
Our study has multiple limitations. We only collected data from a single academic system with one large academic tertiary center and two associated community sites. We did not have a large sample size despite reviewing nearly a decade of patient charts, and thus the study is underpowered for our primary outcome. The identification of our charts to review depended on the diagnosis code for adnexal torsion. It is very plausible that several surgical explorations went unreviewed if the diagnosis code was never associated with the patient. On the other hand, ICD codes could have been associated with a patient even if it was not the leading clinical diagnosis at the time. We reduced this chance by confirming that adnexal torsion was the leading diagnosis and main concern prompting emergent surgical intervention based on clinical documentation. We did not include patients under 18, even though adolescence is a risk factor for torsion, because all pediatric patients are transferred outside of our academic system. Despite all the above, we believe these data are still an important step toward better understanding the relationship between endometriosis and adnexal torsion.
Additionally, there are limitations due to the challenge of diagnosing endometriosis. We did not confirm preoperative diagnosis of endometriosis with histology. Rather, it was found in the patient chart in either a clinical note, problem list, past medical history, or past operative report. Professional societies, such as the European Society of Human Reproduction and Embryology, have emphasized the importance of broadening the diagnostic criteria of endometriosis to include both clinical and surgical diagnoses, even with negative histology. 16 Our definition of preoperative endometriosis is reflective of the clinical information a provider will likely have at time of emergency department evaluation. We felt it was inclusive of different diagnostic methods and reflected clinical practice. On the other hand, chart review was also limited to one EMR. Patients could have had previously documented endometriosis that was not accessible.
Not all the cases with intraoperative findings suggestive of endometriosis had a biopsy submitted for histological review. We believe this was due to two factors: Surgeon comfort with peritoneal biopsy and lack of surgical specimen if no excision of tissue was indicated or planned during surgery. Similarly, some ovarian cysts were also diagnosed visually without histological confirmation. If an endometrioma was misdiagnosed as a hemorrhagic cyst, this could have contributed to an underestimation of intraoperative endometriosis. In the future, prospective studies should require biopsies of cysts to overcome these challenges.
We acknowledge that there may be a sampling bias inherent to the study design. However, we believe that the providers in this study are a good representation of standard clinical practice at the time of the review.
Conclusions
Overall, our data show that patients with endometriosis have a lower risk of adnexal torsion, particularly if they have ovarian involvement. The presence of pelvic adhesions between the adnexa, pelvic side wall, and uterus was also associated with a lower risk of adnexal torsion regardless of the adhesion etiology. Moving forward, providers should consider taking a focused history and asking directly about dysmenorrhea, pelvic pain, history of pelvic infections, and endometriosis when considering adnexal torsion on differential diagnosis. Furthermore, clarification between acute pelvic pain versus acute-on-chronic pelvic pain would provide critical clinical information to help distinguish between patients who may have an acute pain flare due to endometriosis versus those with torsion. This study is an important step forward toward understanding the role endometriosis may play in acute pelvic pain.
Authors’ Contributions
C.P.: Conceptualization, methodology, investigation, analysis, and writing. M.S.: Investigation and writing. B.B.: Conceptualization, methodology, and writing—review and editing.
Footnotes
Author Disclosure Statement
B.B. has received a past grant from Pfizer. The other authors have no conflicts of interest to disclose.
Funding Information
No funding received for this article.