
Abstract
Research has identified higher rates of mental disorders among former child welfare youth and youth experiencing homelessness when compared with their peers in the general population. Given the growing number of campus support programs serving these youth, research should focus on students in these programs to understand whether mental health problems interfere with these students’ receipt of program services, which can lead to unsatisfactory academic performance. This study collected both quantitative and qualitative data from students in a campus support program to examine the prevalence of mental disorders, mental health service use, receipt of program services, students’ grade point average, and their perceptions of obstacles and motivations to academic success. Implications for social work research and practice are discussed.
Keywords
Introduction
For many people, finishing college is an important step toward a successful life. This is also true for former foster youth and youth experiencing homelessness who are enrolled in college. Yet former foster youth and youth experiencing homelessness often face multiple obstacles to college success. One such obstacle is mental health problems (Day, Riebschleger, Dworsky, Damashek, & Fogarty, 2012; Morones, 2013; Pecora, 2012; Unrau, Font, & Rawls, 2012). In this study, we focused on former child welfare youth and youth experiencing homelessness who participated in a campus support program to examine whether mental health problems interfered with their receipt of services from the campus support program, and compromised their grade point average (GPA). We also examined their perceptions of support and obstacles that influence college success.
Mental Health Among Former Foster Youth and Youth Experiencing Homelessness in College
The most common mental health problems among former foster youth are depression, anxiety, and posttraumatic stress disorder (PTSD; Courtney, Terao, & Bost, 2004; Havlicek, Garcia, & Smith, 2013; Salazar, 2012; Salazar, Jones, Emerson, & Mucha, 2016; White, Holmes, O’Brien, & Pecora, 2005). Previous literature reported 6% to 8% incidence of PTSD among former foster youth who had recently exited foster care (Courtney et al., 2005; Courtney et al., 2004; Havalchak, White, & O’Brien, 2008; McMillen et al., 2005). Similarly, many students experiencing homelessness reported mental health problems (National Center for Homeless Education [NCHE], 2015). In their study of 24,537 students from 23 campus of California State University, Crutchfield and Maguire (2018) reported that students with food and housing insecurity reported high levels of personal concerns indicated by anxiety, fear, irritability, and depression. Hallett and Crutchfield (2017) suggested that housing insecurity is a form of trauma that can negatively affect a student’s ability to engage in academic and social activities, as well as his or her mental and physical health.
Studies have also indicated that there is significant overlap between populations of former foster youth and youth experiencing homelessness (Courtney et al., 2007; Wong, 2008). According to results from the Midwest Evaluation of the Adult Functioning of Former Foster Youth (Midwest Study) of 624 youth from Iowa, Wisconsin, and Illinois, 31% to 46% experienced homelessness at least once by age 26 (Dworsky, Napolitano, & Courtney, 2013). A report from the National Health Care for the Homeless Council (2015) indicated that young adults experiencing homelessness are as high as 4 times more likely to have at least one psychiatric disorder, such as depression, anxiety, and PTSD, compared with their peers in the general population.
The literature consistently reports that mental health challenges can interfere with school performance of former foster youth and youth experiencing homelessness. Among former foster youth in college, mental health problems increase the likelihood of poor academic progress, poor retention rates, and low graduation rates (Day et al., 2012; Dworsky & Pérez, 2010; Emerson, Duffield, Salazar, & Unrau, 2012; Hernandez & Naccarato, 2010; Pecora, 2012; Salazar, 2012). Generally, former foster youth and youth experiencing homelessness become vulnerable to mental health problems and poor educational outcomes because of instability and exposure to family dysfunction, especially during their childhood. For instance, foster youth and youth experiencing homelessness experience frequent changes in living arrangements, recurrent school changes and missed school days, economic struggles, and family dysfunction such as parental substance abuse (Day, Dworsky, & Feng, 2013; Edidin, Ganim, Hunter, & Karnik, 2012; National Working Group on Foster Care and Education, 2014; Pecora, 2012). Moreover, as reported in a study by Geenen et al. (2015), low expectations from child welfare and school professionals limit preparedness for college among foster care youth with mental health challenges. Geenen et al. (2015) added that foster youth are reluctant to disclose mental health struggles and seek help due to fear of stigmatization and discrimination, thus increasing their vulnerability to poor educational outcomes.
Mental Health–Related Services
Studies have reported that use of mental health services decreases among foster youth as they age out of the child welfare system (Courtney et al., 2011; Courtney et al., 2007; McMillen & Raghavan, 2009). For example, in their Midwest Study, Dworsky and Courtney (2009) reported a significant decline in usage of mental health services across different treatment types, such as outpatient and inpatient therapy, as youth get older. In Missouri, McMillen conducted two studies comparing foster youth’s mental health service use at ages 17 and 19. Studying a sample of 149 youth aged 17 who experienced a psychiatric disorder in the preceding year, McMillen et al. (2004) reported that 136 (91%) received a mental health service during that year and 120 (81%) were receiving a mental health service at the time of the study. In their follow-up study (McMillen & Raghavan, 2009), the authors reported that the use of mental health services decreased from age 17 to age 19. The use of mental health services is especially low among the 19-year-old youth who had been discharged from the foster care system. Over 60% of the discharged youth chose to stop taking psychotropic medications that had been prescribed to them. Some former foster youth in college gain access to mental health services through services provided by their university and/or college. Merdinger, Hines, Osterling, and Wyatt (2005) examined the mental health service utilization of 216 emancipated foster youth attending a 4-year university and reported that over one third of the sample received mental health services, including therapy or counseling (31%), outpatient (10.2%), and inpatient services (6.9%).
So far, studies on college students experiencing homelessness are still limited (Gupton, 2017; Hallett & Crutchfield, 2017). The few studies on college students experiencing homelessness assessed their use of services in general, but did not focus on their use of mental health services (Goldrick-Rab, Richardson, Schneider, Hernandez, & Cady, 2018; Gupton, 2017). Analyzing personal narratives of four community college students in LA experiencing homelessness, Gupton (2017) reported that these students rarely sought out services from their academic institutions. Goldrick-Rab and colleagues (2018) conducted a national survey of 43,000 college students and reported that 9% of them were homeless within the preceding year but only small proportions of students experiencing homelessness (8% among 2-year and 5% among 4-year college students experiencing homelessness) received housing assistance.
In the past two decades, support programs for underserved populations have emerged on college campuses (Dworsky & Pérez, 2009; NCHE, 2015). Several college support programs include a mental health service component for former foster youth and youth experiencing homelessness. For example, students experiencing homelessness at Florida State University, Kennessaw State University, and the University of Massachusetts in Boston have access to a wide array of mental health services including workshops and individual and group counseling focused on depression, anxiety, low self-esteem, crisis intervention, eating disorders, and suicidal thoughts and behaviors (NCHE, 2015). When the availability of on campus mental health services is limited, campus support programs such as the Guardian Scholars programs refer former foster youth to community mental health providers (Ball State University, 2007).
In addition, precollege programs have been developed to address mental health problems in students prior to college attendance. For example, Geenen et al. (2015) examined the Better Future Project, which was a program designed to prepare and help foster care youth with serious mental health problems access postsecondary education. Randomly assigning participants to intervention and control groups, the authors reported that, at the end of the intervention, youth in the intervention group rated higher on postsecondary participation, postsecondary and transition preparation, hope, self-determination, and mental health empowerment than their peers in the control group. Moreover, youth in the intervention group continued to improve in the areas of mental health recovery, quality of life, and high school completion at 10 months and 16 months after enrollment in the intervention.
Current Study
Most of previous studies on former foster youth and youth experiencing homelessness examined mental health among the general populations of both groups of youth. Only a few of these studies focused on the former foster youth and youth experiencing homelessness in college (Merdinger et al., 2005; Salazar, 2012; Salazar et al., 2016). Moreover, no study has focused on former foster youth and youth experiencing homelessness who participate in campus support programs. It is important to understand whether mental health problems interfere with their receipt of services from campus support programs, which can lead to unsatisfactory academic performance. This study aims to address this knowledge gap. This study collected both quantitative and qualitative data from participants in a campus support program to address six research questions:
Method
Design
We used a mixed-method design, with qualitative and quantitative methods used equally and in parallel (Creswell, Plano Clark, Gutmann, & Hanson, 2003). We used quantitative methods to address Research Questions 1 to 4 and qualitative methods to address Questions 5 and 6.
Study Site
This study focused on a campus support program at Florida International University (FIU) in the Miami metropolitan area of Florida. The university has a student population of nearly 54,000, including 61% Hispanic, 15% White non-Hispanic, 13% Black, 4% Asian or Pacific Islander, and 7% other minority groups. Most students at FIU are from the local community; over half of the undergraduates are first-generation college students and many of them are nontraditional students working at one job or more to support themselves while going to school. In the 2013 fall semester, FIU established its campus support program to serve students from three background types: former foster youth, adoptees from the Florida State Department of Children and Families (DCF), and youth experiencing homelessness. FIU identifies eligible students through tuition waiver records in their administrative data. On the records, the waiver for adoptees is recorded as “Adoptees from Department of Children & Families,” the waiver for former foster youth is recorded as “Road-to-Independence Scholarship,” which was provided to former foster youth, and the waiver for students experiencing homelessness is recorded as “homeless.”
Following Florida Statute 1009.25(1)(c) and (d), students who are adoptees from DCF and former foster youth need to contact the local child welfare agency to verify their background and get the tuition waiver form and submit it to the campus support program (FIU, 2019a). Unlike adoptees from DCF and former foster youth, a student experiencing homelessness receives a homeless tuition exemption through an application process that requires showing proof of homelessness during enrollment (FIU, 2019c). The campus support program has an intake process to screen individuals who may be referred to the program or who may refer themselves because they believe they are eligible for the exemption. Following Florida Statute 1009.25(1)(f), applying for the homeless tuition exemption requires documentation in the form of a letter from a publicly or privately operated homeless shelter, food/clothing bank, and/or transitional ministry, as an official proof of homelessness. If a student provides preliminary evidences of experiencing homelessness but does not have an official proof, the student will be directed by the campus support program to call the county’s Homeless Helpline, which links them to immediate services and assists them in acquiring the proof of homelessness.
When the program started in the fall semester of 2013, FIU identified over 40 former child welfare youth and youth experiencing homelessness. Since then, the number of eligible students has grown significantly. As shown in Table 1, in spring of 2016, FIU identified 141 eligible students: 56 former foster youth, 45 adoptees from DCF, and 40 students experiencing homelessness. Program staff are called “success coaches” and provide case management and advising services to students in the program. Our earlier publication (Huang, Fernandez, Rhoden, & Joseph, 2018) examined program staff’s and mentors’ perceptions of the elements and impacts of the program. The program provides financial support, academic services, referral services, and emotional support. Financial support includes scholarships, on campus housing voucher, and book voucher. All forms of financial support are competitive, and are selected based on students’ engagement with the program and their academic performance. Academic services include intensive monitoring of students on academic probation and organizing monthly workshops on academic-related topics. Referral services are provided to students in needs of other services (e.g., tutoring, counseling) inside and/or outside the university. Emotional support is provided through one-on-one meetings with the success coach and mentors, and social events involving students, mentors, and success coaches.
The study was funded by a competitive research grant from the university and was approved by the University Institutional Research Board (IRB).
Bivariate Analysis to Compare Respondents and Nonrespondents.

Note. DCF = Department of Children and Families; GPA = grade point average.
Quantitative Method
Data
This study used quantitative data from two sources: university administrative data and survey data. The university provided us with administrative data for all of the 141 students eligible for the campus support program in 2016 spring semester. The university administrative data contained information on student demographics, major, and high school and college GPAs. We also collected survey data. The survey was adapted from a previously published survey on campus support programs (Dworsky & Pérez, 2010). Survey questions asked about respondents’ educational histories and current performance, their experiences with the campus support program, past and current mental health diagnoses, and experiences with child welfare and homelessness. A copy of our survey is available from the first author upon request. The two sets of data (administrative data and survey data) were linked using student identification numbers.
Study sample
We invited all 141 eligible students to participate in the survey through emails and phone calls. On average, each student received two emails and four calls from the authors. As a result, 56 students completed the survey, which resulted in a response rate of 40%. Each participant received an incentive of US$20 cash.
Of the 56 students who completed the survey, one could not be matched with the university administrative data, and five others did not participate in the campus support program. The remaining 50 students comprise the study sample. We examined whether the 50 students in the study sample are representative of all 141 students eligible for the campus support program by comparing the 50 respondents and the 91 nonrespondents on characteristics including age at the time of entering the university, gender, ethnicity, high school GPA, and experiences with child welfare and homelessness. For the comparisons, we used t-test statistics for numerical variables and chi-square statistics for categorical variables. Age at the time of entering the university, which was included in the analysis as a report from the National Center for Education Statistics (Snyder, de Brey, & Dillow, 2018), showed that entering the university at a younger age is associated with higher retention rates. As shown in Table 1, the two groups of students did not have statistically significant differences on any of these characteristics, suggesting that the study sample is representative of all eligible students.
Data preparation and analysis
We used quantitative data to answer Research Questions 1 to 4. To answer Research Questions 1 and 2, we used descriptive analyses (frequencies) to present the prevalence of self-reported mental disorder diagnoses and, among the ones with mental disorders, the rates of mental health services use. The third research question examines the relationship between mental disorders and the receipt of services from the campus support program. As both mental disorders and receipt of services from the campus support program are binary variables, chi-square statistics were used to test their relationship (Field, 2017). The fourth research question examines the relationship between mental disorders and GPA. As mental disorders are binary variables while GPA is a numerical variable, t-test statistics were used to test their relationship (Field, 2017). All analyses were conducted on IBM SPSS Statistical Software.
Qualitative Method
Participants
Survey participants were recruited to participate in the in-depth interviews. At the end of each survey, we asked the participant if he or she would be willing to meet with the first author for an individual interview. In total, 17 students participated in the interviews.
Procedures
The authors used structured guidelines for the interviews with the former child welfare youth and youth experiencing homelessness. The guidelines covered four areas: the interviewees’ perceptions of support and obstacles to succeeding in college, their experiences of transitioning into college, their understanding and utilization of services provided by the campus support program, and their experiences with child welfare and homelessness. We followed the guidelines closely in the interviews. A copy of our guidelines is available from the first author upon request. Each interview, approximately 1 hour in duration, was audio-recorded with the participants’ consent and was transcribed verbatim. To answer Research Questions 5 and 6, we used qualitative data from the interviewees’ responses on their perceptions of support and obstacles to succeeding in college.
Analysis
The authors used a conventional thematic content analysis to analyze the data (Braun & Clarke, 2006). The first author read all transcriptions and developed a preliminary codebook structured in a way consistent with the interview guidelines. The other three authors coded the transcriptions using the codebook. Each transcription was coded by two authors. Discrepancies occurred only occasionally. Most discrepancies pertained to whether to add new codes or apply existing codes. To resolve discrepancies, all four authors met to review the related transcription and decide collectively. At the end of the coding stage, all four authors met to merge similar individual codes into common themes. All coding and analyses were conducted using NVivo 11.
Results
Prevalence of Self-Reported Mental Disorder Diagnoses
Among the 50 participants, 15 (30%) reported currently having at least one diagnosis of mental disorders. As shown in Table 2, the four most prevalent current diagnoses were depressive disorder (16%), attention deficit hyperactivity disorder (ADHD; 14%), PTSD (8%), and anxiety disorder (8%). We also examined whether the prevalence of mental disorders varied with students’ backgrounds (homeless, former foster youth, and adoptees from the child welfare system) and found no statistically significant differences.
Prevalence of Mental Disorder Diagnoses.

Note. PTSD = posttraumatic stress disorder.
Prevalence of Mental Health Services Use
Among the 15 participants currently with diagnoses of mental disorders, nine of them (60%) reported currently receiving mental health services. Among these nine students, six reported receiving psychotropic medications, seven reported receiving individual counseling, and one reported receiving group counseling (each individual can receive one or more types of services). Family counseling was not used by students with any diagnosis. The rates of mental health service use were high among the participants with any of the four most prevalent diagnoses: 75% among the participants with depressive disorders, 57% among the participants with ADHD, 75% among the participants with PTSD, and 100% among the participants with anxiety disorders. Among the nine students receiving services, six (67%) reported substantial progress, five (56%) reported they were very satisfied, two (22%) were somewhat satisfied, one (11%) was somewhat unsatisfied, and one (11%) was very unsatisfied.
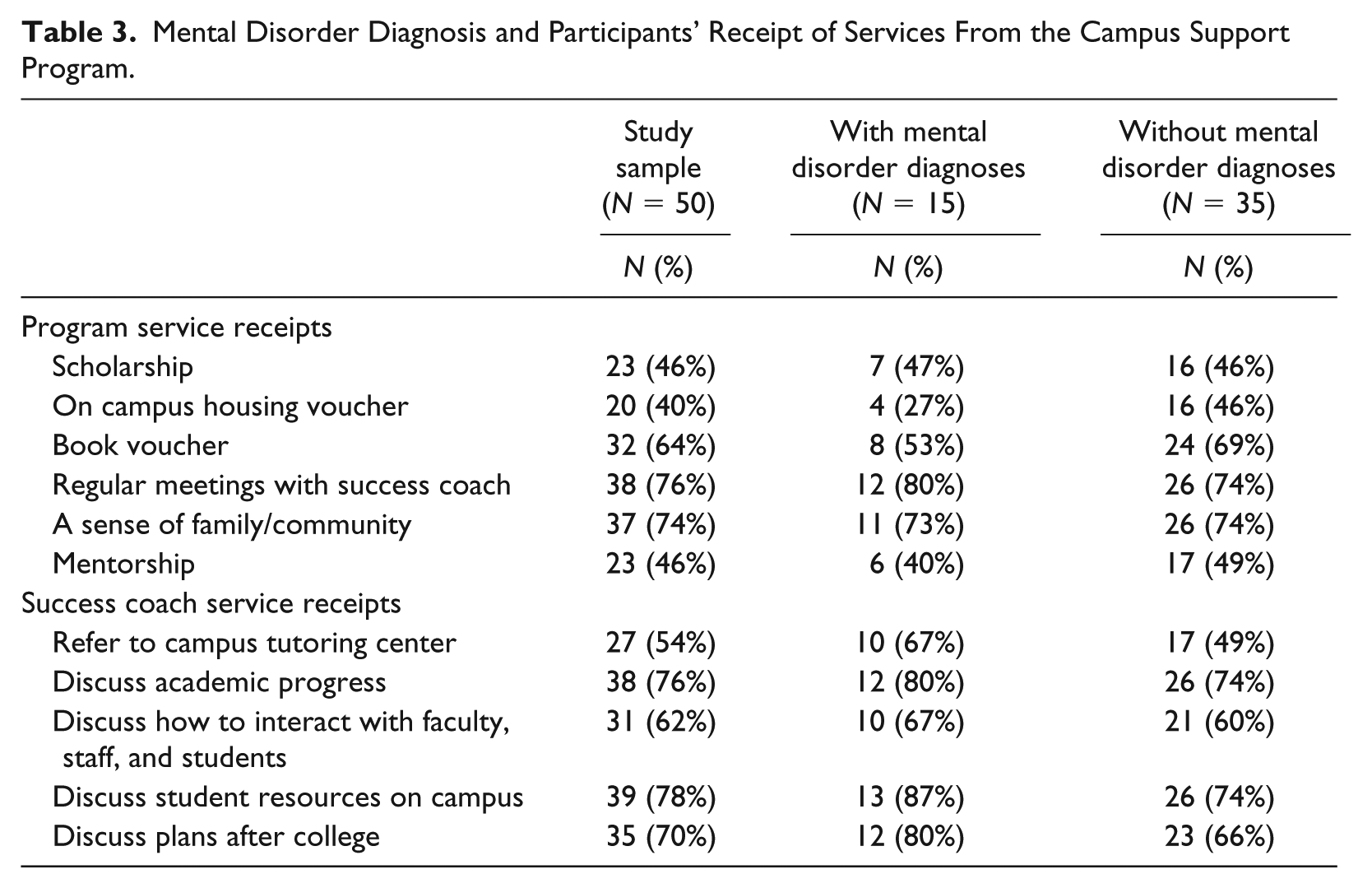
Mental Disorder Diagnoses and Receipt of Services From the Campus Support Program
We examined the relationship between self-reported mental disorder diagnoses and participants’ receipt of services from the campus support program and the success coach. The results from chi-square statistics did not show a statistically significant relationship between mental disorder diagnoses and receipt of services. Participants both with and without diagnoses reported high rates of services receipt. Forty-six percent of the study sample were awarded a scholarship offered by the campus support program, 40% received housing vouchers to stay in the campus dorm, 64% received book vouchers, 76% had regular meetings with the success coach, 74% felt a sense of family and community through participating in the program, and 46% had a mentor matched by the campus support program. Regarding the services provided by the success coach, 54% were often referred to the campus tutoring center by the success coach; 76% often discussed academic programs with the success coach; 62% often discussed with the success coach about how to interact with faculty, staff, and students on campus; 78% often discussed student resources on campus with the success coach; and 70% often discussed future plans (e.g., applying for jobs and graduate school) with the success coach (Table 3).
Mental Disorder Diagnosis and Participants’ Receipt of Services From the Campus Support Program.
Mental Disorder Diagnosis and GPA
The average GPA of the 50 participants in our sample was 2.74 (SD = .75). As shown in Table 4, we did not find a statistically significant relationship between participants’ self-reported mental disorder diagnoses in general, nor ADHD, PTSD, anxiety disorders, and depressive disorders in particular and GPA.
Mental Disorder Diagnosis and GPA (N = 50).

Note. GPA = grade point average; ADHD = attention deficit hyperactivity disorder; PTSD = posttraumatic stress disorder.
Obstacles for Former Child Welfare Youth and Youth Experiencing Homelessness in College
Qualitative data showed that former child welfare youth and youth experiencing homelessness face a number of obstacles to succeed in college. Many of them had to work jobs while in college to support themselves as they received little or no financial support from their family. Some of them even provided financial support to their family members, who often struggled financially and had limited employment prospects for a variety of reasons, such as limited education, physical and mental illness, and criminal history. Working jobs while in school and dealing with dysfunctional families were commonly cited as major sources of stress that made it difficult for students to focus on academics. One participant shared that he had to work to support his family who struggled to meet basic needs: Interviewee: Money. I have to earn money for myself and my family, basically my brother and my mom. My mom especially reaches a point where she can’t work. My brother and I have to work to support her daily financial needs . . . We went to a free clinic. The most they can do is just the physical. They said, “You really need a specialist.” But for that you need to pay. Even with Obamacare, there is co-pay. It’s very difficult because my brother and I, combined, we don’t earn 1,000 dollars per month. We have everything in a storage and we have to pay for car insurance, food, gas and all those expenses, though we don’t live in a home. That’s basically it. It’s all we can cover.
Another student reflected that having to balance work and school responsibilities is a struggle that directly affects his ability to perform well academically: Interviewee: I normally don’t go to sleep any earlier than 5:30 in the morning. I work Monday through Thursday. Friday is the day that I get to really catch up with my classes. With assignments due on Wednesday and Thursday I am up super late trying to complete them. Sometimes I miss assignments due mainly to fatigue, as sometimes I don’t get home from work until 10 pm.
Several students reported being negatively affected by dysfunctional family members who they remain in contact with even after being removed from the home, due to emotional attachment.
Interviewee: I say my mom, she has a lot of issues. She has mental health issues . . . My mom would always be angry. I would always have to be scared that she would take that out on me, that she would take that out on my brother, and that I would have to, you know, do something about it. It was just not an environment that I was able to let down my defenses, down enough, you know, and really focus on anything else.
In summary, former child welfare youth and youth experiencing homelessness reported working jobs while in school and dealing with dysfunctional families as obstacles to succeeding in college.
Motivations for Former Child Welfare Youth and Youth Experiencing Homelessness to Focus on Academics in College
Qualitative data highlighted three sources of motivation keeping participants focused on academics. First, students overwhelmingly reported wanting to improve their lives and the lives of their families through achieving success in college. Most participants did not have financial security in their earlier life. Through getting a college degree, they wanted to have a career that can provide them a sense of self-value and financial security. They believe that achieving financial security will allow them to provide more resources to their family.
Interviewer: What are the things that help you to stay in school? Interviewee: I guess I just want to be somebody, like I don’t want to . . . I don’t want to struggle. Like I had to struggle. If I were to have a family or something, I don’t want them to struggle like I had to struggle and like basically I don’t want to be nobody. I want to have a career. I want to have a job, somewhere to lay my head that I can call my own. I don’t want to have to depend on people. I want to be able to depend on myself. I don’t want to have them to worry about having a job at 14 or 15, trying to paying all the bills. Or like not having because you don’t have the money or I didn’t have the money so I want to be able to do stuff. I don’t know, peace of mind.
Second, participants reported that staff and mentors of the campus support program motivated them to stay focused by using both a strength-based approach and close monitoring. Several participants reported regularly meeting the program staff and their mentors. In the meetings, they discuss academic progress and other topics, and felt encouraged to stay focused on their academic goals, especially at the time when they had self-doubts about their ability to succeed in college. They also learned about study strategies (e.g., time management) and academic resources (e.g., tutoring services) from the program staff and their mentors.
Interviewer: What do they [the staff of the campus support program] expect from you? Interviewee: Well, I feel there are not even expectations, but more they want you to succeed. Like they didn’t try to pressure me into, “Oh you failed so you have to do this this and that.” They were like you failed, but let’s see what you can do to improve. They didn’t make it seem like you have to do this or you have to do that. They made it seems like we want you to do this. You should want to do this for yourself. . . . I guess that’s the point of the program to have somebody to talk to and have somebody to be on your side when you feel like nobody else is on your side.
Third, participants frequently identified support from positive peers and other adults outside of the university as sources of motivation. Several participants reported participating in student associations, where they engaged in positive activities and met positive peers. In socializing with positive peers, they developed self-expectations similar to their peers. Some participants also reported receiving mentorship from mentors outside of the university, such as mentors whom they met through other community service agencies. Similar to staff and mentors of the campus support program, these mentors kept track of their progress in college in general and provided advice on study strategies and life skills in general (e.g., budgeting skills).
Interviewer: What external or environmental characteristics increase your chance to succeed in college? Interviewee: Peer support. I have a lot of friends from other universities and campuses. We kind of support each other. I am also part of the [student organization], which is an organization where you fundraise on a social issue in another country or city . . . There is a lot of support there. I am very friendship-oriented.
In summary, former child welfare youth and youth experiencing homelessness identified three sources of motivation to focus on academics: their desire for a better life, support from staff and mentors of the campus support program, and positive peers on campus and supportive adults outside of the university.
Discussion
Mental Disorder Diagnoses
We compared the prevalence of mental disorder diagnoses among our study sample with college students in general and found that the prevalence of mental disorder diagnoses was higher in our sample than among college students in general. Our study found that 16% of our sample reported depressive disorder, 8% reported PTSD, and 8% reported anxiety disorder. Using data from the 2001 to 2002 National Epidemiologic Survey on Alcohol and Related Conditions, Blanco et al. (2008) reported that of the 2,188 college students in their sample 7.04% of them had major depressive disorder and 1.64% had generalized anxiety disorder, though they did not report on the prevalence of PTSD. The result from the comparison indicates that former child welfare youth and youth experiencing homelessness had higher rates of mental disorder diagnoses than their peers in college, which is consistent with previous literature (Day et al., 2012; Morones, 2013; Pecora, 2012; Unrau et al., 2012). It is likely to be caused by their experience of trauma, such as child abuse and neglect, placement instability, and homelessness. Also, the difference may be partly attributable to differences in measurement type. We used self-reported measures of mental disorder diagnoses (i.e., asking participants to report their current diagnoses), whereas professional interviewers made diagnoses using Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV; American Psychiatric Association, 1994) criteria in Blanco et al.’s (2008) study.
As two thirds of our sample were former child welfare youth, we compared our findings with previous studies on youth aging out of foster care. Our finding is consistent with the finding from previous literature showing the higher rates of mental health diagnoses among youth with foster care experience than those in the general population (Courtney et al., 2005; Havalchak et al., 2008; McMillen et al., 2005). Our finding that depressive disorder, ADHD, PTSD, and anxiety disorder are the most common mental disorders is consistent with previous studies (Courtney et al., 2004; Salazar, 2012; Salazar et al., 2016; White, O’Brien, Pecora, & Buher, 2015). A qualitative study of 248 college graduates who were formerly in foster care reported depression, anxiety, and PTSD as the most commonly expressed mental health challenges (Salazar et al., 2016).
The prevalence of depressive disorders and PTSD are lower in our sample than among homeless youth in homeless youth–serving agencies such as shelters. Bender, Ferguson, Thompson, and Langenderfer (2014) studied a sample of 601 homeless youth (ages 18-24) from homeless youth–serving host agencies in Los Angeles, Denver, and Austin, and found that 31% and 23% of their sample had major depressive episodes and PTSD, respectively, which are higher than the 12% rate for each diagnosis among the youth experiencing homelessness in our sample. The lower rates in our sample are likely to be related to the fact that the homeless youth are attending college. That is, the homeless youth who manage to get into college tend to suffer less from mental health problems.
Utilization of Mental Health Services
We compared the rates of mental health service receipts between our sample and college students in general and found that the rates are higher in our sample than college students in general. Blanco et al. (2008) reported that in their sample, 34.1% of college students with mood disorders and 15.9% of those with anxiety disorders received mental health treatment. In our sample, on the contrary, 75% of the participants with depressive disorder, 100% of participants with anxiety disorders, and 75% of participants with PTSD received at least one type of service, including psychotropic medications, individual counseling, and group counseling. These findings are consistent with the results of the Midwest Study, which showed that former foster youth ages 23 to 24 are more likely to receive psychological or emotional counseling than their Add Health Study counterparts (11.3% vs. 6.5%; Courtney, Dworsky, Lee, & Raap, 2009). However, the Midwest Study did not compare the rates of mental health service receipt among the individuals with diagnoses. Therefore, it is unclear whether the higher rates of receiving psychological or emotional counseling for former foster youth in the Midwest Study is due to their higher rates of mental disorders or their greater access to services.
The high rate of mental health service utilization in our sample is likely attributable to two health care insurance–related policies. First, this study was conducted shortly after the passage of the Patient Protection and Affordable Care Act (ACA), which extended Medicaid coverage to individuals who aged out of foster care up to age 26 (Florida Department of Children and Families, 2016). In Florida, Medicaid covers several mental health–related services, including state mental health hospital services, statewide inpatient psychiatric program services, mental health targeted case management, and community behavioral health services (Agency for Health Care Administration, 2018). Second, the University Student Health Insurance Plan is available for all full-time students (FIU, 2019b). The plan offers comprehensive benefits such as inpatient and outpatient mental health services. Moreover, when students with the plan get health services from the Student Health Center on campus, their deductible and copays are waived. The plan offers an unlimited policy year maximum and low annual deductibles, even when students receive services off campus.
Mental Disorders, Receipt of Services From the Campus Support Program, and GPA
Our findings did not show that current mental diagnosis is associated with lower GPA among the former child welfare youth and youth experiencing homelessness in our sample, which was unexpected, as previous studies reported mental disorders are associated with college disengagement (Dworsky & Pérez, 2009; Salazar, 2012; White et al., 2005). That our findings differ from those of previous studies may be attributable to five factors. First, we used GPA as our measure of academic performance, whereas previous studies mostly used college disengagement as their measure of academic performance. Although some cases of college disengagement are caused by having a GPA below the requirements for graduation, other cases of college disengagement can be caused by non-GPA related reasons such as emotional, funding, or time restraints (Dworsky & Pérez, 2009).
Second, in our sample, the majority of participants with mental disorder diagnoses received mental health services. Unlike previous studies (Dworsky & Pérez, 2009; Salazar, 2012; White et al., 2005), this study was conducted after ACA was in effect, and the participants in this study were likely to benefit from the ACA coverage of mental health services for aging out foster youth up to age 26. The receipt of mental health services might protect students from the negative effects of mental disorders on their academic performance.
Third, in our sample, the majority of participants, including those with mental disorder diagnoses, received financial support, such as scholarship, housing vouchers, and book vouchers from the campus support program, which helps to reduce their stress. The qualitative finding showed that some participants identified working jobs while in school as a distraction from academics. To them, receiving financial support can reduce financial stress, allowing them to work fewer hours and have more time for study.
Fourth, the majority of participants, including those with reported mental disorder diagnoses, received regular advising and referral services from the success coach. The qualitative finding showed that some students felt motivated by the success coach. Some students also reported that the referrals to tutoring and mentoring services are helpful. In addition to success coaches, students found guidance from positive peers and external mentors. Fifth, participants reported a strong sense of motivation to better their lives through completing their college education. Their motivation kept them on track with their education.
Limitations and Research Implications
This study has two limitations. In this section, we acknowledge each limitation and provide research implications for addressing each of them. First, this study examined separately the relationship between mental disorder and receipt of campus support services and the relationship between mental disorders and GPA, and found neither relationship to be statistically significant. We suggested that the lack of a statistically significant relationship between mental disorder and GPA might be attributable to the buffering effects of mental health and campus support services. That is, because most former child welfare youth and youth experiencing homelessness with mental health problems receive mental health services and campus support services, they were able to cope with their mental health problems without interfering with their GPA. However, we did not test the moderation mechanism directly by including mental health and campus support services as moderators in modeling the relationship between mental health and GPA. Our small sample size provided limited statistical power to test a complicated model with moderators. Future research with greater sample sizes should examine the moderation effects directly by including mental health and campus support services as moderators in modeling academic performance on mental dis-orders. This way, the results can directly indicate the statistical significance of the hypothesized moderation effects.
Second, this study used the tuition waiver records to identify participants’ background as adoptees from DCF, former foster youth, or youth experiencing homelessness. We did not collect data to measure specific experiences within each background, such as the initial age of entering substitute care, the initial age of being adopted, the initial age of experiencing homelessness, the duration of time in substitute care, the duration of time since being adopted, and the duration of time experiencing homelessness. Without data on their specific experiences, we also were not able to identify participants with experiences with both child welfare and homelessness. It is possible that these unmeasured experiences are associated with mental health and GPA of the sample. Future research should collect data on the students’ specific experiences with child welfare and homelessness, and examine their impacts on mental health and GPA of former child welfare youth and youth experiencing homelessness in college.
Implications for Social Work Practice
The findings of our study present four implications for social work practice for campus support programs. First, campus support programs might consider obtaining information about the mental health of students in their programs. For example, at the beginning of each semester, the program staff can ask their students to self-report their mental disorder diagnoses. The program staff can also use psychometrically verified tools to screen their students for ADHD, PTSD, generalized anxiety disorder, and major depressive disorder, which are the most common mental disorders among their clients. While keeping the information confidential, the program staff can also use the information to make an individualized service plan accordingly.
Second, campus support programs can facilitate access to mental health services for students with mental disorders. The program staff may inform students of available mental health services on and off campus, especially the on campus counseling center that is typically geographically convenient for students to visit. Also, the program staff may educate students about related health care policies, such as the Medicaid coverage for former foster youth up to age 26 and the University Student Health Insurance Plan. Understanding benefits from these policies can alleviate students’ concerns regarding the cost of seeking services.
Third, campus support programs can benefit students, regardless of whether they have mental disorders. A major component of their services is financial support, such as scholarship, housing vouchers, and book vouchers. Such financial support can alleviate the need for employment while in school, which can reduce the work–life balance–related stress. When financial support is limited, program staff can establish transparent selection criteria to include measures of students’ engagement in program services, such as case management and academic services. Case management services can be critical to students with great need for services, such as those with mental health problems and/or who are on academic probation. Specifically, program staff can meet these students individually on a weekly basis to assess their attendance at various services (e.g., mental health services, tutoring, and mentoring) and their progress in the services. In addition, program staff can organize academic services that serve the common needs among students. For example, program staff can organize workshops on time management and study skills training, which can prepare students to cope with study-related stress, and indirectly prevent mental disorders.
Fourth, case managers and educational specialists in child welfare agencies can familiarize themselves with services provided by campus support programs and refer their clients to these programs. Engagement in these programs helps students gain access to financial, academic, and other resources, which can support their transition into college. Moreover, case managers, educational specialists in child welfare agencies, and staff of campus support programs can work together to support students with mental disorders. They can share with each other information on students’ support systems, their stressors, their history of mental disorder diagnoses, treatment history, and their responses to previous treatment. They can use this information to develop service plans that match students’ needs. Their teamwork can also serve as a strong support system for students coping with mental disorders. Meanwhile, it is important to establish joint agreements on protecting students’ rights to confidentiality in the process of data sharing (Darlington & Feeney, 2008). The agreements can include boundaries, priorities, and approaches for data sharing. For example, the agreements can specify what information can be shared between agencies, when it is appropriate to share information, how information can be shared, and how information can be stored by other agencies.
Conclusion
This study shows that former foster youth and youth experiencing homelessness reported higher rates of mental disorder diagnoses than college students in general, which is consistent with previous literature. In this study, foster youth and youth experiencing homelessness with mental disorder diagnoses had high rates of receiving mental health services and reported similar rates of using of services from the campus support program and similar GPAs as compared with their peers without mental disorder diagnoses. Foster youth and youth experiencing homelessness face many obstacles to focus on studying, but they also have tremendous motivation to succeed in college. Understanding the benefits of mental health services and services provided by campus support programs can help campus support programs make effective service plans to serve foster youth and youth experiencing homelessness with mental disorder diagnoses. Establishing collaborations between campus support program, mental health service providers (e.g., on-campus counseling center), and child welfare case management agencies can facilitate the implementation of service plans involving interdisciplinary approaches.
Footnotes
Disposition editor: Sondra J. Fogel
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Florida International University (the 2015 Fostering Panther Pride Research Award).