
Abstract
This longitudinal population cohort study tracks the transition of 1,405 adolescents with autism spectrum disorders (ASDs) into adulthood, and highlights functional and social skills as core predictors of social outcomes (tertiary education, civic volunteering, and employment). Applying regression methods with sample selectivity to administrative data records obtained from Israel’s National Insurance Institute, we show that these outcomes are not highly correlated, suggesting that the high/low functioning dichotomy frequently used to categorize individuals with ASD is not supported by these data. We show that there is no causal relation between civic volunteering at an earlier stage and subsequent participation in tertiary education. This suggests that the traditional sequential model of developmental disability does not apply to ASD, and that the social-functional model of disability seems more applicable. We also show that functional and social severity vary inversely with year of diagnosis, due probably to the application of more liberal diagnostic standards. Disability among successive birth cohorts has been decreasing and is expected to decrease further in the future. Parents’ income has only a modest beneficial association with the transition into adulthood, and socioeconomic environments have no effect at all. Findings are discussed with respect to policy and practice.
Although study of children and adolescents with autism spectrum disorders (ASDs) has expanded enormously, research on their transition into adulthood is sparse (Levy & Perry, 2011; Wehman et al., 2014). Such studies have tended to focus on one or two interrelated outcome measures, primarily symptomatology and communication skills (Schall & McDonough, 2010), or on the relation between ASD symptoms and employment placement (Holwerda et al., 2012; Taylor et al., 2012). We are unaware of studies that track the relation between multiple functional measures, such as social and communication skills and/or activities of daily living (ADL), and multiple outcomes, such as engagement in social activities, tertiary education, and employment. Moreover, although population cohort data are increasingly used to study ASD among children (Beenstock et al., 2015; Raz et al., 2015; Russell et al., 2015), research on the transition into adulthood is based on survey and clinical data. Population cohort data are methodologically superior because they contain more observations and are free of potential sample selection bias.
The traditional model used in disability studies has been primarily medical, assuming that successful transition into adulthood is sequential, if not necessarily linear (Marks, 1997). Accordingly, the completion of earlier developmental milestones lays the foundations for the successful passage of subsequent milestones. This medical model has been challenged by the social-functional model (World Health Organization [WHO], 2001), according to which “successful participation” in adult life is not necessarily sequential but interfaced with activities, and personal and environmental opportunities, such as leisure or employment programs (Orsmond et al., 2013). Whereas the traditional model hypothesizes causal effects between type and severity of impairment and functioning, the social-functional model offers an alternative transactional approach. In the case of the transition into adulthood, the lack of consensus about developmental milestones is even greater, especially compared with children with other developmental disabilities (Matson et al., 2012). Investigation of both models in the context of ASD is naturally more complicated than it is with other developmental disabilities, which are easier to assess at an early age.
Diagnosis and Measurement
Diagnosis of pervasive developmental disorder (PDD) or ASD begins at about 30 months and has a long tail extending into teenage years (Beenstock et al., 2015; Raz et al., 2015). Importantly, diagnostic criteria have changed over time. Until 1995, ASD was defined by Diagnostic and Statistical Manual of Mental Disorders (3rd ed.; DSM-III; American Psychiatric Association [APA], 1980) as a pervasive lack of responsiveness to other people, gross deficits in language development, and bizarre responses to various aspects of the environment (DeMyer, 1979). Subsequently, the definition was broadened in DSM-IV (Diagnostic and Statistical Manual of Mental Disorders [4th ed.]; APA, 1994), DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders [4th ed., text rev.]; APA, 2000), and DSM-5 (Diagnostic and Statistical Manual of Mental Disorders [5th ed.]; APA, 2013). In Israel, the clinical assessment of ASD was based on the traditional medical model. In recent years, there has been a shift to the social-functional model. Although Matson et al. (2011) found differences in expressions of symptoms among people with ASD in Israel, the United States, the United Kingdom, and Korea, they found no significant differences in social relationships.
Studies of the transition into adulthood have almost exclusively been informed by sample data for the United States with occasional exceptions. Historically, ASD outcome data were mainly clinical and measured functioning in communication skills and dependency by the severity of symptoms. Studies focused primarily on adolescents and adults living with their parents and enrolled in educational or rehabilitation settings (Rumsey et al., 1985; Szatmari et al., 1989). It was assumed that individuals with better communication and ADL skills did better than their less skilled counterparts (Kanner, 1971).
Lockyer and Rutter (1970) were the first to propose non-clinical outcome measures, including educational attainment, employment history, degree of independent living, and social relationship skills. The most salient measures were related to performance in educational and employment settings, and ability to live independently (Magiati et al., 2014). Studies of severity utilized subjective measures, primarily professional observation–based assessments, or parents’ ratings of their children’s symptoms and behavior. Standardized studies report improvement in behavioral problems in late adolescence, which are attributed to the maturation processes (Byrd, 2002; Howlin & Moss, 2012; Matson & Horovitz, 2010). Some studies report improvements particularly among individuals who function better, participating in educational or habilitation programs (Byrd, 2002; Howlin & Moss, 2012; Shattuck et al., 2007; Shea & Mesibov, 2005). Interestingly, they fail to track changes in severity over time (Billstedt et al., 2007; Larsen & Mouridsen, 1997), noting that early adolescence is the most difficult phase, which plateaus in mid- to late adolescence (Larsen & Mouridsen, 1997; Venter et al., 1992).
Outcomes in Young Adulthood
The most common social outcome that is linked to independence used in adult ASD research is employment followed by educational attainment, social participation, and family support (Chen et al., 2015; Orsmond et al., 2013). Individuals with ASD may be able to work but are impeded from doing so (Hendricks, 2010). Indeed, employment cannot be separated from functioning and social participation (Roux et al., 2015). Investigating social participation and social engagement in community activities among young adults with ASD is important given the incidence of detachment from social contact. According to Orsmond et al. (2013), almost 40% of youth with ASD had never got together with friends, and almost 50% of young adults never received phone calls from friends or were invited to social activities. However, engagement in volunteering and activities after graduating high school promotes success in life (Carter et al., 2013).
About 50% of students with ASD drop out from school (Chung et al., 1990), and even fewer complete college or university (Eaves & Ho, 2008; Howlin & Moss, 2012). These individuals underachieve and demonstrate high job separation rates (Barnhill et al., 2007; Eaves & Ho, 2008). The most important predictors of success in the workplace are lack of disadvantages in the labor market and substantial support received from employers and coworkers (Baldwin et al., 2014). Most young adults with ASD are highly dependent on their families, and about half of those who functioned better live with their parents (Eaves & Ho, 2008). The socioeconomic status (SES) of parents plays an important role in helping children with ASD. Pickard and Ingersoll (2015) reported that educated middle- and upper-middle-class parents tend to be more aware of their children’s needs and are better at accessing services. By contrast, parents with lower SES find it more difficult to cope with their children and are more in need of information and in-home services.
In their review of the transition into adulthood, Anderson et al. (2018) have drawn attention to the lack of research into the roles of social capital, including family systems, social networks, communities, neighborhoods, delivery systems for services, and the role of public policy. The present study touches upon some of these issues through its focus on parents, neighborhoods, ethnic groups, the peripherality of communities, and policy toward civic volunteering in Israel.
In this article, we offer a new methodology for studying the transition into adulthood of individuals with ASD using longitudinal population cohort data for Israel. Specifically, we investigate whether subsequent outcomes, such as participation in tertiary education, depend on the successful passage of earlier outcomes, such as civic participation, as predicted by the traditional medical model. We also investigate whether this association is induced by social functioning as predicted by the social-functional model. We use measures of ADL and social functioning at age 18 as potential predictors of outcomes in adulthood. In addition, controls include demographic and background variables such as gender, ethnicity, and parents’ income, as well as controls for socioeconomic environments in terms of their SES scores and the peripherality of their localities. Because we focus on several outcomes, we are able to estimate the roles of differential ability in achieving them. Indeed, these measures facilitate the identification of the causal effects hypothesized by the medical sequential model. In this article, we focus on these theoretical models and are not concerned with specific practices designed to help youth with disabilities find work (Luecking, 2009).
In summary, our study involves several interrelated research questions:
We use longitudinal population cohort data for Israel to answer these questions. This is the first study of the transition into adulthood using population cohort data and is one of the few studies for a country other than the United States.
Method
Davidovitch et al. (2013) estimated ASD prevalence in Israel at 0.48% for 1- to 12-year-olds and 0.65% for 8-year-olds in 2010. By contrast, according to the Centers for Disease Control and Prevention (CDC), prevalence at 8 years in the United States is currently 1.7%. However, ASD prevalence has been rising in Israel as elsewhere (Raz et al., 2015).
The data for the present study, which covered 1,405 individuals with ASD ages 18 to 30 in 2014, were obtained from administrative records at Israel’s National Insurance Institute (NII), which, since 1981, has provided a special disability allowance to parents of children diagnosed with ASD (Supplementary Material 1. Contact
Three months before eligibility to this allowance expires at age 18, NII invites beneficiaries to apply for disability allowance as adults. Their applications include specialist doctor’s reports containing a score for ability to fulfill social roles (“social severity”) and another to measure their degree of dependency, ADL (“functional severity”). Applicants are subsequently examined by a specialist doctor appointed by NII, who also has access to applicants’ records at NII and who may adjust both scores. These scores are used to determine eligibility for disability allowances. Rejected applicants may appeal to a panel of three physicians. We use the final scores measured on a 5-point scale (1 = mildest and 5 = most severe) for “social severity” and (1 = independent and 5 = totally dependent) for “functional severity.”
Three outcomes are measured: months registered in tertiary education (vocational training or university), months volunteered in civic service, and the proportion of months employed since age 18 until December 2013 (the cutoff date for the data), excluding time spent in vocational training, tertiary education, and civic volunteering. Registration data on vocational training were obtained from the Rehabilitation Unit at NII. Registration data in higher education were obtained directly by NII from colleges and universities. Data on volunteering in civic service were obtained by NII directly from the agencies concerned (Israel Defense Force or National Civic Service; Supplementary Material 7). NII has monthly information on national insurance contributions, which constitute the longitudinal data source for months employed as well as monthly earnings.
Personal demographic data at NII consist of gender, immigrant status, age and year of diagnosis, and whether individuals lived with their parents at age 18. Because social science research in Israel attaches importance to ethnicity, we also distinguish between ultra-orthodox Jews, other Jews, and Arabs. The data have been matched to parents using NII records, including their monthly earnings and employment status. The municipalities in which children lived when they were 18 years old have been matched to socioeconomic clusters and peripheral clusters calculated by Israel’s Central Bureau of Statistics and are distinguished by urban and rural status. Because these data are from administrative records, measurement error is expected to be minor.
Characteristics of the study group, compared with the Israel population born between 1995 and 2005, are reported in Table 1. As expected, males and more recent birth cohorts are disproportionately represented. As observed by Raz et al. (2015), only about half are diagnosed by 8 years. The correlation between “functional severity” and “social severity” is 0.67; however, this correlation weakens with severity. The lowest group, in terms of “functional severity,” is the largest (64%). The largest “social severity” group (scoring 3) comprises 43% of the study group. Table 1 also records that the study group is overrepresented in the higher socioeconomic and peripheral cluster localities.
Characteristics of the Study Group (N = 1,405).

Note. NA = not applicable; ADL = activities of daily living.
Local authorities are clustered by their access to Tel Aviv and to each other (Tsibel, 2009). bLocal authorities are clustered by nine variables, including economics, housing, car ownership, schooling, social problems, and demography (Central Bureau of Statistics, 2003). cBased on professional assessments at age 18 at the National Insurance Institute of communication skills. See text. dBased on professional assessments at age 18 at the National Insurance Institute of ADL and related skills. See text.
Procedures
Most of the study group did not participate in any outcome. Therefore, to test hypotheses about the determination of these outcomes, a statistical methodology is required, which recognizes that the outcome data are neither continuous, a requirement for linear regression, nor dichotomous, a requirement for logistical regression. We therefore use the incidentally truncated regression (ITR; Heckman, 1976) method, which hypothesizes two populations: one that does not participate in the outcome of interest, hence y = 0, and another that participates for which the outcome is positive.
ITR involves the joint estimation by maximum likelihood of Equation 1 for participation, and Equation 2 for positive outcomes:


where φ( ) and Φ( ) are the density and cumulative density of the standard normal distribution, i labels individuals,
As there are three key outcomes in the study, ITR generates estimates of residuals e and u for each outcome. These estimates measure unobserved functional abilities, which are likely to be correlated within individuals. We specify estimates obtained for one outcome in the ITR models for the other two outcomes. For example, if individuals more likely to study are also more likely to work, e for tertiary education is specified as a “generated regressor” (Pagan, 1984) in the ITR model for employment (Supplementary Material 3). Whereas in single outcome studies these unobserved characteristics are concealed, in multiple outcome studies, such as ours, they are revealed. There are two natural stages to the generated regressor methodology. In the first, the three ITR models are estimated without generated regressors. In the second stage, the ITR models are re-estimated using the residuals obtained from the first stage, as generated regressors in the second. Because the residuals from the first stage are used as generated regressors in the second, there is no order in which the residuals are estimated and incorporated.
There are several time-related effects. First, individuals who happened to be younger in December 2013 had more opportunity to participate than their older counterparts; they are more censored. Second, there may be birth-cohort effects, which affect participation and outcomes. Third, if diagnostic criteria broaden over time, year-of-diagnosis is expected to have a positive effect on outcomes because individuals diagnosed more recently are likely to be higher up the spectrum. Fourth, if severe cases are diagnosed when younger, outcomes are expected to vary directly with age-at-diagnosis. Because year-of-diagnosis equals year-of-birth plus age-at-diagnosis, it is impossible to distinguish these three phenomena. Also, year-of-birth is perfectly negatively correlated with age in 2013.
The first effect is hypothesized to depend on the reciprocal of age in 2013 because younger individuals in 2013 are disproportionately more censored than their older counterparts. Because the reciprocal of age in 2013 is imperfectly correlated with year of birth, the first two effects may be identified parametrically. Because we are able to control for severity at age 18, the need to distinguish between the other effects is less crucial, as we comment in discussing the results.
A general-to-specific (GTS) search procedure (Hendry, 1995) has been used to select the final model specifications reported in Table 2. GTS initially includes X and Z variables suggested by theory and previous research. Subsequently, variables that are not statistically significant are excluded. However, GTS differs from a backward stepwise procedure because variables omitted at an earlier stage are subsequently respecified to check whether their previous exclusion was path-dependent (Supplementary Material 4).
ITR Models for Outcomes.
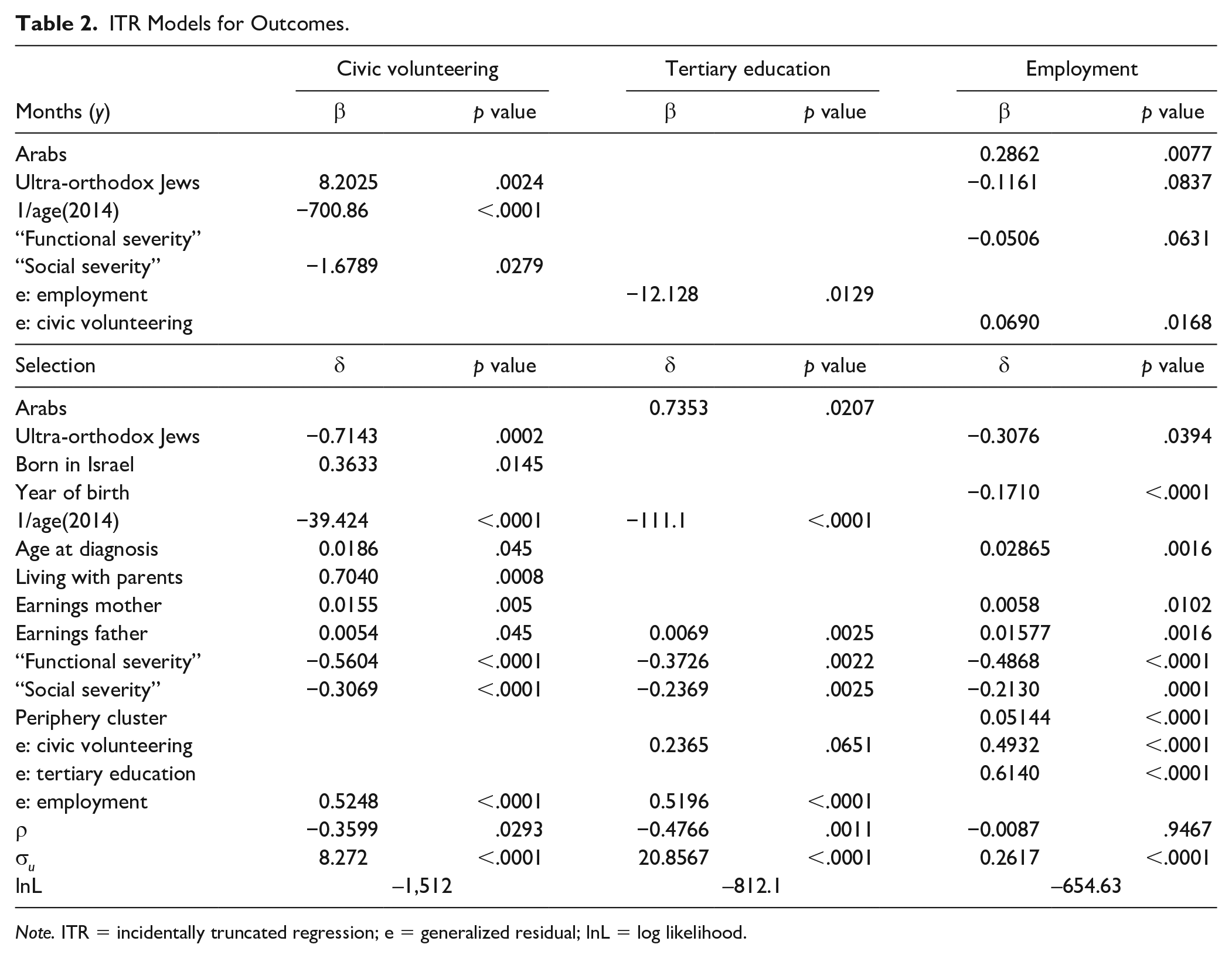
Note. ITR = incidentally truncated regression; e = generalized residual; lnL = log likelihood.
We also use a recursive bivariate probit (RBP, Greene, 2012) methodology to test whether there is a causal effect of earlier outcomes on subsequent outcomes. RBP involves the joint estimation of Equations 4 and 5 by maximum likelihood:


where y1 occurs before y2, disturbances e1 and e2 are correlated within individuals, and Y1 is a dummy variable if y1 is positive. If θ is positive and statistically significant, participation in Outcome 1 has a beneficial causal effect on participation in Outcome 2. If θ is not statistically significant, participation in Outcome 1 merely predicts participation in Outcome 2.
Results
Table 1 reports social outcome rates. Although 91.7% never participated in tertiary education, almost 20% engaged in civic volunteering and almost 30% had been in regular employment. The correlations between these outcomes are quite small, ranging from .2 between civic volunteering and tertiary education to .293 between tertiary education and employment. Also, 50% of those engaged in civic volunteering were employed, but only 35% of the employed engaged in civic volunteering. Therefore, just because someone did not participate in tertiary education or civic volunteering does not necessarily mean that he or she did not work. These outcomes are sequential insofar as civic volunteering always precedes tertiary education, and very few worked prior to civic participation and tertiary education (Supplementary Material 7).
ITR Models
We begin by reporting in Table 2 estimates of the ITR models for the three social outcomes in the study. The upper part of Table 2 reports the results for Equation 2 in which the dependent variable refers to the number of months spent in civic engagement, months of tertiary education, and employment measured by the fraction of time since age 18 spent employment. The lower part (selection) reports the results for Equation 1, which refers to the probability that the number of months is non-zero, that is, participation. Initial and interim specifications (Supplementary Material 4) show that the salient variables in Table 2 were salient in the initial and interim GTS specifications. Some variables, such as socioeconomic cluster and DSM regime, do not feature in Table 2 because they were not statistically significant. Other variables, such as demographic group, feature in some outcome models but not others, or they feature in the selection models but not the regression models (Equation 2), or vice versa.
The statistical significance of the variables retained in Table 2 is naturally high because of GTS; the largest p value is .0837. Variables were either clearly significant, as in Table 2, or their p values were prohibitively large. “Functional severity” and “social severity” were statistically significant in all three selection models. However, “functional severity” mattered for months employed but not for other outcomes, and “social severity” mattered for months of civic volunteering but not for other outcomes. “Year of birth” or the reciprocal of age in 2014 mattered for all selection models and for months of civic volunteering but not concurrently. Age-at-diagnosis mattered for selection into civic volunteering and employment but not for these outcomes in months. Some variables, such as periphery cluster, born in Israel, or living with parents (at age 18), only mattered for selection with respect to single outcomes.
Finally, the generalized residuals used to represent e in Equation 1 were statistically significant, especially for employment. Individuals with a greater susceptibility for employment as measured by its generalized residual were more likely to engage in civic volunteering and tertiary education but were also more likely to drop out of studying. Individuals with a greater susceptibility to engage in civic volunteering were more likely to work and study, and to work more if they do. These correlated effects are not causal because they express the unobserved functional abilities of members of the study group.
The estimates of ρ were negative in the cases of civic volunteering and tertiary education, and ρ was not statistically significantly different from zero in the case of employment. The former mean that individuals with a greater susceptibility to engage in civic volunteering and tertiary education volunteered and studied less if they did (negative selection). The latter means that the ever-employed and the never-employed stratified into distinct population subgroups. Indeed, because ρ was zero, the probit model for employment could have been estimated independently of its selection model.
Size effects of these variables for the three outcomes are calculated for the external and internal margins in Tables 3 (Supplementary Material 2). We begin with the probability of participation (external margin). The size effects of “functional severity” and “social severity” on all probabilities were large. For example, moving to a higher group of “functional severity” (e.g., from low to medium, or medium to high) reduced the probability of employment by 0.165 and the probability of studying by 0.051. Because “functional severity” and “social severity” comprise the same number of categories (five), Table 3 shows that the size effects for “functional severity” were larger (more negative) than for “social severity.” For example, in the case of employment, the size effect was twice as large for “functional severity” than for “social severity.”
Size Effects on Outcomes.
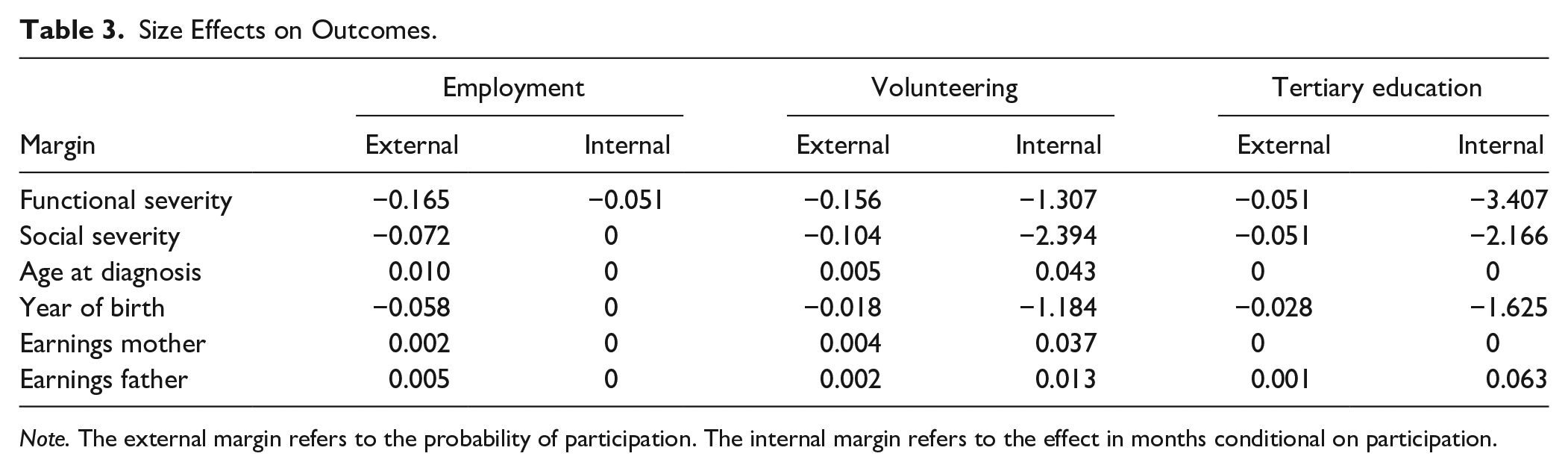
Note. The external margin refers to the probability of participation. The internal margin refers to the effect in months conditional on participation.
The marginal size effect of age-at-diagnosis was 0.01 in the case of employment, that is, the probability of employment is almost a percentage point higher. This effect was almost twice as large as the size effect for civic volunteering. The size effect for tertiary education was zero because age-at-diagnosis does not feature in Table 2 for tertiary education. The marginal size effect of year-of-birth was −0.058 in the case of employment, that is, individuals who were younger in 2014 were less likely to be employed because they were more censored. This censoring effect was strongest for employment and weakest, as expected, for civic volunteering. The implicit size effects for year-of-diagnosis are obtained by summing these two effects, which were negative in all three cases, for example, the size effect of year-of-diagnosis on the probability of employment was −0.0483; year-of-diagnosis reduced the probability of employment by almost 5 percentage points. Because earnings are measured in 1,000s of shekels (about US$250), the size effects for parents’ earnings were small. For example, if mothers earned an extra 1,000 shekels, the probability of employment increased by only a fifth of a percentage point. In the case of fathers, this effect was about half a percentage point.
Size effects for internal margins refer to months engaged in the outcomes conditional on participation. For example, the marginal effect of a category of “functional severity” reduced tertiary education and civic volunteering by 3.4 and 1.3, respectively. The effect of “functional severity” on the proportion of months employed was small (5 percentage points).
Observed Effect Between Civic Volunteering and Tertiary Education
Table 2 shows that individuals who were more likely to engage in civic volunteering were also more likely to engage in tertiary education. These effects do not have a causal interpretation. Because civic volunteering is the only outcome to precede another (tertiary education, Supplementary Material 7), the RBP model tests whether civic volunteering has a causal effect on tertiary education. Hence, y1 in Equation 4 refers to civic volunteering and y2 in Equation 5 refers to tertiary education.
Table 4 reports results. As in Table 2, the probabilities of engaging in civic volunteering and tertiary education varied inversely with “functional severity” and “social severity,” and there are other similarities. Table 4 shows that θ in Equation 5 was almost zero and is not statistically significant. Therefore, civic volunteering did not have a causal effect on subsequent engagement in tertiary education.
Recursive Bivariate Probit Model for Civic Volunteering and Tertiary Education.
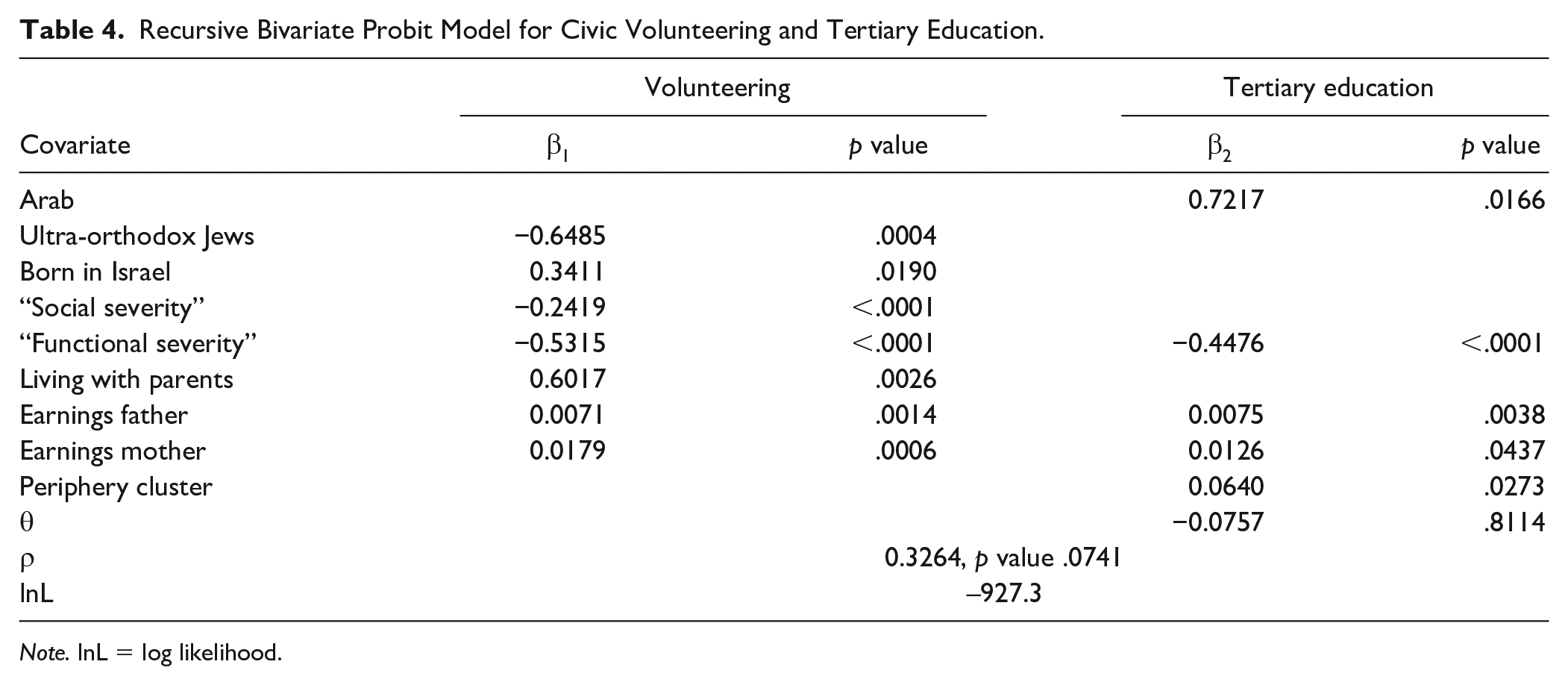
Note. lnL = log likelihood.
Severity Assessments at Age 18
If the increase in the incidence of ASD is due to the application of broader diagnostic standards, children diagnosed more recently are likely to have less disability as adults. If the increase in prevalence results from broader diagnostic standards, severity assessments at age 18 should vary inversely with year-of-diagnosis.
We use multiple regressions to estimate the determinants of severity assessments at age 18. Results for social (SS) and functional (FS) severity are reported in Equations 6 and 7, respectively, where the covariates are year-of--diagnosis (YOD), age-at-diagnosis (AAD), female (F), and born in Israel (BII) and Arab, and p values are reported in parentheses:
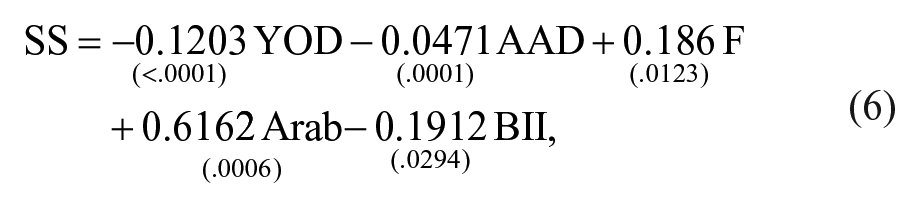
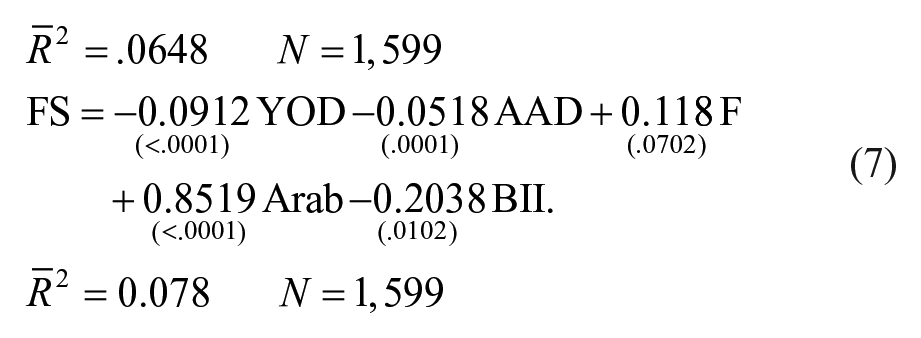
Both regression models confirm that severity assessments varied inversely with year-of-diagnosis. They imply that over 20 years, social severity assessments decreased by 2.4 points out of 5, and functional severity assessments decreased by 1.824 points. These decreases were very large and highly statistically significant. Apart from this, ASD was more severe among women (Sumi et al., 2006) and Arabs, and less severe among those born in Israel, and, as expected, was slightly lower for those diagnosed when older. A unit decrease in severity scores raised employment rates by 16% in the case of functional severity and by 7.2% in the case of social severity.
Earnings
For the 349 study group members who worked, we estimated an unbalanced panel regression with fixed effects to quantify the return to labor market experience for the study group, where experience is defined as the number of months worked (Supplementary Material 6). The fixed effects control for measured and unmeasured differences between members of the study group, including severity, ability, education, birth cohort, and selectivity.
The regression model is
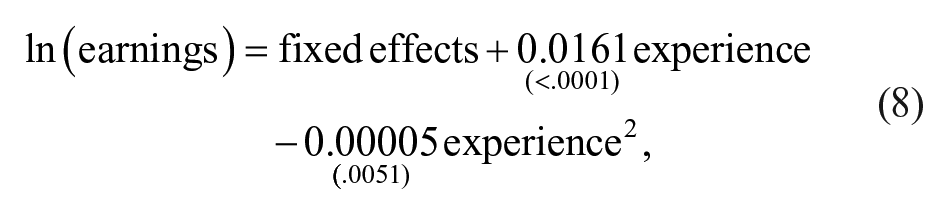
with p values reported below their parameters and adjusted R2 = .81. Both terms in experience were statistically significant, and the negative coefficient on the square of experience means that the effect of experience on earnings was convergent. The return to a month’s experience was initially 1.6% falling to 1% after 5 years and to 0.5% after 10 years.
Discussion
Three outcomes were used to study the transition into young adulthood by individuals with ASDs in Israel: civic volunteering, tertiary education, and employment. Although the majority (62% of males and 67% of females) did not engage in any of these outcomes, a substantial minority were engaged in one or more. Almost 30% were engaged in regular (unsheltered) employment.
Our results, which are informed by longitudinal population cohort data, tend to support the social-functional model of transition rather than the traditional sequential model in several respects. First, sequencing does not imply causality. Although earlier milestones such as civic volunteering precedes subsequent ones such as tertiary education, this does not mean that civic volunteering helped individuals with ASD to enter the regular labor market through schooling. Indeed, statistical tests clearly reject this causal pathway. Instead, sequencing is induced by self-selection; more capable individuals happen to engage in both earlier and later milestones. Second, the correlations between these outcomes are small. This means that just because someone does not participate in one outcome does not mean that he or she will not participate in another. For example, failure to participate in civic volunteering and tertiary education does not mean that the individuals concerned are less likely to enter the regular labor market. Consequently, we do not think that the classification of young adults with ASD into “high” or “low” functioning is helpful. Third, “functional severity” measured at age 18 predicts all three outcomes, and “social severity” predicts two (tertiary education and civic volunteering), regardless of their sequencing. This result is consistent with the social-functional model.
These results conflict with longitudinal studies, which typically find that measures of adult adaptive functioning serve as better predictors of outcomes than do measures of social communication abilities and skills (Gillespie-Lynch et al., 2012; Howlin et al., 2000; Szatmari et al., 2009). One reason for this difference may be that measures of functional severity are less subjective than measures of social severity (Magiati et al., 2014). Another is that adaptive functioning among children higher up the spectrum tends to improve with the transition into adolescence and adulthood more than do communication and social abilities (Gillespie-Lynch et al., 2012; Szatmari et al., 2009).
Our results show that what matters is the immediate family environment, as represented by parents’ income, although these effects are small. The children of Arab families are more likely to engage in tertiary education and spend more time in employment than the children of Jewish families. The children of ultra-orthodox families are less likely to engage in civic volunteering, but if they do, they volunteer for longer. Also, they are less likely to have been employed and work less otherwise. These results suggest that social capital in terms of family capacity and social networks (Anderson et al., 2018) matters for some but not all outcomes. On the contrary, the fact that outcomes do not depend on the SES of locations suggests that social capital beyond the family does not seem to be important. The same applies to the finding that peripheral status of locations does not matter. The transition into adulthood is the same for people with ASD raised in Tel Aviv where SES is high as it is in Jerusalem where SES is low, and it is the same in Tel Aviv where services are plentiful as it is in the periphery where they are not. These results do not conform to the expectations of Anderson et al. (2018).
The earnings of workers with ASD increase more rapidly with their employment experience than they do for the general population (Ehrenberg & Smith, 2016). These returns are 4 times larger than for the general population in Israel (Dahan, 2001), implying that although the earnings of workers with ASD are initially low, the gap with respect to the general population narrows over time but does not close. Our results suggest that because employers expect the productivity of workers with ASD to be low, their wages are initially low. Subsequently, their rapid wage growth results from employers’ realization that, on average, the productivity of workers with ASD is higher than initially expected.
Complete stratification arises when the probability of participating in an outcome is independent of the intensity of participation, measured by its duration. In this case, the population that participates and the population that does not do not overlap. Complete stratification arises between the never-employed and ever-employed because the duration of employment is independent of the probability of employment. Hence, the ever-employed and the never-employed constitute non-overlapping populations. Incomplete, or negative, stratification arises in civic participation and tertiary education, where we find that individuals more likely to participate do so for less time. This suggests that participants overestimate their ability to persist in the activity, or that less able children are pushed into activities beyond their ability.
This study has several implications for policy regarding the transition of individuals with ASD into young adulthood. Just because there is no causal effect of civic engagement on subsequent outcomes such as studies does not mean that the policy to encourage civic engagement is not justified. Civic engagement may improve the quality of life and is justified in its own right regardless of the implications for employment. In this context, negative stratification in civic volunteering and tertiary education suggests that participants need help in remaining engaged in these activities. Complete stratification in employment implies that programs based on the experience of the employed aimed at increasing the employment prospects of the non-employed are unlikely to be successful, because the never-employed and ever-employed constitute separate populations.
Our results are relevant to recent attempts to estimate the economic burden of ASD (Buescher et al., 2014; Leigh & Du, 2015). The growing prevalence of ASD implies that the economic burden is likely to increase in the future. This would be true if the degree of disability among the population with ASD remained stable. However, we find that severity assessments at age 18 years varied inversely with year-of-diagnosis, suggesting that diagnostic criteria have broadened over time. This implies that the prospective economic burden is likely to decrease, and that employment rates among young adults with ASD are likely to be greater in the future than they have been in the past.
Limitations
Because the study is limited to young adults in their 20s, it may be too early for forming judgments about their transition into mature adulthood. Data deficiencies include whether individuals attended special or regular schools, their residential status after age 18, including hostels and sheltered accommodation, and their participation in protected employment. Finally, the statistical methodology that we used assumes that what we do not observe about selection into an outcome, and its intensity have bivariate normal distributions. Although the normal distribution enjoys a central place in hypothesis testing, our results might be sensitive to alternative parametric assumptions.
Supplemental Material
JDPS_Pinto_et_al_Supplementary_Material – Supplemental material for Transition Into Adulthood With Autism Spectrum Disorders: A Longitudinal Population Cohort Study of Socioeconomic Outcomes
Supplemental material, JDPS_Pinto_et_al_Supplementary_Material for Transition Into Adulthood With Autism Spectrum Disorders: A Longitudinal Population Cohort Study of Socioeconomic Outcomes by Michael Beenstock, Ofir Pinto and Arie Rimmerman in Journal of Disability Policy Studies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available on the Journal of Disability Policy Studies website along with the online version of the issue.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.