
Abstract
Although family-centered practice has been implemented nationwide in child welfare, measures for evaluating family-centered practice have not been well-established. This study aimed to evaluate the factor structure of the Family-Centered Practice Questionnaire. Confirmatory factor analyses were conducted to examine the factor structure of the Family-Centered Practice Questionnaire. The five-factor and second-order five-factor models of the revised Family-Centered Practice Questionnaire with 31 items both demonstrated adequate fit. The higher order of this scale was family-centered practice and five factors were mutual trust, shared decision-making, family as a unit, strengths-based practice, and cultural competence and sensitivity. Findings suggest that the revised Family-Centered Practice Questionnaire may be helpful to practitioners and researchers seeking to measure the implementation of family-centered practice in child welfare settings.
Since the 1960s, family-centered practice has been adapted for use in health and human services disciplines, which represents a shift in service delivery from a professional/child-centered approach to a family-centered approach (Allen & Petr, 1998; Johnson, 2000). The fundamental philosophy of the family-centered approach includes respecting family members’ rights, roles, and abilities in family-related issues; thus, this approach treats the family as a service unit, respecting the family’s culture and valuing the family’s strengths and input (Allen & Petr, 1998).
In child welfare, the family-centered practice framework is informed by the Adoption Assistance and Child Welfare Act of 1980 and the Adoption and Safe Families Act of 1997 (Allen & Petr, 1998; Nelson et al., 1990). The Adoption Assistance and Child Welfare Act of 1980 required child welfare agencies to make efforts to provide services to families and to keep children safe in a stable home (Child Welfare Information Gateway, n.d.). The Adoption and Safe Families Act of 1997 further emphasized the use of kinship care to preserve families (Child and Family Services Review, n.d.). In 2018, the Family First Prevention Services Act was signed into law, which also pointed to the importance of providing in-home services to families and keeping children safe at home (Children’s Defense Fund, 2018). These legislative acts have continuously guided the implementation of family-centered practice in child welfare across the United States.
Family-centered practice models have been implemented across the child welfare service continuum, including child maltreatment prevention and intervention, preserving families, and promoting permanency (Child Welfare Information Gateway, n.d.). Family Group Decision Making (FGDM), Kinship Navigator programs, and Family Connections programs are some well-known family practice models (O’Reilly et al., 2010; Rushovich et al., 2017; Xu et al., 2017). The FGDM can be used in any stage of child welfare services to engage family members, which aims to engage family members by focusing on the shared decision-making process between family members and professionals (Asscher et al., 2014; Levine, 2000). The Kinship Navigator program is another family-centered practice model linking kinship caregivers with resources and services in the community to keep children safe at home (Rushovich et al., 2017). The Family Connections program provides community- and family-based services to families at risk for child maltreatment (DePanfilis & Dubowitz, 2005).
Implementing and measuring family-centered practices are important because children’s safety, permanency, and well-being outcomes are more easily achieved when there is corporative spirit of joint responsibilities between families and the child welfare agency. To facilitate shared resources and responsibilities, an essential step is to respect the culture of the family, acknowledge family strengths, and involve family members in the decision-making process. Emerging research has shown that implementing family-centered practice increases family’s satisfaction with services (Ahn et al., 2018), helps fulfill children and families’ short-term goals (Xu et al., 2017), and prevents child maltreatment (DePanfilis & Dubowitz, 2005). Although family-centered practice has been widely implemented in the United States, there is a lack of valid and reliable measures to capture child welfare workers’ family-centered practices. Without a measure evaluating family-centered practice in child welfare, it is challenging to examine child welfare workers’ implementation of family-centered practice and its associations with families and children’s short-term and long-term outcomes.
Theoretical and Conceptual Frameworks of Family-Centered Practice
Because achieving permanency in child welfare practice is a goal of family-centered practice, there is an emphasis on the role of family and the importance of a stable environment (Pecora et al., 2000). The theories of family-centered practice evolved out of services for children and families and include ecological theory, family systems theory, social development model, and strengths-based perspective theory (Pecora et al., 2000; Thomlison, 2008). Drawing from these theories, some researchers have proposed key components of family-centered practice. Across different frameworks, family-centered practice comprised common themes, such as treating the whole family as a unit, strengths-based perspectives, shared decision-making processes, mutual and trust relationships between professionals and families, and sensitive to families’ cultures (Allen & Petr, 1998; Child Welfare Information Gateway, n.d.; Epley et al., 2010). More specifically, Allen and Petr (1998) highlighted three elements: treating the family as a service unit, respecting family choice, and having a family strengths-based perspective. Epley and colleagues (2010) proposed five similar components of family-centered practice, including serving the family as the unit, respecting family choice, incorporating family strengths, building a mutual family–professional relationship, and providing individualized family services.
In summary, family-centered practice is a general concept implemented through respect for the family’s decisions based on family members’ strengths, providing culturally responsive services to the whole family and building mutual trust and respectful relationships between family members and professionals.
Measures of Family-Centered Practice
Some family-centered practice instruments have been used to capture family-centered practice in children and families service settings, but not specifically in child welfare settings. For example, McWilliam and Winton’s (1990) family-centered service self-assessment tool was developed for pediatric health professionals in a medical setting. Also, McWilliam and Winton’s (1990) measure was limited to newly diagnosed infants and toddlers with foci on health care professionals’ understanding of program policies and direct medical services. The other family-centered practice self-assessment tool (Murphy et al., 1995) with reliabilities ranging from .73 to .84 was designated for children with disabilities up to 5 years old and their families. Different from children and family members who seek social services in health care settings, children and families who are involved in the child welfare system may be involuntary clients and are strongly resistant to engaging in social services (Platt, 2012). Also, the child’s age in the child welfare system ranges from 0 to 21 years, which is broader than the scope of two previous measures. Furthermore, child welfare systems face unique structural challenges, such as high turnover, lack of quality training, court mandates and consent decrees, and building partnerships across multiple agencies, all of which impact family-centered practice (Aiken et al., 2015; Maher et al., 2009). Given differences in characteristics of children and families and the workforce between child welfare settings and other medical/social services settings, having a reliable and valid instrument that captures family-centered practices in child welfare is needed to promote child well-being and foster workforce development.
The Family-Centered Practice Questionnaire was developed by Craft-Rosenberg et al. (2006) using multidisciplinary health care practitioners, including nurses and social workers, who served children in a Midwest state. However, this measure has been rarely used or tested in child welfare settings. Craft-Rosenberg et al. (2006) developed and explored prior factor structures of the Family-Centered Practice Questionnaire by conducting a principal components analysis. It has 39 items measuring seven factors, including mutual trust (13 items), shared decision-making (five items), reciprocal relationships (four items), facilitation of family participation in service (seven items), strengths-based practice (four items), interdisciplinary teamwork (three items), and cultural competence and sensitivity (three items). A complete list of 39 items with seven factors are presented in Table 4. Furthermore, Craft-Rosenberg and colleagues (2006) further collected qualitative data from social workers, nurses, and other health care professionals to explain these factors. For instance, the mutual trust was defined as establishing relationships with family members, hearing and respecting each other, and mutually sharing information with the family. The factor-shared decision-making illustrated the importance of the collaborative process in decision making. The concept of reciprocal relationships was defined as treating families with dignity and respect and understanding each family’s unique needs. The component of facilitation of family participation in service encouraged family members to make and carry out services-related plans. The strengths-based practice aimed to improve family members’ feelings of control and independence in the process. Interdisciplinary teamwork emphasized providing comprehensive and integrated services across disciplines (Craft-Rosenberg et al., 2006). The reliability of the total scale was tested in their initial survey among Euro-American multidisciplinary health care practitioners, including social workers, who worked with children in a Midwestern state in the United States and it yielded a .86 Cronbach’s alpha (Craft-Rosenberg et al., 2006).
Purpose of This Study
The purpose of this study is to examine the factor structure of the Family-Centered Practice Questionnaire which was developed by Craft-Rosenberg et al. (2006) using a Confirmative Factor Analysis (CFA) among child welfare workers. It involves two-stage analyses. In the first stage, CFA is used to confirm that Craft-Rosenberg et al. (2006) proposed a one-factor model and a seven-factor model among child welfare workers and further tested the second-order seven-factor model in a comparison with the seven-factor model. The second stage of analyses is to modify the factor structures proposed by Craft-Rosenberg et al. (2006) based on CFA statistical modification indices (MIs) with support from family-centered practice theoretical frameworks (Allen & Petr, 1998; Child Welfare Information Gateway, n.d.; Epley et al., 2010). This study is the first to evaluate the factor structure of the Family-Centered Practice Questionnaire with child welfare workers. Moreover, tests were conducted for internal consistency, convergent validity, and discriminant validity to further provide a family-centered practice instrument for child welfare practice and research.
Measuring the implementation level of family-centered practice and examining the effectiveness of family-centered practice on children’s outcomes requires a reliable and valid instrument which suits child welfare settings. The Family-Centered Practice Questionnaire (Craft-Rosenberg et al., 2006) was used to examine the effects of individual characteristics and organizational climate on the implementation of family-centered practice in child welfare (Ahn et al., 2016). However, no studies have evaluated the established factor structure for the Family-Centered Practice Questionnaire in child welfare settings. Thus, this study makes a unique contribution to provide an instrument to capture family-centered practice in child welfare.
Method
Data Source
This study used secondary data from a 2011 statewide family-centered practice follow-up online survey among child welfare staff including social workers, supervisors, and administrators (Ahn et al., 2011). The data were collected 6 months after child welfare professionals were trained in and implemented the family-centered practice model. The family-centered practice model in this state focused on strategies for child welfare staff to engage families in assessment, planning, and intervention, with a primary strategy of utilizing FGDM. The survey aimed to assess child welfare staff’s perceptions of family-centered practice efforts and their personal attitudes toward family-centered practice (Ahn et al., 2011). A total of 364 child welfare staff responded to this online follow-up survey. However, 57 participants did not answer any of the 39 items of the Family-Centered Practice Questionnaire; therefore, only 307 participants were included in this study. The current study received a determination of human subjects’ research exempt review by the University Institutional Review Board.
Sample
Participants’ characteristics are presented in Table 1. The majority of participants were female (n = 272; 88.6%) and White (n = 239; 77.9%). Almost three-quarters had Master of Social Work (MSW) degrees (n = 226; 73.6%) and most were between 25 and 54 years old (n = 242; 78.8%). Participants’ primary service areas included child protective services (n = 91; 29.6%), in-home family services (n = 72; 23.5%), and foster care (n = 127; 41.4%). Most participants worked as frontline social workers (n = 223; 72.7%), followed by supervisors (n = 41; 13.4%) and administrators or managers (n = 28; 9.1%). On average, they had worked in public child welfare for 10 years (M = 10.4, SD = 9.4) and their average caseloads per month were about eight (M = 7.7, SD = 8.3).
Sample Characteristics (N = 307).

Note. DHR/SSA = Department of Human Resources/Social Service Administration.
A comparison of demographics between 57 participants who did not complete the Family-Centered Practice Questionnaire and 307 participants who filled out this measure was conducted. Bivariate analyses showed that these two samples were different in their degree types (χ2 = 12.84, p = .03) and their role in the agency (χ2 = 12.59, p = .01). Compared to the 307 in the sample, there was a similar proportion of MSWs, but no one of the 57 sample had master’s degrees in other disciplines and no one provided foster parents–related services.
Measures
Demographics
The demographics in this study included participants’ sex, race, ethnicity, education, age range, special areas in child welfare (e.g., child protective services, in-home family services, foster care, adoption, foster parent services, Department of Human Resources/Social Service Administration, and other), and positions in agencies (e.g., social worker, supervisor, administrator or manager, and other).
The Family-Centered Practice Questionnaire
The Family-Centered Practice Questionnaire included seven components (i.e., mutual trust, shared decision-making, reciprocal relationships, facilitate family participation, strengths-based practice, interdisciplinary teamwork, and cultural competence and sensitivity) of family-centered practice and had a 4-point scale with ordered categorical response options (1 = never to 4 = almost always). The original questionnaire also had an option of “5 = not applicable or uncertain” in the original questionnaire. However, the option of “not applicable or uncertain” was recoded as missing in this study to allow for the questionnaire to have an interpretable scale. The scores of each of the seven subscales were the sum of items without reverse coding and the Family-Centered Practice Questionnaire total score was calculated as the sum of all 39 items.
Data Preparation and Screening
The data were screened by examining the distribution of each item across categories and no outliers were identified. The data indicated high levels of child welfare workers’ adherence to family-centered practice. The response “almost always” was the most frequent response on all items, followed by “usually.” The percentage ranged from 40.4% on Item 18 to 86.0% on Item 3 for “almost always” option. For “usually,” it ranged from 8.5% to 31.9%, while “occasionally” ranged from 0.3% to 16.0%. For “never” option, it ranged from 0.0% to 8.1%.
Data Analysis
Data cleaning and descriptive data analysis were conducted with SPSS version 24 (IBM Corp, 2016). Craft-Rosenberg and her colleagues (2006) have provided framed factors and items for the Family-Centered Practice Questionnaire based on the family-centered practice theoretical framework and their empirical data; therefore, an exploratory factor analysis was not conducted for this study. Mplus Version 8.0 was used to conduct a confirmatory factor analysis (CFA; Muthén & Muthén, 1998–2017). The items were treated as ordinal data and the analyses used the weighted least squares means and variance (WLSMV)-adjusted estimator (Byrne, 2012).
Missing data
The percentage of missing data for each item ranged from 2.0% (Item 35) to 17.6% (Item 18), with only seven items (Items 1, 17, 18, 36, 32, 49, and 33) having missing data greater than 10.0%. Little’s Missing Completely at Random (MCAR) test was conducted with χ2 = 2623.86 and p < .001. The significant chi-square indicated that data were not MCAR. Thus, full information maximum likelihood and multiple imputations, which both assume data missing at random, may not be the most appropriate in this case (Muthén & Muthén, 1998–2017). The WLSMV estimator, which allows analysis of cases with partially missing data by pairwise methods, was used (Muthén & Muthén, 1998–2017).
Multiple fit indices were used to assess the model fit. According to Kline (2016), a nonsignificant χ2 indicates a good model fit. However, χ2 is sensitive to discrepancies in model fit especially in large sample size (Byrne, 2012; Kline, 2016). Byrne (2012) recommended the comparative fit index (CFI) and Tucker–Lewis Index (TLI) be greater than .90 for an adequate fit and greater than .95 for a good fit. The root mean square error of approximation (RMSEA) value less than .05 indicates a good model fit and the upper bound of the 90% confidence interval should be less than .08. Tabachnick et al. (2012) suggested .63 as a cutoff score for good item loadings on factors.
A total of five models were tested. The first three models with 39 items (one-factor, seven-factor, and second-order seven-factor models) were derived from the original measure scoring instructions, and the second two models with 31 items (five-factor model and the second-order five-factor model) were derived from modifications to the original 39-item structure. Due to statistical implications of the data, models were revised. The modification process included dropping items and combining factors according to factor loadings, correlation residuals, modification index, and theories. Specifically, the tests for revised models with five factors were carried out according to statistical fit indices with support from key elements of family-centered practice summarized from previous conceptual and theoretical frameworks (Allen & Petr, 1998; Child Welfare Information Gateway, n.d.; Epley et al., 2010).
The sample contained social workers who were directly working with children and families. It also included administrators and supervisors who were indirectly serving children and families. Considering the sample heterogeneity, we also ran the same CFA models within caseworkers and social workers (N = 223), excluding supervisors, administrators or managers, and others. However, the model fit indices were not improved significantly. Although chi-square decreased slightly, the decreased chi-square was due to the decreased sample size. Thus, all types of child welfare workers were included in the CFA models (N = 307).
Internal consistency and discriminant and convergent validity
Internal consistency was tested using coefficient alpha. Convergent validity was tested by calculating the average variance extracted (AVE) scores. The AVE for each latent variable indicates how much variance is explained by each latent construct. When AVE is greater than .5, it indicates that convergent validity is achieved (Fornell & Larcker, 1981). Furthermore, convergent validity was assessed by using Hair et al.’s (1998) criteria for standardized factor loadings of all items that are not less than .5 and composite reliability is not less than .7. Composite reliability, similar to Cronbach’s alpha, is an indicator of internal consistency in scale items (Brunner & SÜβ, 2005; Netemeyer et al., 2003). It is equal to the total amount of true score variance relative to the total scale score variance (Brunner & SÜβ, 2005).
Discriminant validity was assessed through correlations between latent factors. Correlations below .85 indicated reasonable discriminant validity between latent factors (Brown, 2015). To further assess discriminant validity, we compared the square root of AVE scores with the correlation between factors (Fornell & Larcker, 1981). If the square root of the AVE of a factor is larger than the correlation between two factors, satisfied discriminant validity is achieved (Fornell & Larcker, 1981).
Results
One-Factor Model With 39 Items
The one-factor model had a poor fit based on the fit indices (RMSEA = .079, CFI = .850, TLI = .841, and χ2 = 2044.595, df = 702, with p < .001). The fully standardized loading coefficients ranged from .31 (Item 1 in Table 4) to .93 (Item 33). The one-factor model with 39 items did not meet the fitness indices mentioned earlier. Thus, this model was rejected as it did not support the original measure factor structure using these child welfare workers’ data.
Seven-Factor Model With 39 Items
The seven-factor model had 39 items, including seven latent variables (i.e., mutual trust, shared decision-making, reciprocal relationships, facilitation of family participation in service, strengths-based practice, interdisciplinary teamwork, and cultural competence and sensitivity). A detailed description of what items loaded on what factors is presented in Table 4. The seven-factor model with 39 items did not have a positive definite matrix, which was caused by the interdisciplinary teamwork factor. The nonpositive definite might be related to the ordinal response options in this measure and a relatively small sample size for a measure with 39 items in this study (Rigdon, 1997).
This model had fair model fit indices (RMSEA = .051, CFI = .940, TLI = .935, and χ2 = 1217.110, df = 681, with p = .000). The fully standardized loading coefficients ranged from .31 (Item 1) to .93 (Item 33), some of which were below the cutoff score for loadings (Tabachnick et al., 2012). The correlations between seven factors ranged from .56 (shared decision-making with mutual trust) to .92 (family participation with reciprocal relationship). Therefore, the seven-factor model with 39 items was rejected.
Second-Order Seven-Factor Model With 39 Items
The higher order in this model was the family-centered practice, and seven lower order factors were the same as the previous model. The second-order seven-factor model with 39 items also did not have a positive definite matrix because of the interdisciplinary teamwork factor. The model had a fairly good model fit (RMSEA = .051, CFI = .938, TLI = .934, and χ2 = 1251.438, df = 695, with p = .000). The fully standardized coefficients ranged from .31 (Item 1) to .94 (Item 33). The second-order seven-factor model with 39 items did not fit well with the data due to the nonpositive definite matrix problem and poor factor loadings. Thus, the second-order seven-factor model with 39 items was rejected as well. With the poor model fit of the models with seven factors, we modified the seven-factor model to a five-factor model.
A Modification of the Seven-Factor Model: Five-Factor Model With 31 Items
The five-factor model with 31 items was conducted with the following steps. First, the interdisciplinary teamwork factor was problematic because it caused nonpositive definite matrix. Moreover, the reliability of interdisciplinary team work subscale was .54 in this sample, which was below .63 (Tabachnick et al., 2012). Also, previous family-centered practice literature in child welfare did not mention interdisciplinary teamwork as a component of family-centered practice, although this measure was originally developed for interdisciplinary professionals. Thus, the interdisciplinary teamwork factor with three items was dropped from the measure. Second, according to Kline (2016), if the correlation between two factors is greater than .85, the measure probably does not have adequate discriminant validity (Kline, 2016). Because the correlation between family participation and reciprocal relationship was high (r = .92), previous literature about the elements of family-centered practice supported that these two concepts did not need to be separated; therefore, these two factors (facilitate family participation and reciprocal relationships) were combined into one factor (family as a unit). We renamed this factor to “a family as a unit” because these items reflected that professionals respected family members and children as a serving unit instead of only considering parents or children’s perspectives, which was consistent with the concept of treating the family as a whole unit in child welfare family-centered practice. In addition, previous literature suggests a consensus around the concept of serving the whole family as a component of family-centered practice (Allen & Petr, 1998; Epley et al., 2010; Lietz, 2011). Thus, the five factors were mutual trust, shared decision-making, family as a unit, strengths-based practice, and cultural competence and sensitivity. Third, four items (Item 1, Item 2, Item 3, and Item 20) were dropped step by step according to .63 loading coefficient cutoff score (Tabachnick et al., 2012). After dropping these four (Items 1–3 and Item 20) low-loading items (loading coefficient < .63), Item 4 (i.e., relate to families as responsible, trustworthy people with loading coefficient = .65) was dropped because the MIs indicated this item caused a problematic effect on the model fit (MI under the “by statement” ranged from 150 to 179). According to Kline (2016), an MI greater than 10 is problematic to some extent and some theoretically justified modifications should be considered. Furthermore, because this instrument was developed for child welfare practitioners, achieving parsimony could be a potential goal in validating this measure in the child welfare sample. Thus, this item was dropped. Finally, 31 items were remaining, and the description of items is presented in Table 4. The five-factor model with 31 items had an adequate overall fit based on the fit indices (RMSEA = .043, CFI = .968, TLI = .965, and χ2 = 659.968, df = 424, with p < .001). The overview of the model fit indices is presented in Table 2. A total of 31 items were significantly loaded on five factors for fully standardized coefficients results, and the loadings are shown in Table 4 and Figure 1. The ranges of fully standardized factor loadings within five factors are shown in the parentheses: mutual trust (.81–.89), shared decision-making (.71–.92), family as a unit (.66–.85), strengths-based perspectives (.82–.90), and cultural competence and sensitivity (.63–.89). The correlations between each factor are presented in Table 3. Five factors were significantly correlated. For example, the cultural competence and sensitivity had the highest statistically significant correlation with strengths-based perspective (r = .82), followed by shared decision-making (r = .76), family as a unit (r = .74), and mutual trust (r = .06).
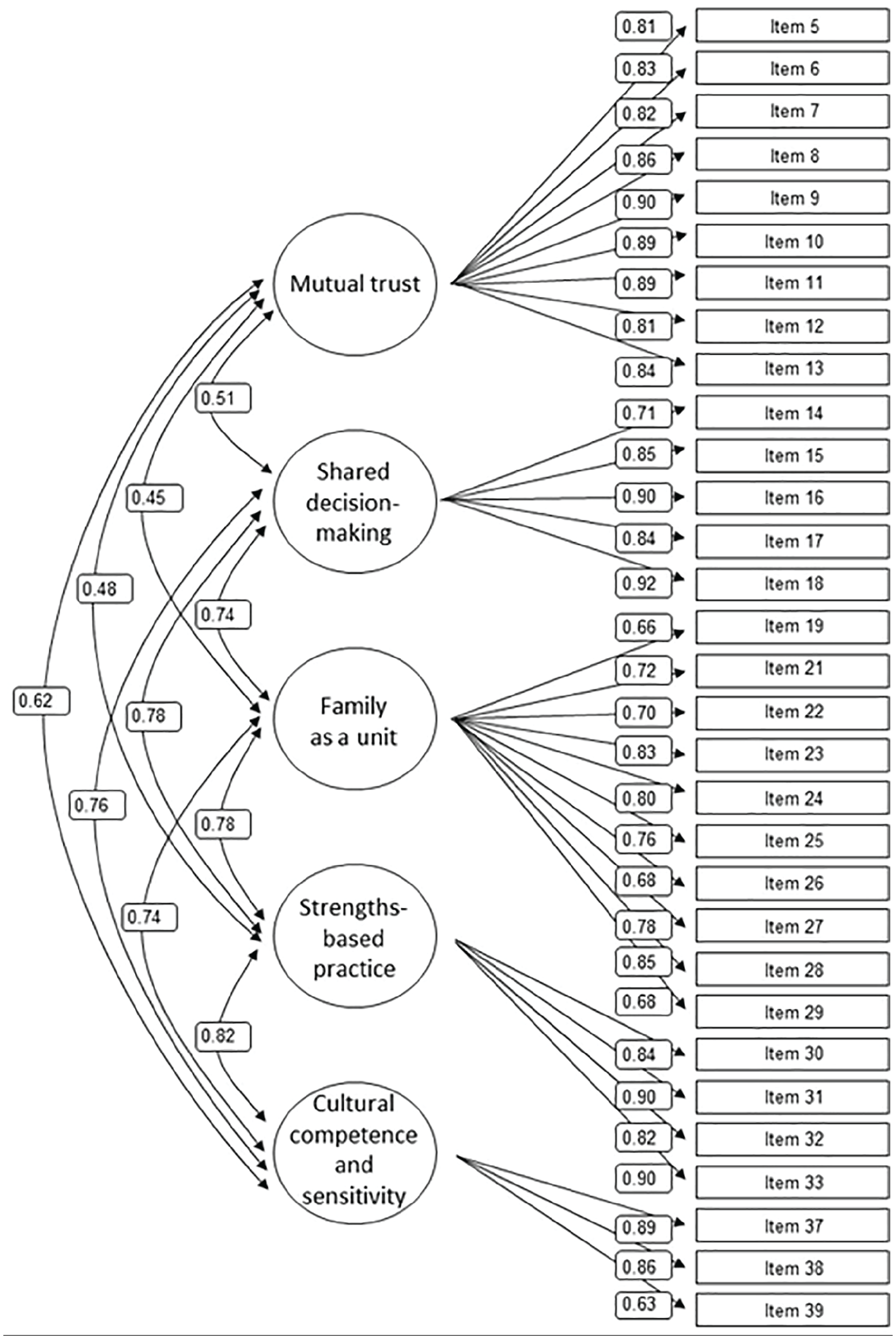
Five-factor model of the Family-centered Practice Questionnaire with 31 items.
Confirmatory Factory Analysis Model Fit Indices.
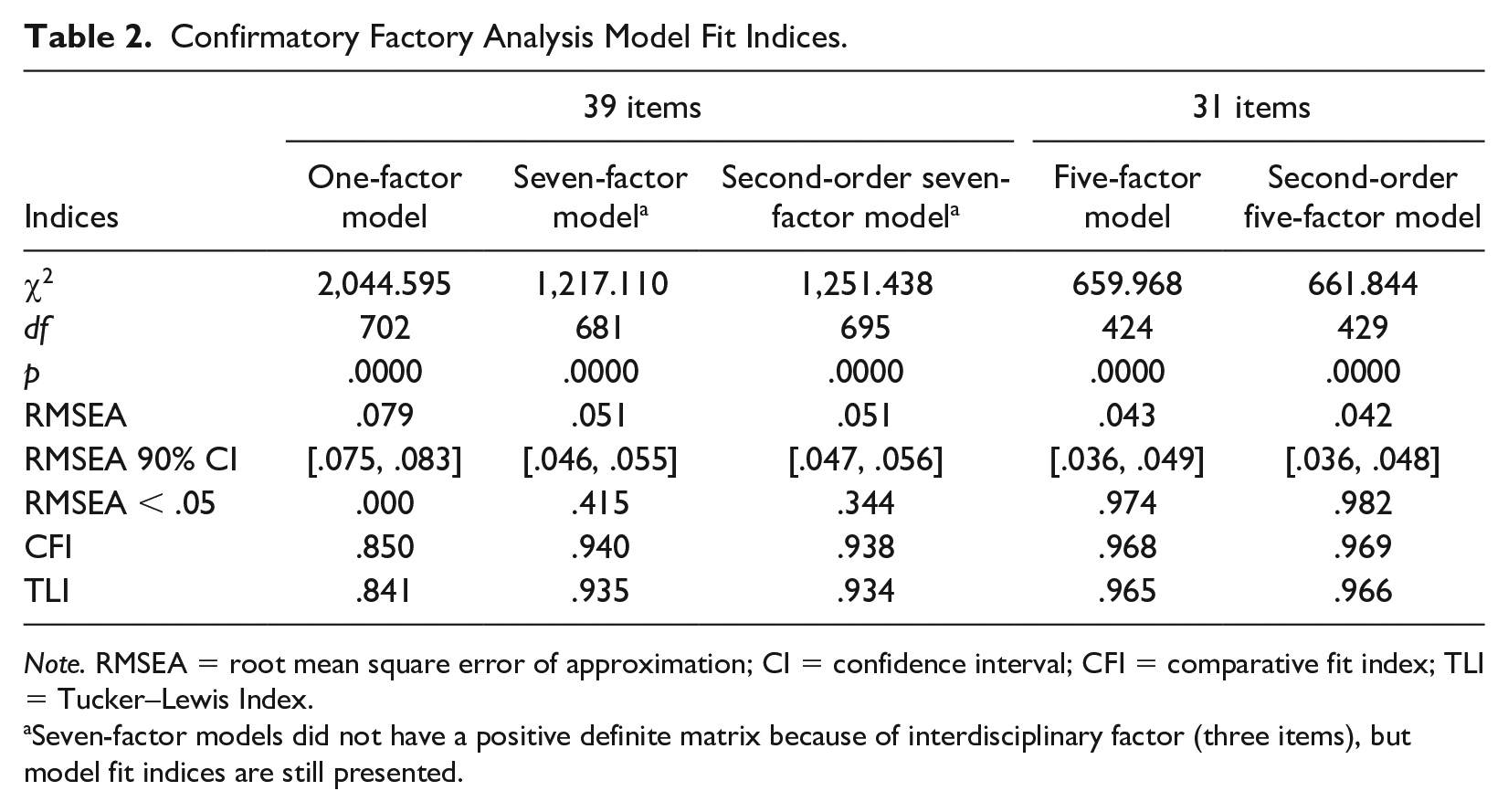
Note. RMSEA = root mean square error of approximation; CI = confidence interval; CFI = comparative fit index; TLI = Tucker–Lewis Index.
Seven-factor models did not have a positive definite matrix because of interdisciplinary factor (three items), but model fit indices are still presented.
Correlations Among Factors in Five-Factor Model and Square Root of AVE of Each Factor.
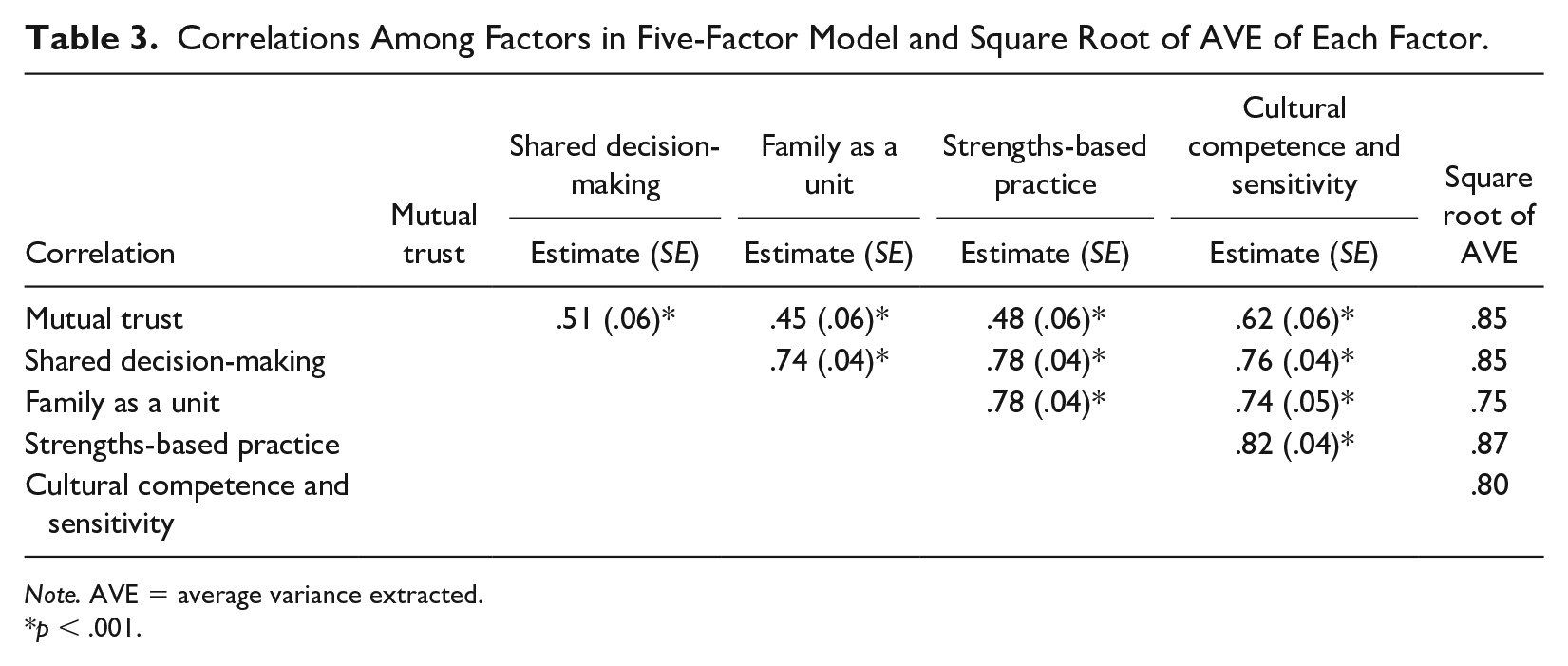
Note. AVE = average variance extracted.
p < .001.
A Modification of the Seven-Factor Model: Second-Order Five-Factor Model With 31 Items
According to theories of family-centered practice in child welfare, the family-centered practice is composed of different elements. Thus, the second-order five-factor model with 31 items was conducted to measure the ability of the Family-Centered Practice Questionnaire to capture general family-centered practices. The second-order five-factor model yielded an overall adequate fit based on the fit indices (RMSEA = .042, CFI = .969, TLI = .966, and χ2 = 661.844, df = 429, with p < .001). The fully standardized item loadings ranged from .63 (Item 39 under the cultural competence factor) to .92 (Item 18 under the shared decision-making factor). The loadings for each factor were significant, and the coefficients are presented in the parentheses: mutual trust (.58), shared decision-making (.87), family as a unit (.84), strengths-based (.90), and cultural competence and sensitivity (.92). The detailed standardized loadings are presented in Table 4 and Figure 2.
The Family-Centered Practice Questionnaire and Factor Loadings for Five-factor Model and Second-Order Five-Factor Model (N = 307).

Note. × denotes items were dropped.
Family as a unit was a new factor, which combined factor of reciprocal relationships and factor of facilitate family participation.
p < .001.

Second-order five-factor model of the Family-Centered Practice Questionnaire with 31 items.
A Model Comparison Between Five-Factor Model and Second-Order Five-Factor Model
To compare model differences between the five-factor model and the second-order five-factor model, a chi-square difference test was conducted. Results, χ(5)2 = 9.6, p = .09, did not reject the null hypothesis and indicated that two models were statistically equivalent (Bryant & Satorra, 2012).
Internal Consistency Reliabilities
In the current study, internal consistency reliabilities for original 39 items are mutual trust with 13 items (α = .89), shared decision-making with five items (α = .87), reciprocal relationship with four items (α = .71), family participation with seven items (α = .83), strengths-based practice with four items (α = .86), interdisciplinary teamwork with three items (α = .54), cultural competence and sensitivity with three items (α = .73), and the total 39-item scale of family-centered practice (α = .95).
For the revised 31-item version, the internal consistency reliabilities are mutual trust with nine items (α = .97), shared decision-making with five items (α = .89), family as a unit with 10 items (α = .92), strengths-based practice with four items (α = .86), and cultural competence and sensitivity with three items (α = .73), and the total 31-item scale of family-centered practice (α = .97).
Discriminant Validity and Convergent Validity
The five-factor model and the second-order five-factor model had the same AVE scores for each latent variable. The AVE scores are presented in parentheses for each factor: mutual trust (.72), shared decision-making (.72), family as a unit (.56), strengths-based practice (.75), and cultural competence and sensitivity (.64). This measure’s convergent validity was achieved because AVE scores were greater than the .5 benchmark (Fornell & Larcker, 1981). Furthermore, using more stringent criteria, this measure had a satisfactory convergent validity with factor loadings greater than .5 and construct reliabilities greater than .7 (Hair et al., 1998).
Regarding discriminant validity, the correlations (.45–.82) between constructs were below the .85 benchmark, which indicated that this measure reached discriminant validity to some extent. To use a more stringent criterion to assess discriminant validity, we further compared the square root of AVE of five factors (i.e., mutual trust, shared decision-making, family as a unit, strengths-based practice, and cultural competence and sensitivity) with the correlation between that factor and other factors (see results in Table 3). Fornell and Larcker (1981) recommended that the value of the square root of AVE of a particular factor should be higher than the correlation between factors. Comparing the square root of AVE (.75–.85) of each factor to the correlations (.45–.82) between that factor and other factors, most constructs met discriminant validity. However, the constructs of family as a unit, strengths-based practice, and cultural competence and sensitivity were not significantly distinguished with each other.
Discussion and Conclusion
The goal of this study is to examine the factor structure of the Family-Centered Practice Questionnaire, which is used to evaluate the level of implementation of family-centered practice among child welfare workers. The results of this study indicate that the three models based on the original measure’s scoring instructions yielded a poor model fit. Our data do not support the original one-factor, seven-factor, and second-order seven-factor models, which imply that child welfare workers’ understanding of the family-centered practice may be different from that of social workers and nurses who work with children in health care settings. These inconsistencies may be related to differences in clients’ attributes and working environments, which highlights the importance of having an appropriate measure for child welfare settings. However, the revised five-factor structure of the 31-item and the second-order five-factor structure of the 31-item had adequate overall fit indices. These two models were statistically comparable and treated as alternative models given that no statistically significant differences were identified in the model comparisons. The five factors under the family-centered practice are mutual trust, shared decision-making, family as a unit, strengths-based practice, and cultural competence and sensitivity. The identified five factors are aligned with a qualitative study examining 44 service recipients’ perceptions of family-centered practice in child welfare services (Lietz, 2011). It also aligns with Dunst’s (2002) description of a family-centered approach, such as “treat families with dignity and respect; information sharing so families can make informed decisions; family choice regarding their involvement in and provision of services; and parent/professional collaborations and partnerships as the context for family program relations.”
Implications for Family-Centered Practice in Child Welfare
This revised version of the Family-Centered Practice Questionnaire with 31 items has some implications for family-centered practice in child welfare. Child welfare agencies and workers could utilize this short version with relatively sufficient psychometric properties to measure the level of the family-centered practice implementation in practice. Child welfare practitioners can use either a summative score of 31 items to capture the full dimension of the family-centered practice or use scores of five subscales to measure each aspect of the family-centered practice. The five distinctive factors of family-centered practice could further help assess the performance level of child welfare practitioners and agencies in each aspect of the family-centered practice.
This five-factor structure suggests that child welfare practitioners need to establish mutual trust among children and families, other professionals, and child welfare agencies. In addition, child welfare practice is a shared decision-making process, which requires child welfare practitioners to view the family as a unit and to emphasize the family’s strengths. To work with diverse children and families, it may also be essential for child welfare practitioners to improve cultural competence and sensitivity, such as providing culturally responsive services to immigrant families (Xu et al., 2018) and affirming and supporting sexual and gender minority youth and their families (Erney & Weber, 2018). Furthermore, building mutual trust with families is warranted as some mistrust exists between families of color and child welfare agencies (Redd et al., 2005). Some evidence-based family-centered programs and strategies, such as FGDM, Kinship Navigator programs, and Family Connections programs, could be integrated to child welfare systems to improve family-centered practices (DePanfilis & Dubowitz, 2005; Rushovich et al., 2017; Xu et al., 2017).
Family-centered practice has been proposed and implemented for decades; however, the lack of reliable and validated measures in child welfare settings has been a limitation in evaluating family-centered practice, given that more work has focused on family-centered practice (Lietz & Rounds, 2009). In addition, the previously validated family-centered practice measures were based on health care settings, and those measures were more suitable for health care professionals instead of child welfare workers (McWilliam & Winton, 1990; Murphy et al., 1995; Woodside et al., 2001). This revised short version of the family-centered practice measure can be an instrument for child welfare researchers to evaluate the family-centered practice in the field and produce more rigorous program evaluation research.
Limitations
It is important to note limitations of the study. First, this study was a female and White-dominated sample in a Mid-Atlantic state in the United States, which was generally indicative of staff members in the child welfare sector. Therefore, caution is required when interpreting the psychometrics of the measure in other groups of social workers. Second, items were unevenly distributed across five factors, ranging from three items (factor: cultural competence and sensitivity) to 10 items (factor: family as a unit). Third, this study made several modifications of factor structures, which may be due to characteristics of this sample. It may not be generalizable to other populations. Furthermore, although this study did not support the original seven-factor structure, the seven-factor structure should be examined in other samples to confirm. In addition, the five-factor structure of this measure needs to be replicated with other samples to confirm, particularly given that this study made several modifications to the structure and tested them with the same sample. Furthermore, the interdisciplinary work factor in the seven-factor model resulted in a nonpositive definite result and we excluded this factor in the current study based on statistical results and theoretical justifications. Interdisciplinary work in child welfare can be important for child welfare staff, although child welfare staff may not perceive it as interdisciplinary work because it is a natural part of child welfare practices. Finally, more work is needed to evaluate this measure’s discriminant validity and criterion validity. This measure’s discriminant validity is not fully achieved among some latent variables, including family as a unit, strengths-based perspective, and cultural competence and sensitivity. This study is not able to test criterion validity of this measure by examining whether child welfare workers’ implementation of the family-centered practice is associated with experiences and outcomes of children and families because these outcomes and experiences with the family-centered practice were not collected in this study.
Implications for Future Research
There are several future research directions. First, this measure should be examined in broader samples with various child welfare workers across different cultural contexts. Validating the Family-Centered Practice Questionnaire with a sample of more racially and ethnically diverse child welfare staff is needed to test the five-factor structure and apply it across child welfare staff populations. Second, some measurement development work is needed. Researchers need to further develop items to capture information for family as a unit and cultural competence and sensitivity in child welfare. Future research should further test if interdisciplinary work is an essential factor of family-centered practice in child welfare practices. In addition, balancing the item distributions among different factors would be beneficial for the instrument. Also, it is critical to use a multi-informant strategy to further develop the Family-Centered Practice Questionnaire. Finally, further validity analysis needs to be conducted to test whether this revised 31-item Family-Centered Practice Questionnaire predicts relevant outcomes.
Conclusion
Having a family-centered practice measure for child welfare workers promotes the implementation of family-centered practice and eventually benefits children and families’ well-being, safety, and permanency outcomes. The revised measure can be a useful tool in evaluating family-centered practice among child welfare workers and agencies. This measure will help to identify gaps in implementation processes and provide concrete guidance for child welfare workers to improve their competency in applying family-centered approaches to their clients.
Footnotes
Acknowledgements
The authors thank Donna Harrington, PhD, for her statistical expertise and generous advice. The authors extend their gratitude to the child welfare workers who contributed to this study by providing valuable information about their practices.
Disposition editor: Sondra J. Fogel
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a contract with a mid-Atlantic state child welfare agency.