
Abstract
To understand the role of Medicaid in financing health services delivered through special education, program characteristics and covered services were compared from all 50 states and Washington, D.C. Data were collected from school-based fee schedules and policy manuals available through state Medicaid or education agencies. Except Wyoming, all states bill Medicaid for school-based health services, but there is substantive variation across states in services covered. The service categories most often covered by states’ Medicaid special education programs are speech–language/audiology, occupational/physical therapy, and behavioral health. Almost all states use a fee-for-service payment methodology to reimburse for services. Implications for the delivery of care to and health outcomes of students with disabilities are discussed.
In the United States today, more than 6 million children with disabilities receive special education services in public schools (U.S. Department of Education, 2012). Special education services are funded primarily under the Individuals with Disabilities Education Act (IDEA), which has been in effect since 1975. IDEA Part B provides guidelines state educational agencies must meet to receive federal funding for special education programs, and the law ensures that children aged 3 to 21 years with a disability receive a free and appropriate public education (IDEA, 2004). To be eligible for special education under IDEA, a child must have one or more disabilities that affect his or her ability to learn. The disability categories covered under IDEA include autism spectrum disorder (ASD), deaf-blindness, deafness, developmental delay, emotional disturbance, hearing impairment, intellectual disability, multiple disabilities, orthopedic impairment, other health impairment, specific learning disability, speech or language impairment, traumatic brain injury, and visual impairment.
If a child is deemed eligible to receive special education services, a team of at least one parent, a regular education teacher, a special education teacher, and a representative of the school district develops an individualized education program (IEP) for the child. The IEP specifies the school services to be provided, how often the services will be provided, present levels of academic performance (e.g., test scores and grades), any accommodations or modifications necessary for the student, and achievable goals for improvement (IDEA, 2004). In addition to educational services, IDEA specifies that children are entitled to receive medically necessary related services that are needed to benefit from special education. These related services may include but are not limited to speech–language pathology and audiology services, psychological services, and physical therapy (PT) and occupational therapy (OT; including orientation and mobility services), and medical services for diagnostic or evaluation purposes, such as developmental or psychological testing (Turnbull, 2005). In addition, IDEA underscores the need to provide services for families and caregivers to enable children with disabilities to participate in the classroom (Cannon, Gregory, & Waterstone, 2013).
Although the disability categories included in IDEA cover a broad range of functional impairment and disability, the majority of students require a variety of continuous health services, including services such as PT, OT, and speech–language services, to actively participate in special education (Schieve et al., 2012). Prior studies have demonstrated that these health services provided through special education can help improve health and educational outcomes among children with disabilities (Boulet, Boyle, & Schieve, 2009; Szymanski & King, 1999; Volkmar et al., 2014). For example, children with developmental disabilities benefit greatly from early diagnosis and intensive treatment (Majnemer, 1998). Studies have demonstrated that developmental delays can be assessed reliably in schools, and schools can deliver behavioral interventions with beneficial outcomes such as reduced repetitive behaviors (Eber, Sugai, Smith, & Scott, 2002; Sugai et al., 2000).
Since IDEA’s passage, the program has been underfunded, leaving schools struggling to find sufficient financing to maintain their programs (Katsiyannis, Yell, & Bradley, 2001). In the 2011–2012 school year, federal IDEA funding covered only 16% of the total cost of educating children with disabilities, including both educational and related health services (Stahl, Albert, Dew, Lockovich, & Reynolds, 2014). Prior studies show that although schools play a dominant role in the provision of health services, access to these services can be severely hampered by lack of funding (Shattuck & Grosse, 2007). To help ensure appropriate access to care for students with disabilities, states often turn to other federal, state, and predominantly local resources to fund special education programs.
As a result, Medicaid, the U.S. health insurance program for low-income individuals, has become an important resource for financing health services delivered through special education for Medicaid beneficiaries (Centers for Medicare and Medicaid Services [CMS], 2012). Medicaid is a federal–state partnership that is primarily managed by states. Each state separately specifies the eligibility requirements, covered services, and delivery systems operating within the Medicaid program. The federal office, CMS, defines a set of mandatory benefits that must be covered by every state (e.g., inpatient and outpatient hospital services and early and period screening, diagnostic and treatment services [EPSDT]), and a set of optional benefits (e.g., PT, prescription drugs, and dental services). Although state Medicaid programs typically cover a comprehensive set of services, there is considerable variation across states in the scope of coverage of optional benefits (Courtot, Lawton, & Artiga, 2012). Currently, school-based health services programs for children with disabilities are an optional benefit, and each state is given considerable autonomy in defining the characteristics of this benefit.
The cost of Medicaid for state and federal governments has grown dramatically over time (Kaiser Family Foundation, 2011). In response, CMS and states have taken different actions to reduce the cost of the program. One common tactic is transformation of the delivery system. Most states have made strides to transition away from providing services within a fee-for-service delivery system, where providers are paid for each service delivered to a Medicaid beneficiary, toward a managed care delivery system. Providers delivering services through managed care organizations typically receive a set per member, per month (capitated) payment (Courtot, Coughlin, & Lawton, 2012; Kaiser Family Foundation, 2014).
As the total cost of the Medicaid program has grown, federal funding for school-based Medicaid programs continues to increase. In 2012, estimated federal Medicaid spending for health services delivered in schools totaled US$2.8 billion, but varied dramatically across states (CMS, 2012; Parrish, Harr, Anthony, Merickel, & Esra, 2004; Sopko, 2006). This is likely due to variation in Medicaid special education program characteristics such as covered services, and has important implications for accessibility of services (Bachman & Flanagan, 1999). In general, state Medicaid programs that cover more services often receive more federal funding and demonstrate greater service use compared to states that cover fewer services (LeBlanc, Tonner, & Harrington, 2001; Verdier & Zlatinov, 2013). This may suggest that variation in service coverage across state Medicaid special education programs has important implications for the amount of reimbursement school districts receive from Medicaid and the availability of school-based services (Jegers, Kesteloot, De Graeve, & Gilles, 2002; Newhouse, 1996).
Documenting variation in the services covered by Medicaid special education programs is therefore an important first step to understanding access to health services for children with disabilities and is particularly important for the many students who receive all or most of their health services in schools. However, no prior study has investigated variation in Medicaid-covered school-based special education services beyond broader service types. Furthermore, due to the complexity of these programs, it is difficult to understand, in practice, how variation in covered services across states affects Medicaid billing for services delivered to a child with a certain disability.
In addition, although program characteristics and reimbursement from Medicaid differs across states, little is known about variation in payment methodology used by state Medicaid special education programs. Prior research suggests that in addition to covered services, payment methodology has important implications for the cost and availability of services (Miller & Luft, 1994). In 2011, 74% of Medicaid enrollees were covered under managed care plans (Kaiser Family Foundation, 2011). The remaining 26% of Medicaid enrollees were covered under fee-for-service plans. Although a Medicaid enrollee may be covered under a managed care plan, states may still opt to carve out Medicaid special education programs and reimburse providers employed by the school using a fee-for-service method. However, no prior studies have investigated which options states use.
To fill these gaps, state variation in Medicaid special education program characteristics for children with disabilities were examined. More specifically, the following research questions were answered:
Method
Characteristics of state school-based Medicaid programs were collected in 2014 for all 50 states and Washington, D.C. The study was determined to be exempt by the Institutional Review Board for human subject protection.
Data Sources
Data were collected, coded, and entered by the lead author and reviewed by the second author. Document collection occurred from November to December 2013. Provider manuals (n = 28) and fee schedules (n = 17) that were specific to Medicaid special education programs and publicly available on Medicaid agency websites were used to gather service category coverage, type of services covered, current procedural terminology (CPT), and state-specific codes for each state. Information about payment methodology was gathered from publicly available Medicaid special education provider manuals (n = 48 states). For the five states—Vermont, North Dakota, Wyoming, Hawaii, and Washington, D.C.—that did not have publicly available school-based Medicaid provider manuals and fee schedules with the appropriate information detailing covered service codes or payment methodology, key informants from state Medicaid or special education programs were contacted via the phone to obtain appropriate documentation of Medicaid school-based direct service claiming. Informants were the directors of Medicaid special education programs or reimbursement directors and were identified on state school-based Medicaid, state Medicaid, or special education websites.
Procedures
Once documents were collected, data were coded from December, 2013, to April, 2014. A structured coding instrument was developed by the lead author in consultation with directors of three Medicaid special education programs and reviewed by the second author and can be made available upon request. The instrument included items measuring (a) service category coverage, (b) type of services covered within each service category, (c) specific billing codes covered within each service category, (d) number of billing codes covered within each services category, and (e) payment methodology. Service categories were based on the related services included in the IDEA law. Service types were based on EPSDT guidance (CMS, 2014), and payment methodologies were based on a review of 10 Medicaid State Plans. The instrument was pilot tested by the lead author on documents from 10 states and reviewed with the second author, and items were refined based on pilot results. More specifically, two service categories were added (nutritional services and targeted case management) and one payment methodology was added (bundled payment).
The lead author coded documentation for each state and Washington, D.C., and reviewed the results from the structured coding instrument with the second author. Given the nature of the information being collected, the authors decided that only one coder was necessary.
The authors determined which categories of services are covered under Medicaid special education programs based on the CPT or state-specific billing codes covered in each state. Services were classified based on the following 11 categories: (a) intake/evaluation (i.e., intake or evaluation service not specific to a service category and generally used to determine eligibility for special education), (b) speech–language/audiology services, (c) developmental diagnostic assessments, (d) vision services, (e) OT and PT, (f) behavioral health services, (g) nursing services, (h) personal aide services, (i) nutrition services, (j) targeted case management, and (k) EPSDT services.
With the exception of Wyoming, all states and Washington, D.C. directly bill Medicaid for health services delivered through special education programs. Wyoming was included in the study because the state provided documentation indicating that no school-based services were directly billed to Medicaid. Some schools or school districts in North Dakota and Tennessee seek reimbursement for services delivered through special education programs, but the two states do not have formal Medicaid special education programs. They were therefore excluded from the study. Based on these exclusions, characteristics of school-based services delivered through special education programs and covered by Medicaid are described for 48 states and Washington, D.C.
Although 45 study states and Washington, D.C., use national CPT codes to bill Medicaid, Connecticut, Pennsylvania, and New Jersey have developed state-specific school-based billing codes. Connecticut’s billing codes use different codes than national CPT codes to bill for services, but the services overlap and were therefore classified in the same way as national CPT codes. Pennsylvania only has billing codes for each category of service; codes for specific services are not available. For example, code 5 refers to PT, so Pennsylvania was coded as covering PT services. New Jersey uses one code for evaluation services, one code for bundled services delivered within the school district, and one code for bundled services delivered outside of the school district. The bundled payment service code identifies a single bundled payment rate for each service delivered to a child within a specified period of time. In addition to New Jersey, six additional states use bundled service codes. For these seven states that bill Medicaid using a bundled service code rather than using service-specific billing codes, documentation was reviewed to determine which categories of service were eligible for reimbursement under the bundle payment code. For example, Minnesota codes all services using CPT code T1018-School IEP service, bundled. This code can be used for OT/PT, speech/language audiology, behavioral health, nursing services, and personal aide services, so Minnesota was coded as covering these six service categories.
For the three most commonly covered of the 11 service categories, speech–language/audiology services, OT and PT, and behavioral health services, billing codes were further classified based on four types of services. Service types included screening, evaluation, individual treatment, and group treatment. In addition, behavioral health included a family services subcategory. These family services are important not only to help ensure that families have the services and support necessary to care for youth with behavioral health needs (Friesen & Koroloff, 1990) but, evidence suggests, also can produce better outcomes for children with mental illness (Dixon et al., 2001).
Information about Medicaid payment methodology was also collected. A state was coded as using one of the following methodologies: (a) fee-for-service, (b) bundled payment, or (c) capitation. A state was coded as using fee-for-service if providers receive compensation at a set rate distinct for each individual service. A state was coded as using a bundled payment method if providers are reimbursed based on a single, fixed rate for each service provided within a specified time period. A state was coded as using capitation if providers receive a set per member, per month rate.
Results
Coverage of Service Categories
Figure 1 summarizes the number of jurisdictions (48 study states and Washington, D.C.) that cover each of the 11 specific service categories for children with disabilities under the school-specific Medicaid program. The most widely covered service categories are speech–language/audiology services (n = 48, 47 states and DC, 98% of jurisdictions), OT and PT (n = 48, 98%), behavioral health services (n = 47, 96%), and nursing services (n = 38, 78%). In contrast, few states cover personal aide services (n = 22, 49%), developmental diagnostic services (n = 18, 37%), targeted case management (n = 17, 35%), intake/evaluation services (n = 16, 33%), vision services (n = 12, 24%), EPSDT services (n = 9, 18%), and nutrition services (n = 4, 8%).

Number of state Medicaid programs covering school-based health services categories within special education programs.
Types of Service Coverage
Of the 47 states and Washington, D.C., that cover speech–language/audiology services delivered through special education (98% of jurisdictions), 43 states and Washington, D.C., cover at least one speech–language/audiology-specific billing code (92%). Minnesota, New Jersey, Utah, and Vermont do not use any speech–language/audiology-specific CPT codes, but the states’ programs cover speech–language/audiology services under a bundled service code. Of the 44 jurisdictions that cover speech–language/audiology-specific CPT codes, 24 jurisdictions cover screening services (55%), all 44 jurisdictions cover evaluation services (100%), 37 jurisdictions cover individual treatment (84%), and 16 jurisdictions cover group treatment (36%) (see Figure 2). Of the states and Washington, D.C., that cover at least one speech–language/audiology-specific billing code, the number of codes covered ranges between one (Kentucky and Nebraska) and 46 (Virginia) (see Table 1).
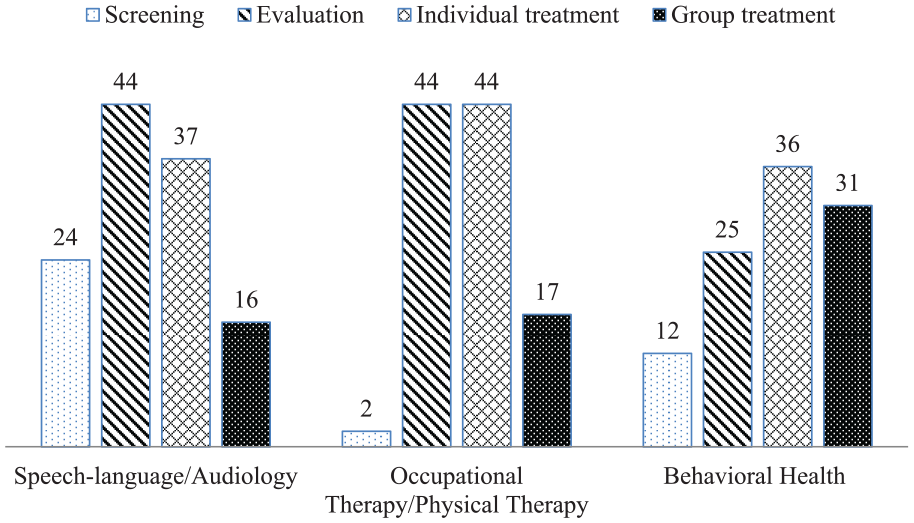
Number of states and Washington, D.C., covering service types within speech–language/audiology, occupational and physical therapy, and behavioral health categories.
Number of Speech–Language/Audiology Service, Occupational and Physical Therapy, and Behavioral Health Services Billing Codes Covered Per State.

Identical to speech–language/audiology services delivered through special education, of the 47 states and Washington, D.C., cover OT/PT services delivered in special education (98% of jurisdictions), 44 jurisdictions cover at least one OT/PT-specific billing code (90%). Minnesota, New Jersey, Utah, and Vermont do not use any OT/PT-specific CPT codes, but the four states’ programs cover OT/PT services under a bundled service code. Of the 44 jurisdictions that cover OT/PT-specific billing codes, two states cover screening services (4%), all 44 jurisdictions cover evaluation services (100%), all 44 jurisdictions cover individual treatment (100%), and 17 jurisdictions cover group treatment (39%) (see Figure 2). Of the states and Washington, D.C., that cover at least one OT/PT-specific billing codes, the number of codes covered ranges between two (Arkansas, Kentucky, and South Dakota) and 40 (Maine) (see Table 1).
Although 46 states and Washington, D.C., cover behavioral health services delivered through special education (96% of jurisdictions), 42 states and Washington, D.C., cover at least one behavioral health service-specific CPT codes (91%). Minnesota, New Jersey, Utah, Vermont, and Wisconsin do not use any behavioral health service-specific CPT codes, but they use a bundled service code that covers behavioral health services. Nebraska does not cover any behavioral health services within their school-based special education Medicaid program. Of the 42 states and Washington, D.C., that cover behavioral health-specific CPT codes, 12 jurisdictions cover screening services (30%), 25 jurisdictions cover evaluation services (60%), 36 jurisdictions cover individual treatment (84%), and 31 jurisdictions cover group treatment (72%) (see Figure 2). In addition, within behavioral health, 20 states cover family treatment services (47%). Of the states and Washington, D.C., that cover at least one behavioral health service-specific CPT code, the number of codes covered ranges between one (South Dakota and Washington) and 31 (Arizona) (see Table 1).
Payment Methodology
A total of 44 of the 48 study states and Washington, D.C., use a fee-for-service payment methodology for billing Medicaid for school-based services (92%), regardless of whether the service recipient is enrolled in a managed care plan. Four states, Minnesota, New Jersey, Utah, and Vermont, reimburse local education agencies based on a bundled payment rate (8%). Vermont, for example, combines all services provided in a given month to determine the rate billed to Medicaid. No study states reimbursed providers using a capitated payment methodology.
Variation in School-Based Service Coverage Across States: ASD and Depression
Examining how Medicaid school-based special education benefits within states map on to the treatment needs of an individual can be helpful to understand how the variation in services offered affects access to services. First, consider a child with ASD that receives services under IDEA Part B. According to a recent bulletin from the CMS, the following service types should be available to a child with ASD covered under Medicaid: behavioral therapies, PT, OT, speech, hearing and language services, EPSDT services, and personal care services (Mann, 2014). A child with ASD may receive the following specific services within these broader service categories: applied behavioral therapy (ABA), family psychotherapy, gait training therapy, range of motion measurements, pure tone audiometry, Childhood Autism Rating Scale (CARS), and personal care services.
If this child with ASD lived in Vermont, the following services would be eligible for Medicaid reimbursement if delivered in schools: gait training therapy, range of motion measurements, pure tone audiometry, and personal care services. All eligible services would be billed using a bundled payment code, and the state would be reimbursed for the number of services delivered to that child per month at the same rate per service. In Vermont, in-school ABA, family psychotherapy, and CARS are not eligible to be billed to Medicaid. In contrast, if the child lived in Rhode Island, the following services would be eligible for Medicaid reimbursement if delivered in schools: gait training therapy (billed as individual physical therapeutic exercises), range of motion measurements (billed as OT evaluation), speech threshold audiometry (billed as individual speech, hearing, or language program), and personal care services (billed as personal care). In-school ABA, family psychotherapy, and CARS would not be eligible for reimbursement from Medicaid. Finally, if the child lived in Indiana, the following services would be eligible for Medicaid reimbursement if delivered in schools: family psychotherapy (billed as family psychotherapy, with patient), gait training therapy (billed as therapeutic procedure; gait training), range of motion measurements (billed as OT evaluation), pure tone audiometry (billed as pure tone audiometry threshold), and CARS (billed as neurobehavioral status exam). In-school ABA would not be available for reimbursement from Medicaid.
Notably, ABA is not eligible for billing in any of these states. In fact, only Florida and Indiana cover any ABA billing codes. However, there are a few states whose Medicaid programs cover ABA, but do not have ABA-specific billing codes, such as Colorado. As a result, schools in states such as Colorado may bill Medicaid for ABA delivered in schools using a generic code for behavioral health counseling (e.g., H0004), but it is not possible to determine based on the code what service is being rendered.
Another scenario for consideration might involve an adolescent with depression who is receiving special education services. Depression is a disorder that can result in adverse psychosocial and educational outcomes, as well as increased the risk of suicide (Fergusson & Woodward, 2002). Children with mental health needs, such as depression, are most likely to receive treatment services in schools, (Fergusson & Woodward, 2002; Leaf et al., 1996) but there is substantial variation across states in the types of mental health services covered by Medicaid special education programs. According to evidence-based guidelines, management of adolescent depression should involve identification, diagnosis, and treatment. Identification includes depression screening, and diagnosis requires psychological evaluation of the patient and interviews with families. Treatment should include counseling for the family, evidence-based treatments for the individual such as cognitive behavioral therapy, group therapy, or antidepressant medication, and case management (Cheung et al., 2007; Zuckerbrot, Cheung, Jensen, Stein, & Laraque, 2007).
If a child with depression served in special education lived in Utah, the following services delivered in schools would be eligible for reimbursement by Medicaid: psychological evaluation and assessment, individual counseling, and medication administration. All services except for medication administration would be billed using a bundled service code, and medication administration would be billed as an itinerant nursing service. Family counseling, group therapy, and case management would not be eligible for reimbursement. If the child lived in Arkansas, the following services would be eligible for reimbursement by Medicaid: depression screening (billed as comprehensive preventive medicine evaluation and management), psychological evaluation (billed as psychological testing or psychiatric diagnostic interview), family therapy (billed as family psychotherapy with patient), cognitive behavioral therapy (billed as behavioral health counseling), group therapy (billed as group psychotherapy), and case management (billed as targeted case management). Medication administration would not be eligible for reimbursement. In contrast, if the child lived in Nebraska, none of these in-school services would be eligible for reimbursement by Medicaid.
Discussion
Our results suggest considerable variation in Medicaid special education programs for children with disabilities across states. The three most commonly covered service categories were speech–language/audiology, OT/PT, and behavioral health. Within these categories, the number of services covered and the types of services varied dramatically.
Notably, only a small number of states cover speech–language/audiology, OT/PT, or behavioral health screening services, which typically lead to further evaluation and subsequent treatment. The lack of coverage of behavioral health screening services is particularly noteworthy given that the U.S. Preventive Services Task Force (USPSTF), which publishes guidelines based on robust bodies of research evidence, currently recommends screening for depression in adolescents aged 12 to 18 years given the seriousness of this disorder and effectiveness of depression treatment in this age group (USPSTF, 2009). Previous research suggests that screening for depression in this age group can “help ensure accurate diagnosis, psychotherapy . . . and follow-up,” which can be effective in improving attendance, academic performance, and health outcomes (Cheung et al., 2007; USPSTF, 2009). School-based Medicaid programs can promote depression screening in one of two ways- by covering in-school behavioral health screening or in-school EPSDT services, which requires routine screening for emotional and behavioral problems. Currently, only 12 states cover behavioral health screening and five states cover school-based EPSDT services. Medicaid coverage of school-based behavioral screening services or EPSDT services for adolescents served under IDEA would likely increase the delivery of these services and improve outcomes for students in need of further evaluation and treatment.
These results also suggest that within behavioral health, only a minority of states are covering family services, such as family psychotherapy with or without the patient. Prior studies have found that family involvement in youth mental health services in general can be effective and improve outcomes for school-aged youth (Carr, 2014; Hoagwood et al., 2010). Furthermore, families play a crucial role in planning and participating in school-specific mental health services to ensure emotional, behavioral, and school functioning (Epstein, 2001). There is significant room for improvement in the involvement of families in the school mental health treatment process, particularly for children in special education (Stephan, Weist, Kataoka, Adelsheim, & Mills, 2007). Medicaid coverage of family services provided in an IEP is an important first step toward promoting family integration and participation in school-based behavioral health services.
Almost all states and Washington, D.C. reimburse school-based health services using a fee-for-service payment model, regardless of whether the child receives services through a managed care plan. These results underscore the reliance of states and school districts on carving out Medicaid school-based special education programs and relying on a fee-for-service reimbursement methodology. This is occurring even as Medicaid beneficiaries are increasingly enrolled in managed care plans that typically do not reimburse providers using fee-for-service payments (Gifford, Smith, Snipes, & Paradise, 2011). Although the implications of using a fee-for-service payment model have not been explicitly tested in school settings, prior research in medical settings suggests that this type of reimbursement often results in higher health care utilization and costs and does not appropriately emphasize the need to coordinate care across providers and service sectors (Miller & Luft, 1994; Newhouse, Schwartz, Williams, & Witsberger, 1985). This could be particularly problematic for children with disabilities who receive health care from multiple providers in a variety of service settings (Newacheck, Inkelas, & Kim, 2004). Additional research is necessary to understand the relationship between payment methodologies and service utilization or quality of care in schools.
The variation found in the number of covered services may have important implications for the amount of reimbursement a school district receives. However, as illustrated by the examples of a child with ASD and an adolescent with depression, the type of CPT code covered by the state Medicaid program could be more important in determining a child’s access to certain types of services than the number of codes covered. Although some states such as Indiana cover a large number of service codes indicating specific services, others states such as Rhode Island use fewer service codes that represent broader service categories. No prior studies have investigated the impact of the number of services covered and the types of billing codes covered on delivery and reimbursement of services for school districts. Future research should investigate these relationships.
Policy Implications
As the Medicaid managed care penetration rate continues to increase, it is increasingly important to understand the implications of carving out Medicaid special education programs and using a fee-for-service payment methodology. If fee-for-service payment models have similar implications in schools as they do in medical settings, it may be necessary to integrate providers into managed care plans or use a different reimbursement methodology. However, several studies investigating payment methodologies used by managed care organizations have demonstrated that certain methodologies such as capitation can result in stinting of services (Frakt & Mayes, 2012; Gosden et al., 2000). The payment methodology used for in-school health providers should promote adequate and appropriate delivery of services, so it will be necessary to closely evaluate the effects of any changes to Medicaid special education programs.
Practice Implications
Special education administrators are tasked with carrying out complex, demanding programs for children with disabilities in an unstable funding environment. Medicaid can be an important financial resource for schools, but it adds an administrative burden to both providers and administrators that must be considered in program planning. For schools to appropriately capitalize on Medicaid special education programs, they have to be tailored to a system dedicated to educating students, as opposed to one built to deliver health services. Although the results of the study do not suggest which program characteristics work best in a school setting, future research should investigate which models reduce the administrative burden while maintaining program integrity.
Limitations
This study has several limitations. First, state Medicaid programs often cover additional services that are not covered by school-based Medicaid programs, such as medication management services. It is possible that states are reimbursed for services delivered in schools that are not explicitly specified in school-based programs but are covered under general state programs. Although these data do not include information about general Medicaid-covered services, we expect that the majority of services reimbursed by Medicaid for children in special education are those specified in school Medicaid fee schedules and provider manuals. Furthermore, states are likely providing additional health services to children served in special education, including those who are enrolled in Medicaid, that are not being billed to Medicaid.
Second, even though CPT codes are the most useful tool to characterize which services a state Medicaid program covers, there may be variation across states in which services are actually delivered when a specific CPT code is used for billing. For example, CPT code 90804 is defined as individual psychotherapy. Some states use this code when a provider performs cognitive behavioral therapy, a common treatment for a variety of mental illnesses. However, it is not possible to tell which specific services are being delivered based solely on the CPT code.
Another important limitation is the lack of publicly available provider manuals or fee schedules for Medicaid special education programs in all states. This required contacting key informants to obtain appropriate documentation. These informants were identified based on publicly available websites, and were not cross-checked with another reference.
Finally, this study did not assess if providers manuals were used with fidelity in the states. It is possible that providers are using different billing codes or payment methodologies that are no specified in the provider manuals.
Conclusion
Medicaid plays a key role in filling the gap in IDEA Part B funding to supplement the cost of providing medically necessary health services for children with disabilities. There is significant variation across states in Medicaid special education programs for children with disabilities, which has important implications for the delivery of services to students with disabilities. Although the number and types of services covered by Medicaid is highly variable, almost all states are reimbursed based on a fee-for-service payment methodology, which, in traditional medical settings, often leads to the delivery of a higher volume of services and deemphasizes care coordination. Including in-school providers in managed care organizations may be one way to emphasize quality of care and coordination of care across service settings, but any changes to Medicaid programs must be closely monitored.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.