
Abstract
There is a distinct lack of a normative theory for diversion of justice-involved individuals with mental illness at the intersection of the criminal justice and health care systems. The nexus where the criminal justice and health care systems are supposed to connect during diversion is not conceptually framed in a measurable way. The paper proposes a potential systems theory of diversion that explicates the overlapping boundaries within and between the criminal justice and health care systems. From a systems perspective, diversion is operationalized differently depending on the entry of an individual with justice involvement and mental illness into one of the systems. The criminal justice and health care systems have multiple levels (micro-, meso-, and macro-), but individuals enter both systems at the respective systems intersection of the micro- and meso-levels. The theoretical disconnect may fail to consider the impact of criminal justice diversion on the health care system. We propose a unified systems theory of diversion to improve evaluation, comparability, sustainability, resource allocation, and outcomes of diversion programs.
Introduction
Is diversion the new deinstitutionalization? The criminal justice system has become the largest provider of mental health care in the United States (American Psychiatric Association [APA], 2020). Incarcerated individuals are 3 to 5 times more likely to have a diagnosed mental illness as adults in the general population (Bronson & Berzofsky, 2017) and individuals with mental illness are charged with minor offenses “just to get them off the streets and as a means of obtaining mental health treatment . . . not available” in the community (Lamb & Weinberger, 2020; Pustilnik, 2005). In the criminal justice system. the objective of diversion is to reduce the number of persons with mental illness in detention; successful outcomes include reduced length of jail stay, reduction in charges, and lower recidivism, the former two often facilitated by mental health courts (Lowder et al., 2018). Yet, reductions in recidivism are heavily dependent on the health care system to sustain mental health treatment of justice-involved individuals (Abracen et al., 2016; Baillargeon et al., 2010). Successful outcomes for the health care system include stabilization of mental health symptoms through community-based treatment and medication and reduced number of acute mental health episodes (Wilkinson et al., 1995). However, continuity of health care may be deprioritized upon release from incarceration due to more immediate concerns such as lack of housing and employment (Dumont et al., 2012). Criminal justice and health care systems are entrusted with serving the population of justice-involved individuals with chronic mental health issues, yet function largely independent of each other via various lines of authority and funding (federal, state, local, private). Therefore, we advocate for a stronger theoretical conceptualization of the connections, measures, clients, goals, and objectives between these systems toward more effective management of chronic mental illness across sectors within and across different local jurisdictions. When these two systems manage justice-involved individuals with mental illness, we contend that neither system resolves the underlying problem to return the individual to the community as a fully functioning member of society. Rather neither system has the function to fully restore the individual without the other system’s assistance. So, the individual is in a state of limbo, as neither system takes complete comprehensive action(s).
A disconnect between the process of diversion and the outcome of diversion as defined by the two systems. Processes are a set of activities or steps that are interconnected; versus outcomes are a desired end result of a process. As defined by the criminal justice system, the process of diversion minimizes contact with the criminal justice system by shifting involved individuals away from the standard steps of arrest, prosecution, and incarceration with the outcome of community reentry without subsequent contact (Mueller-Smith & Schnepel, 2021). As defined by the health care system, the process of diversion is transferring individuals from acute psychiatric emergency service to community-based mental health services with the outcome of stabilizing a chronic medical disorder to reduce risk of relapse and reentry into psychiatric emergency services (McNiel & Binder, 2005). A disconnect occurs, and consequences follow because of failure to reintegrate individuals within society, at the juxtaposition of the two systems. The systems share the objectives of (a) rehabilitation, different definitions: criminal justice process of re-educating and retraining in individuals who commit crimes (Martinson, 1974) versus process of optimizing function and reducing disability in individuals who lost them because of a disease/injury Cohen et al., 1990, (b) efficient case processing, and (c) reducing system resources devoted to one individual. But defining and detecting individual successful re-entry into civil society (Rawls, 1971) becomes convoluted as a result of the systems having inconsistent definitions, jurisdictions and boundaries during the process of diversion. Because of the disconnect, a cycle of reentry, repetition, reappearance, recidivism, and reprocessing are created (Cohen and Felson, 1979).
The concept of diversion is difficult to formally define because diversion is being defined by collective action by each jurisdiction (Mueller-Smith & Schnepel, 2021), which is in turn, informed by the community attributes and street-level settings of each distinct locale (Lipsky, 2010; Ostrom, 2011). It is notoriously difficult to understand and report the nuances of each of these local program settings because of the number of the different programs (Mueller-Smith & Schnepel, 2021), the multitude of meaning (Stallworth, 2015) each community assigns to diversion, and barriers for information sharing between organizations within each system (Asheim et al., 2011).
The article is organized as follows: (a) discusses the lack of normative theory explaining diversion, (b) examines diversion policies effects from one system on the other, (c) explores the gap between the two systems when performing diversion, (d) proposes a system theory approach to describing diversion, and (e) calls for future research to test the proposed systems theory.
Lack of Normative System Theory of Diversion
A distinct lack of a normative system theory of diversion at the intersection of the criminal justice and health care systems is apparent. A normative theory of diversion would provide a framework for understanding the goals of diversion, measure the types of programs and services that are most effective, and determine the best way to deliver these programs between the criminal justice and the health care systems. Without such a theory, it is difficult to make informed decisions about how to optimize diversion programs and services. Across the systems, diversion represents a major criminal justice and public health issue stemming from a complex history of policing, corrections, treatment, and management of mental health disorders. Thus, at the systems level, a contradiction occurs, diversion instead of punishment can be viewed as a reward for deviance by one system and as justified therapy by the other system. Nevertheless, each system’s understanding of what is meant by diversion—and how the objective of diversion is achieved—is defined in a manner categorically independent of the other system. The entire concept of diversion becomes muddled when the systems converge with one another when individuals who would otherwise be categorized as having a mental illness engage in criminal behavior.
The criminal justice system is based on an individual having the mental capacity to understand their behavior in relation to societal norms regarding laws and rules (Malinowski, 1932; Platt, 1965). An individual with mental illness may have lapses in understanding those same societal norms, thus, the US justice system was initially structured to characterize individuals with mental illness as: “either furious or melancholic. These two labels symbolize the extremes of behavior which society has designated ‘mentally deviant’; both definitions have played major roles in legal theories of criminal responsibility” (Platt, 1965). Many of the terms historically used to describe individuals with mental illness are today considered offensive, yet it is relevant to note that the negative connotations tied to many of these terms shaped the criminal justice and health care landscape. Deviation is considered outside the boundaries of the social norm and the only option is to force a punitive form of compliance to bring the individual back into the system of social order. Conversely, the health care system is based on quickly diagnosing symptoms so treatment can occur, and an individual can return to a state of functionality. An individual with mental illness most often enters the health care system through psychiatric emergency services because of behavior which is not within the bounds of society’s norms and are considered difficult patients (Harris et al., 2016). The difficult patient with mental illness is considered chronically ill requiring continuous treatment, professional monitoring, continuity of care, and is at risk for relapse requiring acute treatment at the time of relapse (Bachrach, 1988).
The need for both criminal justice and mental health professionals is to act in concert to not only treat the mental illness but also to maintain social order (Sullivan, 1998). Local communities’ respective law enforcement and health care agencies were not created nor were they funded to provide services for large numbers of individuals with mental illness (Mongelli et al., 2020). Diversion releases individuals with mental illness into community treatment because it is more cost-effective and potentially more therapeutically effective than being in jail (Cowell et al., 2004). Nonetheless, community treatment is a broadly defined concept that requires long term adherence to therapeutic treatment(s) but is not equipped to mandate compliance (World Health Organization [WHO], 2003). Justice-involved individuals with mental illness who need stable community treatment to avoid jail frequently lack the resources to maintain stable treatment (Dumont et al., 2012).
Diversion Occurs at Systems Nexus
There is a nexus where the criminal justice and health care systems connect. Nexuses can be complex and difficult to manage, especially for diversion policies and programs. This is because they involve multiple stakeholders in different systems, each with their own interests and priorities. Nexuses can be dynamic, as changes in one system can have multiple effects on the other system; the nexus approach provides a lens to understand dynamic cross-sectorial interactions, manage limited resources, and consider the synergies and impacts of decisions that extend beyond one specific system (Afshar et al., 2022). Diversion policies within the criminal justice system affect the policies within the health care system and vice versa and in some cases may conflict because neither system when enacting policy accounts for the other system. For a nexus to function when two systems intersect, definitions need to be understood and agreed upon across both systems (Stone, 1997).
Confusion is created because diversion definitions in criminal justice and health care are not consistent (Gittner & Dennis, 2021). No common definition of diversion between the systems creates conditions for imperfect (cyclical) jurisdictional transfers of justice-involved individuals with mental illness. This is because both systems resort to defining individuals within their system context as “cases” that can be processed again in a narrow context versus a context spanning definition that captures the nuances of an individual with both justice involvement and mental health needs. The words used to describe individuals within each system have very different connotations. In the criminal justice system, an individual is considered a perpetrator, offender, inmate, or prisoner, versus the health care system where an individual is considered a patient or client (Schneider & Ingram, 1993). Functional outcome definitions for justice-involved individuals with mental illness are also different in the systems; productive citizen, criminal justice (Rawls, 1997), versus healthy well-being, health care (WHO, 2003).
In the criminal justice system, diversion describes a wide array of programs ranging from pre-arrest counseling by the police rather than arrest, to admission to an in-jail treatment program during detention center booking, to court ordered alternative sentences (Steadman et al., 1994). Here, diversion program outcomes are based on avoiding or reducing incarceration rates or charges and transferring jurisdiction to a non-criminal justice program. In the health care system, the definition for diversion pertains to alleviating facility overcrowding, maintaining appropriate facility capacity (Geiderman et al., 2015; Ramirez et al., 2009), and has nothing to do with treatment, nor is it related to addressing the needs of individuals with mental illness as in the criminal justice system. We suspect because acute mental illness is often associated with a need for increased resources in both systems, ultimately at the nexus, the criminal justice and health care systems rely on their respective conceptualization of diversion to reduce their system resource expenditures. Each system, then, focuses on diversion from their system. The lack of shared meaning at the system nexus creates competition to discharge the individual out of their respective system rather than focusing on unified diversion to assure each individual has a successful outcome.
Diversion Fills the Gap Between Systems
From a systems perspective, diversion is also operationalized differently depending on the entry of an individual with justice involvement and mental illness into one of the systems. Each system has multiple levels (micro-, meso-, and macro-) but individuals enter both systems at the respective intersection of the micro- and meso-level. Micro-, meso-, and macro- are terms used to describe different levels of system organization. Diversion includes many crisis services used to intervene after the onset of an acute symptom or behavior but before an individual has either (a) been admitted to a health care facility or (b) engaged in arrest-worthy criminal conduct (Draine & Solomon, 1999). Diversion may work well within each system; however, justice-involved individuals with mental illness require the criminal justice and health care systems to act in a concerted manner (Figure 1: Proposed Systems Theory of Diversion) at both the meso- and macro-levels (Rogers et al., 2019). Knowledge of the policies, structures, processes, procedures, and outcomes of both systems is necessary to explain unified diversion. At the micro-level, both systems independently intersect with individuals. Diversion programs reside at the meso-level in both systems and do intersect. But at the macro-level where policies, resources and priorities are established the systems do not intersect. Intersection may not mean coordination and in many cases, diversion occurs at the gap between systems.
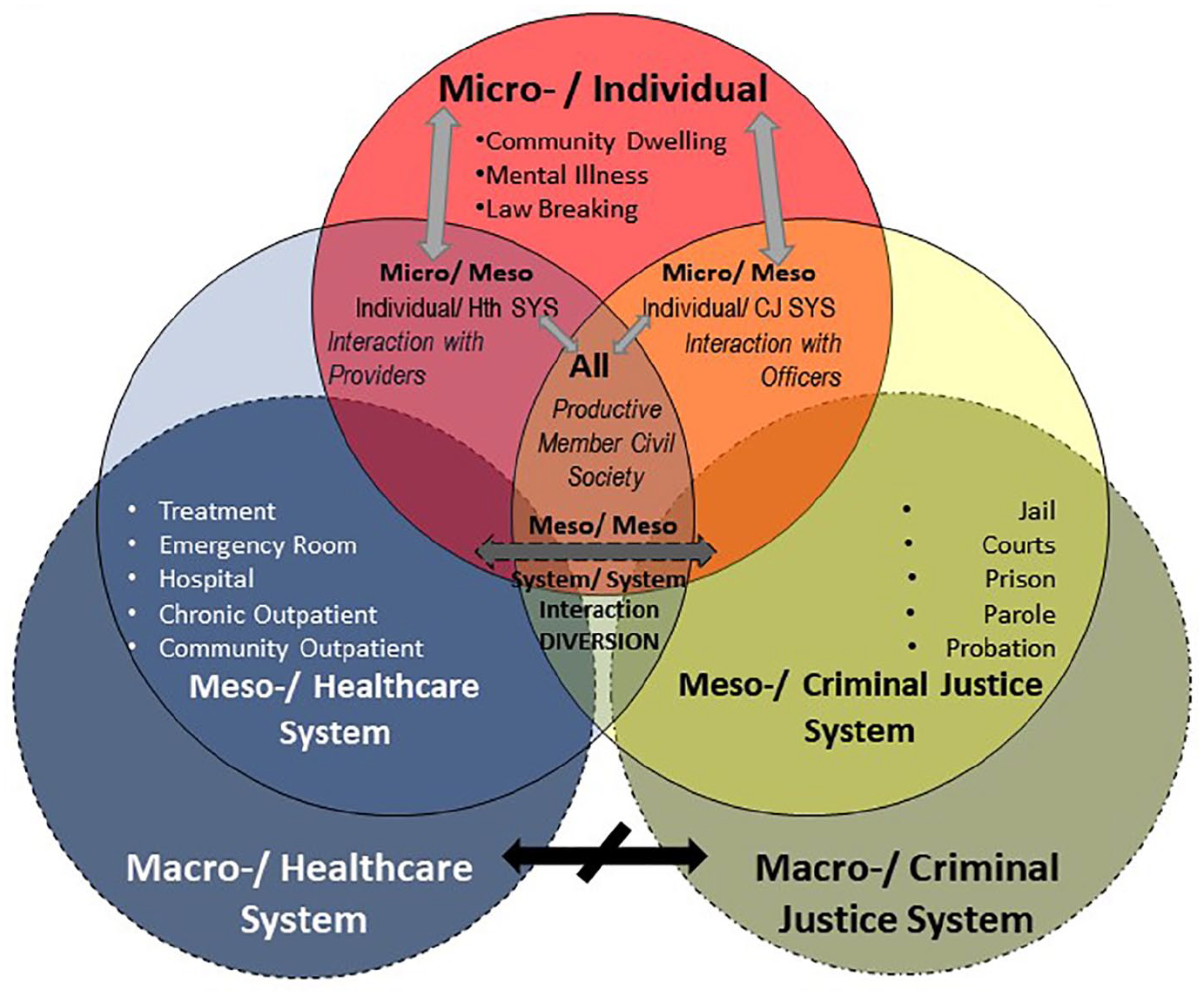
The Diversion Nexus of the Criminal Justice and Health care Systems.
System Boundaries: Macro, Meso, and Micro
Confusion is created because as previously discussed, the constructs between the criminal justice and health care systems are not consistent. Both systems resort to defining individuals within their contexts as cases processed in a narrow context versus a context spanning definition that captures the nuances of an individual acting reciprocally through criminal justice involvement and mental health treatment.
Macro-Level: Criminal Justice System
Macro-level services within the criminal justice system use specific laws to deliver the desired outcome, an interdependent civil society (De Tocqueville, 1835/2015, pp. 272–274). Criminal justice macro-level system boundaries are rooted in control of society, institutions, norms, and individuals (De Tocqueville, 1835/2015, pp. 131–145). Boundaries created for the criminal justice system are grounded in the law based on jurisdictional boundaries. The boundaries are geographic (States, Counties, Cities) and cultural with broad mandates for government to act (e.g., reduce economic deprivation, strengthen social support) (Ostrom, 2011; Pratt & Cullen, 2005). At the macro-level criminal justice system, the social impacts of the system are assessed, both positive and negative, and a determination is made whether the system behaves and distributes resources in a way that conforms to basic tenets of equal protection under the law, due process (Frank & Munro, 1950). The macro-level criminal justice system views social support and institutional burden as the strongest predictors of crime/criminal behavior (Cullen, 1994). The basis for the criminal justice system is premised on an individual behaving according to the societal norms (i.e., laws and rules). An individual with mental health issues may not have the capacity to understand those same societal norms in a manner consistent with the macro-level criminal justice system controls. Thus, the macro-level criminal justice system views individuals with mental health issues as difficult inmates with high resource needs (Haney, 2017; O’Keefe & Schnell, 2007).
Macro-Level: Health care System
Macro-level services within the health care system use specific treatments to obtain the desired outcome, a functional individual with positive emotions, psychological functioning, and social functioning (Keyes, 2007). Mental health care is a part of the health care system but is not clearly integrated within the health care system at either the macro- or meso-levels, rather mental health treatment is decentralized throughout (referred to as the “mental health non system system” Frances, 2020). Health care system macro-level boundaries are rooted in symptom treatment; boundaries focus on entryways and flow through the system creating a dynamic moving individuals through the system in a graduated process, escalating and quickly deescalating care to return individuals to either the base of the system or out of the system altogether (Wagner, 1998). The macro-level health care system diagnoses symptoms so treatment and disease management can occur. The boundaries are designed to maximize efficiency during processing as many patients (i.e., cases) as possible through the orderly tiers in the system. Even though mental health is part of an individual’s health, the macro-level health care system has been optimized to prioritize and process physical symptom treatment (Wagner, 1998). An individual with mental health issues most often enters the health care system in a disordered fashion creating difficulty in efficient case processing and impeding macro-level health care system policies. Thus, the macro-level health care system efficiently processes cases by moving them through the system to less intense care (Wagner, 1998). An individual diagnosed with mental illness is different from one with physical symptoms. Thus, the macro-level health care system considers individuals with mental illness as difficult patients (McNiel & Binder, 2005).
Meso-Level: Criminal Justice System
The meso-level criminal justice system encompasses the delivery and organization of law enforcement services including patrol, arrest, booking, detention, charge disposition, court proceedings, probation, and parole. Contact between law enforcement and an individual initially begins because an individual’s behavior is outside or at the fringes of the law. Civil society covenants dictate socially acceptable behavior and when individuals’ behavior deviates, law enforcement’s purpose is to squelch the deviant behavior in accordance with the laws (Verma & Jaiswal, 2010). The criminal justice system is premised upon the individual understanding their behavior, so they can be punished for said behavior, and then return to society with an implied understanding that the punishment has deterred repeat offense, or in the case of parole, that the person’s risk is reduced and remorse sufficient to reintegrate into society (Ward & Maruna, 2007, p. 32).
Conformity with the laws is enforced by the criminal justice system and deviation is punished with the goal of eventual rehabilitation (G. F. Cole et al., 2021, pp. 24–25). Meso-level criminal justice system policy output is to rehabilitate and return individuals to function within civil society. Success in achieving the system’s overarching objective is measured by the collective rate of recidivism (Lowder et al., 2018). However, once time has been served, the individual is considered rehabilitated whether or not the individual has fundamentally changed their deviant behavior patterns with little lasting impact on recidivism (Lösel, 1995; Sechrest et al., 1979; Ward & Maruna, 2007). It is important to note here that repeat offenders, those deemed as such by the system by the frequency of their deviant behavior are subject to increasing levels of punishment. Specifically, longer episodes of internment and exposure to programs aimed at rehabilitation are dependent upon sentencing guidelines (Tonry, 2006). All components at the meso-level criminal justice system work in concert to turn an individual into a case and efficiently process the case to their culmination in punishment or rehabilitation. However, as mentioned earlier; the criminal justice system process does not always produce productive citizens. Rather, the medicalization of deviant behavior as mental illness calls into question both a) the appropriate punishment for the behavior, and b) the ability to be rehabilitated from a chronic mental illness (Rafalovich, 2020).
Delving into the meso-level criminal justice system, it becomes quickly apparent criminal and legal processes are ordered in a structured hierarchy designed for efficiency and control (Feeley, 1979). The order is because the criminal justice system as a whole is composed of both law enforcement and legal judiciary agencies in the tradition of federalism (Randazzo, 2008). Throughout the system then, there is a structured hierarchy within a bounded jurisdiction where turning an individual into a case proceeding in due course through the system’s jurisdiction. The criminal justice system as a whole is constrained, and control is emphasized in that (a) law enforcement officers use strict process control when enforcing the law using patterns to codify individual actions into crimes, and (b) officers of the court use strict rules of judicial procedure when deliberating guilt or innocence of a crime as well determining the degree of punitive action taken by the system based on the required compliance with the law (G. F. Cole et al., 2021). Each agency within the meso-level criminal justice system from its staff (officer categories hierarchy) to its physical structure (police station, dispatch, jail, prison) to its processes (arrest, charges, booking, detention) are designed to strip individuality by substituting case numbers and requiring compliance. Legal judicial agencies again are hierarchical tiers of legal rules and codified charges with its staff relegated into specific roles (magistrates, judges, defense attorney, prosecution, probation, and parole officers) and specific agencies (courts, bondsman, probation, parole) (G. F. Cole et al., 2021; Feeley, 1979).
Meso-Level: Health Care System
The meso-level health care system encompasses the delivery and organization of health care services and clinical procedures including primary, secondary, and tertiary prevention, acute and chronic symptom management, treatment, and delivery of mental health services. Contact between the health care system and an individual initially begins because an individual is either at risk of or experiencing symptoms of a disease. Symptoms are managed using a variety of interventions to treat and improve an individual’s quality of life to return them to a functional state of physical and mental well-being so they can contribute to society (WHO, 2003).
The health care system rewards treatment adherence but also requires individuals to actively manage as much of their treatment as possible outside the health care system within the community (Wagner et al., 1996). However, treatment adherence is less than 50% for most individuals with severe mental illness (Xia et al., 2020). The entryway into the health care system for mental health is not as clear as for physical health, identification, and management of mental illness progression at lower levels of care is fragmented and driven by insurance coverage decisions, not clinical decisions (Frances, 2020). Furthermore, 25% of the population lacks a primary care provider and may have no mental health screening prior to an acute mental health episode (Levine et al., 2020). Numerous individuals with mental health issues never come to the attention of the health care system until an acute episode occurs (Kessler et al., 2007). Instead of entering the health care system at the base, individuals with mental illness many times enter the health care system at a much higher level (ambulance or Emergency Room) because of an acute episode where costs and labor intensity are much higher (Tsemberis, 2010). All components at the meso-level health care system are designed to increase patient care effectiveness by efficiently turning an individual into a case and treating the case at the lowest possible level of intensity to reduce costs (Rosenthal et al., 2010). However, treatment for mental illness does not have the same restorative capacity as treatments for acute physical illness. Pneumonia can be completely treated and cured; an acute severe mental illness break can be treated but will not be cured. Health care providers are trained to reduce symptoms and do not emphasize factors relevant for treating individuals with chronic mental illness with a high risk of arrest for criminal behavior (Bewley & Morgan, 2011).
However, the meso-level health care system as a hierarchical arrangement is dissimilar to the ordered hierarchy of federalism in the criminal justice system. There is no hierarchical legal basis for the health care system, rather it is fragmented and driven by insurance, diagnosis, and care access. The health care system is hierarchical in structure and is a four-tier system of care delivery (Reid et al., 2005). The macro-level is where all societal constructs and policies are grounded and where the social determinants of community health are based (broad health care policy) (Ostrom, 2011); the other three tiers are at the meso-level built for health care delivery (Reid et al., 2005). Entry points into the meso-level health care system are numerous: physician office, clinic, ambulance, emergency room, and so on. As a physical condition either becomes more severe or an acute episode occurs, entryways into the health care system become fewer and the cost and labor-intensity exponentially increase (Weine, 2017). Entryways and flow through the meso-level health care system create a dynamic that moves individuals through the system in a graduated process, escalating and quickly deescalating care to return individuals to either the base of the system or out of the system altogether (Wagner et al., 1996).
Micro-Level: Criminal Justice System
The micro-level criminal justice system focuses on individual interactions, explaining actions between criminal justice professionals and offenders. Criminal justice professionals make rational decisions in specific cases and follow the proper procedures, processes, rules, but have significant discretionary authority (G. F. Cole et al., 2021). Services are delivered on an individual basis with one-on-one interactions between law enforcement personnel and the individual. Decisions by individuals to commit a crime may or may not be rational, but micro-level criminological theories assume rationality with individuals acting in their own best interests (Matsueda, 2020). Theories of crime at the micro-level assume behavior is self-promoting (Akers, 2009) but are criticized for being too simplistic. Differential association and social learning theories specify attitudes are learned thus affecting an individual’s decisions and behaviors, general strain theory contends individuals’ negative emotions are minimized by behaviors and social control theory asserts behaviors simply maximize an individual’s self-indulgence (Proctor, 2010). Individuals who lack the capacity to understand (cognitive impairment through mental illness or substance use disorders) their behaviors cannot be explained by existing theories (Proctor, 2010). Social theories of crime cannot easily explain how the purposive acts of individuals are constrained by behaviors outside of community social norms (Sampson & Groves, 1989).
Law enforcement and court officers have wide discretion in their decisions and interactions (Lipsky, 2010), their street-level decisions enforce civil society’s given rules, laws, and social norms (G. F. Cole et al., 2021). When dealing with individuals with mental illness, officers also function as policy decision makers regarding diversion and their micro-level decisions have lasting policy implications at the criminal justice meso- and macro-levels (G. F. Cole et al., 2021; Lipsky, 2010). However, exerting social control over individuals assumes an individual has the mental capacity to understand socially acceptable behavior.
Dating back to the beginnings of the Anglo-Saxon jurisprudence system, individuals with mental illness who committed crimes, were considered responsible for their actions but were not guilty of crime because they did not have the intent or reason to understand the crime (Platt, 1965). Justice-involved individuals with mental illness were exempted from punishment with a system developed to label, treat, and warehouse them (Platt, 1965). Interactions between officers and individuals with mental illness demonstrate the extensive latitude of discretion officers can exercise (Lipsky, 2010). Formal criminal justice system processes are more likely when there is evidence of a crime; the individual has a criminal history, is eligible for admission to a hospital or other social support system; the encounter exceeds the community’s tolerance for deviant behavior; and there is a high likelihood the individual will continue to cause problems (Watson & Angell, 2007). Harsh crime control and drug laws have reduced sentencing discretion (Lurigio, 2011), but guidelines are beginning to change to treat an individual with mental illness differently by recognizing their susceptibility to serious harm within the criminal justice system (Johnston, 2013). Nonetheless, because of limited availability of community-based mental health treatment, many times the only option is arrest, sentencing, and incarceration rather than diversion (Lurigio, 2011).
Micro-Level: Health Care System
The micro-level health care system focuses on individual interactions, where health care providers treat patients. Services are delivered on an individual basis with one-on-one interaction between medical providers and the individual. The disordered entry of an individual with mental health issues creates a ripple effect within the micro-level health care system. Health care providers must both treat and also maintain order (Sullivan, 1998); there is an expectation patient behaviors should be controlled. For an individual with mental illness, behaviors associated with the disease are often seen as unacceptable and contrary to social norms (Sullivan, 1998). The biomedical model of patient care is reductionist, reducing illness to singular treatable causes using disease management; it is still the predominant model of care because of focus on diagnosis and treatment which are orderly and billable (Wade & Halligan, 2004). The biopsychosocial model (Engel, 1977) of patient care interweaves the social psychological and behavioral dimensions of disease into a theory of health care, it better accounts for treating patients with mental health issues (Wade & Halligan, 2017). However, it was never intended to replace the biomedical model, and it suggested extending the model so the health care providers would look outside symptomology and treat the patient’s entire social condition (Wade & Halligan, 2017). Addressing a patients’ entire living situation, however, is beyond the health care micro-system boundaries.
There is wide variation among providers’ skills in dealing with mental health issues (Price et al., 2015). The more time a provider has to deal with de-escalation, the less time they have to actually treat the individual (Price et al., 2015). Erratic behavior in individuals with mental illness leads to inefficiency in case processing at the micro-level (Harris et al., 2016; Knaak et al., 2017).
The diagnostic relationship between patients and physicians is paramount, rooted in a patient-centered approach (Bodolica et al., 2016). But, there is significant latitude in diagnosis and treatment of individuals with mental illness, especially when acute episodes occur. Because of this lack of clarity on stabilization and treatment of individuals with mental illness, the individual can languish for hours (and sometimes) days in an emergency room (Nolan et al., 2015). In the last 20-years (2006 onward), for example, there has been a 50% increase in emergency department visits involving mental health issues (Weiss et al., 2016). Individuals with mental health issues require more resource-intensive care, have longer wait times than other patients, and often receive substandard care while they wait in the emergency department (Nolan et al., 2015). But psychiatric hospital beds are expensive thus governments are increasingly seeking ways to save money and the threshold for mental health hospitalization has tightened (Dvoskin et al., 2020) leading to few options within the health care system for diversion.
A Nondisciplinary Theoretical Grounding of Diversion
A nondisciplinary theoretical grounding of diversion is a way of understanding diversion that does not rely on any one discipline, such as criminology, law, medicine, or psychology. Instead, we draw on insights from a variety of disciplines allowing us to conceptualize diversion in a holistic fashion. Does diversion really exist as a separate system or does it exist in the gap between the meso-level criminal justice and health care systems? Even though diversion is located at the nexus of the criminal justice and health care systems, diversion theory does not spring from either discipline (D. H. Cole & McGinnis, 2017). The Theory of Trans-institutionalization describes an inverse relationship between psychiatric bed numbers and prison population rates (Mundt & Konrad, 2019). It is the only theory that describes the gap between the two systems. Unfortunately, because of the difficulty in studying the actual nature of the relationship of individuals moving between the two systems the theory has not been tested (Mundt & Konrad, 2019). Ergo, diversion steps into this gap, a perceived unstudiable space. The concept of diversion is principally grounded in two different theories: labeling theory and differential association/social learning theory. Labeling theory emphasizes the stigma and negative consequences if an individual is labeled as “mentally ill” or “a criminal” (Becker, 1963). Differential association/social learning theory uses universal identifiers to explain the origin of crime as mechanisms outside of specific structural, social, and individual conditions (Akers, 2009; Cressey, 1960). Diversion is conceptualized by both systems as an outcome of an authority transfer versus a continuum of service to an individual with mental illness. Diversion is used by both systems to reduce costs to the intake agency and becomes a main outcome rather than the actual success of the individual undergoing diversion. For example, deinstitutionalization at its most basic form remains a mechanism to shift costs from one jurisdiction to another (Harcourt, 2011).
At the micro-level, criminal justice professionals are the de facto gatekeepers for both the criminal justice system and mental health subsystem (within the health care system); officers, responding to incidents with an individual with mental illness, play a pivotal role in shaping outcomes (Watson & Angell, 2007). From the criminal justice perspective, theories of diversion have been limited to the micro-level without consideration of the macro- or meso-levels (Pratt & Cullen, 2005) leading to the deficit of theory explaining diversion programs spanning criminal justice and health care systems. Macro-level health care theories explain service delivery and institutional strain as the strongest predictors of reducing services utilized and returning individuals to function within society (Mair & May, 2014).
Diversion does not uniformly occur at the macro-level between the two systems of criminal justice and health care. Rather, diversion for justice-involved individuals with mental illness occurs at the nexus of the micro- and meso-levels of the criminal justice and health care systems. For a theoretical grounding of diversion to occur, the proposed theory describes the micro- and meso-level interactions within and between both systems as a system unto itself.
New Institutionalism
At the meso-level, individuals operate within a social network and are then grounded by their community connections. An individual’s social network is surrounded and defined by their communities’ various degrees of support and environmental factors. Individual factors may dictate insurance status, access to mental health care, or the awareness of need for mental health care. However, community-specific agencies and resources dictate the types of mental health care available during crisis, the types of first responders available to manage crises (e.g., crisis teams, mental health police officers), and the options for diversion at various points (Asheim et al., 2011; D. H. Cole & McGinnis, 2017).
The meso-level criminal justice system is designed in such a way that the individual is accused of deviant behavior and charged with a crime, thereby losing their free choice. The aim of the meso-level criminal justice system is rehabilitation, restraint, retribution, and deterrence as the path to re-entry within civil society (Dvoskin et al., 2020). Punishment as a time-based process is woven into the system, where individuals are required to atone for their actions. Criminality aside, our concern is that this is objectively true when an individual has mental illness, their behavior may not be completely within their control leading to behavior outside the norm, the significance being that the criminal justice system begins with a premise the individual being rehabilitated is capable of rehabilitation (Talati, 2009). The criminal justice system is based upon due process; whereas an individual with mental illness may not have the capacity to understand due process and be rehabilitated.
This does not mean that diversion is theoretically bankrupt, however, but is rather based on differing constructs of diversion by the two systems. Explaining and evaluating diversion in the intersection of the two systems is not possible without a unified theory of diversion. A normative theory of diversion explains the intersection and provides definitions for constructs spanning criminal justice and health care systems.
The constructs encompass both the criminal justice and health care agencies providing services. Agency service area, service type, and service scope are defined internally and externally, and inter-agency relationships are demarcated internally and externally to each system’s formal meso-level boundaries. Negotiation of interagency transfers and jurisdiction sharing become key constructs. Therefore, connectivity of agency relationships becomes highly relevant. The strength of inter- and intra-agency connectedness is related to case processing ability and the seamless jurisdictional transfer of cases within and between agencies. [Inter] Dependency of agencies also comes to bear. Agency orientation bias ranging from treatment to punishment governs their accountability practices, organizational mission and values, and employee motivation(s) and action. The internal agency bias, which is of particular relevance in context to the criminal justice system, can affect diversion processing and return of the case to civil society. System complexity then also contributes to the structural conditions surrounding diversion; thus, application of a unified diversion theory needs to be modulated by the complexity of the system diversion occurs within.
Diversion at the meso-level involves individuals exhibiting symptoms of mental illness or who have a diagnosis of mental illness and who meet one or more broad categories—minor offenses, nonviolent offenses, first time offenders, frequent offenders, and/or persons who have clearly broken a law. Diversion of these individuals does not require or bring about an individualized treatment plan, but rather channels them into programs that are broadly designed to connect them to mental health resources while living in society, rather than a correctional facility. Macro-level structures provide the setting for individuals to interact by building meso-level programs with micro-level structures that provide the framework for future encounters between individuals, as micro-level interactions change over time, the underlying meso-and macro- structure also changes.
Conclusion
At its best, diversion has the potential to keep individuals with mental illness out of jail for nonviolent offenses and to maintain mental health with stable community-based treatment in the health care system with minimal need for high resource utilization of the emergency department. The proposed theory of diversion encompasses: (a) hand-offs between organizations and agencies in different systems; (b) inter-agency relationships; (c) individual case flow, (d) system complexity including policies, procedures, and interdependencies; and (e) managing roles, accountabilities, and motivations between all the different agencies. We suspect that there is a disconnect between the outcomes of diversion and the actual real world street-level implementation of diversion. The disconnect occurs and consequences follow when individuals fail to reintegrate within society. Disconnection is the greatest at the systems nexus where the reintegration objectives (rehabilitation, case processing efficiency, individual stability) become entangled in the gap between the macro- and meso-level criminal justice and health care systems (Gittner & Dennis, 2021). Because of the disconnect, a cycle of instability, reentry-rearrest, and recidivism, is created within and across both systems, which is most apparent at the micro-levels.
At its worst, diversion represents a new deinstitutionalization of individuals with mental illness from detention facilities into the community. Detention facilities may nonetheless stabilize individuals to an extent that their incarceration appears unnecessary, and perhaps inhumane. Whereas the deinstitutionalization of state mental hospitals was followed by closure of these facilities, detention centers do not have the same ability to permanently close after release of diverted individuals. That is, no institution exists to take on these individuals in the way that detention centers have assumed the burden of mental hospital deinstitutionalization. As such, many diversion programs may reduce length of stay in detention centers but increase recidivism and/or health care costs.
To answer the question: Is diversion the new deinstitutionalization? We argue that policy experimentation is proceeding, at the local micro- and meso-levels where a wide variety of policies and programs merging criminal justice/health care systems of diversion are being created (Asheim et al., 2011; D. H. Cole & McGinnis, 2017). Unfortunately, evaluation of what is and is not working is difficult due to the proliferation of experimentation occurring across jurisdictions. Lacking systemic uniformity, a theoretical framework of diversion is necessary for future research efforts to test the proposed systems theory of diversion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Drs. Gittner and Dennis received financial support for the research, from the United States Department of Justice Bureau of Justice Assistance Award MO-BX-0031 and MO-BX-0030. Dr. Forbis received no financial support for the research, authorship an publication of this article.