
Abstract
Deaf and hard-of-hearing (DHH) students have exhibited deficient language competencies and low academic achievement for over four decades. As a result, Individuals With Disabilities Education Act (IDEA) 2004 requires schools to address special language and communication factors through each student’s Individualized Education Program (IEP). States have responded in a variety of ways with several that supplement their IEPs using a communication plan. This article examined states’ IEP or communication plan templates to identify the format and specificity with which they addressed these requirements. The IDEA language was parsed into distinct items to allow ratings using a Likert-type scale. The analyses performed descriptive, t test, and ANOVA comparisons on the forms posted on states’ website. Those states using a communication plan had significantly higher ratings overall. Kentucky’s form was the most highly rated IEP and identified each required item. Most state IEP forms identified these factors more generally with a majority rated as only minimally specified. Use of a communication plan or IEP form that incorporates IDEA language similar was the most effective strategy. Overt specificity ensures that DHH students’ language and communication needs are being met in the educational environment and facilitates states’ oversight in meeting their educational responsibilities.
Introduction
For young children with hearing loss, parental worries may focus on their child’s inability to hear environmental sounds, especially warnings and alerts (King, 2017; Zaidman-Zait & Young, 2008). However, the most consequential and lifelong impact of hearing loss is from their child’s reduced access to language (Bowers & Schwarz, 2013; Kushalnagar et al., 2011). It is through listening and hearing that most children acquire the syntactic, semantic, and pragmatic skills that result in fluent interpersonal communication (Easterbrooks & Baker, 2002; King, 2017). For those with normal hearing, acquisition occurs naturally and without much effort from parents or family members: Typical communication and environmental interactions provide the stimuli that the infant brain needs to compile a complete system of language.
The infant brain is receptive and acts upon the stimuli it receives (Easterbrooks & Baker, 2002; Humphries et al., 2015). However, insufficient or indistinct linguistic signals result in an incomplete and/or incorrect set of language structures (Mayberry, Chen, Witcher, & Klein, 2011). Significant neurophysiological differentiation is completed very early with morphological, semantic system growth peaking during a child’s second and third year of life, after which it substantially slows (Lecours, 1975; Lenneberg, 1967; Penicaud et al., 2013). It is this time-limited developmental process that can have a devastating effect on a DHH (deaf and hard-of-hearing) child’s language and communication (Boudreault & Mayberry, 2006; Kuhl & Rivera-Gaxiola, 2008; Mayberry, 2007; Mayberry et al., 2011; Mayberry, Lock, & Kazmi, 2002; Paul & Whitelaw, 2011).
Most DHH infants are born to hearing parents (Gallaudet Research Institute, 2013) and as this research indicates, often struggle to perceive spoken communication with sufficient clarity to develop a complete language. And it is only during these very early years that the brain’s linguistic centers are most receptive to acquisition, after which point the brain transitions to other critical developmental tasks. The fundamentals of language are acquired principally within these first 3 years (U.S. Department of Health & Human Services, 2010) and, quite importantly, prior to beginning formal school-based services (Individuals With Disabilities Education Act [IDEA], 2004, Part B, Section 619). If DHH children arrive at school without full language fluency, they are unlikely to acquire it later. Even intensive instructional interventions cannot reopen the neurolinguistic centers, although nominal plasticity remains into adolescence (Boudreault & Mayberry, 2006; Mayberry, 2007; Mayberry et al., 2011; Mayberry et al., 2002).
Because children with milder hearing losses hear more of the language within their environments, it is logical that their linguistic abilities would be more comparable with their typical peers. Their hearing loss is measured uses a logarithmic scale with loudness designated as the decibel (dB). The American Speech-Language-Hearing Association (n.d.) identifies levels of loss. Those with losses in the mild through severe range typically are identified as “hard-of-hearing” and those with profound hearing losses as “deaf.” Functionally, the difference is that hard-of-hearing individuals can acquire some elements of language through their hearing, with hearing aids or assistive technologies. Those who are deaf typically cannot: They do not have sufficient residual hearing, even with a range of devices, to acquire spoken language.
However, despite their better hearing, research shows that young children with mild to moderate hearing losses demonstrate substantial and long-term deficits in language acquisition (Davis, Elfenbein, Schum, & Bentler, 1986; Gilbertson & Kamhi, 1995; Moeller, Osberger, & Eccarius, 1986; Nicholas & Geers, 2003). Across a range of language and academic assessments, these children have been shown to function more similarly to those with severe to profound losses than to their normal-hearing peers. In fact, several studies have found no relationship between levels of hearing loss and subsequent vocabulary skills (Blamey et al., 2001; Mayne, Yoshinaga-Itano, & Sedey, 1998; Mayne, Yoshinaga-Itano, Sedey, & Carey, 1998; Moeller, 2000). Calderon and Naidu (1998) found that level of hearing loss explained just 1% of the variance in language development beyond that explained by age of early intervention services. Various measures continue to show that most children with mild to moderate hearing losses do not perform like their typical peers, and do not perform significantly better than those with severe to profound losses (Friedmann & Szterman, 2005; Marschark & Knoors, 2012; Mayne, Yoshinaga-Itano, & Sedey, 1998; Moeller, 2000).
Studies of children using cochlear implants also have not shown outcomes concomitant with those of their normal-hearing peers (Blamey et al., 2001; Marschark, Rhoten, & Fabich, 2007). Blamey and Sarant (2002) found that implanted children performed instead more like those with a severe hearing loss. Barker et al. (2009) found that implanted children 1.5 to 5 years of age displayed significantly more language, attention, and behavioral difficulties compared with their normal-hearing peers. A review by Archbold and Mayer’s (2012) examined cochlear implant outcomes since 2000, and although several studies reported early gains, these were not maintained through older childhood and adolescence. Early childhood hearing loss, regardless of its severity and use of new technologies, compromises the innate, neurologically determined linguistic acquisition processes through a lack of full linguistic access.
The same neurolinguistic developmental timelines also affect DHH children learning American Sign Language (ASL). As a separate language that is visual rather than auditory, that utilizes unique syntactic, semantic, pragmatic, and phonemic qualities (Parasnis, 1998; Stokoe, 1960), some might expect distinctive developmental trajectories. However, it has been shown that critical linguistic milestones occur with the same sequence and timing as do spoken languages (Anderson & Reilly, 2002; Mayberry & Squires, 2006). A similar range of linguistic deficits also is seen with children experiencing late exposure to ASL (Mayberry, 2007; Mayberry et al., 2011; Mayberry & Lock, 2003; Mayberry et al., 2002; Singleton & Newport, 2004). Boudreault and Mayberry (2006) found that the age of acquisition affected subsequent language acquisition and final ASL syntax. ASL development conforms to the same preexisting and neurologically determined characteristics that support spoken language acquisition, with developmental patterns again emphasizing the importance of early and complete linguistic access.
A number of measures have been undertaken to ensure that young DHH children have adequate linguistic access to the language of their environment. The Universal Newborn Hearing Screening legislation requires hearing testing beginning at birth and state-based intervention services (Anderson, 2006). The Joint Commission on Infant Hearing (2007) has similarly recommended that newborns are tested within the first month, with a diagnosis by 3 months, and early intervention services started within 6 months. However, ensuring that these early critical steps occur has not yet been solved as suggested by Holte et al. (2012): Of 193 infants who did not pass initial hearing screening, only 32% met the two subsequent timelines.
Communication Concerns
The presence of hearing loss, irrespective of the level of loss, not only creates barriers to language acquisition but also compromises much of these children’s access to academic content. The substandard performance of DHH students has been documented for over four decades: Mean reading comprehension scores for 18 year olds on the Stanford Achievement Test have never exceeded the fourth grade since the 1970s, and math procedures scores peak at around the seventh grade (Qi & Mitchell, 2012; Traxler, 2000). Schools are required to accommodate hearing loss under both the Americans With Disabilities Act Amendments (2008) and the IDEA (2004). However, these do not compensate for missing linguistic structures, world understandings, or the higher order cognitive skills required to retain and utilize academic content. These deficits exist despite typical intellectual abilities but are the results of inadequate neurological activation in conjunction with missing linguistic competencies and language-mediated learning experiences.
DHH students from preschool (age 3) through 12th grade typically qualify to receive special education services in that their disability has an adverse effect on their educational performance (IDEA, 2004). These students’ language, communication, and subsequent academic learning needs are addressed through the IDEA (1997, 2004) requirements. Section 300.347(a)(2) of this act requires the educational team to document services through an Individualized Education Program (IEP) that must include a number of elements, the key academic items being the following:
A statement of the child’s present levels of academic achievement and functional performance;
A statement of measurable annual goals, including academic and functional goals designed to meet the child’s needs and support progress in the general education curriculum;
A description of how progress toward meeting the annual goals will be measured and when progress reports will be provided (American Foundation for the Blind, 2016; U.S. Department of Education, 2006; Wright & Wright, 2016).
The individualized nature of these services is important because DHH children use a range of communication modalities and languages (Allen & Anderson, 2010; Andrews & Rusher, 2010; Stredler-Brown & Arehart, 1998). These can be conceptualized as a continuum anchored by ASL and largely visual communication on one end, and use of oral/aural spoken English and auditory-only communication on the other (Scott, 2006).
IDEA Special Factors
As described earlier, despite requirements for individualized educational services that meet their unique learning needs, DHH student achievement has remained substantially below that of their normal-hearing peers for several decades (Karchmer & Mitchell, 2003; Marschark & Lukomski, 2001; Marschark et al., 2007; Qi & Mitchell, 2012; Shaver, Newman, Huang, Yu, & Knokey, 2011; Traxler, 2000; Wagner, Newman, Cameto, & Levine, 2006). This led the U.S. Department of Education to set policy guidance in 1992 and 1994 in applying the IDEA to ensure an appropriate education for DHH children. Language added to the IDEA 1997 and 2004 requires that each DHH child’s IEP address the following:
(2) Consideration of special factors. The IEP Team must— (iv) Consider the communication needs of the child, and in the case of a child who is deaf or hard of hearing, consider the child’s language and communication needs, opportunities for direct communications with peers and professional personnel in the child’s language and communication mode, academic level, and full range of needs, including opportunities for direct instruction in the child’s language and communication mode. (§300.324(a)(2)(iv))
The range of language and communication preferences among DHH students (Allen & Anderson, 2010; Andrews & Rusher, 2010; Stredler-Brown & Arehart, 1998) emphasizes the importance of individualized planning. These requirements entail opportunities for direct communication with peers and educational professionals, and direct instruction from teachers. Several accommodations (captioning, use of interpreter) require a device or individual to serve as a mediator. This provides access but leads to indirect communication, which can be a barrier to forming interpersonal relationships with peers and others. Direct communication requires the professional or peer to be fluent in the child’s preferred language and mode of communication.
The implementation of federal statutes is complicated by the Tenth Amendment of the Bill of Rights with education among the powers reserved to states (Rothstein & Johnson, 2010). The IDEA federal regulations serve as a basic framework. However, each state determines IEP document formats although individual school systems may design their own IEP forms with oversight from the State Educational Agency (SEA; U.S. Department of Education, 2007). As such, “The local educational agency, in providing for the education of children with disabilities within its jurisdiction, has in effect policies, procedures, and programs that are consistent with the State policies and procedures established under section 612” (IDEA, 2004, Section 613).
One effect of states’ educational rights is the variability with which they meet federal requirements. Morningstar and Liss (2008) found few states with policy or guidance documents to meet IDEA 2004 transition requirements. Instead, interpretation of requirements often was left to IEP teams. This led the Office of Special Education Programs (OSEP) to require evidence of meeting 17 IDEA indicators as part of each state’s annual performance plan. A more recent Results Driven Accountability initiative focuses on programmatic results rather than compliance but still requires data on key IDEA indicators (U.S. Department of Education, 2015, 2016).
The specificity with which states delineate the IDEA requirements on educational planning forms is important. Only by detailing these conditions can states ensure that school-age DHH students have full access to academic instruction and the interactions that support their acquisition of comparable cognitive, social, and linguistic skills. The variability in state responses potentially affects these students’ access and overall academic outcomes. Early state efforts to meet requirements to address these special language and communication factors were undertaken by New Mexico and Colorado who developed communication plans that accompanied the IEP. Other states have instead revised their IEP forms.
This study examined state IEP and communication plan templates posted on state websites to examine this diversity. These templates were examined for the ways in which they identified the special factors for DHH students. The research was undertaken with the assumption that because states remain accountable to meet IDEA requirements, their posted forms provide a template for schools and districts. Even in states allowing district independence, these districts may expand but cannot eliminate elements, and must remain in compliance with state and federal requirements. The research questions investigated the format and specificity of state IEP and communication plan templates to answer the following:
Given states’ sovereignty in educational issues, planning documents that included a communication plan were not expected to be any more specific than requirements to use only an IEP form. Each format could instead address unique state-identified concerns rather than responding to these federally defined special factors.
Method
Data collection consisted of identifying and downloading the IEP and communication plan templates posted on each SEA’s website, based on a search of all 50 state departments of education. State departments also were contacted by email or phone when documents or their requirements were not clear through these website materials. This supported a descriptive analysis of each state’s IEP or communication plan template to identify the ways in which IDEA requirements were met regarding the first research question. Each state’s IEP or communication plan template was rated for meeting each element of the requirements to compare among the states’ IEP and communication plans with regard to the second research question.
Instrumentation
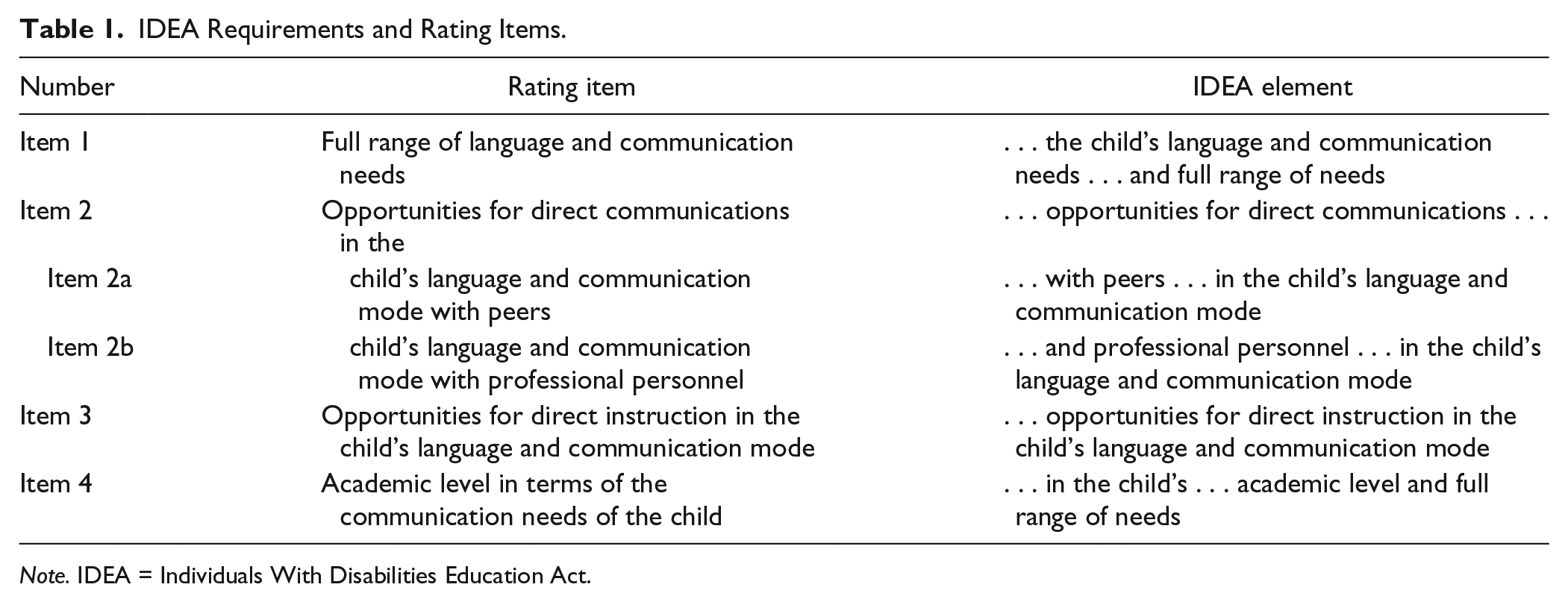
The IDEA special factors’ language was used to develop a rating instrument for Research Question 2. This language (see page 3 above) was parsed into separate items to allow evaluation of each of the required elements. These are shown in Table 1.
IDEA Requirements and Rating Items.
Note. IDEA = Individuals With Disabilities Education Act.
The IDEA included redundancies concerning the importance of the full range of the child’s needs and his or her language and communication mode preferences, which were merged into the parsed items, as appropriate. Item 1 addressed the full range of communication and language needs. Item 2 addressed the requirement for direct communication opportunities, separated to evaluate opportunities with peers (2a) and with professional personnel (2b). Item 3 identified opportunities for direct instruction in the child’s language and communication mode, and Item 4 addressed the child’s academic level in conjunction with his or her full range of needs.
Because the instrument language was taken directly from IDEA, its validity was not evaluated. These elements were part of the 1992 and 1994 guidance policies, and incorporated into IDEA 1997 and 2004 legislation, and therefore considered evidence of content and construct validity. The instrument was carefully scrutinized for rating consistency and reliability. Ratings used a Likert-type scale defined as 0 = absent or not addressed, 1 = minimal, 2 = somewhat, 3 = mostly, and 4 = completely addressed. The 1 to 4 range was chosen in forcing evaluators to choose a valence, as either more or less evident. This forced choice avoids a tendency to centralize or neutralize ratings that can reduce the strength of evaluative comparisons.
The reliability and fidelity evaluation used independent ratings of each of the 50 state’s IEP or communication plan templates by both authors. Each scanned the entire IEP and/or communication plan for the location of each rating item. If the item could not be found or language of the document did not address the item, it was marked as 0. Once the item and language were identified, it was coded between 1 and 4. Items coded as 1 included an indirect or partial reference to the item; those as 2 included a direct reference but omitted critical elements; those as 3 included most of the critical elements; and those as 4 directly referenced all elements. The authors met to compare ratings, discuss discrepancies, and provide evidence for each rating, and to compare with other states’ ratings to ensure consistency. Individual ratings were used to calculate interrater reliability.
The order for evaluating the state plans was calculated using a randomly generated sequence, divided into five groupings. The first group consisted of three states to serve as an assessment of scale and coding validity and reliability. The comparison of ratings across the items between the two evaluators was identical, and therefore no item or scale revisions were made. The grouping size increased to 10 for the next three groups with the last group comprising the remaining 17 states. The rating accuracy and fidelity continued to be demonstrated across each of the groups. The two evaluator spreadsheet of ratings were compared at each session with discussion of evidence to support ratings, and a final rating decision made separately. Evaluation discrepancies were anticipated; however, all were resolved using this process. Few differences occurred overall with a majority being due to difficulties in locating item language for some states’ IEP forms due to form diversity. Rather than issues with interpretation and evaluation of state items, most of the differences were due to identifying the location of content. This is additional evidence of the reliability and fidelity of the rating procedure, and interpretation of item and rating descriptors. Final interrater agreement was calculated at 100% (r = 1.00).
Analyses
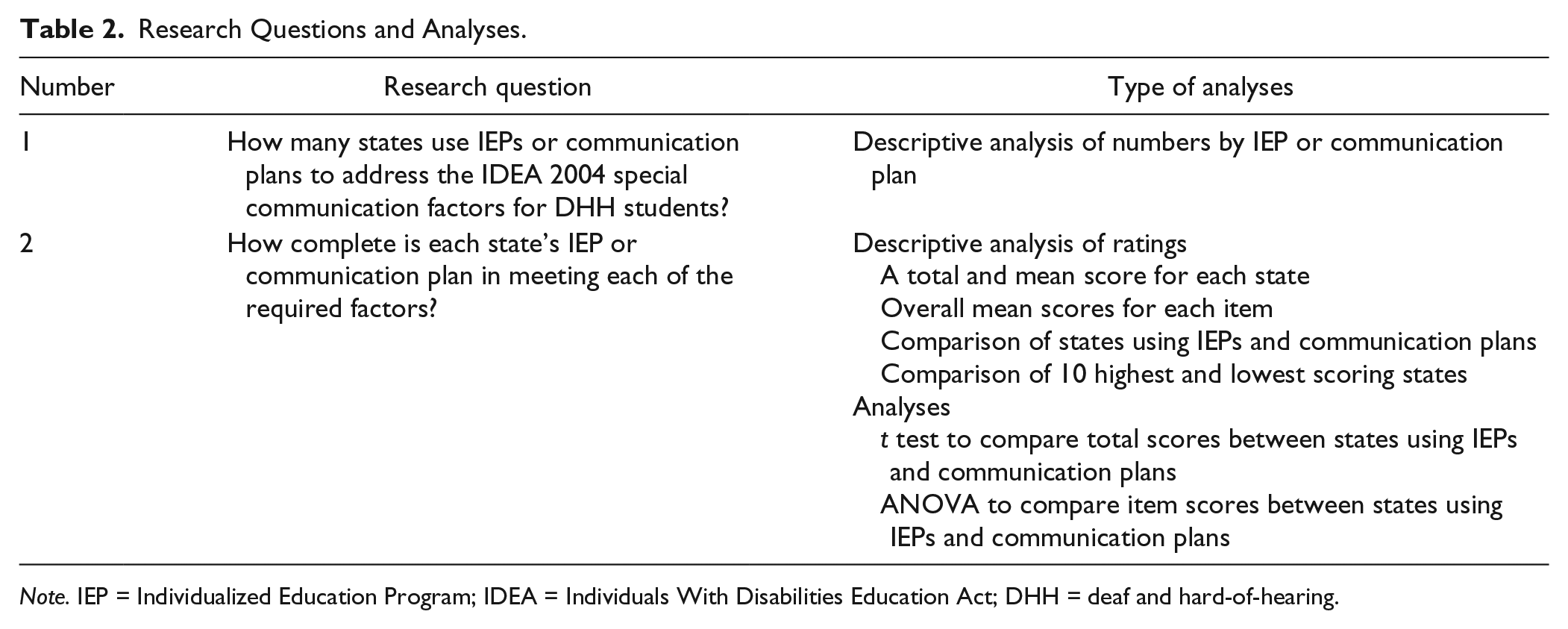
The first research question examined the number of states using IEPs or communication plans to address special factor requirements. This was answered using descriptive data compiled across the state templates. The second question examined the specificity of these templates in addressing the special factors. This was answered by rating each state’s template using a Likert-type scale and calculating mean ratings across states and items. Statistical analyses used a t test to compare mean ratings between states that used IEPs and those that used communication plans. An ANOVA compared mean ratings across states and among individual items to further identify patterns. Table 2 lists the analyses by research question.
Research Questions and Analyses.
Note. IEP = Individualized Education Program; IDEA = Individuals With Disabilities Education Act; DHH = deaf and hard-of-hearing.
Results
Research Question 1 examined the number of states using IEPs compared with those using communication plans. Eighteen states used a communication plan as part of each DHH student’s IEP (CO, CT, DE, FL, GA, IA, IL, IN, KS, ME, NC, NH, NM, OH, PA, TX, VA, WV) of which 16 were required (all except OH & TX). Several states’ communication plans were linked to an electronic IEP form as a pop-up element that appeared when teams marked the presence of a hearing loss. The 32 states using their IEP template took a variety of approaches with two states not including any language regarding the special factors. Typical strategies among the other states consisted of the following, used singly or in various combinations:
A single checkbox on the IEP form denoting that the DHH student had communication needs,
A multipart checkbox on the IEP that listed each of the special factors, or
Special narrative sections to describe communication or educational issues.
The checkboxes in many state IEP templates used a yes or no choice to identify presence of a hearing loss. Many did not require further description regarding the range of language or communication needs. Just one state (KY) listed each of the factors on their IEP template, with a narrative text box to describe individual issues and programming supports. This was the most detailed IEP form across all 50 states in responding to the federal requirements.
Research Question 2 examined the specificity of each state’s template in addressing the special factors. Each state was rated separately by the two authors, and the results used for descriptive and statistical analyses. The Ohio and Texas ratings were based on their IEPs in that their communication plans are not required. The frequency of ratings across items showed that the 0 rating was most numerous with a total of 95 out of 250, or 38%. Items rated as 4 had the second highest frequency with a total of 78 (31.2%). There were 46 ratings of 1 (18.4%), 26 of 2 (10.4%), and five of 3 (.02%). Overall, patterns suggest that states did not identify each element or did so with minimal specificity based on the number of low ratings. Only in a few instances did states include most of an item without listing all of its component elements (rating of 3).
A further examination compared patterns among the 10 states with the highest and lowest total ratings. Eleven states with the highest rating of 20 (maximum of four for the five items) including CO, FL, IL, IN, IA, KS, NH, NC, PA, VA, and WV. All contained comparable elements and several utilized a similar communication plan. States with the lowest ratings included ID and LA whose IEP templates included no elements of the IDEA language (totals of 0). States with total ratings of 1 included CA, HI, MN, MT, and UT, and 11 other state totals of 2 (AL, MS, MO, NV, NJ, OH, OK, RI, TX, VT, and WA). Eighteen states’ rating totals were 2 or less out of a possible 20. All of these states used their IEP template, included little if any of the IDEA language, and used generic program and disability descriptors (ratings available from first author).
Ratings were then used to compute means for each state and for each item across states. The overall mean rating for the five items across the 50 states was 1.56 (SD = 1.52; 4 = highest). A subsequent analysis examined the means of the five items individually 1, 2a, 2b, 3, and 4, with item means of 1.82, 1.34, 1.22, 1.32, and 2.08, respectively, across the 50 states. Two items with the highest mean scores, numbers 1 and 4, also showed a high frequency of ratings above 0, with 42 above 0 ratings for each. A majority of states asked for some type of description of the DHH students’ communication needs for Item 1. Many states required a description of how each student’s academic performance was affected by hearing loss for Item 4 and how these needs were met. Items 2a, 2b, and 3 were less specifically addressed by states with each item having more than half of the states rated at 0 (range of 26–28 states). States were less likely to include specific language regarding direct communication with peers and professional personnel, or direct instruction, using the child’s preferred language and communication mode. States more explicitly required that the child’s full range of language and communication needs, and their academic levels be addressed on these forms, with means of 1.82 and 2.08, respectively.
The next analysis compared states with and without communication plans, finding that those using communication plans had overall mean ratings of 3.84 out of 4.0 (SD = 1.90), indicating that most elements were explicitly identified. States without a communication plan had a mean of 0.65 (SD = 0.65), indicating an overall rating between absent or not addressed and minimal. A t test between the two groups was significant (p < .000, df = 1, mean square = 2,166.212, F = 140.822) supporting higher positive ratings of states using communication plans. A Levene test for homogeneity of variance was not significant (p = .052) although close, suggesting that the assumption of homogeneity of variance was upheld. A test of skewness indicated a positive .823 score due to a longer right tail (for higher ratings), also upheld by a kurtosis score of −1.124. This affirms the effect of the larger group of comparatively lower scores for the states using IEPs.
A multivariate comparison of the two groups (with/without communication plans) across each of the five items was significant for every comparison (p < .000) with higher ratings for states with communication plans. Across all states, communication plans were most similar on Item 4 which was information about the student’s academic level and was most commonly addressed on the state IEP forms. The ratings were most different on Item 2a, which was opportunities for direct communication with the DHH students’ peers.
Discussion
The purpose of this study was to examine the format and specificity with which states included the IDEA 2004 special factors for DHH students in their annual educational planning documents. This was accomplished by examining each of the IEP or communication plan templates on state’s department of education website. The lifelong adverse effects of poor language have made this an educational priority (IDEA, 1997, 2004). The first research question tallied the number of states using IEP and communication plan templates with 16 of the 50 states requiring use of a communication plan. The remainder used their state IEP templates with the variety of formats signifying the strength of state sovereignty in choosing the means by which they meet their educational responsibilities.
The second research question rated each state’s template for including each of the federally required special factors. Overall, states using a communication plan had higher ratings across all of the factors. Statistical analyses showed that states using IEP templates were rated significantly lower compared with state communication plans. State plans with higher ratings would likely be found as more compliant in response to federal audits.
Across the different communication plans, many were similar and scored high by including the IDEA language. Most required detail about the child’s language and communication mode preferences including the persons and environments in which these preferences were used. Many included a comprehensive list of receptive and expressive language options from among those on the communication continuum (see Scott, 2006). Some plans included elements not in the IDEA 2004, such as the DHH child’s access to deaf peers and role models, and communication training needs for parents or professionals. These address important factors that support a child’s linguistic and academic success although not part of this study. Use of communication plans as part of the annual IEP process not only meets a child’s current needs but also allows for modifications as the child matures and as new communication technologies and accommodations become available. This helps to ensure that communication and language preferences are appropriate not only when the child first enters school but also over time as well.
Several states utilized communication plans that did not include as many of the IDEA’s required elements. These were the states of Connecticut, Delaware, and Maine with rating totals from 5 to 12 out of a possible 20 and were lower than other communication plans. The Connecticut and Maine plans focused on the type and nature of accommodations selected for the DHH student. The Delaware plan briefly identified language and communication preferences but did little to address direction communication or instruction with professional personnel, or the child’s range of academic needs. Two other states, Ohio and Texas, suggested use of a detailed and specific communication plan but this was not required and therefore not evaluated. These plans were similar to that of Colorado and would otherwise have led to high ratings.
The rating process revealed one high-scoring state’s IEP form. Kentucky’s IEP clearly delineated each required IDEA element followed by a narrative section for each item to specify issues and programming supports for DHH students. No other state’s IEP template was comparable. Interestingly, both the Ohio and Texas’s IEP templates included a separate page to document strategies used to address the special factors for students with visual impairments (IDEA, 2004), but had no such page to address the special factors for DHH students.
Implications
The large number of states whose templates are rated poorly should concern educators and parents of DHH children, particularly those living in the 18 states with rating totals of 2 or less out of 20. Overall, 81.125% (26/32) of states without communication plans had totals of less than 5 (average of <1.0 for each item). The IDEA instituted these requirements first in 1997 and again in 2004; yet despite more than a decade, a majority of state templates do not include the specific language that ensures annual educational plans that meets DHH students’ language and communication needs. These students have critical needs for full access to language and communication for maximizing their academic achievement. Although their greatest language development occurs prior to entering school-based services, the brain retains some plasticity with linguistic plateaus not occurring until adolescence (Boudreault & Mayberry, 2006; Delage & Tuller, 2007; Mayberry et al., 2011). Therefore, full access to communication remains important throughout much of DHH students’ K−12 programs to support their continuing linguistic development and the ongoing availability of instruction.
In that schools focus primarily on academic access for students with disabilities, it may not be surprising that Item 2a, direct communication access with peers, had the greatest disparity (3.2684) between states with and without communication plans. However, the impact of neglecting this element may result in limited opportunities for DHH students to form interpersonal relationships in schools. Particularly at secondary levels, the presence of an interpreter or an assistive device creates a barrier to teenage interactions. Yet schools are social as well as academic learning environments for all other students, and should be equally so for DHH students. Reports of isolation and marginalization from the school community suggest that limited direct peer communication may be common (Foster, 1998; Gannon, 1981; Johnson, DesGoerges, & Seaver, 2013; Ramsey, 1997). Societal goals to graduate fully participating adults require that DHH students have full access to the typical range of school-based activities and interactions. These are the opportunities that also allow for their acquisition of world and sociocultural knowledge that are critical to their lifelong success as future citizens.
What is more surprising is that Item 3, which requires direct instruction, had the second greatest disparity (3.0221) between states with and without communication plans. This implies that many schools may not recognize the importance for DHH students to communicate directly with teachers or school professionals without use of captioning or an interpreter. Although similar in disparity (2.8934), there was a somewhat greater recognition of the importance of some professionals who could communicate directly with DHH students, Item 2b. Overall, the lack of attention to opportunities for direct communication and instruction for DHH students suggests that many of these students may remain socially marginalized during their PreK−12 experience.
Limitations
This study did not review completed IEPs that would have provided a more authentic evaluation of IEP and communication plan compliance with IDEA. However, this examination would require samples from multiple school districts within states, weighted for demographic and other key characteristics. Membership of IEP teams would need to be controlled given annual fluctuations among representatives. A particular individual could substantially effect team decisions requiring a wide sample to address cohort variations by year and region. Such a study was not within the resources of the research team.
Conclusions and Recommendations
The IEP and communication plan templates examined in this study documented a range of state responses in meeting federal IDEA 2004 requirements regarding special factors affecting the education of DHH students. Those states using IEP templates typically were less specific in identifying these factors with a majority including only minimal references to the elements. Twenty-six states had rating totals of less than 5 out of 20. It is not clear how such states can provide effective oversight and audits of their districts regarding these requirements. Use of a communication plan or IEP template with specific IDEA language would facilitate oversight procedures and is utilized by 17 states. Kentucky was the one state that incorporated much of the federal language into its IEP template.
The study suggests that a strategy for meeting federal or state requirements is to include specific language in required IEP or communication plans. That many states include little of this indicates the strength of state sovereignty over educational issues, despite federal regulations. States are required to report on IDEA indicators in their annual plans (U.S. Department of Education, 2007, 2015, 2016) but there appear to be few sanctions for noncompliance.
One recommendation for improving educational planning for DHH students is to require a communication plan in conjunction with an IEP. Several highly rated states referenced the Colorado plan, one that thoroughly addresses the range of expressive and receptive language and communication preferences of each student. The form includes a range of options such as home and idiosyncratic sign languages, as well as support and training needs for parents and professional personnel. This plan also identifies strategies for increasing opportunities for DHH students to have direct communication and instruction, and access to deaf peers and mentors. These all support opportunities for forming interpersonal relationships, improving the overall educational experience and access to informal learning, and minimizing the marginalization that can occur for DHH students in the school environment.
To ensure that IEP teams complete required communication plans as part of the IEP, several states have used hyperlinks with electronic IEP forms. The communication plan appears as a pop-up item after the team identifies a student as having a hearing loss. A benefit of completing the communication plan early in the IEP planning process is that supports and opportunities for direct peer and professional interactions, direct instruction, and parent or personnel training can be included on the IEP’s listing of supports and services. This ensures that these activities will occur as a result of IDEA’s legal protections. Another important element of many communication plans was their identification of personnel or technology accommodations and, most importantly, alternative plans in case of personnel absence and technology malfunction or failure. Any of these can leave a DHH student isolated until the situation is rectified, and upon occasion, these students have been removed from scheduled classes until this happens. Preparing for these and related situations is important in guaranteeing effective educational support of DHH students and in meeting the educational responsibilities assigned to districts and schools.
A second strategy for ensuring compliance is for states to develop a highly specific IEP form that includes required elements. The Kentucky plan included IDEA language on their IEP form. Two states’ IEPs offer an alternative although neither used this for their DHH students. Both Ohio and Texas had a required IEP addendum page for students with visual impairments that listed all of the special factors for these students (IDEA, 2004).
Communication remains the fundamental means through which most academic learning is transmitted. Given the continuing low achievement of many DHH students, guaranteeing full communication access in accordance with their preferences is a critical step toward raising their performance (Karchmer & Mitchell, 2003; Marschark & Lukomski, 2001; Marschark et al., 2007; Qi & Mitchell, 2012; Shaver et al., 2011; Traxler, 2000; Wagner et al., 2006). Otherwise, their generally poor academic performance, which has been a defining characteristic across more than four decades, will likely remain unabated. The cost of specialized services and supports for DHH students provided during the PreK−12 experience is more than recouped as these individuals become working members of society (cf. Bowe, 2003). However, this presumes that needed services are provided in appropriately individualized ways. The DHH student population’s range of language and communication preferences emphasizes the importance of individualized planning and supports required to meet their needs (Allen & Anderson, 2010; Andrews & Rusher, 2010). The IDEA 2004 added these special factors to its requirements to ensure that this population’s unique needs were addressed. But only by specifying these elements on planning forms can there be some assurance that DHH students will receive the educational services they deserve in the language and communication mode they prefer.
Footnotes
Authors’ Note
This article uses the terminology DHH children, placing the descriptor prior to the noun as the usage preferred by the Deaf community (Lane, Hoffmeister, & Balan, 1996).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.