
Abstract
Mental health is quickly becoming a major topic of concern in education, particularly as it relates to the provision of services for students with emotional and behavioral disorders. In this study, state policies related to the provision of mental health services were reviewed, with specific attention paid to the capacity of services and relationships between state policies and the educational environment. Open coding was used to determine the variables and services provided within each state’s policies. Axial coding was used to determine relationships between codes and ensure alignment and accuracy of findings. Interrater reliability, using a 7-point rubric, was conducted to ensure accuracy of coding. Findings indicate that the majority of states have policies related to the provision of mental health services, but the structure and implementation of these services differ vastly by state. Similarities were found in the provision of mental health services within the educational environment, which typically occurred as a collaboration between schools and community agency partnerships. Implications for practice and the preparation of educational professionals will be discussed.
Keywords
Child and adolescent psychological health is a major topic of concern in the field of education as the number of students experiencing mental health issues becomes more prevalent (Centers for Disease Control and Prevention, 2013). Current research indicates that approximately 12% of school-aged children experience these issues (Forness, Freeman, Paparella, Kauffman, & Walker, 2012; Merikangas et al., 2010). Youth mental health is also at the forefront of many educational policies, such as the President’s New Freedom Commission on Mental Health (2003) which proposed an alignment of the provision of mental health services within the school context (Atkins, Hoagwood, Kutash, & Seidman, 2010). This is particularly important as schools struggle to provide adequate services for students with emotional and behavioral disorders (EBD; Kern, 2015).
Students with EBD typically are identified for special education services due to social and behavioral difficulties (Kauffman & Landrum, 2013; Kavale, Forness, & Mostert, 2005; Marsh, 2016). Disorders that fall under the EBD category comprise externalizing and internalizing forms of EBD including oppositional defiant disorder (ODD), conduct disorder (CD), depression, anxiety, and schizophrenia, all of which are mental health disorders that can affect a student’s functioning in school (Forness et al., 2012). Unfortunately, very little is known about the connection between the provision of mental health services in schools, particularly in the implementation of Individualized Education Programs (IEP) for students with EBD (Santiago, Kataoka, Forness, & Miranda, 2014). With child and adolescent mental health prevalence rates following a similar trend to adult rates, an argument can be made that school-based early intervention and provision of services for students with EBD at a younger age may mitigate mental health issues in adulthood (Atkins et al., 2010; Merikangas et al., 2010).
In addition to students with EBD, approximately 5% of children and youth experience serious difficulties in concentration, behavior, and peer interactions within the school environment that may require mental health services (Pastor, Reuben, & Duran, 2012). Students experiencing academic problems because of mental health issues who do not receive services are at a higher risk of dropping out of or being expelled from school (Edmonds-Cady & Hock, 2008; Lehr, Johnson, Bremer, Cosio, & Thompson, 2004). Estimations are that those who receive services early for these issues have the lowest rates of problematic outcomes and the highest levels of positive school-related outcomes (i.e., better connections to school, better decision-making, lower rates of suicide attempts; Fleming et al., 2005; Greenberg et al., 2003; Lester, Water, & Cross, 2013; McGorry & Purcell, 2009; Zenere & Lazarus, 1997). It appears that early access to mental health services whether from schools, after school programs, or through direct service providers builds resiliency in children and adolescents (Nelson, Leone, & Rutherford, 2004).
Current research focusing on service access for children and youth with mental health issues shows that the percentage of those identified and receiving services is lower than those not receiving services (Mental Health America 2015; Merikangas et al., 2011). Merikangas et al. (2011) found that 36.2% of children and adolescents with mental health issues actually received treatment for their condition, with the greater number of students receiving services related to externalized behavior problems (Pastor et al., 2012). This is consistent with current findings that indicate students who exhibit more externalized forms of EBD are often more likely to be identified for special education services (Marsh, 2016). Unfortunately, many students with internalizing EBD are not identified for services, and those who are identified do not receive the necessary accommodations and modifications to address their mental health needs (Forness et al., 2012; Mental Health America 2015). This lack of services may be related to school staff who lack the training to correctly identify students with internalizing forms of EBD (Essex et al., 2009; Forness, 2005; Lane, 2007; Marsh, 2016).
In addition to the low rate of mental health service access, there are differing rates of service usage by sector. Of children and youth receiving mental health services, 46.5% access services through a mental health professional and 35.4% receive services in the school setting (Merikangas et al., 2011). Pastor et al. (2012) reported similar rates of service access by children and adolescents from mental health professionals and in the school setting. These rates are lower than indicated by previous research findings that suggest more than 75% of children received services in the school setting (Burns, Costello, Angold, & Tweed, 1995). The disparity in percentages of service access in the school environment may be due to a larger nationally representative sample population than previous studies, where participants were from a single state (Burns et al., 1995; Merikangas et al., 2011).
Many school districts have not adopted overall policies to address the mental health of students. Currently, more than 75% of schools employ at least one individual capable of addressing student mental health needs (Brener, Weist, Adelman, Taylor, & Vernon-Smiley, 2007). This individual typically is a school counselor, school psychologist, or school-based social worker. Many schools have adopted the use of school-wide positive behavior supports, which may address many mental health needs of students on a single campus (Cook et al., 2015), although these supports often do not address the individualized and intensive mental health needs of students identified as having mental health issues, particularly those with EBD. Also, the services provided by specialized individuals and quality of the implementation of programs by schools differ state-to-state and district-to-district (Adelman & Taylor, 2000; Brener et al., 2007; Cook et al., 2015). As it appears that the majority of schools struggle to provide adequate mental health services on campus due to lack of awareness of state policies or lack of training regarding identification of possible mental health issues, it is important for educational professionals to be aware of state and local policies related to the provision of these services (Atkins et al., 2010; Forness et al., 2012; Marsh, 2016; Santiago et al., 2014).
Research Questions
To this end, the purpose of this study was to (a) review state policies related to the provision of mental health services to children/adolescents with mental health issues, (b) determine the capacity and location of mental health services provided by the state, and (c) identify relationships between state policies related to the provision of mental health services and the educational environment (e.g., provision of services at schools, provision of services through community-school partnerships, access of mental health services). Two specific research questions were addressed within this study:
Method
To determine the extent to which states have policies in place to address the mental health needs of school-aged students, members of the research team located, collected, and reviewed state policy documents relative to the provision of mental health services. Once documents for each state were located, members of the research team analyzed these policy documents using a coding procedure adapted from the work of Freeman and Sugai (2013). This coding procedure determined (a) the agency responsible for the provision of services, (b) the location of mental health services for the student, and (c) the capacity of services provided under the policy.
Sample and Search Procedures
Members of the research team began to search for state policy information related to the provision of mental health services to school-aged students, particularly those identified as having EBD. For the purpose of this study, a “state mental health policy” was defined as the assessment and provision of mental health services through a state-sponsored agency (e.g., Department of Health and Human Services, Department of Education). The search parameters used in an Internet-based search engine included “mental health services for students with disabilities in insert state” and “mental health children in insert state.” The websites of each state’s Departments of Education and Health and Human Services (or the state’s respective department that addressed similar policies) were searched directly for these terms. Based on this search, mental health policies were located from 50 of the 50 states and the District of Columbia. Following the initial search, the state policies were divided into three groups, and the research team completed an independent search to ensure the accuracy of the policies identified (see Figure 1 for the conceptual framework of research activities). Policies were not analyzed for content at this time. The goal was to ensure fidelity of policy identification from the initial search. This resulted in 100% agreement among the team.
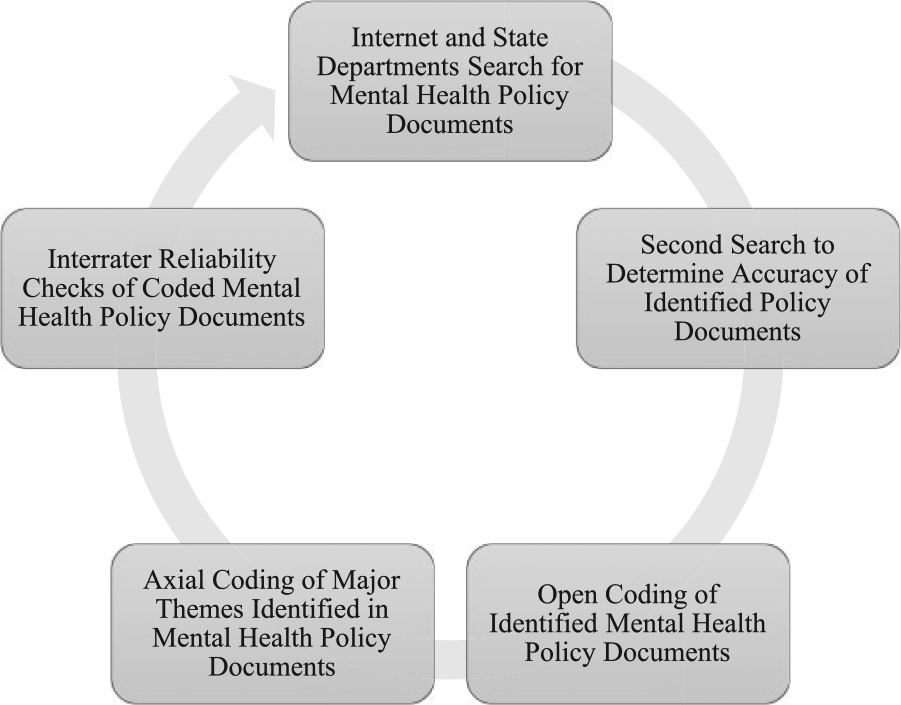
Conceptual framework of major study activities to ensure accuracy of findings from state mental health policy documents.
Coding
Coding of the policy documents involved determining (a) the agency in the state responsible for ensuring the provision of mental health services to students, (b) the location of the provision of services (i.e., community, school, clinic), and (c) the capacity of services provided (i.e., therapy, medication). An open coding procedure was used initially to determine the different variables and services provided within each of these policies. Once open codes were determined, axial coding occurred to determine the relationships between codes and ensure alignment and accuracy of findings. These axial codes were entered per state into a shared, master Excel spreadsheet.
Interrater Reliability Scoring of Identified State Mental Health Policies
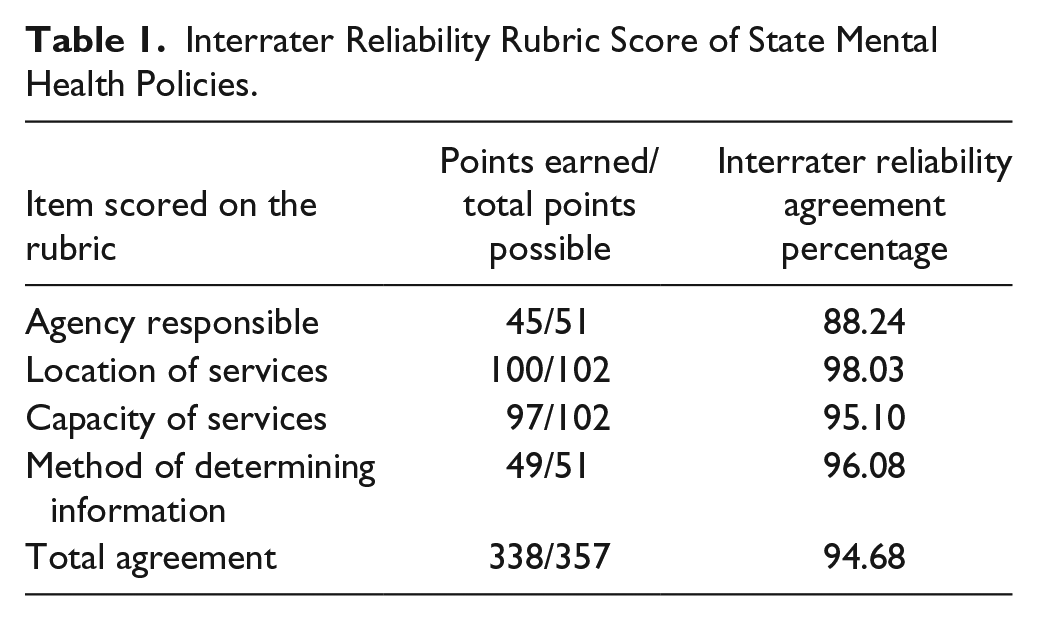
Following the initial coding, the two members of the research team who conducted the initial coding alternated states and completed validity checks using an agreement rubric (i.e., the person who scored the first 25 states during initial coding then scored the second 25 states during interrater reliability coding). Interrater reliability scoring was completed using a 7-point rubric that focused on (a) agreement on agency responsible (1 = agree, 0 = disagree), (b) location of services (2 = agree with complete list, 1 = agree with partial list, 0 = disagree with list), (c) capacity of services (2 = agree with complete list, 1 = agree with partial list, 0 = disagree with list), and (d) method of determining information (1 = agree, 0 = disagree). The interrater agreement threshold set was 80% or higher on each item on the rubric, as well as on the rubric overall. Any items below 80% were targeted for follow-up analysis to determine if agreement could be reached. There were four states that had agreement below 80%. The policies for these states were re-analyzed by a member of the research team who had not participated in the policy identification or coding to determine the accuracy of the information, and the interrater scoring rubric was updated. Following this secondary analysis, each component of the rubric reached 80% or higher agreement. Overall, there was approximately 95% agreement on the overall rubric score (see Table 1 for interrater reliability scoring for each item on the rubric).
Interrater Reliability Rubric Score of State Mental Health Policies.
Results
Results for each focus area (e.g., responsible agency, location of services, capacity of services) are presented below. Each state’s educational and mental health policies were coded to determine the specific requirements for the provision of mental health to students with mental health issues and identified as having EBD. These codes were then counted to determine the frequency of specific service structures and to identify any themes that existed across state mental health policies (Freeman & Sugai, 2013).
Agency Responsible for Provision of Mental Health Services
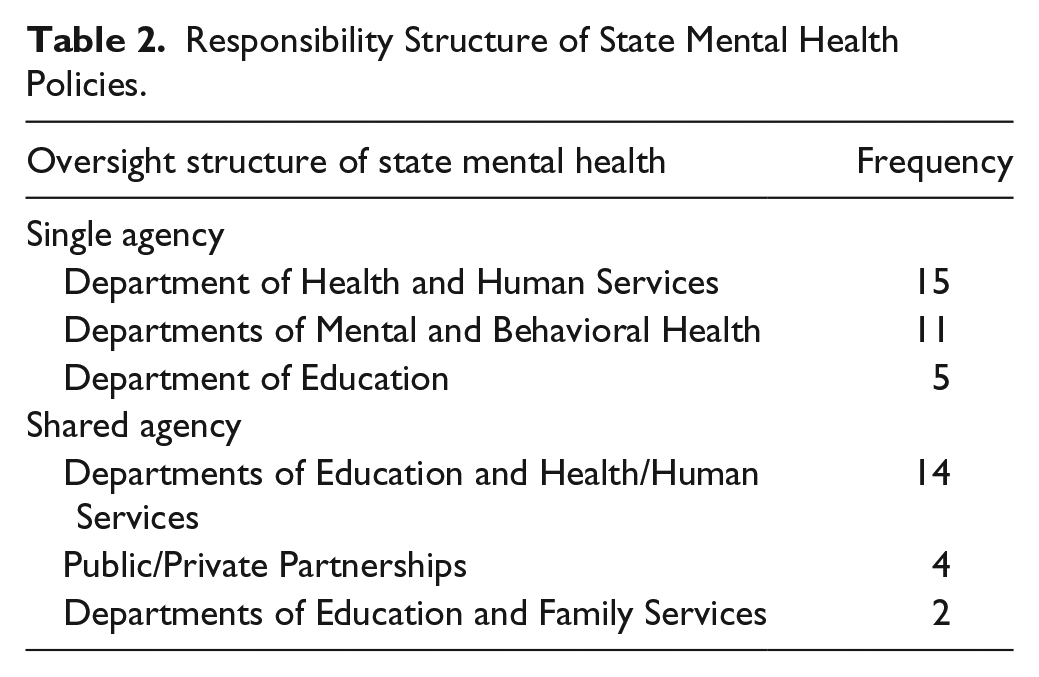
The agency responsible for the provision of mental health services at the state level was defined as the specific unit or entity within state governmental structures that had oversight of the implementation and provision of mental health policies to students in public schools. Of the 51 states and the District of Columbia, 31 of the states (61%) had a single state agency responsible for these policies (e.g., Departments of Education, Departments of Health and Human Services). A state was deemed as having a single agency responsible if there was no explicit mention of agency collaboration regarding the provision of mental health services on the primary agencies’ website. In these states, the vast majority of agencies responsible were either Departments of Health and Human Services (48% of agencies responsible) or Departments or Agencies of Mental and Behavioral Health (35% of agencies responsible).
In 20 of the states (39%), there was a shared and collaborative oversight process for these policies (i.e., Department of Education and the Department of Health and Human Services, public–private partnerships). The most common structure of these collaborations across states was a partnership between the Department of Health and Human Services and the Department of Education or Office of Public Instruction. These partnerships represented 70% of the collaborations found throughout state mental health policies. See Table 2 for a summary of the different oversight structures found throughout the state policies, including specific examples of the different agencies involved in the implementation of state mental health policies.
Responsibility Structure of State Mental Health Policies.
Location of Mental Health Services
Within state mental health policies, required services were provided at a variety of different locations in and around the school community. Three main categories were identified within these state mental health policies relative to the location of services: (a) school-based services, (b) community-based services, and (c) services provided in the clinical setting. Some state policies allotted for the provision of services in multiple settings. See Table 3 for an analysis of the location of provided services identified in state policies.
Location of the Provision of Services Within State Policies.
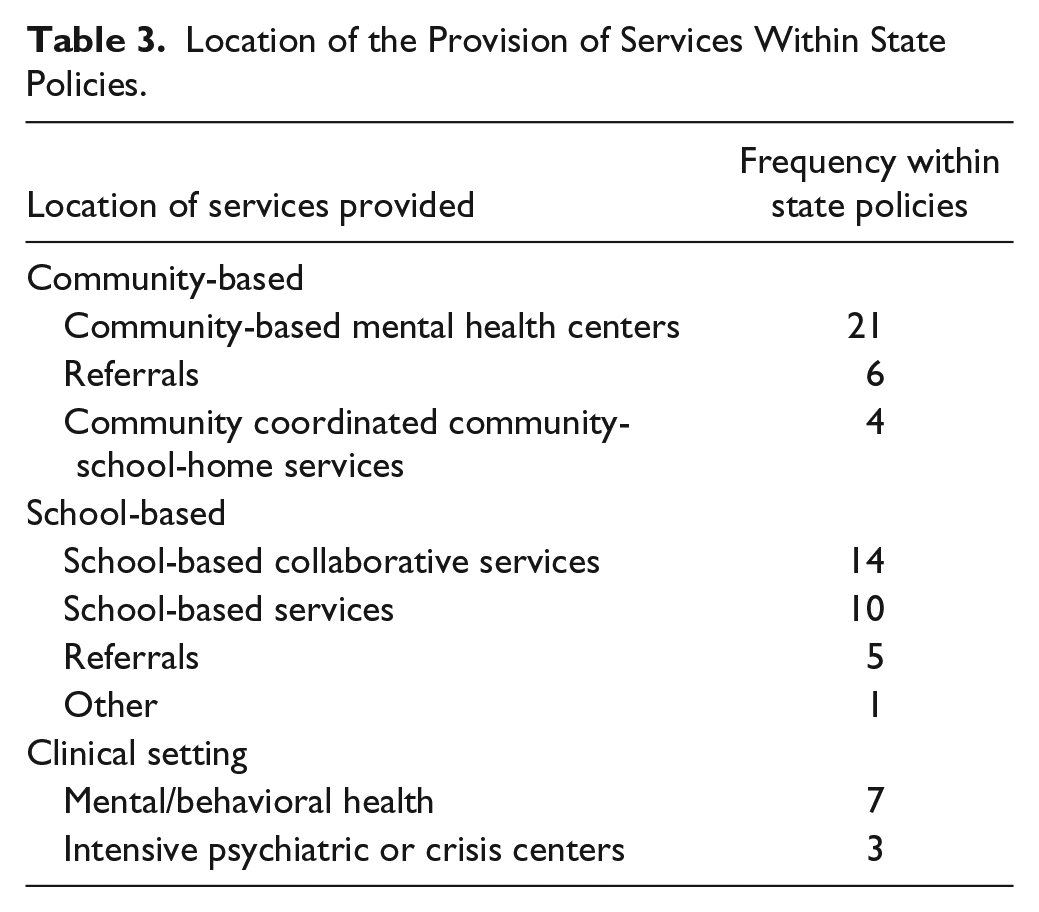
Within state policies, the most common location of services was within the community (31 states, 62% of the state policies reviewed). The specific locations within the community varied slightly, but the majority of community-based services were required to be provided within community-based health centers (68% of community-based services). Students identified as having a mental health concern would be referred to a community-based health center outside of the school environment under the majority of these state policies. States also had provisions for the referral of students to local agencies for assessment or support, or for coordinated efforts between key stakeholders.
It also was common for services to be provided within the school setting (30 states, 60% of the state policies reviewed). Fourteen of the 30 school-based service provision structures included collaborations with community-based mental health service providers (47%). Although similar in nature to the community-based services, these collaborations partnered directly with schools to ensure adequate access to mental health services for students identified as having a need. These services were not referrals to community-based organizations or mental health providers. Examples of these collaborations included school district contracts with private non-profit organizations to provide mental health services and supports on the school campus, and school coordination and follow-up of the provision of services to students identified as having mental health issues. While the actual services may have been provided through a different agency or setting, the school was primarily responsible for ensuring that these services were accessible to students and families.
In addition to these school-based collaborations, 10 state policies placed the responsibility of the provision of mental health services on school personnel (30% of state policies reviewed). School counselors, school psychologists, or social workers were expected to deliver mental health services to students identified with needs under these models. All services were required to be delivered by school personnel. The majority of services in this model were designed to be prevention-focused, with some level of secondary intervention for students identified as at risk (e.g., screening for mental health services, short-term counseling for students having some level of mental health need). School personnel were required to coordinate with outside agencies if the needs of the student were beyond the scope of services that could be provided within the school setting.
The final structure implemented across states for the provision of mental health services to students was within clinical settings. Ten of the states (20%) had systems in place through which mental health services were provided to children/youth through clinical settings. These included inpatient and outpatient services for students identified as having mental health issues, referrals to intensive treatment in clinical settings, or referrals to crisis clinics or mental health centers. Generally, these services were provided in addition to community and school-based services and were a tertiary intervention for students who may not be responding to the services provided more locally.
Capacity of Services Provided Through State Mental Health Policies
Another unit of analysis for state mental health policies was the capacity and types of services provided through each state. Within the state mental health policies, there were four primary categories of services provided to children/youth identified as having mental health issues: (a) assessment, (b) therapy, (c) community/hospital programs, and (d) medication. Each of these categories is described below. Table 4 describes the frequency counts of the capacity of services across mental health policies and states.
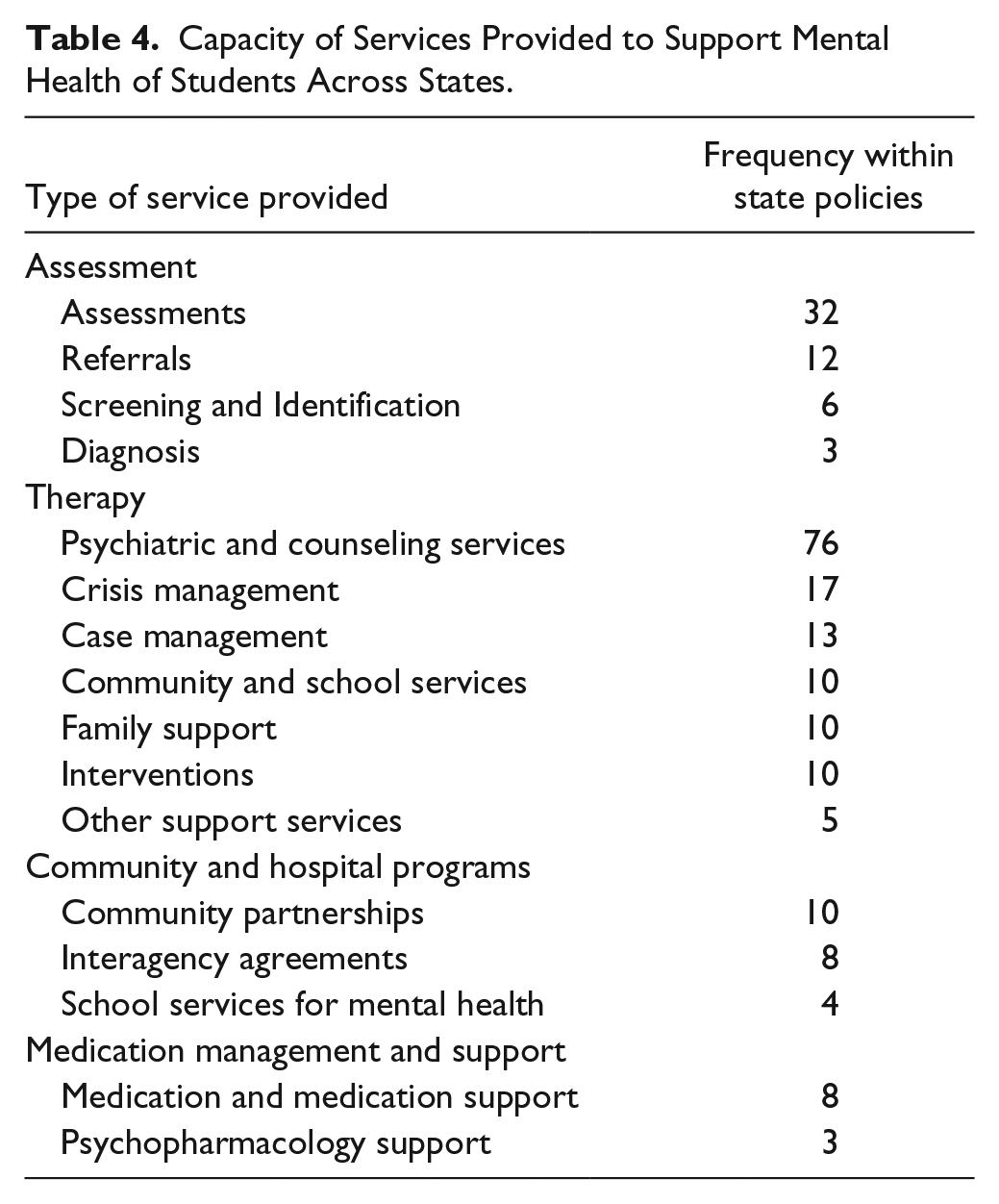
Capacity of Services Provided to Support Mental Health of Students Across States.
Assessment
Across all state mental health policies, there were 53 specific mentions of the provision of assessments to students with mental health issues. The majority of these references within the policies were related to assessment and diagnosis of possible mental health issues (35 of 53, or 66% of references). Within the policies, assessments were provided when a student was considered at risk or if a mental health concern was reported. Several of the assessment policies were related to the screening of students across the school population, although these references were limited (six of 53, or 11% of references). This indicates that the majority of diagnostic assessment was focused on assessment after a referral was made, but not necessarily on screening students for mental health issues as a proactive measure of assessment (see Table 4).
Therapy
The most frequently provided service through state mental health policies was the provision of therapy and therapeutic services to students identified as having mental health issues. Therapy and therapeutic services were cited a total of 141 times in the state mental health policies reviewed. The majority of states required the provision of multiple types of therapy to students needing mental health supports. Most frequently, state policies required psychiatric and counseling services (76 of 141, or 54% of references). These services were varied in nature, including the provision of counseling and support groups, inpatient and residential services, and day treatment services. In addition to the provision of psychiatric and counseling services, state policies provided supports for crisis management (17 of 141, or 12% of references). The policies also provided for the implementation of various supports for students in the home and school setting (28 of 141, or 20% of references). Overall, the state policies tried to account for a variety of different services and needs that students with mental health issues might experience. There was a clear indication that the majority of resources allocated through the policies were focused on therapy and therapeutic services.
Community and hospital programs
With less frequency, state mental health policies provided for the provision of community and hospital program services. Twenty-two references to community and hospital programming were made within the state policies. The majority were focused on developing coordinated service efforts between schools and communities. They discussed bringing community resources to schools and allowing for the provision of wraparound and case management services for students identified as having mental health issues in the school community. These services appeared to be designed to provide holistic services for the needs of children/youth within the public school environment. Some of the services were focused on providing support in classrooms to ensure structure and environmental consistency for students identified as having mental health issues.
Medication
Finally, state policies made mention of the provision of medication and medical services to support students identified as having mental health issues. This was the least frequently cited service provided within the policies, with only 11 references to medication and medication management. However, several states recognized the need for support of students with mental health issues who received medication support and made special note of the provision of these services throughout their policy (see Table 4).
Discussion
The purpose of this study was to review state policies relevant to the provision of mental health services to students with suspected or diagnosed mental health issues, particularly those with EBD. This analysis was conducted to determine the types and location of services provided by states to students experiencing mental health issues. This study also explored the implications of the provision of these services within the educational environment. Contrary to the findings of Brener et al. (2007), the present study found that every state has some type of state policy that requires the provision of mental health services and supports for students with mental health issues. Although states vary in the structure of these supports and services, every state has some system in place to address the increasing mental health needs of children/youth enrolled in public school environments.
The majority of the state policies reviewed identified a single agency as being responsible for the provision of mental health services to students within the state, and a majority of these agencies were focused on health and human services. This is important for educational environments, as schools and districts may not always be aware of the services being provided to eligible students if the policy is far removed from the school location. A growing number of states, however, have assigned shared responsibility to multiple agencies within the state. In alignment with the President’s New Freedom Commission on Mental Health (2003), the majority of these shared responsibility states mandate that Departments of Education and Health and Human Services coordinate efforts in the provision of mental health supports for students with EBD or those with mental health issues. These shared responsibility policies are important as professionals in educational environments are often the first to identify that there may be an issue related to student mental health (Marsh, 2016).
It was common throughout all of the state policies that the majority of services being provided to children/youth with EBD or those with mental health issues were provided either at community-based mental health centers or through school-based collaborative services (45 instances of these combined services). Although some states provided services to students directly on the school campus, the majority of policies allocated resources for community-based services. Whereas a large number of states provided for community-based services, fewer mandated a coordinated effort between the community and school or school districts. It appears that community agencies were eligible to accept referrals from schools and school districts, but no indication was found that follow-up coordination of responsibility on either entities’ part was required. Determination of follow-up services and impact of referrals are important to ascertain if students received the supports they needed to address their mental health issues. Coordinated efforts with a single case manager responsible for ensuring access to services have the biggest impact on the mental health of participants (Committee on School Health, 2004). Therefore, systems with coordinated efforts should ensure that there is a single point of management to ensure that the child/youth is accessing required services.
Finally, the majority of state policies provided therapeutic supports for students with EBD or those with mental health issues. This is a positive finding in that students who receive support for mental health issues are less likely to suffer from deleterious effects on their academic outcomes (Fleming et al., 2005; Greenberg et al., 2003; Lester et al., 2013; McGorry & Purcell, 2009; Zenere & Lazarus, 1997). However, Merikangas et al. (2011) and Pastor et al. (2012) reported that the majority of students who reported mental health issues while enrolled in public school environments did not have access to psychological and therapeutic services.
Two important components of the provision of mental health services to students with EBD or those having mental health issues were deemed underrepresented based on the comparison of state policies and the reported access to services. First, the majority of states did not mandate screening, assessment, and diagnostic systems within schools to provide early identification of students with mental health issues. Without this screening and diagnostic procedures, students with mental health issues may not be referred for services (Lane, 2007). This may result in the discrepancy between the provision of services and student-reported access to the services. Second, states may provide services throughout the community and the referral process from schools to services may not be designed to ensure that students have access to the needed services. Therefore, continuity of care may not be closely monitored within school environments and this may lead to ineffective provision of services. Additional research should focus on procedures occurring on school campuses to support the referral to and receipt of mental health services for students with EBD or those mental health issues at school or in the community.
Limitations
The findings and summaries related to this study should be viewed through the context of a few limitations. The data for this study were collected through a systematic review of state websites and policy documents related to the provision of mental health services to children/youth. Because of this data source, there may be additional policies and procedures related to state provision of mental health services to students that were not readily available on the websites. While several steps were taken to guard against this (e.g., completing multiple reviews of state policies to ensure the most current information, calling state departments when there was confusion about a policy), policies may exist in other sources that were not available publicly.
States may have adopted new policies related to the provision of mental health services over the course of the study. At least three checks were completed on state policy websites to ensure relevance and accuracy of information, but it is possible that changes to policy were enacted but not posted to the website. This emphasizes the importance for stakeholders interested in the mental health of children/youth to review current policies and practices in their state frequently.
This systematic policy review was limited to state departments and did not consider additional policies to support the mental health of students at the district or individual school level. Comprehensive policies and procedures may exist at a level closer to the child, but this analysis was beyond the scope of the present study. Future inquiry should focus on determining how districts and schools address the mental health needs of students enrolled in their district. Related to this point, the present study did not review the implementation of the state policies. The websites revealed little information concerning the implementation of the policies within school or local communities.
Finally, a qualitative coding procedure was used to determine common themes across state mental health policies. A codebook was developed by members of the research team to ensure consistency of coding across state mental health policies. However, it is possible that a specific component of the policy was coded in one manner, whereas the intent of the policy was something different. Triangulation of these data was beyond the scope of the present study. Future research should focus on drilling down into state policies and having conversations with state leaders on the implementation of the identified policies within the school community.
Recommendations
Although this exploratory study has limitations, it underscores the efforts in play across the nation to address the mental health needs of students on public school campuses. It is likely that local educational agencies are providing additional services to students beyond the scope of state policies, involving stakeholders who are in place to address mental health needs as they arise on school campuses. However, even with the increased recognition of the need for mental health supports throughout state policies, there exists a large variation in how states address these issues on school campuses. The results of this study indicate that states have policies to assist students and families in accessing mental health services; however, these policies outline different agencies responsible for providing services, differing locations of those services, and differing capacity of services that are available (Atkins et al., 2010; Forness et al., 2012; Merikangas et al., 2011; Pastor et al., 2012). Therefore, several recommendations can be made for schools and school districts to ensure that students receive necessary supports.
Comprehensive Screening and Assessment Procedures
The number of students with mental health issues is increasing on U.S. public school campuses, yet the number of children/youth reporting an inability to access and receive services also is increasing. Therefore, it is important for states, districts, and schools to consistently implement comprehensive screening and assessment procedures to identify students who have, or are at risk for, mental health issues (Essex et al., 2009; Lane, 2007). While many states have systems in place for screening of possible mental health issues, it is important that mental health service providers become more involved with districts and schools. Mental health service providers could provide additional training for school personnel regarding screening and available services as well as help to ensure that students with mental health issues are able to access services from a community agency or within the school. Screening and assessment can help ensure that students with mental health needs have appropriate access to provided services.
Capacity Development of Educational Professionals Relative to Mental Health Services
Because many state policies focused on the provision of mental health services exist in sectors that may not have a direct connection to the educational environment, it is imperative for all individuals working with students with EBD and those with mental health issues, on a school campus, to be aware of available service options. Educational professionals are often the first line of identification of students with mental health issues (Marsh, 2016). It is important for these stakeholders to know the policies and procedures for referring a student who may be exhibiting mental health problems and for ensuring that the student and their family are readily aware of the services available for supporting their needs. While all educational professionals may not be trained to provide supports relative to mental health (nor should they be), it is important that they be educated on the policies, procedures, and systems that exist within their state to ensure the provision of appropriate services to children/youth. Professional developments and resource guides are important steps in increasing the access that families with children experiencing mental health issues, particularly those with EBD, have to community-based services.
Teacher preparation programs also should include policies and procedures regarding the provision of mental health services in their course programming (Marsh, 2016). These programs would help to ensure that incoming professional educators of students with EBD are well versed in their state’s mental health policies and are knowledgeable of service options. By incorporating information regarding state mental health policies, teacher preparation programs can develop teachers who are prepared to assist families in the process for accessing mental health services which could result in increased access of services by students with EBD.
Develop Coordinated Collaborative Support Networks
As many state policies focus on the provision of services within the community or through integrated systems, schools and school districts must actively work to develop coordinated, collaborative support networks. Awareness of the services provided within the community as well as referral follow-up will contribute to student access to appropriate supports and services. In this coordinated collaborative network, it is important for schools and school districts to name a case manager or someone responsible for coordinating these services. This person should be a member of the school team (i.e., administrator, counselor, school social worker, school psychologist) or may be an additional team member from a community service provider. Having a designated case manager can help ensure that educational professionals consistently are aware of services being provided and eliminate barriers to the child’s access to services. The results of this study suggest that mental health services may be available across the country; however, access to those services can be affected by issues related to location and socioeconomic status.
The mental health of students in the K–12 public education system throughout the United States is a topic of great importance, both for educational professionals and community leaders. Mental health is connected to a variety of life outcomes, including academic success, postsecondary education completion, and job security and satisfaction. Interventions and supports provided to students with mental health issues can help alleviate the impact of these problems and ensure that children/youth maintain high qualities of life. Because educational professionals interact with students in a variety of settings and populations, it is important for them to be aware of and understand state policies for supporting the mental health of students in public school environments. Schools can serve as a centralized hub of a coordinated, collaborative support system to identify the mental health needs of students and ensure that students and families have access to high quality mental health services.
Footnotes
Authors’ Note
Since the time this research was completed, Robbie J. Marsh has changed affiliations. He is now with Mercer University, Tift College of Education.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.