
Abstract

In this Letter to the Editor, we examine two cases of catatonia in siblings with profound autism and shared genetic mutations. To our knowledge, this is the second report in the literature of siblings with autism and catatonia who were treated using electroconvulsive therapy (ECT) (Bailine and Petraviciute, 2007). We will discuss the timeline of diagnosis and treatment for each child as well as the pharmacotherapy regimen and number of ECT treatments each child received.
Catatonia is a severe neuropsychiatric syndrome marked by motor, affective, and behavioral symptoms such as mutism, posturing, impulsivity, and aggression (Hirjak et al., 2024). In neurodivergent youth, catatonia may also manifest as incontinence, self-injury, and regression, with externalizing symptoms often misattributed to autism or oppositionality (Luccarelli et al., 2024; Smith et al., 2024). As a result, catatonia is frequently underdiagnosed in autistic children. This case series describes Sibling 1 and Sibling 2, siblings’ ages 11 and 13, who presented with catatonia in the setting of profound autism.
Sibling 1 and Sibling 2 share the genetic mutation SLC6A1. SLC6A1 plays a critical role in GABAergic transmission, and a growing body of evidence implicates impaired GABA signaling in the pathogenesis of catatonia (Carvill et al., 2015). The shared genetic vulnerability observed in this case further supports the role of GABAergic dysfunction in catatonia and underscores the need for continued investigation into catatonia across genetic syndromes, particularly those involving genes that regulate GABA transmission.
Sibling 1 was evaluated at age 4 for hyperactivity and impulsivity. By age 6, episodes of screaming and agitation led to risperidone treatment. At age 7, he trialed several medications (Table 1), with clonazepam 0.25 mg daily yielding the most benefit for behavior. He exhibited posturing and unresponsiveness, but electroencephalography showed no seizure activity. He remained on anti-epileptic therapy.
Summary of Clinical Features, Treatments, and Genetic Findings in Two Siblings With Autism and Catatonia
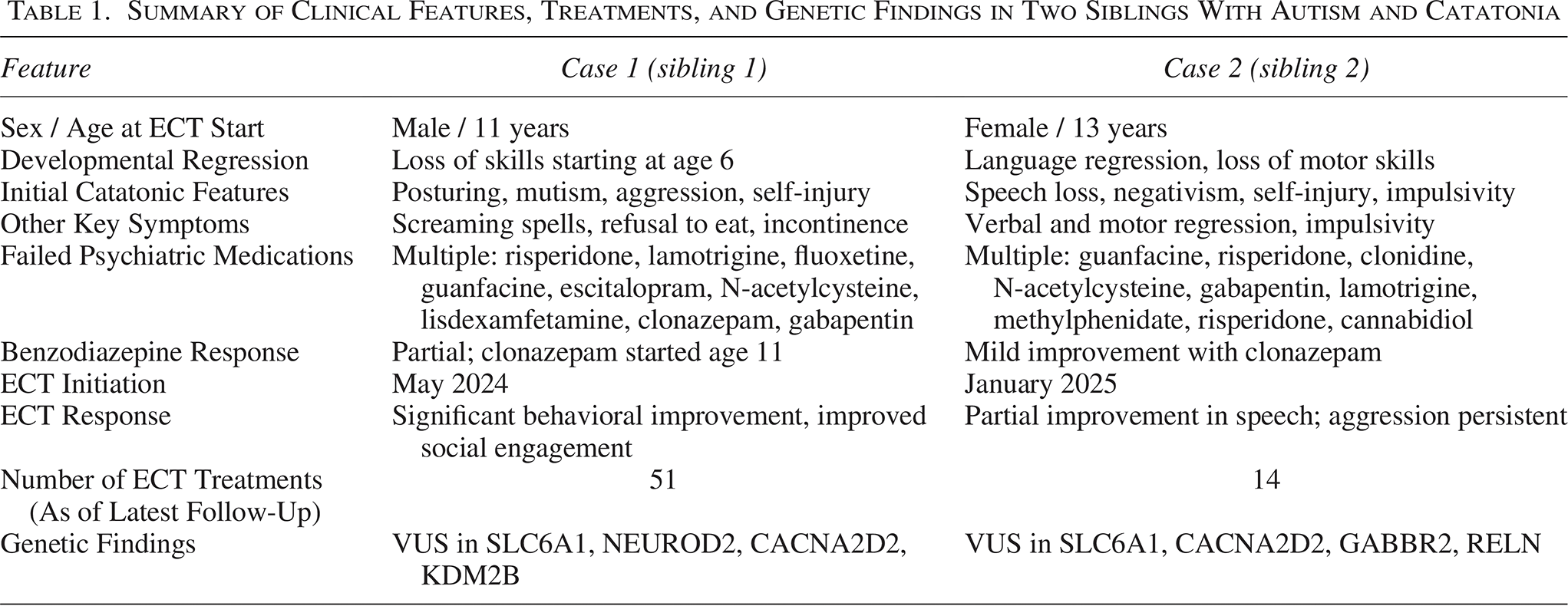
At age 8, Sibling 1 was referred for ECT due to his response to clonazepam and possible catatonia. His Bush Francis Catatonia Rating Scale (BFCRS) score was 15; KANNER Catatonia Severity Scale (KCS) and KANNER Catatonia Examination (KCE) scores were 28 and 1, respectively. He developed new-onset headbanging, which improved with increased clonazepam but later recurred. After initiating ECT, his mother noted improved aggression, communication, and social engagement.
Sibling 2 is a 13-year-old female with Lennox–Gastaut syndrome and profound autism. She developed seizures at 21 months, followed by self-injury and impulsivity by age 10. By age 12, she had fewer language skills than at age 3 and exhibited regression. Clonazepam partially improved her aggression and self-injury (see Table 1 for failed medications). Initial BFCRS was 20; KCS and KCE were 32 and 4, respectively. At age 13, she began ECT. After seven treatments, her mother observed improved spontaneous speech and word variety, though aggression persisted. Her most recent KCS and KCE scores are 8 and 2, respectively.
Sibling 1 and Sibling 2 continue receiving bitemporal ECT with brief pulse width (0.5 ms). Sibling 1 has received 51 treatments, and Sibling 2 has received 14.
This series contributes to growing evidence supporting ECT’s safety and effectiveness for catatonia in pediatric patients with profound autism. Maintenance ECT is often necessary in those with co-occurring intellectual disability (Wachtel et al., 2025). Sibling 1 demonstrated mild improvement following several initial ECT sessions but required additional treatments to achieve a more robust response. Subsequently, he received maintenance ECT to sustain therapeutic benefit.
Emerging data suggest genetics may influence catatonia risk in neurodevelopmental disorders. Behavioral features such as aggression, regression, and affective instability also appear in syndromes like Synaptic GTPase Activating Protein 1 -related disorders. Both siblings in this series carry variants of uncertain significance, including one in SLC6A1, a gene associated with epilepsy and neurodevelopmental delay. This supports a possible shared genetic vulnerability to catatonia, epilepsy, and neurodevelopmental delay.
In conclusion, these cases highlight the potential role of ECT and genetic susceptibility in pediatric catatonia among profoundly autistic patients.
Authors’ Contributions
A.S.: Conceptualization, methodology, investigation, data curation, investigation, writing—original draft. I.B.: Investigation, data curation, writing—review and editing. J.R.S.: Conceptualization, methodology, investigation, data curation, writing—review and editing, supervision.
Footnotes
Compliance with Ethical Standards
We received institutional review board approval from Vanderbilt University Medical Center to waive consent and review, analyze, and report anonymously on these patients (IRB Number: 220898). We have also obtained written consent for this report to be published. The consent form is attached to this submission.
Data Availability
The data that support the findings of this study are available from the corresponding author, J.R.S., upon request.
Disclosures
J.R.S. receives funding from the National Institute of Child and Human Development. J.R.S. also receives support from Axial and Roche.