
Abstract
Objective:
Evidence for medical cannabis use and effectiveness in autism has begun to accumulate but remains limited, even as clinical interest has rapidly increased. In Israel, medical cannabis may be prescribed for autism with severe behavioral disturbances under strict Ministry of Health criteria requiring prior trials of two Food and Drug Administration (FDA)-approved antipsychotics. Using a large real-world dataset, this study aimed to characterize autistic individuals prescribed medical cannabis and evaluate adherence to national guidelines.
Methods:
A retrospective cohort study was conducted using electronic medical records from Clalit Health Services, Israel’s largest Health Maintenance Organization. All individuals with a documented autism diagnosis between 1990 and 2025 were identified (N = 36,610) and classified as cannabis-prescribed (N = 462) or not-prescribed (N = 36,148). Demographic and clinical characteristics were compared, including prior use of FDA-approved antipsychotics.
Results:
Only 1.2% of individuals with autism were prescribed medical cannabis. Of these, 4.3% of prescriptions were issued for children under 5 years of age. The cannabis-prescribed group was diagnosed earlier (median 3 vs. 5 years, p < 0.001) and had higher rates of ADHD (42% vs. 30%), intellectual disability (12% vs. 5%), and epilepsy (14% vs. 6%) (all p < 0.001). While 69% had used at least one FDA-approved antipsychotic medication prior to cannabis initiation, only 28% had documented trials of both, as required by national guidelines. Marked sociodemographic disparities were also observed: the cannabis-prescribed group had a higher socioeconomic status (median SES 7 vs. 6, p < 0.001) and lower representation of Arab individuals (2.7% vs. 11%, p < 0.001).
Conclusions:
Medical cannabis use among autistic individuals was rare and mainly observed among those with more complex clinical profiles and higher socioeconomic backgrounds. Most prescriptions did not fully comply with guidelines requiring prior antipsychotic trials. These findings underscore the need for enhanced regulatory oversight, equitable access, and longitudinal research to evaluate real-world outcomes and guide evidence-based clinical practice.
Introduction
Autism is a neurodevelopmental condition characterized by deficits in social communication and presence of restricted, repetitive patterns of behavior. Comorbidity is common, particularly behavioral and emotional challenges such as irritability, temper outbursts, aggression, anxiety, and self-injurious behaviors (Hirota and King, 2023). To date, only two medications—Risperidone and Aripiprazole—are approved by the Food and Drug Administration (FDA) for treatment of irritability and aggression in autistic individuals. Both have demonstrated significant efficacy, with effect sizes in the large range (Fung et al., 2016; Meza et al., 2025; Pablo et al., 2023). However, their use is often limited by adverse effects. Moreover, treatment response is not universal, with a non-negligible proportion of individuals not responding to either medication (Marcus et al., 2009; Pablo et al., 2023). Given the need for new pharmacological options, medical cannabis has emerged as a potential treatment (Mostafavi and Gaitanis, 2020; Poleg et al., 2019); however, evidence regarding its efficacy for both core symptoms and comorbidities remains limited (Agarwal et al., 2019; Aran and Cayam Rand, 2024). Most available evidence comes from observational and open-label studies (Fleury-Teixeira et al., 2019) with a notable lack of high-quality randomized controlled trials (Parrella et al., 2023; Rice et al., 2024). Existing studies also vary considerably in cannabis formulations, dosages, and outcome measures (Riera et al., 2025). Nevertheless, existing studies suggest potential improvements in behavioral symptoms and irritability (Aran et al., 2021; Barchel et al., 2018; Jawed et al., 2024), and possibly in social communication and quality of life (Hacohen et al., 2022; Mazza et al., 2024), with reported benefits in about 60%–90% of participants (Aran et al., 2019; Schleider et al., 2019; Silva et al., 2022). Adverse effects varied in severity, ranging from mild somnolence to more serious outcomes such as seizures, severe aggression, and psychosis (Aran et al., 2019; Chhabra et al., 2024; Jawed et al., 2024; Schleider et al., 2019). Due to the current lack of sufficient evidence, medical cannabis is not an FDA-approved or standardized treatment for autism (Aran and Cayam Rand, 2024).
Globally, there are no established clinical guidelines regarding indications, patient selection, dosing, or treatment management for medical cannabis in autism, and it remains unclear which subgroups of individuals use it and may benefit from it. However, some preliminary findings suggest that individuals with more severe baseline symptoms may experience greater improvement (Hacohen et al., 2022).
Cannabis Use for Autism in Israel
In Israel, cannabis is a controlled substance under the Dangerous Drugs Ordinance. Medical use requires authorization by the Ministry of Health and its use outside the specific medical indications is prohibited by law. Prior to 2021, access to medical cannabis for individuals with autism in Israel was not formally approved and occurred only through individual, case-by-case authorizations or within research protocols. In 2021, autism spectrum disorder (ASD) with comorbid behavioral disturbances was added as an approved indication under strict criteria. These include age above 5 years, a documented Diagnostic and Statistical Manual of Mental Disorders fifth edition diagnosis of ASD, daily behavioral disturbances rated 5 or higher on the Clinical Global Impression scale (Busner and Targum, 2007) or an equivalent validated measure, persisting for at least 6 months, and failure of at least two FDA-approved antipsychotic medications due to lack of efficacy or discontinuation because of adverse effects. Treatment is restricted to cannabidiol-rich oil formulations prescribed and monitored by qualified specialists, and its use requires prior licensing by the Ministry of Health and the Israeli Medical Cannabis Agency.
In 2024, a regulatory reform enabled authorized specialists within the public health care system (under the Health Maintenance Organizations [HMO]) to issue electronic Ministry-approved licenses for medical cannabis through a national digital platform. These appear in the HMO medical record similarly to standard prescriptions. The reform also allowed case-by-case exceptions for children under 5 years of age with autism. All applications must include full documentation demonstrating compliance with the eligibility criteria.
Study Objectives
These policy and regulatory reforms have facilitated more systematic documentation and monitoring of the real-world use of medical cannabis among autistic individuals within their general medical records, enabling better characterization of this population alongside their broader clinical features, an area for which no empirical data are currently available. The aim of the present study is to utilize large-scale data from Israel’s largest HMO to describe the characteristics of autistic individuals prescribed medical cannabis and to evaluate whether real-world prescribing patterns align with national guidelines.
Methods
Data extraction
This retrospective, community-based observational study included all individuals insured by Clalit Health Services—the largest HMO in Israel, with over 4.9 million members, approximately half of the national population, and providing medical services across diverse geographic and socioeconomic regions. Using a structured query, we systematically reviewed electronic medical records of all HMO members to identify individuals with a documented diagnosis of ASD based on International Classification of Diseases (ICD) codes (the full list appears in Supplementary Table S1), between January 1990 and May 2025, yielding a total of 36,610 participants. There were no exclusion criteria. The presence of an ASD diagnosis in medical records is considered reliable and unlikely to be underreported, as it typically requires formal evaluation by two qualified professionals and is often recorded in the medical file to facilitate access to disability-related benefits.
From the full cohort, we identified individuals with ASD who had documentation of a medical cannabis prescription in their medical record and divided the sample into two groups: those with a documented prescription for medical cannabis (Cannabis-Prescribed, N = 462) and those without (Not-Prescribed, N = 36,148). A flowchart describing cohort selection is presented in Supplementary Figure S1.
Clinical and demographic variables were extracted to characterize the study groups. In line with previous research methods, all variables were retrieved using a standardized query of the Clalit Health Services electronic medical records(Shmueli et al., 2025), where such data are routinely documented in members’ medical files. Sociodemographic data included age at diagnosis and cannabis prescription, sex, population group (general Jewish population, Arab population, or ultra-Orthodox Jewish population as defined by the national registry), and socioeconomic status score (ranging from 1 [lowest] to 10 [highest], based on the national decile index assigned to the individual’s area of residence by the Central Bureau of Statistics). Clinical variables included documented comorbid neurodevelopmental diagnoses and psychotropic medication use, identified using relevant ICD and Anatomical Therapeutic Chemical codes. We defined Attention-Deficit/Hyperactivity Disorder (ADHD) as those with a formal ADHD diagnosis or those for whom stimulants were used at least three times. Among Cannabis-Prescribed individuals, we examined whether FDA-approved antipsychotic medications had been used prior to cannabis prescription, as required. Among nonprescribed individuals, we assessed whether they had ever used these medications at any point, regardless of timing.
Analysis
We compared these two groups based on demographic and clinical data using a univariate analysis. Descriptive statistics were used to summarize the characteristics of the study population. Continuous variables are presented as means and standard deviations or medians and interquartile ranges (IQR), as appropriate. Categorical variables are presented as counts and percentages. Group comparisons between the Cannabis-Prescribed and Not-Prescribed groups were performed using t-tests or Mann–Whitney U tests for continuous variables and chi-square tests for categorical variables. Data analysis was conducted using R statistical software, version 4.0.1 (R Project for Statistical Computing). All p- values were from two-sided tests, and results were deemed statistically significant at p < 0.001.
This study was approved by the Clalit Health Services Research Ethics Committee (Helsinki approval number: 0127-23-com2). The use of data from Clalit Health Services was permitted because all information was fully anonymized and therefore did not require individual informed consent.
Results
Only 1.2% of individuals with autism received medical cannabis. Table 1 presents the demographic characteristics of the study groups. The groups showed a similar gender distribution, with approximately one-quarter of each group being female, consistent with known gender patterns in autism. Individuals in the Cannabis-Prescribed group were significantly younger at the time of ASD diagnosis compared with the Not-Prescribed group (median age 3 years [IQR: 2–7] vs. 5 years [IQR: 3–9]; p < 0.001). Approximately 70% of individuals were between 5 and 18 years of age at the time of cannabis prescription, while 4.3% were younger than 5 years. The full distribution of ages is presented in Table 1. Arabs comprised 11% of the total autism cohort, already lower than their proportion in the general Clalit population (27%). Their representation was significantly lower in the Cannabis-Prescribed group, at just 2.7%, compared with 11% in the Not-Prescribed group (p < 0.001). Accordingly, the socioeconomic status of the Cannabis-Prescribed group was higher than that of the Not-Prescribed group, with a median SES score of 7.0 (IQR: 5.0–8.0) versus 6.0 (IQR: 4.0–7.0), respectively (p < 0.001).
Demographic Characteristics of the Study Groups
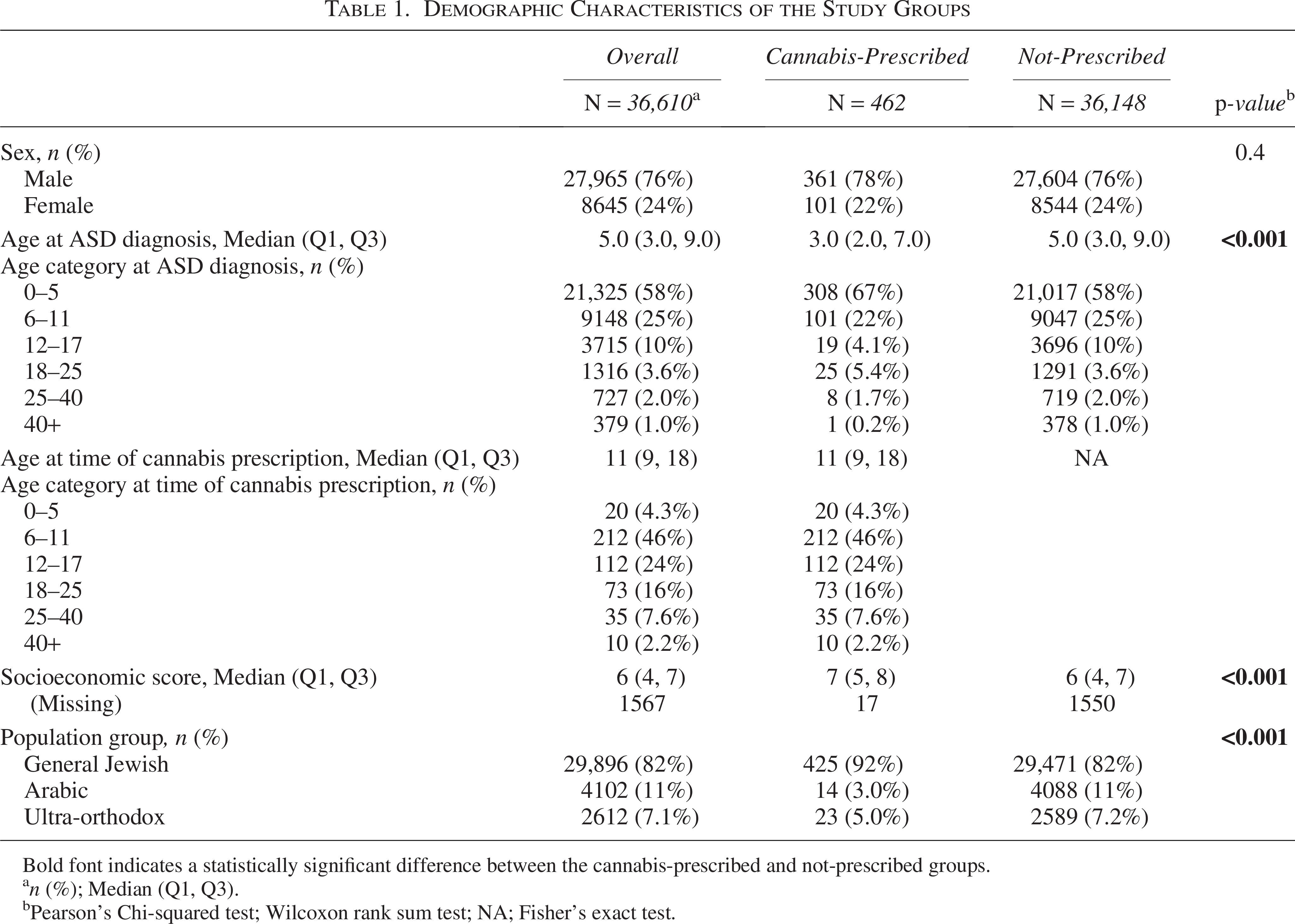
Bold font indicates a statistically significant difference between the cannabis-prescribed and not-prescribed groups.
n (%); Median (Q1, Q3).
Pearson’s Chi-squared test; Wilcoxon rank sum test; NA; Fisher’s exact test.
Table 2 presents the comorbidities among the study groups. All neurodevelopmental comorbidities—epilepsy, intellectual disability, and ADHD—were significantly more prevalent in the Cannabis-Prescribed group than in the Not-Prescribed group (14% vs. 5.8%, p < 0.001; 12% vs. 5%, p < 0.001; 42% vs. 30%, p < 0.001, respectively).
Comorbidities among the Study Groups
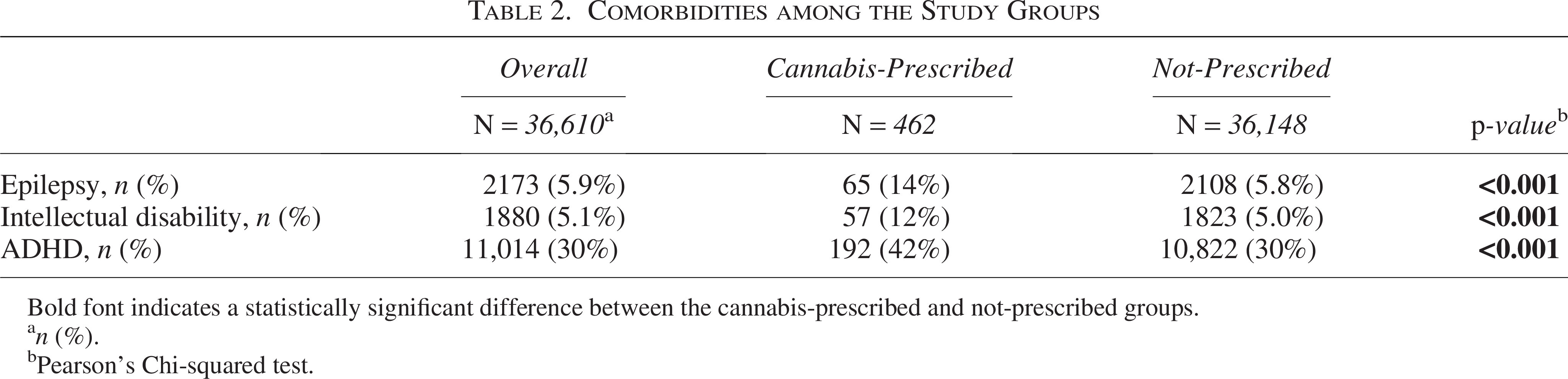
Bold font indicates a statistically significant difference between the cannabis-prescribed and not-prescribed groups.
n (%).
Pearson’s Chi-squared test.
Table 3 presents the use of FDA-approved antipsychotic medications among study groups. Among individuals prescribed medical cannabis, only 28% met the Ministry of Health criteria, having used both FDA-approved antipsychotics (Risperidone and Aripiprazole) prior to initiating medical cannabis, while 69% had used at least one. In contrast, among individuals Not-Prescribed cannabis, only 5.7% had ever used both medications, and 24% had used at least one of them.
Use of FDA-Approved Antipsychotic Medications Among Study Groups

Bold font indicates a statistically significant difference between the cannabis-prescribed and not-prescribed groups.
Median (Q1, Q3); n(%).
Wilcoxon rank sum test; Pearson’s Chi-squared test.
Discussion
To the best of our knowledge, this is the first large-scale study to examine real-world prescription patterns of medical cannabis in individuals with autism. As the prevalence of cannabis use among individuals with autism remains poorly defined in large population-based studies, we found that only a small proportion of individuals with a documented ASD diagnosis received medical cannabis. In contrast, the use of other psychotropic medications in this population is much more common, with previous studies reporting rates of up to 50% (median 18%) and high polypharmacy rates (Feroe et al., 2021; Jobski et al., 2017). These findings indicate that, although the literature on medical cannabis is expanding, its clinical use in this population remains relatively limited.
Moreover, the results consistently indicated that individuals prescribed medical cannabis tended to exhibit more severe autistic symptomatology. This was reflected in the younger age at diagnosis observed in the cannabis-treated group, consistent with prior evidence that more severe cases are typically identified earlier (Rattaz et al., 2022). This pattern was further supported by the higher prevalence of comorbid neurodevelopmental disorders—specifically intellectual disability and ADHD—among those prescribed cannabis, both of which are commonly associated with greater autism severity (Mansour et al., 2017; Rao and Landa, 2014; Vivanti et al., 2013). Epilepsy followed a similar trend to ADHD and intellectual disability, and was also more prevalent among the Cannabis-Prescribed group. This may again reflect the well-documented association between greater autism severity, comorbid epilepsy, and intellectual disability. (Ewen et al., 2019; Viscidi et al., 2013). Alternatively, the higher prevalence of epilepsy may relate to previous findings suggesting that children with both epilepsy and autism are less responsive to standard antipsychotic treatments (Pablo et al., 2023), potentially influencing the decision to initiate medical cannabis. As more severe core autistic features are often associated with greater behavioral disturbances and irritability (Anderson et al., 2011), this finding suggests that patient selection for medical cannabis treatment generally aligned with clinical guidelines-specifically, with the indication for individuals with ASD who exhibit significant behavioral disorders.
Additionally, notable demographic disparities emerged, particularly in relation to ethnicity and socioeconomic status. Although previous studies have shown that Arab individuals with autism in Israel tend to present with more severe symptoms and higher rates of comorbid intellectual disability (Levaot et al., 2019; Mahajnah et al., 2015), they were less likely to receive medical cannabis treatment. This finding contradicts the overall trend observed in the study, in which individuals with more severe presentations were more likely to be treated. These results highlight significant inequities in awareness of, and access to, medical cannabis among underserved populations.
Despite the apparent alignment between individual clinical profiles and guidelines, only about one-quarter of those prescribed cannabis had documented prior trials of the two FDA-approved antipsychotic medications. As private purchase of these medications is costly without an official HMO prescription, documentation is likely to be generally reliable. This assumption is further supported by our finding that 23% of the total cohort had use at least one antipsychotic medication, consistent with previous reports on the prevalence of antipsychotic use among individuals with autism (Jobski et al., 2017).
The relatively low rate of prior medication trials may therefore suggest that, in certain cases, clinicians considered medical cannabis earlier in the treatment course, potentially reflecting individualized clinical judgment in complex or severe presentations. Alternatively, families facing substantial behavioral and functional difficulties may have actively sought medical cannabis treatment, reflecting both growing public awareness to cannabis treatment and the challenges of managing severe symptoms, a phenomenon observed in other diagnoses as well (Gibbard et al., 2021). Such advocacy may have contributed to earlier consideration of medical cannabis by clinicians. However, when advocacy is driven by unrealistically high expectations regarding treatment outcomes, it has been shown to negatively affect adherence and long-term engagement with care (David et al., 2024). The finding that individuals prescribed medical cannabis had higher socioeconomic status may be explained by this mechanism. Families from higher socioeconomic backgrounds, often with higher educational levels, may be more aware of emerging treatment trends and more proactive in pursuing or advocating for cannabis prescriptions, even when supporting evidence remains largely anecdotal and not yet well-established.
Overall, this real-world pattern and the observed gap between clinical practice and existing guidelines—where 72% of patients received a non-proven medication before trialing well-established, evidence-based medications—are concerning. Although national guidelines require documented trials of two FDA-approved antipsychotics when applying for medical cannabis, the specific point of breakdown in the authorization process remains unclear. These findings highlight the need for stricter regulation of medical cannabis prescribing and usage processes. Moreover, they underscore the importance of carefully considering the policy and clinical implications of this trend, including continuous evaluation of prescribing practices, systematic safety monitoring, and evidence-based policy development as knowledge in this field continues to evolve.
The main strength of this study lies in the use of comprehensive, population-based data, which is rarely available in research on medical cannabis use in autism. The large sample size enables robust analysis and increases the generalizability of the findings. Importantly, as almost no large-scale data exist on real-world patterns of medical cannabis use in autism, this study provides valuable empirical insight into this understudied area.
Several limitations should be acknowledged. The cross-sectional design restricts the ability to assess temporal aspects, such as the age at treatment initiation or duration of use. In addition, information on prescription renewals was unavailable, preventing evaluation of treatment continuity or adherence over time. Details regarding cannabis formulation and dosage were also not accessible in the dataset. Finally, the observational design limits the ability to draw conclusions regarding treatment safety or efficacy. Another limitation arises from the reliance on routinely collected health records, which are subject to omissions or imprecise documentation. However, as noted above, we consider the documentation of ASD diagnoses and medication data to be generally reliable, given the administrative and regulatory requirements associated with these records.
Future research should focus on treatment trajectories, including initiation patterns, discontinuation rates, dosage changes, and potential side effects. Longitudinal studies are particularly needed to provide deeper insights into the long-term outcomes of medical cannabis use in this population and to inform evidence-based clinical guidelines.
Conclusion
Medical cannabis use among individuals with autism was rare and primarily observed in those with more severe presentations. Most prescriptions did not fully align with national guidelines requiring prior antipsychotic trials. These findings highlight a gap between policy and practice and emphasize the need for clearer regulation and monitoring. Further research is warranted to assess long-term outcomes and ensure evidence-based use.
Authors’ Contributions
H.S.: Writing—original draft (lead), conceptualization (equal), and methodology (equal). T.R.: Formal analysis (lead), data curation (lead), and software (lead). R.A.: Writing—review and editing (equal), conceptualization (equal), methodology (lead), and formal analysis (equal). D.N.: Writing—review and editing (equal) and conceptualization (equal). G.M.: Writing—review and editing (lead) and conceptualization (lead).
Footnotes
Author Disclosure Statement
The authors have no relevant competing interests to disclose.
Clinical Significance
This study provides essential real-world evidence on how medical cannabis is used in autistic individuals, helping clinicians and policymakers understand which patients receive it and under what circumstances. Clarifying and enforcing clinical indications, alongside generating long-term outcome data, will be essential for ensuring that medical cannabis is integrated safely and appropriately into autism care.
Ethics Approval
This is an observational study. The Clalit Health Services Research Ethics Committee has confirmed that no ethical approval is required.
Consent
Informed consent was waived due to the retrospective, anonymized nature of this observational study, as approved by the institutional ethics committee.
Data Availability
The data that supports the findings of this study is not openly available due to reasons of sensitivity and is available from the corresponding author upon reasonable request. Data is in controlled access storage at Clalit Health Service, Tel Aviv, Israel.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.