
Abstract
Aim:
To evaluate perioperative antithrombotic management strategies and their effects on hemoglobin change and postoperative outcomes in women undergoing gynecologic surgery.
Methods:
This retrospective study included women aged ≥18 years who underwent gynecologic surgery while receiving long-term antithrombotic therapy between December 2022 and December 2024. Patients were categorized according to perioperative management strategies, including continuation, temporary interruption, or bridging. The primary outcome was perioperative hemoglobin change and the need for blood transfusion. Secondary outcomes included thromboembolic events, surgical complications, and intensive care unit admission. Statistical analysis was performed using nonparametric and categorical tests, with a significance threshold of p < 0.05.
Results:
Seventy-three women were included. The mean age was 59.5 years, and obesity and hypertension were common. Most surgeries were classified as high bleeding risk. Hemoglobin values were available for 59 patients. Hemoglobin decrease ranged from minimal change in the bridging group to greater declines in those with prolonged interruption, but no statistically significant difference was identified among management strategies. Postoperative complications occurred in 9.6% of patients, including one pulmonary embolism. Three patients required transfusion, and no major cardiovascular events were observed.
Conclusions:
Different perioperative antithrombotic strategies were not associated with statistically significant differences in blood loss or postoperative complications; however, these findings should be interpreted cautiously given the limited sample size and subgroup distribution. The results should be considered hypothesis-generating rather than definitive, and individualized decision-making based on thromboembolic and bleeding risk remains essential in gynecologic surgery.
Keywords
Introduction
Cardiovascular and thromboembolic diseases have become increasingly common in the aging female population, resulting in a substantial rise in the number of women who require long-term antithrombotic therapy. Many patients routinely use aspirin for secondary prevention or clopidogrel following coronary stenting, while others are maintained on direct oral anticoagulants (DOACs) for atrial fibrillation or prior venous thromboembolism.1–3 As life expectancy increases and multimorbidity becomes more prevalent, gynecologic surgeons are encountering a growing subset of patients in whom perioperative antithrombotic management is not simply an adjunct consideration but an essential part of surgical planning.
Gynecologic surgery presents a distinctive challenge in this context. Many procedures involve highly vascular pelvic tissues or mucosal surfaces that inherently carry a heightened risk of bleeding compared with other surgical specialties. Even routine operations, such as hysterectomy or adnexal surgery, may lead to unpredictable blood loss in women using chronic antithrombotic agents.1,2 On the other hand, inappropriate interruption of therapy—particularly in patients with recent coronary stents, mechanical heart valves, or high-risk atrial fibrillation—can significantly elevate the risk of perioperative stroke, valve thrombosis, stent occlusion, or pulmonary embolism.3,4 These competing priorities make perioperative decision-making uniquely complex for gynecologic surgeons.
Although widely used guidelines, most notably the American College of Chest Physicians (CHEST) perioperative antithrombotic guideline, offer general principles regarding the continuation, interruption, or bridging of antithrombotic agents, these recommendations are predominantly based on evidence derived from cardiology, general surgery, or mixed surgical cohorts. 3 Gynecologic surgery patients—particularly those operated on for benign indications—remain underrepresented, which limits the direct applicability of existing guidance. Consequently, perioperative management strategies vary considerably across institutions, often influenced by surgeon preference, anesthesiologist judgment, and local practice patterns rather than gynecology-specific evidence.
Recent studies from abdominal and minimally invasive surgery fields suggest that certain antithrombotic agents, particularly low-dose aspirin, may be continued safely in select patients without increasing major bleeding risk.5,6 Conversely, routine low-molecular-weight heparin bridging—traditionally employed in high-thrombotic-risk patients—has been questioned due to its association with increased perioperative bleeding without a consistent reduction in thromboembolic complications.3,4 However, the extent to which these findings apply to gynecologic surgery remains unclear. In addition, DOAC management in urgent or semi-urgent gynecologic procedures continues to pose practical difficulties, as emphasized by Piran and Schulman. 7
The scarcity of gynecology-specific data creates a meaningful evidence gap. Most available studies focus on oncologic populations or small heterogeneous cohorts, leaving benign gynecologic surgery—where the majority of daily surgical volume lies—relatively underexplored.1,2 As a result, clinicians often rely on extrapolated data or institutional customs rather than discipline-specific evidence. Retrospective analyses, while imperfect, may provide valuable real-world insights and help inform a more nuanced, risk-adapted approach tailored to gynecologic patients.
In this context, the present study aims to evaluate perioperative antithrombotic management strategies among women undergoing gynecologic surgery at a tertiary care center. By examining hemoglobin change, postoperative complications, and comorbidity profiles across different management strategies, we aim to contribute to the limited body of evidence and support safer, more informed perioperative decision-making in this increasingly common clinical scenario.
Methods
This retrospective observational study was conducted at the University of Health Sciences Istanbul Training and Research Hospital, a tertiary referral center performing a wide spectrum of benign and urgent gynecologic surgeries. The study covered a 2-year period between December 2022 and December 2024. Ethical approval was obtained from the institutional Clinical Research Ethics Committee (Decision No: 136, Date: 13.12.2024). All patients admitted to the hospital routinely sign institutional consent forms permitting the use of anonymized clinical data for research purposes.
Study population
Women aged ≥18 years who underwent gynecologic surgery while receiving chronic antithrombotic therapy were eligible for inclusion. Antithrombotic agents included acetylsalicylic acid (ASA), clopidogrel, warfarin, and DOACs, such as apixaban and rivaroxaban. The majority of procedures were elective; however, a limited number of urgent cases (e.g., tubo-ovarian abscess) were also included.
Patients were excluded if they had histopathologically confirmed malignancy, had undergone oncologic staging surgery, were receiving intravenous anticoagulation (heparin), or had incomplete perioperative data. Therefore, all included cases represented non-oncologic (benign) gynecologic procedures.
Patients were also excluded from specific analyses if they had:
missing perioperative hemoglobin measurements (for hemoglobin-related analyses), procedures classified as low bleeding risk without recorded postoperative laboratory follow-up, incomplete perioperative documentation regarding antithrombotic status.
Although 73 patients met the general inclusion criteria, perioperative hemoglobin change was analyzed in 59 patients with complete laboratory data. Patients undergoing minor procedures (e.g., diagnostic hysteroscopy, office diagnostic curettage [D&C]) were retained for descriptive assessment of complications but excluded from hemoglobin evaluation due to routine same-day discharge without postoperative blood testing.
All patients were of Turkish ethnicity, and no patients were identified as active smokers in the medical records.
Data collection
Demographic features (age, body mass index [BMI]), comorbidities (hypertension, diabetes mellitus, coronary artery disease, arrhythmia, prior thromboembolism), previous abdominal/pelvic operations, type and indication of antithrombotic therapy, and operative details were extracted from the hospital’s electronic medical record system. Operative notes were reviewed to confirm procedure type, surgical approach, and intraoperative findings. Postoperative outcomes—including complications, transfusion, and intensive care unit (ICU) admission—were documented from inpatient charts.
Perioperative antithrombotic strategies
Patients were categorized into six predefined groups reflecting real-world clinical practice:
Group 0: Antithrombotic therapy continued uninterrupted Group 1: Bridging with low-molecular-weight heparin (LMWH) Group 2: Interruption ≤2 days Group 3: Interruption for 3–5 days Group 4: Interruption ≥5 days Group 5: Interruption status unknown or inconsistently documented.
Bridging criteria (institutional practice)
According to hospital protocol, LMWH bridging was reserved for patients considered to have very high thromboembolic risk, including the following:
mechanical heart valve replacement, venous thromboembolism within the preceding 3 months, CHA2DS2-VASc ≥ 6 (when available), recent coronary stent placement with cardiology recommendation.
Patients outside these categories typically underwent either short-term interruption or continued therapy, depending on bleeding risk and anesthesiology/surgery consensus.
Surgical bleeding risk classification
Procedures were classified using a predefined institutional scale adapted from previously published classifications of procedural bleeding risk in gynecologic surgery.1,2
Moderate bleeding risk
total laparoscopic hysterectomy (TLH) cystectomy or adnexal surgery with limited dissection operative hysteroscopy
High bleeding risk
total abdominal hysterectomy (TAH) vaginal hysterectomy extensive adhesiolysis surgery for tubo-ovarian abscess or pelvic inflammatory disease
Low-risk diagnostic procedures (e.g., D&C, office hysteroscopy) were excluded from hemoglobin-based analysis due to absence of postoperative laboratory monitoring.
Outcome measures
The primary outcome was perioperative hemoglobin change and the need for blood transfusion, calculated as the difference between preoperative hemoglobin and the value measured on postoperative days 1 to 2.
Secondary outcomes included:
postoperative ICU requirement, surgical site infection, ileus, relaparotomy, wound dehiscence, thromboembolic complications (deep vein thrombosis, pulmonary embolism, stroke) during the same admission.
Management of missing data
Cases lacking postoperative hemoglobin measurements—primarily minor procedures discharged on the same day—were excluded from hemoglobin analysis but retained for descriptive postoperative complication evaluation. No imputation methods were applied, as missingness was nonrandom and procedure-dependent.
Statistical analysis
Statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were assessed for normality; none met parametric assumptions. Therefore, comparisons of hemoglobin change between management groups were conducted using the Kruskal–Wallis test. Categorical variables were compared using chi-square or Fisher’s exact test, as appropriate. A two-sided p-value <0.05 was considered statistically significant.
Results
A total of 73 women receiving chronic antithrombotic therapy underwent gynecologic surgery during the study period. The mean age of the cohort was 59.5 ± 11.2 years (range: 34–84), and the average BMI was 30.4 ± 5.8 kg/m2. Obesity (BMI ≥ 30) was present in 58.9% of patients. Hypertension was the most common comorbidity (65.8%), followed by diabetes mellitus (28.8%) and coronary artery disease (20.5%) (Table 1). Thirty women (41.1%) had a history of prior abdominal or pelvic surgery, and seven patients (9.6%) had previously undergone a major orthopedic operation.
Distribution of Systemic Comorbidities Among Patients
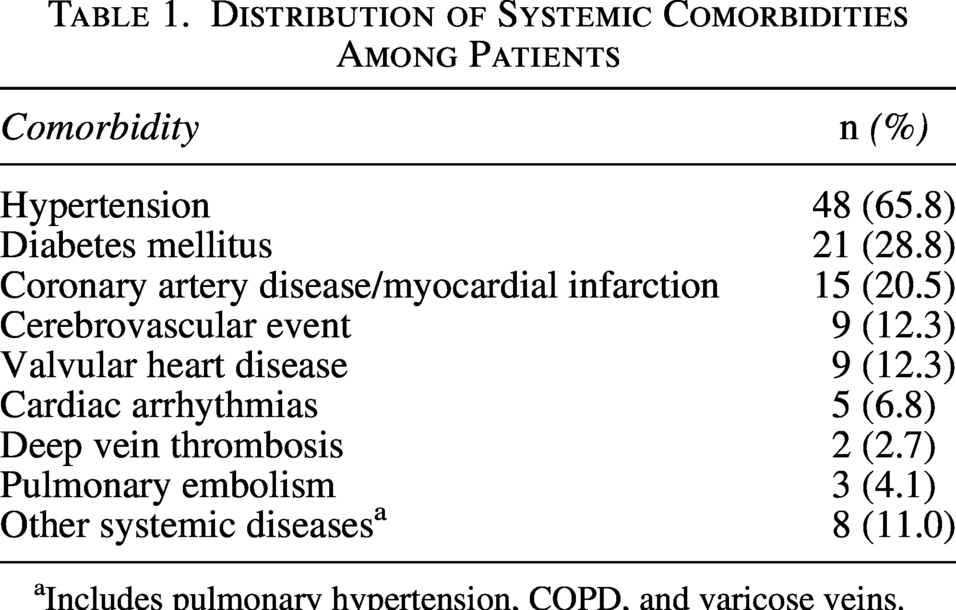
Includes pulmonary hypertension, COPD, and varicose veins.
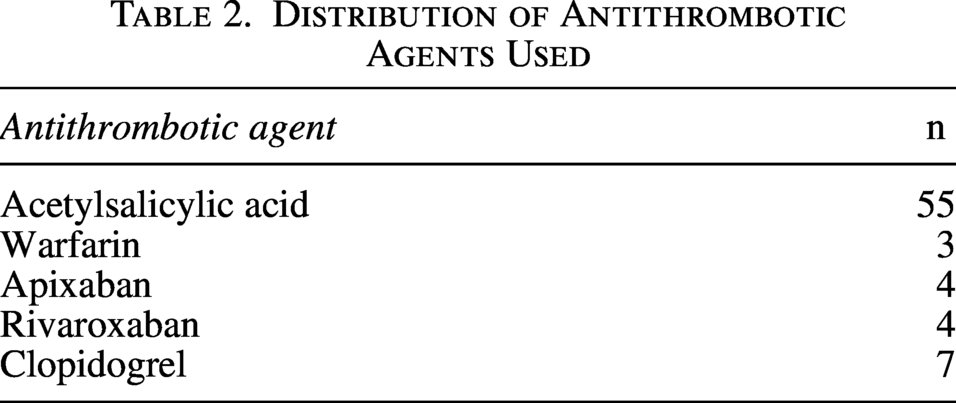
ASA was the predominant antithrombotic agent, used by 55 patients (75.3%). Clopidogrel was used by seven patients (9.6%). Eight women (11.0%) received DOACs (apixaban or rivaroxaban), and three (4.1%) were on long-term warfarin therapy. Each patient was receiving only one antithrombotic agent. Indications included atrial fibrillation, coronary artery disease with stenting, previous thromboembolism, and peripheral vascular disease (Table 2).
Distribution of Antithrombotic Agents Used
A range of gynecologic procedures was performed. The most frequent were TAH, TLH, and dilation and curettage. Other interventions included adnexal surgery (e.g., cystectomy), operative hysteroscopy, and vaginal procedures. Based on institutional criteria, 65.8% of cases were classified as high bleeding risk and 34.2% as moderate risk. Four patients (5.5%) received LMWH bridging therapy (Table 3).
Types of Gynecologic Surgical Procedures Performed
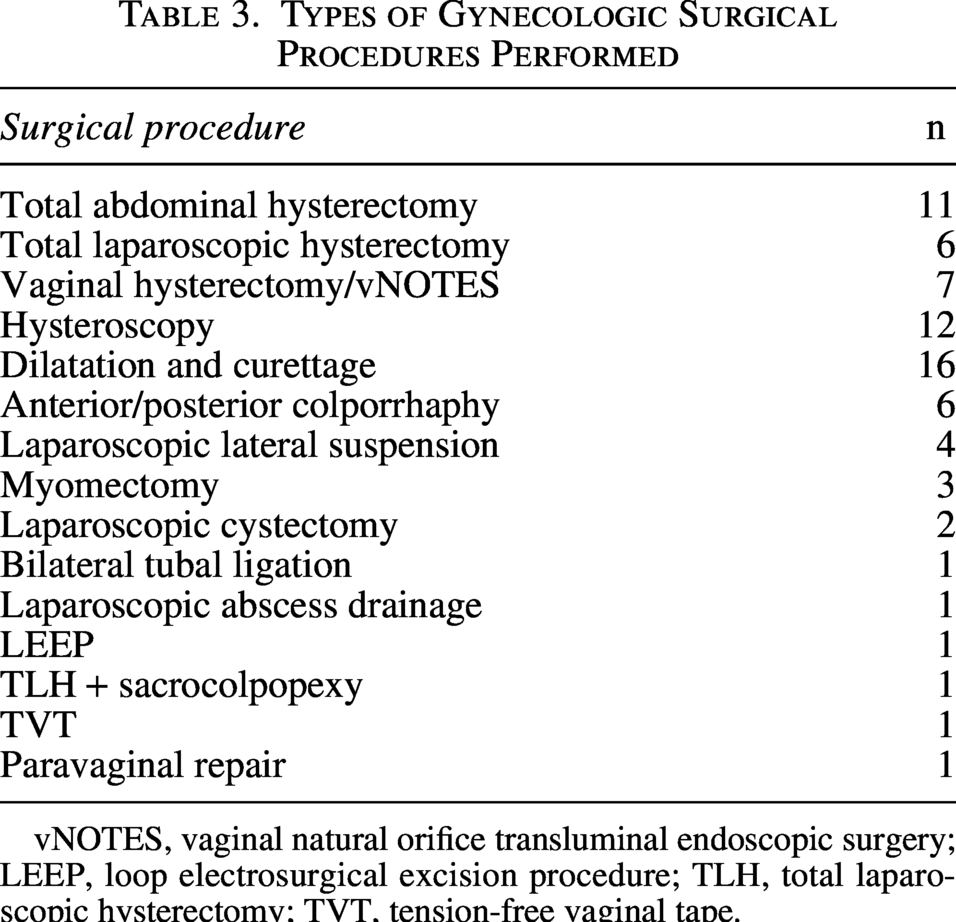
vNOTES, vaginal natural orifice transluminal endoscopic surgery; LEEP, loop electrosurgical excision procedure; TLH, total laparoscopic hysterectomy; TVT, tension-free vaginal tape.
Subgroup sizes were small across several perioperative management categories, particularly in the LMWH bridging and short-interruption groups, which should be considered when interpreting comparative analyses.
Postoperative hemoglobin measurements were available for 59 women. Hemoglobin decline varied across perioperative management groups, ranging from a mean decrease of 0.35 g/dL in the LMWH-bridging group to 1.30 g/dL in the 3–5-day interruption group. The Kruskal–Wallis analysis demonstrated no statistically significant difference in hemoglobin change among the six antithrombotic management strategies (p = 0.999; Table 4). These findings are further summarized in Tables 4 and 5, which present hemoglobin change according to perioperative management strategy and surgical bleeding risk.
Mean Hemoglobin Change by Antithrombotic Strategy
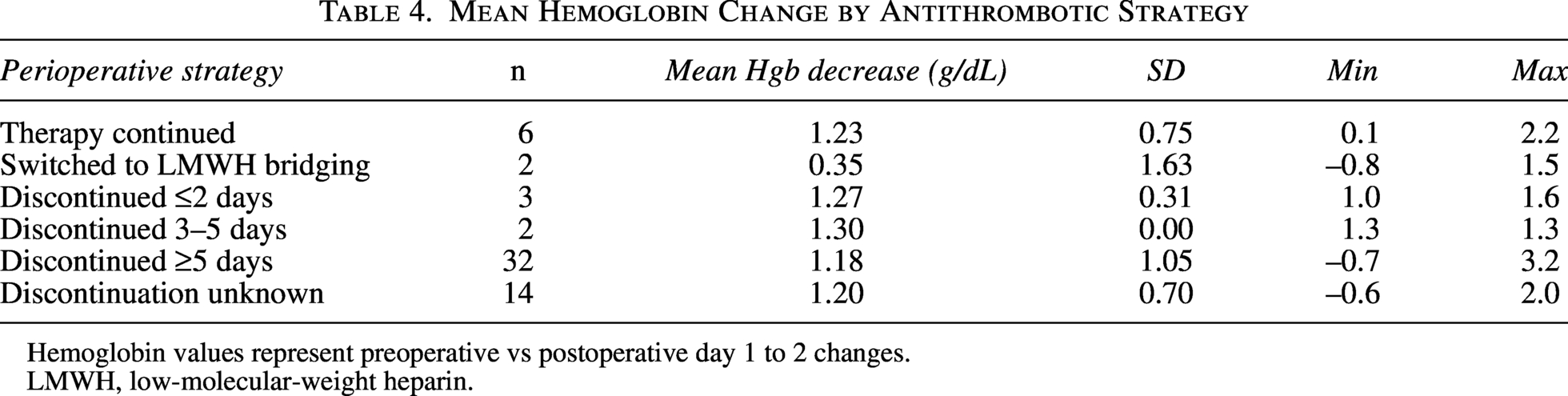
Hemoglobin values represent preoperative vs postoperative day 1 to 2 changes.
LMWH, low-molecular-weight heparin.
Hemoglobin Decline by Surgical Bleeding Risk and Antithrombotic Strategy
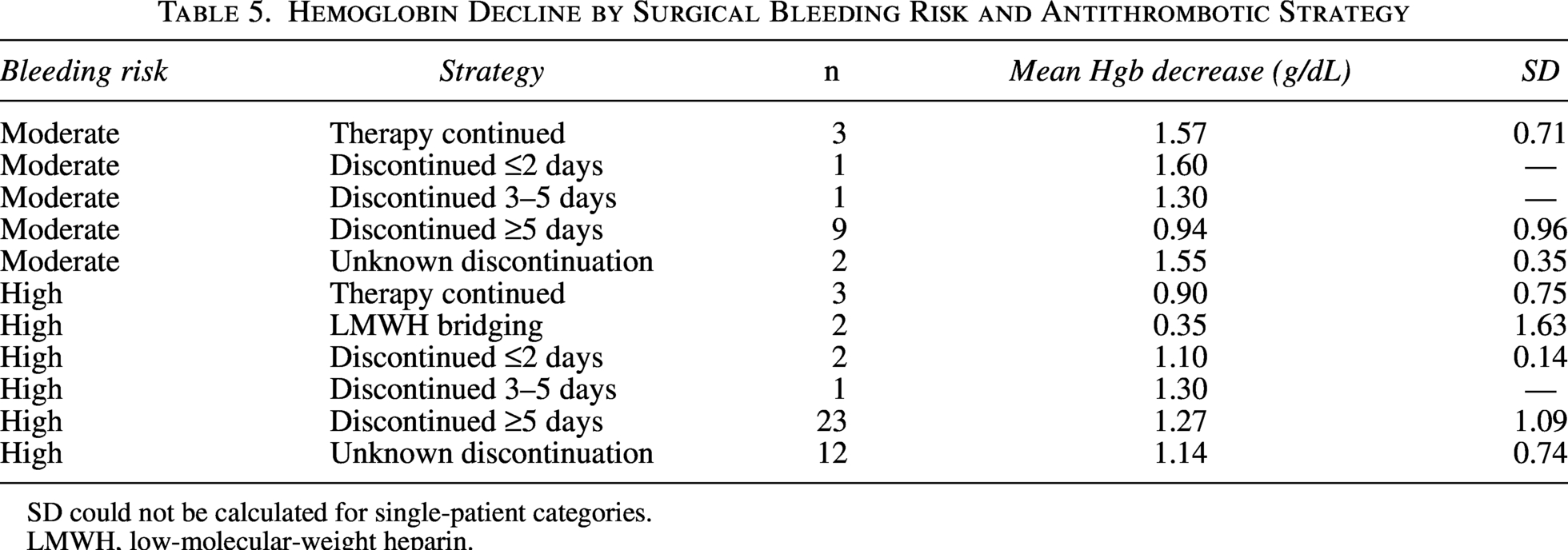
SD could not be calculated for single-patient categories.
LMWH, low-molecular-weight heparin.
When stratified by surgical bleeding risk, patients undergoing moderate-risk procedures showed the greatest variability in hemoglobin decline in the continuation (Group 0) and ≥5-day interruption (Group 4) groups. In high-risk surgeries, hemoglobin decrease was most pronounced in Group 4 (mean 1.40 g/dL, SD 1.14). No statistically significant differences were observed within either bleeding-risk subgroup (Table 5). The distribution of hemoglobin decline in moderate-risk surgeries across the antithrombotic strategy groups is illustrated in Figure 1.
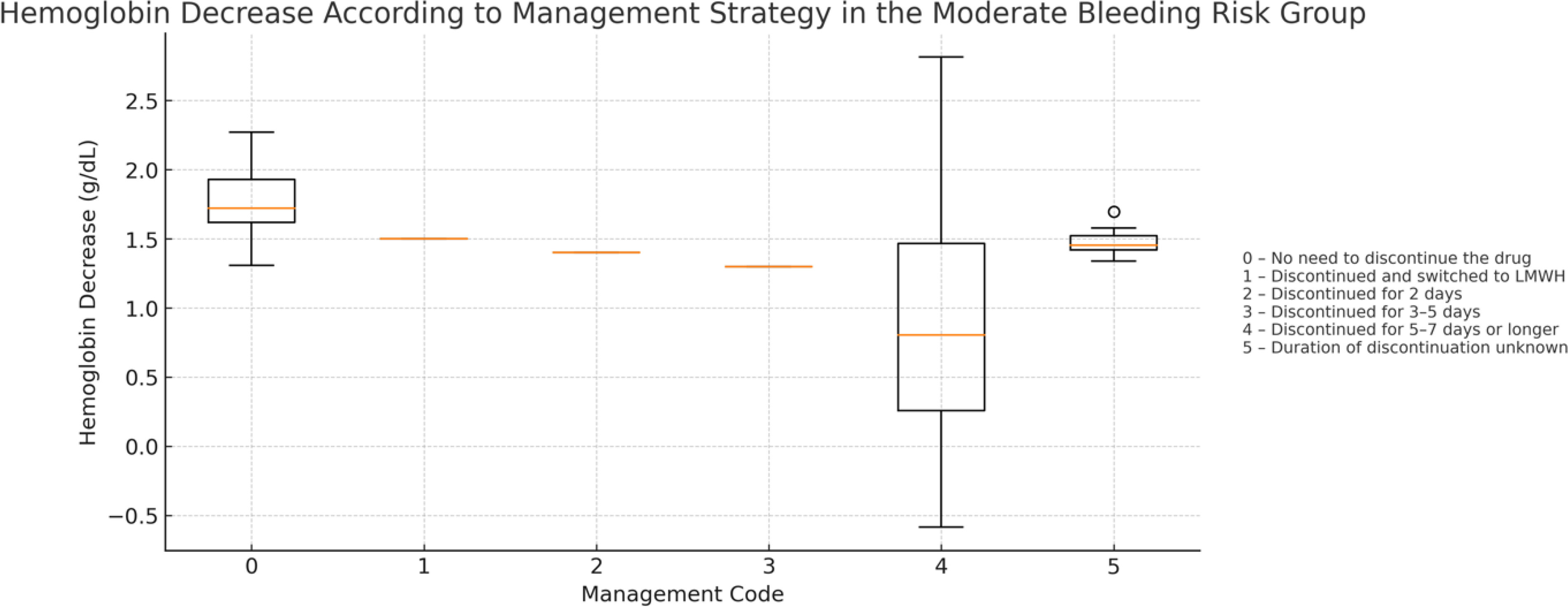
Boxplot of hemoglobin decline in moderate-risk surgeries according to antithrombotic strategy. This figure displays the distribution of hemoglobin decline in moderate-risk gynecologic surgeries across the different perioperative antithrombotic management strategies. Although the Kruskal–Wallis test showed no statistically significant difference (p = 0.306), wider variability in the uninterrupted and ≥5-day discontinuation groups suggests that individualized perioperative assessment may be warranted for patients with higher bleeding variability.
Seven postoperative complications occurred (9.6%). These included one pulmonary embolism, which developed 12 hours after emergency laparoscopic surgery in a patient who continued aspirin perioperatively; this patient was subsequently transitioned to warfarin therapy. Other complications included ileus (n = 1), wound dehiscence requiring relaparotomy (n = 1), and surgical site infections (n = 2). Two patients required postoperative ICU monitoring for hemodynamic instability unrelated to bleeding (Table 6).
Postoperative Complications According to Antithrombotic Strategy
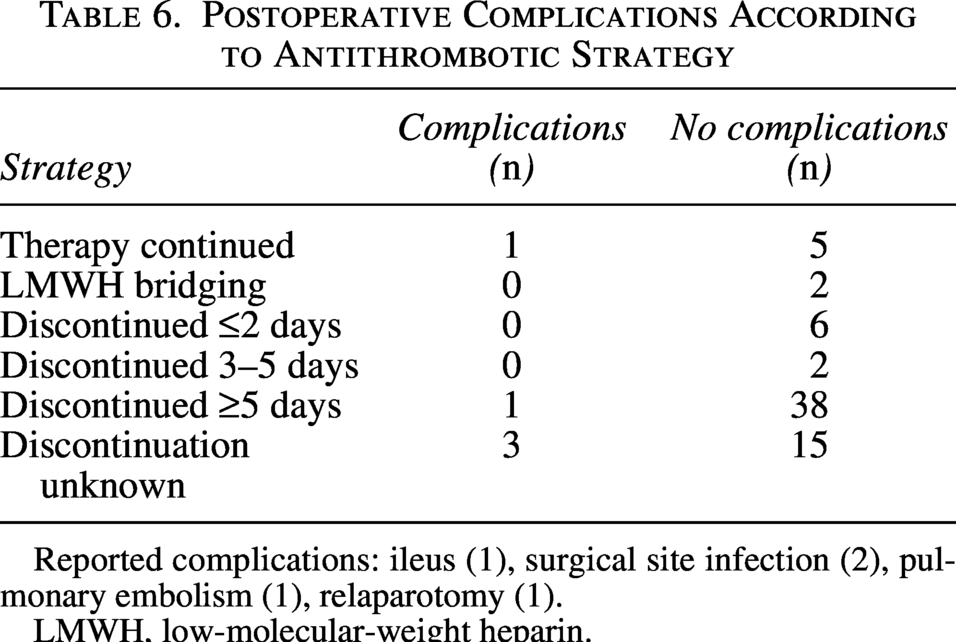
Reported complications: ileus (1), surgical site infection (2), pulmonary embolism (1), relaparotomy (1).
LMWH, low-molecular-weight heparin.
Importantly, no cases of deep vein thrombosis, myocardial infarction, or cerebrovascular events were recorded within 30 days postoperatively.
Fourteen women underwent minor procedures such as diagnostic curettage or office hysteroscopy. As these patients were discharged on the same day and showed no clinical signs of bleeding or complications, postoperative hemoglobin levels were not obtained.
Three patients (4.1%) required red blood cell transfusion, with no statistically significant differences observed between antithrombotic management strategies. Twelve women (16.4%) required postoperative ICU observation, primarily due to advanced age, comorbidity burden, or intraoperative instability rather than antithrombotic management.
Discussion
The perioperative management of antithrombotic therapy in gynecologic surgery remains a clinically challenging area, largely because available recommendations are derived from heterogeneous surgical populations rather than gynecologic cohorts. In this study, we evaluated real-world perioperative strategies in women receiving chronic antithrombotic therapy and found no statistically significant differences in postoperative hemoglobin decline across continuation, short interruption, prolonged interruption, and LMWH-bridging strategies. Although these findings are consistent with several reports suggesting that carefully selected patients may tolerate continued antiplatelet or anticoagulant therapy without excessive bleeding, they should be interpreted with caution due to the retrospective nature and small subgroup sizes.1,2,6 The absence of statistically significant differences should not be interpreted as evidence of equivalence between management strategies. The lack of statistically significant differences observed in this study is likely influenced by limited statistical power, particularly within small subgroups.
Our data showed that hemoglobin variability was greatest in the uninterrupted therapy group and the ≥5-day interruption group. While the absence of a statistically significant difference suggests that no single strategy was clearly superior in terms of blood loss, this pattern highlights the importance of individualized management. As noted in CHEST guidelines and perioperative reviews, bleeding and thromboembolic risks cannot be predicted solely by the duration of interruption but must be considered within the broader context of comorbidity burden, procedure type, and pharmacologic profile.3,4 This is especially relevant in gynecologic surgery, where surgical planes often involve richly vascular pelvic tissues and mucosal surfaces.
Notably, only one thromboembolic event occurred—a postoperative pulmonary embolism in a patient who continued aspirin during an emergency laparoscopic procedure. Given the acute inflammatory nature of tubo-ovarian abscess and the patient’s comorbid profile, this event likely reflects multifactorial risk rather than the continuation strategy alone. Prior publications similarly emphasize that urgent or unplanned surgeries pose distinct challenges and that rapid reversal or withholding of DOACs may not always be feasible, underscoring the need for case-by-case decision-making. 7
The group receiving LMWH bridging consisted of only four patients; although this subgroup exhibited minimal hemoglobin decline and no complications, the extremely small sample size precludes meaningful interpretation. Importantly, patients undergoing major pelvic surgery while receiving therapeutic anticoagulation (warfarin or DOACs) were underrepresented in our cohort. Therefore, our findings should not be extrapolated to this high-risk subgroup, which remains of particular clinical importance in gynecologic surgery. This mirrors the evolving body of literature questioning the benefit of bridging therapy. Several studies have shown that routine bridging may increase perioperative bleeding without a clear reduction in thromboembolic events, particularly in non-cardiac surgical populations.3,4,8–10 Nonetheless, selected high-risk patients—such as those with mechanical heart valves or very recent thromboembolism—may still require bridging according to guideline-based criteria.
The overall complication rate in our cohort (9.6%) is comparable with previously reported ranges in women on chronic antithrombotic therapy undergoing non-oncologic surgery.1,2 Importantly, most complications occurred in patients with multiple systemic comorbidities, suggesting that patient-specific factors may outweigh the choice of antithrombotic management strategy. This observation aligns with Swan et al., who highlighted that bleeding outcomes among patients on antiplatelet therapy are strongly influenced by underlying cardiovascular and metabolic disease rather than the pharmacologic agent itself. 5
A notable strength of this study is its focus on benign gynecologic surgery—a clinical area that remains underrepresented in perioperative antithrombotic research. Existing literature has largely centered on oncologic populations or broad procedural categories, making it difficult to extrapolate findings to the typical gynecologic surgery patient.1,2 Our study contributes additional real-world data to this limited evidence base.
However, several limitations should be acknowledged. The retrospective design, modest sample size, and incomplete availability of standardized risk scores (such as CHA2DS2-VASc or HAS-BLED) restrict detailed risk stratification. In addition, the inclusion of a wide range of gynecologic procedures with varying bleeding risks, as well as different antithrombotic agents, introduces clinical heterogeneity, which may have obscured potential differences between management strategies. However, this heterogeneity also reflects real-world clinical practice, where perioperative decisions must be individualized across diverse patient and procedural contexts.
Despite these limitations, the overall consistency of our results with existing studies supports the growing recognition that individualized, risk-adapted strategies may be more valuable than rigid interruption algorithms in the perioperative management of gynecologic patients on chronic antithrombotic therapy.
This study has several limitations that should be considered when interpreting the findings. First, the retrospective design inherently restricts the ability to control for confounding factors and introduces dependence on the accuracy and completeness of electronic medical records. Perioperative management decisions were made by different clinicians, and the rationale behind continuation, interruption, or bridging could not always be fully reconstructed.
Second, although the overall sample size was moderate, several perioperative management subgroups—particularly the LMWH-bridging group—were small, limiting the ability to detect differences in rare but clinically important events such as thromboembolism or major bleeding.
Third, widely used thrombotic and bleeding risk scoring systems (such as CHA2DS2-VASc, HAS-BLED, or Caprini models) were not consistently available in the medical records and therefore could not be applied uniformly. This limitation introduces potential confounding, as perioperative outcomes may be influenced by underlying patient risk profiles rather than the antithrombotic management strategy itself. The inability to incorporate standardized risk stratification reduces the granularity of the analysis and limits the strength of comparative interpretations.
Fourth, postoperative hemoglobin measurements were missing in patients undergoing minor procedures due to routine same-day discharge. These cases were excluded from hemoglobin analysis, which may have introduced selection bias, as patients with seemingly uncomplicated recoveries were systematically omitted from quantitative assessment.
Fifth, this study was conducted in a single tertiary care center with unique perioperative workflows, antithrombotic management habits, and surgical case distribution. Institutional protocols and surgeon preference may differ from those of other centers, potentially limiting generalizability.
Finally, intraoperative blood loss was not measured using a standardized method across cases. Although intraoperative bleeding is routinely assessed in clinical practice using surrogate indicators such as suction volume, surgical field assessment, and intraoperative laboratory values, these measures were not consistently or systematically recorded in the medical records and therefore could not be included in the analysis. Hemoglobin decline was used as a surrogate marker for perioperative bleeding, which may be influenced by perioperative hydration status, timing of laboratory sampling, and baseline anemia. Although the requirement for blood transfusion was also evaluated as a clinically relevant indicator of bleeding, the overall low event rate limits the ability to detect meaningful differences between groups. The absence of standardized intraoperative blood loss measurements and validated bleeding endpoints further constrains the assessment of true perioperative bleeding risk.
Despite these limitations, the study provides clinically relevant observational data that reflect real-world perioperative antithrombotic management in gynecologic surgery and may help inform future prospective research.
Conclusion
In this retrospective cohort, different perioperative antithrombotic management strategies—including continuation, temporary interruption, and limited LMWH bridging—were not associated with statistically significant differences in postoperative hemoglobin decline or overall complication rates. However, these findings should be interpreted with caution given the modest sample size, heterogeneity of surgical procedures, and small subgroup distributions. The absence of statistically significant differences should not be interpreted as evidence of equivalence between strategies.
The variability observed across patient groups reinforces the importance of tailoring perioperative antithrombotic decisions to individual thromboembolic risk, bleeding risk, and procedural complexity rather than relying solely on uniform interruption intervals. These results should be considered exploratory and hypothesis-generating, reflecting real-world clinical practice rather than definitive comparative evidence.
As the number of women receiving long-term antithrombotic therapy continues to grow, further prospective, adequately powered studies incorporating standardized risk stratification and detailed perioperative metrics are needed to guide clinical decision-making and support the development of gynecology-specific perioperative guidelines.
Ethical Approval
The Health Sciences University Istanbul Training and Research Hospital’s Clinical Research Ethics Committee granted approval (Decision No: 136, Date: 13.12.2024). Every author conducted the study in complete accordance with the Declaration of Helsinki.
Consent for Publication
All authors have reviewed and approved the final version of the article and consent to its publication.
Availability of Data and Material
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Use of Artificial Intelligence Tools
Artificial intelligence–based language models were used only to assist with grammar correction and improving the clarity of the article text. No part of the study design, data analysis, or interpretation of findings was generated by AI. All scientific content was written by the authors.
Authors’ Contributions
T.I.: Conceptualization, investigation, writing—original draft, formal analysis, data curation, and methodology. E.E.: Data curation, investigation, writing—review and editing, and conceptualization. Z.Y.Y.: Data curation, writing—review and editing, and conceptualization.
Footnotes
Acknowledgments
No external funding was received for this study. The authors thank the clinical and administrative staff of the participating institution for their assistance with data retrieval.
Author Disclosure Statement
The authors have no conflicts of interest.
Funding Information
This research received no external funding.