
Abstract
Background:
Digital solutions are increasingly integrated into gynecological services to improve efficiency and reduce avoidable cancellations. A smartphone-dependent home urine dipstick pathway was proposed as part of a quality improvement initiative to reduce same-day cancellations of urodynamic investigations. Understanding patient access to and confidence with digital technology is essential for successful implementation.
Objective:
To evaluate smartphone ownership, digital confidence, and familiarity with QR code technology among patients attending a urogynecology service and to assess readiness for a smartphone-based diagnostic pathway.
Methods:
A cross-sectional survey was conducted among adult patients attending urogynecology outpatient clinics at a UK district general hospital between May and July 2025. The survey assessed smartphone ownership, self-reported confidence using smartphones (5-point Likert scale), quick response code (QR code) familiarity, and acceptability of digital components of care. Age-stratified analyses were performed.
Results:
Of 156 patients invited, 108 participated (69.2%). Overall, 92 participants (85.2%) owned a smartphone. Ownership declined significantly with age (p < 0.001), from 100% in patients aged <50 years and 97.4% in those aged 50–69 years to 67.4% in those aged ≥70 years. Mean smartphone confidence scores and QR code familiarity also decreased significantly with increasing age (p < 0.001). Overall, 39.8% of participants met predefined criteria, indicating a potential need for additional support or alternative pathways.
Conclusion:
While smartphone access is high in urogynecology patients, significant age-related disparities in digital confidence and QR familiarity may limit equitable implementation. Quality improvement initiatives introducing smartphone-dependent pathways should incorporate flexible, inclusive strategies to prevent digital exclusion.
Introduction
Digital integration within healthcare delivery is a strategic priority for the National Health Service (NHS), with the NHS 10-year health plan for England emphasizing expansion of digital tools to improve efficiency, reduce avoidable delays, and enhance patient experience. 1 NHS England guidance has further promoted digital-first approaches across outpatient services, including electronic communication, digital consent processes, remote monitoring, and online patient information resources.2,3 Increasingly, routine elements of care are delivered through smartphone-based or web-based platforms.
Within urogynecology, digital tools offer the potential to streamline care pathways that are particularly vulnerable to inefficiencies. Urodynamic testing remains a core diagnostic investigation in the assessment of lower urinary tract symptoms; however, same-day cancellations are common and contribute to service inefficiency and prolonged waiting times. 4 In our department, an internal audit demonstrated that approximately half of same-day urodynamic cancellations were attributable to positive urine dipstick results suggestive of urinary tract infection, with the remainder due to nonattendance. Such cancellations are disruptive for patients and reduce effective clinic utilization, making their reduction an important quality improvement (QI) target.
Home urine testing prior to urodynamic appointments has been proposed as a pragmatic strategy to identify infection in advance and avoid unnecessary hospital attendance. 5 Recent commercially available dipstick systems allow home testing with interpretation via smartphone-based applications requiring QR code scanning and digital result submission.6,7 These interventions align with national digital strategy and have the potential to improve pathway efficiency.
However, urogynecology services predominantly care for an older female population in whom digital access and confidence may vary. While mobile phone and internet use are widespread, engagement with more complex digital tasks declines with increasing age. 8 Importantly, ownership of a device does not equate to readiness to use technology for healthcare-related tasks such as QR code scanning or app-based result submission. Introducing smartphone-dependent systems without understanding baseline digital access risks excluding patients and widening inequalities in care. 9
The Urogynaecology Department at Buckinghamshire Healthcare NHS Trust, therefore, undertook a service evaluation to assess digital access and readiness prior to implementation of a smartphone- and QR code-dependent home urine dipstick pathway as part of a QI initiative to reduce same-day urodynamic cancellations.
Aim and objectives
The aim of this service evaluation was to determine the feasibility of implementing a smartphone-dependent home urine testing pathway in a district general hospital urogynecology service.
The objectives were to:
Determine the proportion of patients who own or have access to a smartphone. Assess patient confidence in smartphone use and familiarity with QR code technology. Examine age-related differences in digital access and confidence. Identify the proportion of patients who may require alternative pathways or additional support.
Methods
Study design and setting
This cross-sectional survey was conducted as a service evaluation within the Urogynaecology Department at Buckinghamshire Healthcare NHS Trust. The survey formed part of a departmental QI initiative aimed at reducing same-day cancellations of urodynamic investigations by introducing home urine dipstick testing prior to appointments. The proposed testing system required patients to use a smartphone application incorporating QR code scanning and digital result submission. The survey was undertaken to assess the feasibility of implementing this smartphone-dependent pathway within the local patient population.
Participants
Adult women attending urogynecology outpatient clinics between May and July 2025 were invited to participate. Inclusion criteria were age ≥18 years and current care under the urogynecology service. Patients were approached either during clinic attendance or by telephone following their appointment, depending on clinic workflow.
A total of 156 patients were invited to participate. Of these, 108 completed the survey (response rate 69.2%). Participation was voluntary. Verbal consent was obtained prior to survey administration. No identifiable patient information was collected. Data were anonymized and analyzed in aggregate as part of service evaluation and QI activity.
Survey instrument and data collection
A structured questionnaire was developed specifically for this service evaluation. The survey was administered verbally by a member of the urogynecology team, and responses were recorded contemporaneously. The completion time was approximately 5 minutes.
The questionnaire assessed the following points:
Mobile phone ownership and smartphone status. Access to a smartphone via family member or carer. Self-reported smartphone confidence (5-point Likert scale). Comfortably accessing online health information. Familiarity with QR code scanning. Willingness to engage with digital elements of care (including electronic patient information, electronic consent, and QR code-linked processes).
Outcomes
The primary outcome was the proportion of participants who owned a smartphone. Secondary outcomes included smartphone access via alternative means, self-reported confidence using smartphones, familiarity with QR code technology, and age-related differences in these measures relevant to implementation of the proposed home urine testing pathway.
Statistical analysis
Data were analyzed using descriptive and inferential statistics. Categorical variables are presented as numbers (percentage). Continuous variables are summarized as mean values where appropriate. Associations between age group (<50 years, 50–69 years, and ≥70 years) and categorical outcomes, including smartphone ownership and QR code familiarity, were assessed using the chi-square test of independence. Effect size was quantified using Cramer’s V. Smartphone confidence was measured using a 5-point Likert scale and treated as ordinal data. Differences in confidence scores across age groups were analyzed using the Kruskal–Wallis test. A two-sided p-value of <0.05 was considered statistically significant.
Ethical considerations and governance
This project was conducted as a QI and service evaluation initiative within Buckinghamshire Healthcare NHS Trust (registered as a QI project, project code Obst & Gynae/2025-26/02). In accordance with NHS guidance, formal Research Ethics Committee approval was not required. The project was undertaken with local governance approval as part of a departmental service improvement activity. All data were collected and stored in anonymized form in line with Trust information governance policies.
Results
Participant recruitment and characteristics
Between May and July 2025, 156 patients attending urogynecology outpatient clinics were invited to participate. Of these, 108 completed the survey, yielding a response rate of 69.2%. Participants represented a broad adult age range: 24 (22.2%) were aged <50 years, 38 (35.2%) were aged 50–69 years, and 46 (42.6%) were aged ≥70 years.
Pelvic organ prolapse, including pessary review with or without urinary incontinence, was the most common reason for attendance (47.2%). Referral indications are summarized in Table 1.
Reason for Attending Urogynecology Clinic (n = 108)
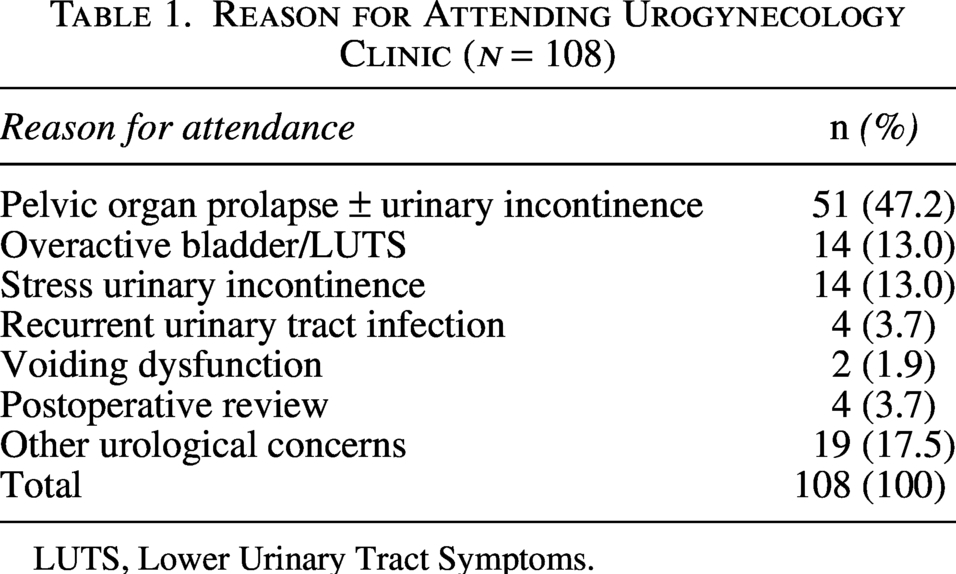
LUTS, Lower Urinary Tract Symptoms.
Smartphone ownership
Overall, 92 of 108 participants (85.2%) reported owning a smartphone. Smartphone ownership differed significantly by age group (Table 2). Ownership was universal among participants aged <50 years (24/24, 100%) and high among those aged 50–69 years (37/38, 97.4%), but substantially lower among those aged ≥70 years (31/46, 67.4%). There was a statistically significant association between age group and smartphone ownership (χ2(2) = 20.18, p < 0.001; Cramer’s V = 0.43).
Smartphone Ownership by Age Group (n = 108)
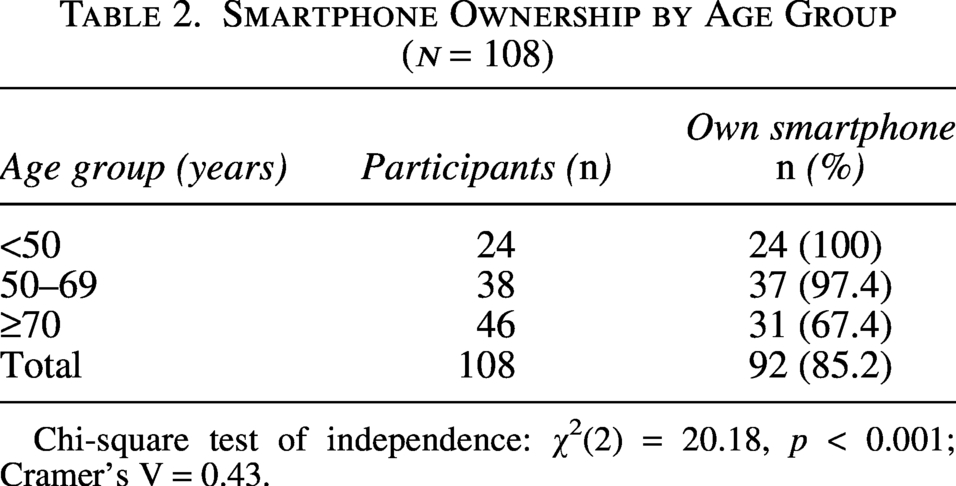
Chi-square test of independence: χ2(2) = 20.18, p < 0.001; Cramer’s V = 0.43.
Among the 16 participants who did not personally own a smartphone, 11 reported access to a device via a family member or carer.
Confidence Using Smartphones
Comfort and confidence with using smartphones and technology for daily use were assessed using a 5-point Likert scale (1 = not confident at all; 5 = very confident/proficient). Mean confidence scores demonstrated a clear age-related gradient (Table 3). Participants aged <50 years reported the highest confidence (mean: 4.61), followed by those aged 50–69 years (mean: 4.07). Participants aged ≥70 years reported substantially lower confidence (mean: 2.84). Differences across age groups were statistically significant (Kruskal–Wallis test, p < 0.001).
Smartphone Confidence Score by Age Group (n = 108)
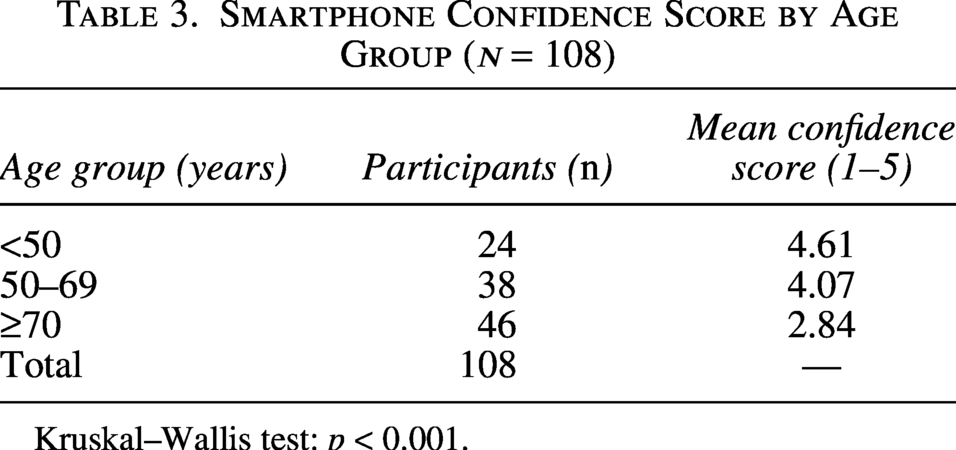
Kruskal–Wallis test: p < 0.001.
Although 76.9% of participants reported being comfortable accessing internet-based health information when signposted, 48.1% expressed a preference for printed materials either exclusively or alongside digital resources.
Familiarity with QR code technology
Overall, 69 of 108 participants (63.9%) reported familiarity with QR code scanning. Familiarity varied significantly by age group (Table 4). All participants aged <50 years were familiar (24/24, 100%). Among those aged 50–69 years, 30 of 38 (78.9%) were familiar. In contrast, only 15 of 46 participants aged ≥ 70 years (32.6%) reported familiarity.
QR Code Familiarity by Age Group (n = 108)
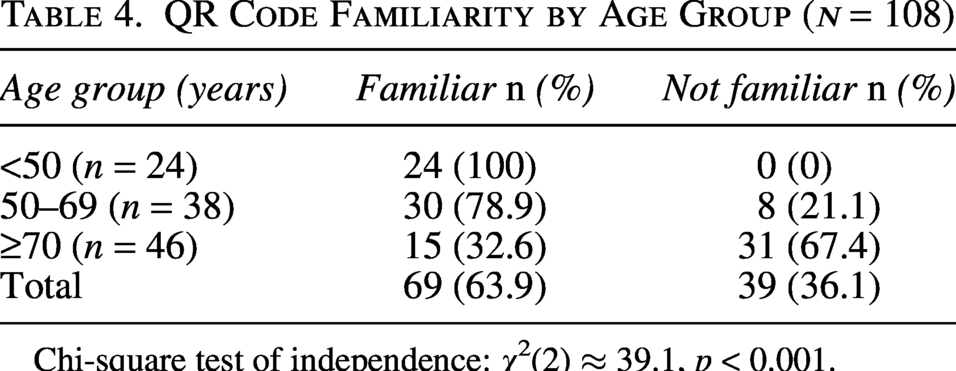
Chi-square test of independence: χ2(2) ≈ 39.1, p < 0.001.
There was a statistically significant association between age group and QR code familiarity (χ2(2) ≈ 39.1, p < 0.001).
Acceptability of digital components of care
Acceptance of digital elements of care reflected patterns observed in smartphone ownership and confidence. Accessing patient information electronically was acceptable to 76.9% of participants, and 64.8% reported comfort with electronic consent processes. Acceptance of QR code-linked processes was 63.9% overall and was notably lower among older participants, many of whom reported that assistance from a family member would be required.
Discussion
Principal findings
This service evaluation demonstrates that while smartphone ownership is high among patients attending a district general hospital urogynecology service, digital readiness is not uniform. Although 85.2% of participants owned a smartphone, confidence in smartphone use and familiarity with QR code technology declined significantly with increasing age.
Critically, smartphone ownership alone did not equate to functional digital capability. A substantial proportion of older patients who owned smartphones reported limited confidence or unfamiliarity with QR code scanning, an essential component of the proposed home urine dipstick pathway. These findings highlight a potential gap between digital access and digital usability within this patient population.
Clinical implications for urodynamic services
Same-day cancellation of urodynamic investigations represents a significant service inefficiency. In our department, approximately half of cancellations were attributable to positive urine dipstick results. Introducing home urine testing has clear potential to reduce avoidable attendance and optimize clinic utilization. However, this study demonstrates that a fully smartphone-dependent pathway would not be universally accessible. Nearly 40% of participants met predefined criteria indicating potential need for additional support or alternative routes. Without appropriate safeguards, digital-first implementation risks excluding older patients, thereby undermining both equity and the intended efficiency gains of the QI initiative.
Successful implementation should therefore include parallel nondigital options, simplified instructions, and optional support mechanisms. Importantly, patients who have access to appropriate devices but lack digital confidence may still be able to engage with smartphone-dependent pathways if targeted support is provided. Potential strategies include step-by-step written or visual guidance, brief in-clinic demonstrations, and involvement of family members or carers where appropriate. Such measures may enable inclusion without defaulting to nondigital alternatives, thereby preserving both accessibility and efficiency. Digital transformation within urogynecology must remain patient-centered rather than technology-driven.
Comparison with existing literature
Our findings are consistent with previous studies showing high rates of device ownership among older adults but reduced confidence and independence in use.10,11 Broader digital health research similarly reports age-related differences in engagement with healthcare-specific digital tasks, particularly those involving multistep processes or unfamiliar interfaces.12–14 U.K. data from NHS Digital continue to demonstrate persistent disparities in digital capability despite increasing internet access.15–17
Importantly, our findings also highlight that simple measures of device ownership are insufficient when designing digital interventions for clinical use. Understanding the baseline digital capability, confidence, and support needs of a defined patient population is fundamental to the successful implementation of clinic-based digital tools. Digital history-taking platforms and tablet-based assessment systems are increasingly being introduced into outpatient services; however, their effectiveness depends not only on technical functionality but also on alignment with the digital readiness of the population they are intended to serve. Assessing local digital confidence, therefore, represents a necessary step in the responsible design and implementation of such innovations.
This study extends existing literature by evaluating readiness for a specific, clinically relevant intervention within a live QI framework, rather than assessing hypothetical digital engagement.
Strengths and limitations
A key strength of this study is its direct integration within a QI initiative targeting a defined clinical problem. The cohort reflected a typical urogynecology population, and the response rate was high.
Limitations include the single-center design and reliance on self-reported digital confidence. Objective assessment of digital skills was beyond the scope of this pragmatic service evaluation. Socioeconomic and educational variables were not collected. The study was not only designed to evaluate clinical outcomes of home urine testing but also to inform implementation strategy. Evaluation of the effectiveness and real-world impact of the full QI intervention is ongoing and will be reported separately.
Conclusions
Digital innovation offers clear opportunities to improve efficiency within urogynecology services. However, this study demonstrates that digital access does not equate to digital readiness. Age-related disparities in confidence and QR code familiarity must be addressed to avoid unintended exclusion. QI initiatives introducing smartphone-dependent pathways should incorporate structured assessment of digital capability and provide inclusive alternatives. Thoughtful implementation will ensure that digital transformation enhances, rather than restricts, access to care.
Authors’ Contributions
A.S.: Design of project, data collection, and writing of article. N.V., M.A., and H.D.: Data collection. I.C.: Supervisor of project and article editing. A.P.: Supervisor of project and article editing.
Ethical Considerations
Our institution does not require ethical approval for service evaluation projects.
Further information can be found here: https://share.google/XkyOW2yh4q3dt9LJm.
Footnotes
Acknowledgments
The authors would like to thank Dr. Bavithra Hemanth for her assistance with the editing of this article.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.