
Abstract
Introduction:
Increasing cultural diversity requires effective educational strategies to support nursing students’ cultural awareness and readiness for culturally competent practice.
Methods:
An explanatory sequential mixed-methods design was used. Forty-three fourth-year nursing students completed a single-group pre-test/post-test study without a control group using the Cultural Competence Assessment Tool. Four weekly sessions were delivered. Semi-structured interviews were conducted with 23 students and analyzed inductively.
Results:
Post-test cultural awareness and total cultural competence scores were higher than pre-test scores (both p < .001; dz = 1.07 and dz = 0.67). Self-assessment scores increased in awareness and cultural sensitivity, whereas no significant change was found in self-assessed cultural practice. Qualitative findings highlighted language barriers, limited cultural knowledge, and the method’s concise, awareness-raising nature.
Discussion:
Pecha Kucha appears to function mainly as a reflective, awareness-oriented pedagogical approach that supports readiness for culturally competent practice, rather than as an intervention producing immediate behavioral competence.
Introduction
With the rapid increase in global migration movements, Türkiye has become one of the countries receiving the highest number of migrants, and its high level of cultural diversity makes it necessary to take cultural differences into account in the delivery of health care services (International Organization for Migration, 2024; T.C. İçişleri Bakanlığı Göç İdaresi Başkanlığı, 2025). In response to this need, theoretical approaches that place cultural differences at the center of nursing have been developed, and the concept of culturally competent care emphasizes that nurses should develop competencies in the dimensions of cultural awareness, cultural knowledge, cultural sensitivity, and cultural practice to meet the care needs of individuals from different cultural backgrounds in an effective, sensitive, and respectful manner (Papadopoulos, 2006).
In nursing education, different teaching strategies have been used to support the development of cultural competence, including simulation-based learning, reflective learning activities, case-based discussions, and interprofessional educational experiences (Tosun et al., 2021). These approaches are often valued because they create opportunities for students to examine their own assumptions, encounter different perspectives, and relate cultural issues to clinical care. In this context, culturally competent care is generally understood as a multidimensional learning process that requires not only knowledge acquisition but also self-awareness, reflection, and the ability to respond appropriately in practice (Leyva-Moral et al., 2023; Ličen & Prosen, 2023).
It has been reported that nursing students prefer modern, interactive approaches to learning. In this context, the Pecha Kucha method, an alternative teaching strategy, is a presentation format designed to sustain learner engagement and attention through structured, visually oriented presentations delivered within a short time frame (Liao et al., 2020; White & Louis, 2023). In this format, presentations consist of 20 slides that advance automatically every 20 s and last approximately 7 min. The intensive use of visual elements, limited use of text, the adoption of a narrative-based presentation style, and the opportunity for presenters to interact more actively with the audience are among the main features of the Pecha Kucha method that support the learning process (White & Louis, 2023). Beyond its structural features, the Pecha Kucha format may also be relevant to cultural competence education because it encourages students to focus on key ideas, engage with visual and verbal content together, and reflect on meaning within a limited time frame. This combination may be particularly useful in addressing topics such as culture, prejudice, communication, and professional sensitivity, which often require not only knowledge acquisition but also self-awareness and reflection. In this respect, the method may support students’ engagement with culturally sensitive content in a more focused and memorable way, while also encouraging them to question their own assumptions. Rather than directly producing behavioral competence, it may be more closely aligned with awareness-building and reflective learning processes that encourage students to reflect on their own assumptions, attitudes, and potential biases in care (Leyva-Moral et al., 2023; Ramos-Rincón et al., 2018; White & Louis, 2023).
From this perspective, the Pecha Kucha method is considered an innovative approach that can be used to support educational activities aimed at sensitively and effectively addressing the cultural needs of individuals, families, and communities, which constitute the fundamental objectives of culturally competent care (Liao et al., 2020; White & Louis, 2023). Although it does not offer the experiential depth of simulation or interprofessional practice, it may provide a practical way to promote awareness, attention, and reflection within limited instructional time. Various teaching strategies have been used to support cultural competence in nursing education, yet the contribution of brief, structured presentation-based methods such as the Pecha Kucha format remains unclear. Therefore, the aim of this study was to examine changes in nursing students’ cultural competence following culturally competent care education delivered using the Pecha Kucha method and to explore nursing students’ views regarding this educational method.
Research Questions
What changes, if any, are observed in the cultural competence levels of nursing students following Pecha Kucha-based cultural competence education?
What are nursing students’ views regarding Pecha Kucha-based cultural competence education?
Methods
Ethical Considerations
Ethical approval for this study was obtained from the Non-Interventional Clinical Research Ethics Committee of Nuh Naci Yazgan University (Decision No: 2024/003/09; Date: March 12, 2024). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Study Design
This study used an explanatory sequential mixed-methods design. The quantitative component was carried out using a single-group pre-test/post-test quasi-experimental design, while the qualitative component consisted of individual in-depth interviews conducted with a semi-structured interview guide. The quantitative phase of the study was reported in accordance with the TREND (Transparent Reporting of Evaluations with Nonrandomized Designs) guidelines for non-randomized intervention studies (Des Jarlais et al., 2004). Reporting of the qualitative phase of the study followed the COREQ (Consolidated Criteria for Reporting Qualitative Research) guidelines (Özden et al., 2022; Tong et al., 2007).
Setting and Participants
The study was conducted with fourth-year nursing students enrolled at a university in Türkiye.
Sample of the Quantitative Phase
The aim was to reach the entire population of 53 fourth-year nursing students. Students who volunteered to participate were included in the quantitative phase of the study. No formal sample size calculation was performed, as the study aimed to include the entire accessible population.
Sample of the Qualitative Phase
For the qualitative phase, criterion sampling, a purposive sampling method, was used (Baltacı, 2019; Campbell et al., 2020). Fourth-year nursing students with no previous intercultural nursing education who volunteered to participate were included. Interviews continued until data saturation was reached. Data saturation was reached at the 15th interview, and a total of 23 participants were interviewed to support the confirmability of the findings. Given the relatively small sample and the absence of a formal sample size calculation, the quantitative findings should be interpreted as exploratory.
Interventions and Procedure
The study was conducted in four stages:
Stage 1
After obtaining ethical committee and institutional approvals and written informed consent, nursing students who agreed to participate in the study completed the Introductory Information Form and the Cultural Competence Assessment Tool as a pre-test, and 43 students were included in the quantitative phase.
Stage 2
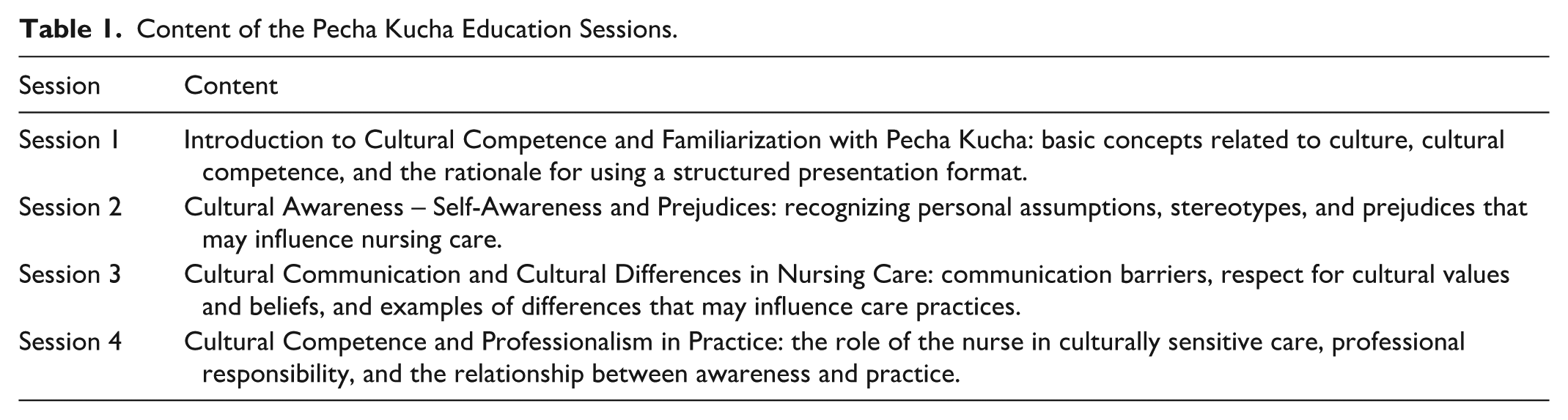
Students received culturally competent care education delivered using the Pecha Kucha method. In this study, the Pecha Kucha presentations were prepared and delivered by the faculty member; students did not prepare or present their own Pecha Kucha slides. The educational content was developed based on the literature and reviewed by experts. The training was delivered by a faculty member experienced in transcultural nursing education and research. The training sessions were scheduled according to students’ availability and held once a week for 4 consecutive weeks. Each session included one structured Pecha Kucha presentation consisting of 20 slides shown for 20 s each, followed by a question-and-answer and discussion period. Each session lasted approximately 30 min. The discussion component allowed students to ask questions, share observations from clinical practice, and reflect on the relevance of the content to culturally competent nursing care. The presentations also included brief visual examples related to cultural assumptions, communication barriers, and culturally sensitive care situations to support discussion and reflection. The sessions were conducted in a classroom setting as part of the educational process. The content of the four Pecha Kucha sessions is presented in Table 1.
Content of the Pecha Kucha Education Sessions.
Stage 3
One week after completing the education, the CCAT was re-administered to assess changes in students’ levels of cultural competence.
Stage 4
In the fourth and final stage, qualitative data were collected to provide a more in-depth explanation of the quantitative findings through a semi-structured interview guide to explore students’ views on culturally competent care education delivered using the Pecha Kucha method. Individual in-depth interviews were conducted with 23 students selected using criterion sampling, conducted face-to-face in a quiet setting at a time convenient for participants after the education, lasted approximately 25–30 min, and were audio-recorded with participants’ permission. Each participant was assigned a code number (K1, K2, K3, . . .), and the quantitative and qualitative data were analyzed separately.
Measures
Introductory Information Form
The Introductory Information Form was developed by the authors based on the relevant literature and consisted of 10 items addressing sociodemographic characteristics and issues related to the care of patients from different cultural backgrounds (Ceylan & Çetinkaya, 2022; Erten et al., 2014; Işık & Can Özdemir, 2024).
Cultural Competence Assessment Tool (CCAT)
The CCAT was designed to assess cultural competence based on the Cultural Competence Model developed by Papadopoulos, Tilki, and Taylor in 2002. The Turkish adaptation of the instrument was conducted by Dığrak and Temel in 2020. The model conceptualizes cultural competence as consisting of four subdimensions: cultural awareness, cultural knowledge, cultural sensitivity, and cultural practice. Each subdimension consists of 10 items, each measured on a four-point Likert-type scale, for a total of 40 items. For the calculation of cultural competence, responses of “strongly agree” or “agree” are scored as correct and assigned one point (1), whereas responses of “disagree” or “strongly disagree” are scored as incorrect and assigned zero points (0). Scores are summed to obtain subscale and total scores. Each subdimension yields a score ranging from 0 to 10, and the maximum total score of the scale is 40. A total score of 40 indicates that the individual is culturally competent. Although the original items are presented in a Likert-type format, the instrument’s dichotomous scoring structure yields bounded scores with reduced variability. This feature should be considered when interpreting the instrument’s ability to detect subtle changes over time.
Visual Analog Scale (VAS)
Each CCAT subdimension includes a Visual Analog Scale (VAS) that allows participants to rate their perceived competence from 1 to 10 (1 = lowest/negative, 10 = highest/positive). In this study, the VAS was not treated as a separate measurement instrument but as the self-assessment component of the CCAT (VAS = Self-assessment of cultural awareness, Self-assessment of cultural knowledge, Self-assessment of cultural sensitivity [comfort], Self-assessment of cultural sensitivity [trust, respect, and empathy], Self-assessment of cultural practice, Self-assessment of cultural practice [attitudes toward racism and discrimination]). Accordingly, the CCAT item scores and the VAS scores were interpreted as reflecting related but not identical aspects of cultural competence: the former providing a structured score derived from item responses, and the latter reflecting participants’ subjective self-perceptions. This distinction was taken into account when comparing objective and self-reported changes (Dığrak & Tezel, 2022). Permission to use the instrument was obtained.
Semi-Structured Interview Form
The interview form consisted of four questions and was developed based on the study by Ceylan and Çetinkaya (2022) and Işık and Can Özdemir (2024) and expert opinions. The semi-structured interview form aimed to enable participants to express their views on the topic in their own words (Adeoye-Olatunde & Olenik, 2021; Polat, 2022).
Data Analysis
Students’ sociodemographic characteristics were summarized using frequencies and percentages. The subscale and total scores of the Cultural Competence Assessment Tool (CCAT) ranged from 0 to 10 for each subdimension and exhibited a discrete, bounded structure. In addition, some subscales showed relatively high baseline values, which may have reduced the instrument’s sensitivity to detect change in this sample. The normality of pre-test/post-test difference scores for each subdimension was assessed using the Shapiro–Wilk test. Paired-samples t-tests were used to examine differences between pre-test and post-test scores for subdimensions that met the normality assumption, whereas the Wilcoxon signed-rank test was applied for subdimensions that did not meet this assumption. The unit of analysis was the individual nursing student.
Given the limited range of scale scores and the possibility of ceiling effects in subscales with high pre-test scores, the findings were interpreted with caution and evaluated within the study’s methodological limitations. The level of statistical significance was set at p < .05 for all analyses. Effect sizes were calculated as Cohen’s dz for variables analyzed using the paired-samples t-test and as r for variables analyzed using the Wilcoxon signed-rank test (r = Z/√N). Quantitative data were analyzed using IBM SPSS Statistics version 27.0 (IBM Corp., 2020).
The qualitative interviews were audio-recorded with the permission of the participants, lasted approximately 30 min, and were transcribed verbatim. The transcripts were imported into MAXQDA software and analyzed using inductive content analysis (VERBI Software, 2024). First, the transcripts were read repeatedly to gain familiarity with the data. Meaningful expressions were then identified and coded through open coding. Codes with similar meanings were grouped into categories, and broader themes were developed based on relationships among categories. The coding process was carried out independently by three researchers, and differences were discussed until consensus was reached. Participant quotations were presented verbatim and identified using participant codes (e.g., K1, K2) to illustrate the themes while preserving anonymity.
Results
Participant Characteristics
As shown in Table 2, 65% of the students were aged 18–22 years, 74.4% were female, 79% were not employed, 72% reported having only basic proficiency in a foreign language, and 67.4% reported rarely interacting with individuals from different cultures. In addition, 79% reported that no individuals with different cultural backgrounds were in their families, 48.8% stated that they frequently provided health care services to individuals from different cultures during their clinical practice, and 74.4% reported that they were willing to provide care to patients from different cultural backgrounds.
Descriptive Characteristics of the Participants (n = 43).
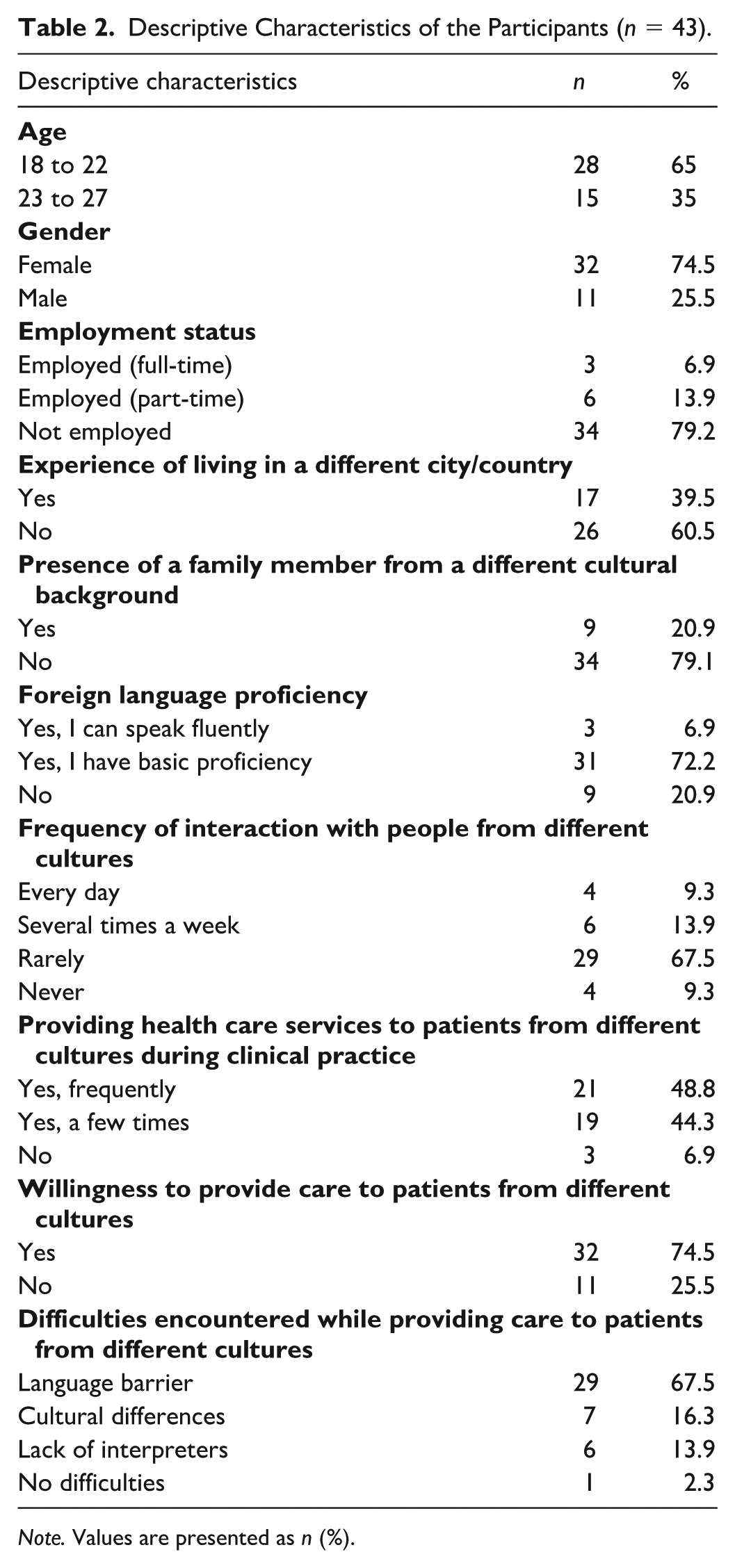
Note. Values are presented as n (%).
Quantitative Findings
As shown in Table 3, cultural awareness scores and total CCAT scores were higher at post-test than at pre-test. A statistically significant difference was observed for the cultural awareness subdimension (t = −7.01, p < .001, dz = 1.07) and for the total scale score (t = −4.38, p < .001, dz = 0.67). No statistically significant difference was observed for the cultural sensitivity subdimension (t = −1.67, p = .101, dz = 0.25). However, pre-test scores in some CCAT subdimensions were already close to the upper limit, which should be considered when interpreting the magnitude of change across subscales.
Comparison of the Cultural Competence Assessment Tool and its Subscale Mean Scores Before and After the Training (n = 43).
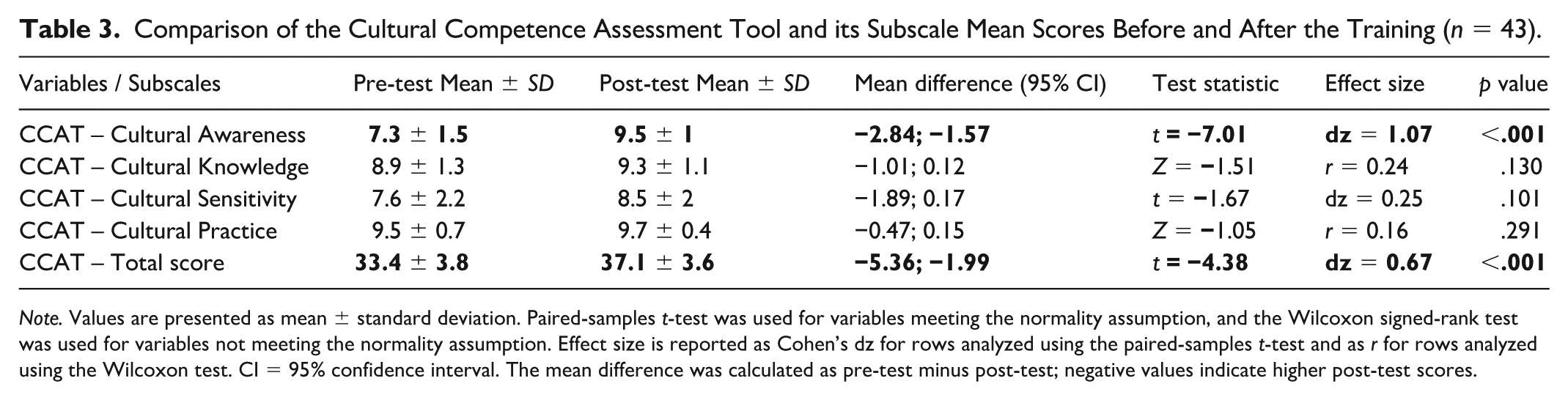
Note. Values are presented as mean ± standard deviation. Paired-samples t-test was used for variables meeting the normality assumption, and the Wilcoxon signed-rank test was used for variables not meeting the normality assumption. Effect size is reported as Cohen’s dz for rows analyzed using the paired-samples t-test and as r for rows analyzed using the Wilcoxon test. CI = 95% confidence interval. The mean difference was calculated as pre-test minus post-test; negative values indicate higher post-test scores.
Table 4 presents a comparison of participants’ self-reported cultural competence levels assessed using the VAS at pre-test and post-test. The analysis showed that post-test scores in the cultural awareness subdimension (7.3 ± 2.7) were significantly higher than pre-test scores (5.9 ± 2.0) (t = −2.52, p = .015, dz = 0.38). Post-test scores in the cultural sensitivity subdimension (6.74 ± 2.31) were also significantly higher than pre-test scores (4.9 ± 2.0) (t = −3.87, p < .001, dz = 0.59). Likewise, post-test scores in the cultural practice subdimension (6.62 ± 2.38) were higher than pre-test scores (5.7 ± 2.41), although this difference was not statistically significant (t = −1.71, p = .095, dz = 0.26).
Participants’ Subjective Cultural Competence Assessments (VAS) (n = 43).
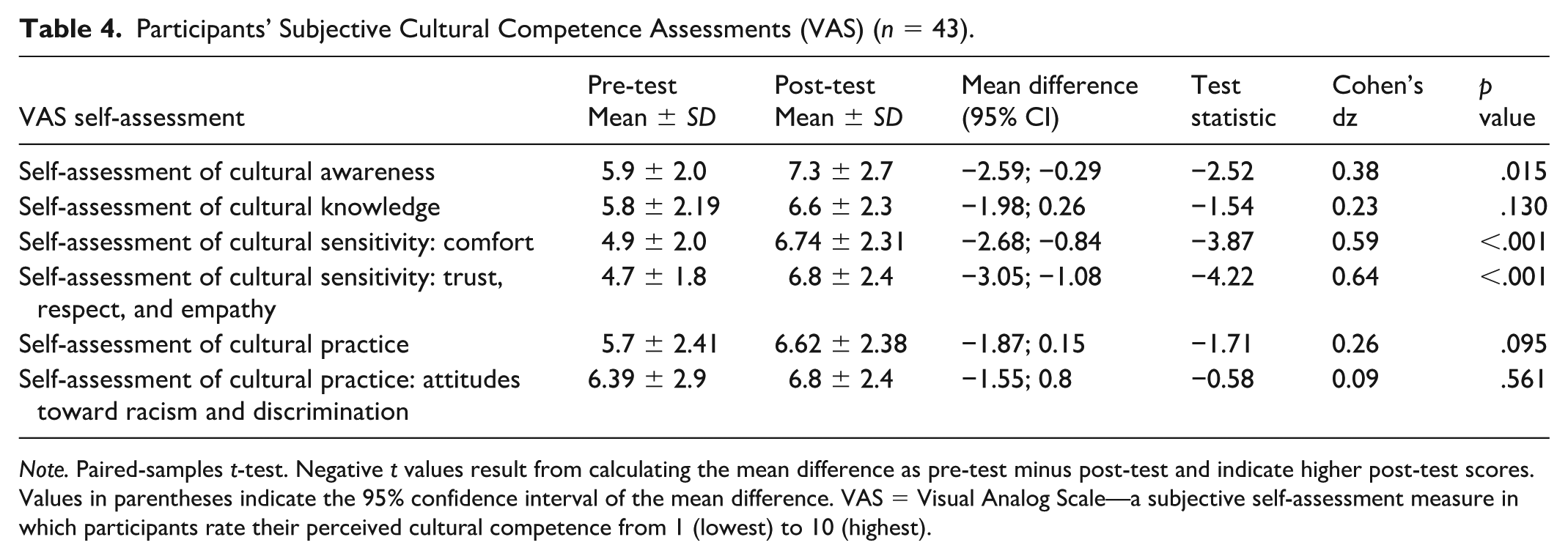
Note. Paired-samples t-test. Negative t values result from calculating the mean difference as pre-test minus post-test and indicate higher post-test scores. Values in parentheses indicate the 95% confidence interval of the mean difference. VAS = Visual Analog Scale—a subjective self-assessment measure in which participants rate their perceived cultural competence from 1 (lowest) to 10 (highest).
Qualitative Results
In line with the explanatory sequential mixed-methods design, qualitative findings were used to provide a more in-depth understanding of the quantitative findings and to explore students’ experiences related to this process. Data obtained from individual interviews with nursing students were organized into two main themes: Nursing students’ experiences of interacting with individuals from different cultures in clinical education and Nursing students’ views on culturally competent care education delivered using the Pecha Kucha method. Each theme was summarized using tables of categories and codes developed based on the questions in the semi-structured interview form.
Under the first theme, students’ views regarding their experiences of interacting with patients from different cultural backgrounds were examined within three categories (Table 5). When encountering patients from different cultures in clinical practice, students most frequently reported feelings of difficulty (n = 5) and anxiety (n = 4). Positive emotions such as empathy (n = 3) and respect (n = 2) were also expressed. For example, participant K6 stated, “I speak a different language from the patient, and I have difficulty communicating . . . When they have different traditions and beliefs, they may not accept the care I provide . . . I feel challenged.”
Themes, Categories, and Codes Related to Nursing Students’ Clinical Interaction Experiences With Different Cultures and the Perceived Effects of the Pecha Kucha Training.
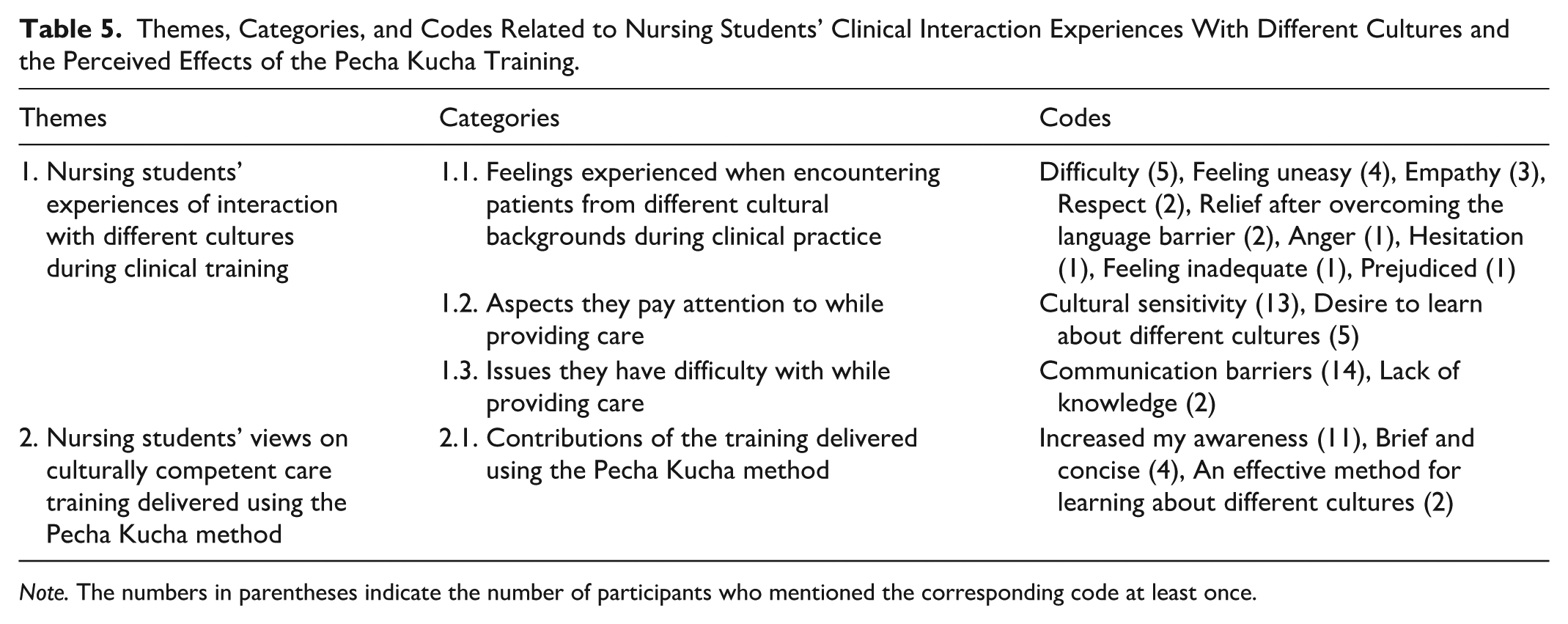
Note. The numbers in parentheses indicate the number of participants who mentioned the corresponding code at least once.
In terms of difficulties experienced during care, students particularly emphasized communication problems (n = 14) and lack of cultural knowledge (n = 2). For example, participant K13 stated,
When providing care to a patient from a different culture, who are usually migrant patients in our country, I cannot communicate. When communication is not possible, I cannot provide care or resolve their problems . . . After a while, problems arise on both sides; neither the patient receives quality care nor can we provide quality care.
Among the aspects they paid most attention to while providing care, cultural sensitivity (n = 13) emerged as the most prominent, followed by a desire to learn about different cultures (n = 5). For instance, participant K4 stated, “I try to provide care by paying attention to the patient’s cultural and religious beliefs. I try to understand their religious practices and the issues they are sensitive about, and I adjust the care I provide accordingly.”
Under the second theme, students described the Pecha Kucha method as an awareness-raising, concise, and effective approach for learning about different cultures (Table 5). For example, participant K16 stated,
I realized that each culture may have different ways of living their social life . . . I understood that the patient’s culture is an important factor to consider in the care process . . . I realized that we should communicate in a healthy and respectful way without judging them, and that if we take these into account while providing care, the care we deliver will be much more effective and efficient.
Participant K9 stated, “I can gain at least some knowledge about the cultures of patients from different backgrounds and have an idea about how I should proceed.” Similarly, participant K17 stated,
I think I received information in a short and effective way with this method. It clearly explained how and to what extent we should pay attention to different cultures and in which areas we should intervene . . . I believe the information was presented very precisely and clearly. However, I would have liked more information on how we can reflect this in our nursing care, because we also experience difficulties when we encounter patients from different cultural backgrounds.
Discussion
In this study, changes in nursing students’ cultural competence following culturally competent care education delivered using the Pecha Kucha method, together with students’ experiences of this process, were examined using an explanatory sequential mixed-methods design. Quantitative findings showed higher post-test scores for cultural awareness and total cultural competence, while no significant changes were observed in the cultural knowledge, cultural sensitivity, or cultural practice subscales. Qualitative findings further suggested that students encountered difficulties in clinical practice, particularly due to language barriers and limited cultural knowledge, and perceived the Pecha Kucha–based education as a concise, awareness-raising experience (Kaihlanen et al., 2019). From a pedagogical perspective, these findings suggest that the Pecha Kucha method may be more closely aligned with reflective learning and the development of cultural awareness than with immediate change in the more practice-based dimensions of cultural competence (Leyva-Moral et al., 2023; Ličen & Prosen, 2023).
Taken together, the quantitative and qualitative findings suggest that the observed post-test changes were more evident in awareness-related dimensions of cultural competence than in knowledge- and practice-based dimensions. The large effect size observed in the cultural awareness subscale (Cohen’s dz = 1.07) and the effect size above the moderate level for the total cultural competence score (Cohen’s dz = 0.67) are consistent with the interpretation that the educational process supported students’ reflection on their own values, prejudices, and cultural positioning. However, these findings do not permit a direct causal interpretation, and the observed changes cannot be attributed solely to the education delivered.
The qualitative findings also help to explain why post-test differences were more evident in awareness-related areas, whereas change was more limited in the knowledge and practice dimensions. Cultural awareness is a cognitive process that involves questioning one’s own cultural assumptions and attitudes in the care process and can be supported by short-term, structured, discussion-oriented educational activities (Leyva-Moral et al., 2023; Sharifi et al., 2019). In contrast, the development of cultural knowledge and cultural practice typically requires longer educational approaches that include intercultural interaction, clinical experience, simulation, and practice-based learning opportunities (Leyva-Moral et al., 2023; Ličen & Prosen, 2023). In the present study, the lack of significant change in the cultural knowledge, cultural sensitivity, and cultural practice subscales may be related to the inherently short, presentation-based nature of the Pecha Kucha format. Although students reported in qualitative interviews that they received information in a concise and clear manner and found the method effective, their emphasis on the need for more examples and practice in applying the content in clinical settings provides an important qualitative explanation for the lack of change in the knowledge and practice dimensions. These findings are consistent with the broader educational literature, suggesting that reflective and discussion-based approaches may be more useful for increasing awareness, whereas simulation-based and interprofessional learning may be more relevant for developing practice-oriented competencies. From this perspective, the Pecha Kucha method may be better suited to supporting reflective learning and cultural awareness than to producing immediate change in the more practice-based dimensions of cultural competence (Leyva-Moral et al., 2023; Ličen & Prosen, 2023; White & Louis, 2023). In practical terms, this suggests that the Pecha Kucha method may be most useful when positioned as a preparatory or complementary educational approach rather than as a stand-alone strategy. It may help students build awareness and reflective readiness before participating in more experiential forms of learning, such as simulation-based activities, case-based application, or supervised intercultural clinical encounters.
Self-assessment scores increased in some VAS dimensions, whereas comparable changes were not observed in the corresponding CCAT scores. This pattern may reflect not only the short-term nature of the educational process, but also the different measurement properties of the two components. While the CCAT produces structured scores based on dichotomously coded item responses, the VAS reflects participants’ subjective perceptions on a continuous scale. The VAS may therefore be more sensitive to perceived short-term shifts, whereas the CCAT may be less sensitive to subtle change. Accordingly, the divergence between self-perceived and scored competence should be interpreted as methodologically meaningful rather than contradictory (Leyva-Moral et al., 2023). Therefore, it would not be appropriate to interpret the observed increases in subjective scores as sustained behavioral change without support from long-term follow-up studies.
The qualitative findings further indicated that the most common difficulties students encountered when caring for patients from diverse cultural backgrounds in clinical settings were language barriers and insufficient cultural knowledge. Students reported difficulties in communicating, which negatively affected the care process. The literature similarly reports that one of the main barriers to intercultural care among nursing students and nurses is communication difficulties and limited cultural knowledge (Güney et al., 2025; Moezzi et al., 2024; Plaza del Pino et al., 2013; Shahzad et al., 2021; Uyanık & Tanrıverdi, 2021). In this context, students’ statements were consistent with the quantitative finding that post-test cultural awareness scores were higher; however, these findings suggest change primarily at a cognitive and reflective level rather than the acquisition of knowledge and skills that can be directly transferred into clinical practice.
Overall, the findings indicate that cultural competence education is a multidimensional learning process and that a single instructional method cannot promote simultaneous development across all dimensions (Okere, 2022). Although the Pecha Kucha presentation format can increase learner engagement, structure information efficiently, and direct students’ attention to the learning process, it does not appear sufficient on its own for the development of behavioral and practice-based competencies (Haramba et al., 2023; Oluic et al., 2025; Ramos-Rincón et al., 2018; White & Louis, 2023). In this respect, the qualitative findings suggest that its educational value may be strengthened when it is integrated with simulation-based, case-based, or other experiential learning opportunities that allow students to apply culturally responsive care in more practice-oriented contexts (Gillan & Johnston, 2024).
The methodological limitations of this study should be acknowledged. First, the study was conducted in a single academic setting with a relatively small sample, which limits the generalizability of the findings. In addition, all participants were final-year nursing students and may already have had relatively high levels of cultural competence from their prior academic and clinical experiences. Accordingly, the findings should be interpreted with caution and should not be assumed to represent students at different stages of training or in other institutional contexts. The absence of a control group and the use of a single-group pre-test/post-test design further limit the extent to which the observed changes can be interpreted as effects specific to the educational intervention. Without a comparison group, the observed differences may also reflect testing effects, maturation, or other educational experiences during the study period. In addition, the short follow-up period did not allow for evaluation of longer-term effects, particularly regarding cultural practices and behavioral change. The use of self-report measures may also have introduced social desirability and testing effects. In addition, because the same self-report measures were administered before and after the educational process, some responses may have been influenced by repeated measurement or response bias. Therefore, the observed increases—especially in the cultural awareness dimension—should be interpreted cautiously, as they may partly reflect temporary changes related to increased awareness and measurement sensitivity. Relatively high baseline scores in some CCAT subdimensions may also have reduced the instrument’s ability to detect further change. Finally, differences in the measurement structure of the CCAT and its self-assessment component may have influenced the extent to which subtle changes were captured across dimensions.
Conclusion
The findings of the study suggest that the Pecha Kucha method may support nursing students primarily by strengthening reflective learning processes and increasing awareness of cultural issues, which are important foundations for culturally competent care. Overall, it may be considered a useful reflective and awareness-oriented educational approach in cultural competence education; however, the study design does not allow conclusions about direct intervention effects or immediate changes in culturally competent clinical behavior.
Footnotes
Acknowledgements
The authors would like to thank all nursing students who voluntarily participated in this study.
The authors used QuillBot solely for English language editing and grammar improvement. The authors take full responsibility for the content and integrity of the manuscript.
Ethical Considerations
Ethical approval for this study was obtained from the Non-Interventional Clinical Research Ethics Committee of Nuh Naci Yazgan University (Decision No: 2024/003/09; Date: March 12, 2024). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from all participants before participation in the study.
Author Contributions
Betül Özen: Conceptualization, methodology, supervision, formal analysis, writing – review and editing.
Cansu Yaşar: Conceptualization, methodology, data collection, formal analysis, writing—original draft.
Zeliha Kaya Erten: Methodology, supervision, formal analysis, writing—review and editing.
Hülya Uçar: Supervision, writing—review and editing.
All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to the protection of participant confidentiality but are available from the corresponding author on reasonable request.
Anonymity and Identifiable Information Statement
All potentially identifying information related to the authors, institutions, funding bodies, and ethics committees has been removed or masked from the manuscript to ensure a blinded peer-review process and to protect the anonymity of the participants and institutions.