
Abstract
Objective:
To systematically review existing evidence on the role of gut microbiota in the pathogenesis of tic disorders (TD) and to assess the therapeutic potential of microbiome-targeted interventions such as probiotics and fecal microbiota transplantation in the management of TD.
Methods:
A comprehensive search was conducted in PubMed, Web of Science, EMBASE, and The Cochrane Library (up to May 26, 2025). The review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines and was registered in PROSPERO (CRD420251067880).
Results:
Eleven studies were included, with four focusing on gut microbiome-based therapies and seven studies with gut microbiota and its metabolites as outcome indicators. At the genus level, children with TD exhibited specific alterations in gut microbiota: increased abundance of Bacteroides, Faecalibacterium, and Ruminococcus, alongside decreased levels of Bifidobacterium and Prevotella. This functional dysbiosis may trigger neuroinflammation via disrupted short-chain fatty acid metabolism and impaired intestinal barrier function, ultimately disturbing the glutamate and γ-aminobutyric acid neurotransmitter balance and leading to dysfunction in the cortico-striato-thalamo-cortical circuit. Meanwhile, probiotics as an intervention have been consistently reported to alleviate tic symptoms, although clinical evidence remains limited.
Conclusion:
Gut microbiota may contribute to TD pathogenesis via immune modulation and neurotransmitter metabolism. While microbiota-based strategies show promise, heterogeneity and methodological limitations in current studies necessitate further high-quality research to validate mechanisms and support clinical application.
Introduction
Tic disorder (TD) is a chronic neurodevelopmental disorder with onset in childhood and adolescence, primarily characterized by involuntary, sudden, rapid, repetitive, stereotyped, and nonrhythmic motor and/or vocal tics (Szejko et al., 2022). The pathogenesis of TD remains controversial, yet it is widely recognized to involve basal ganglia dysfunction and neurotransmitter abnormalities in the cortico-striato-thalamo-cortical circuit (CSTC). Specifically, there is an elevation in excitatory neurotransmitters such as glutamic acid (Glu), aspartate (ASP), and dopamine (DA) in the striatum. Meanwhile, reduced levels or diminished activity of inhibitory neurotransmitters, including γ-aminobutyric acid (GABA) and 5-hydroxytryptamine (5-HT), are observed in the anterior cingulate cortex (Wu et al., 2025). The theory of neurotransmitter imbalance within the CSTC circuit in TD is supported by clinical pharmacological practice, neuropathological findings, and neuroimaging studies (Hao et al., 2023; Maia and Conceição, 2018).
The brain–gut axis (GBA) is a critical pathway mediating bidirectional communication between the gut and the brain, involving complex interactions among the central nervous system (CNS), autonomic nervous system, enteric nervous system, and gut microbiota (Macpherson et al., 2023; Nakhal et al., 2024). Gut microbiota play a pivotal role in maintaining brain functional homeostasis through diverse mechanisms, including the construction of intestinal barrier integrity, regulation of immune system equilibrium, and modulation of the efficacy and pharmacokinetics of certain neurotherapeutic agents. Dysregulation of the gut microbiota has been implicated in the pathogenesis of anxiety, depression, and a spectrum of neurodegenerative disorders (Nakhal et al., 2024; Vasiliu, 2023; Vendrik et al., 2020). This indicates that gut microbiota may also serve as a potential biological link in the onset and progression of TD.
This review synthesizes current clinical evidence to address three core objectives: (1) To characterize the compositional and functional alterations of gut microbiota in patients with TD; (2) To investigate the potential causal links between gut dysbiosis and tic symptom severity; (3) To evaluate the therapeutic efficacy and underlying mechanisms of microbiome-targeted interventions, including probiotic supplementation and fecal microbiota transplantation, in the management of TD. This systematic review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 2020 (Page et al., 2021) (Fig. 1).
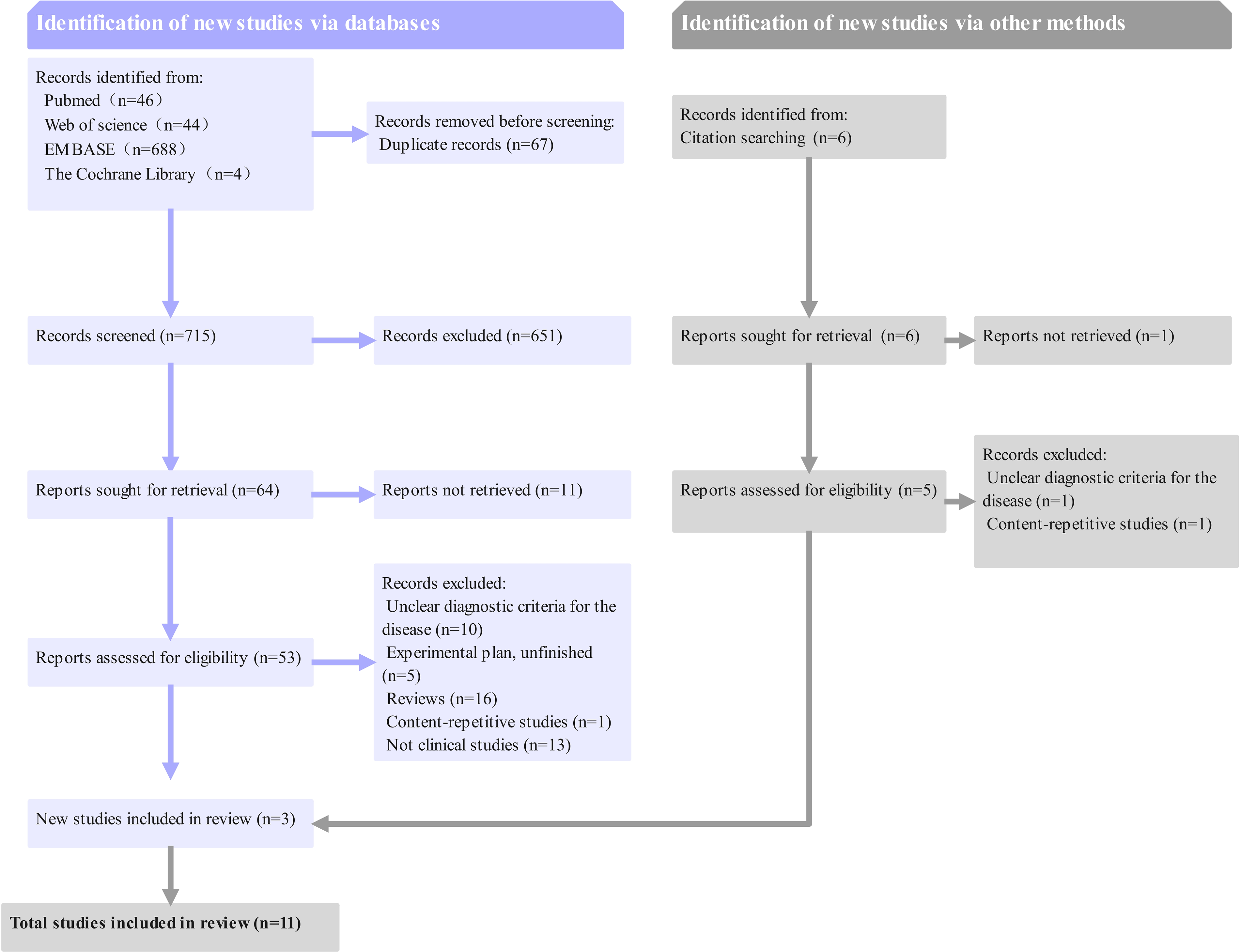
Flowchart of the systematic review.
Materials and Methods
Search strategy
A computerized search was conducted across PubMed, Web of Science, EMBASE, and The Cochrane Library databases. Based on the characteristics of each database, both MeSH subject headings and free-text terms were utilized. The core search query was formulated as follows: (tic disorder OR Tourette syndrome) AND (((intestinal OR gastrointestinal OR gut) AND microbi*) OR brain-gut axis OR short-chain fatty acid OR enteric nervous system). The publication timeframe covered all records from database inception to the present, with no language restrictions applied. The search was executed on May 26, 2025. This systematic review has been registered in the International Prospective Register of Systematic Reviews (PROSPERO), with the detailed search strategy publicly disclosed under registration number CRD420251067880.
Inclusion and exclusion criteria
Inclusion criteria
(1) Participants: Humans diagnosed with TD as defined by DSM-5. (2) At least one of the following: A. Intervention methods: Probiotics, fecal microbiota transplantation; B. Outcome measures: Gut microbiota testing, analysis of gut microbiota metabolites. (3) Study type: Clinical studies, primarily including interventional and cross-sectional studies (CSSes).
Exclusion criteria
(1) Duplicate studies. (2) Studies with unavailable full text. (3) Reviews, case reports, letters, conference abstracts, and book chapters (unless they provide original data). (4) For study protocols: If corresponding result reports are found, inclusion will be determined based on the criteria; if no reports are found, the study will be excluded.
Systematic review methodology
Literature screening protocol
All identified records from database searches were imported into EndNote reference management software for automated deduplication. Following deduplication, the remaining publications underwent relevance screening conducted independently by two investigators (Reviewer A: Bingxue Cao; Reviewer B: Chunyu Liu). The screening process comprised two phases.
Primary Screening: Titles and abstracts were examined to exclude clearly irrelevant studies. Full-text Assessment: The remaining publications advanced to full-text retrieval and detailed examination to determine final eligibility for inclusion.
During full-text review, reference lists of included studies were systematically examined to identify additional potentially relevant publications that might have been missed in the initial search strategy.
Quality assessment framework
Randomized Controlled Trials (RCTs): Assessed using the Cochrane Risk of Bias Tool version 2 (RoB 2, 2019 update). Non-randomized studies of the effects of interventions (NRSIs): Evaluated with the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) instrument. CSSes: Appraised using the Joanna Briggs Institute critical appraisal checklist.
Given the established susceptibility of gut microbiota profiles to confounding by antibiotic and probiotic exposures, this critical factor was incorporated as a specific domain within the methodological quality evaluation framework.
Information Extraction and Heterogeneity Analysis
A standardized data extraction matrix was developed using Microsoft Excel to systematically capture the following variables from included studies: Literature, research type, sample size, age (years), gender ratio, intervention, microbiome metrics, and clinical outcomes.
Statistical tests and subgroup analyses were employed to identify and quantify inter-study differences, assess gut microbiota structural variations between patients with TD and healthy children (HC), and evaluate the impact of probiotic interventions on tic symptoms. The results of heterogeneity analysis were integrated as critical evidence into the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system for overall evidence quality assessment.
All discrepancies in screening decisions or data extraction between reviewers were resolved through consensus discussions. Persisting disagreements were adjudicated by a third independent reviewer (Junwei Shi) to ensure methodological rigor.
Results
Given the significant clinical and methodological heterogeneity among the included trials, we employed a narrative descriptive synthesis to summarize the evidence, rather than conducting a quantitative meta-analysis.
Characteristics of included studies
Among the 11 studies included in this review, 3 were RCTs (Liang et al., 2025; Wang et al., 2022a; Wu et al., 2021), 5 were NRSIs (Bao et al., 2023; Chang et al., 2023; Guo et al., 2024; Zhang et al., 2024a; Zhao et al., 2020), and 3 were CSSes (Li et al., 2025; Wang et al., 2022b; Xi et al., 2021). Notably, one study was registered as a controlled trial but lacked an actual intervention component and longitudinal time span. Consequently, it was reclassified as a cross-sectional study. In terms of research focus, four studies specifically explored the application of gut microbiota interventions in children with TD (Liang et al., 2025; Wang et al., 2022a; Wu et al., 2021; Zhao et al., 2020), while seven studies examined the utilization of gut microbiota and its metabolic byproducts as outcome measures in broader clinical research contexts (Bao et al., 2023; Chang et al., 2023; Guo et al., 2024; Li et al., 2025; Wang et al., 2022b; Xi et al., 2021; Zhang et al., 2024a).
Risk of bias assessment
Risk of bias assessment results are summarized in tables (Table 1, Table 2, Table 3).
Outcomes of Quality Evaluations in RCT Studies
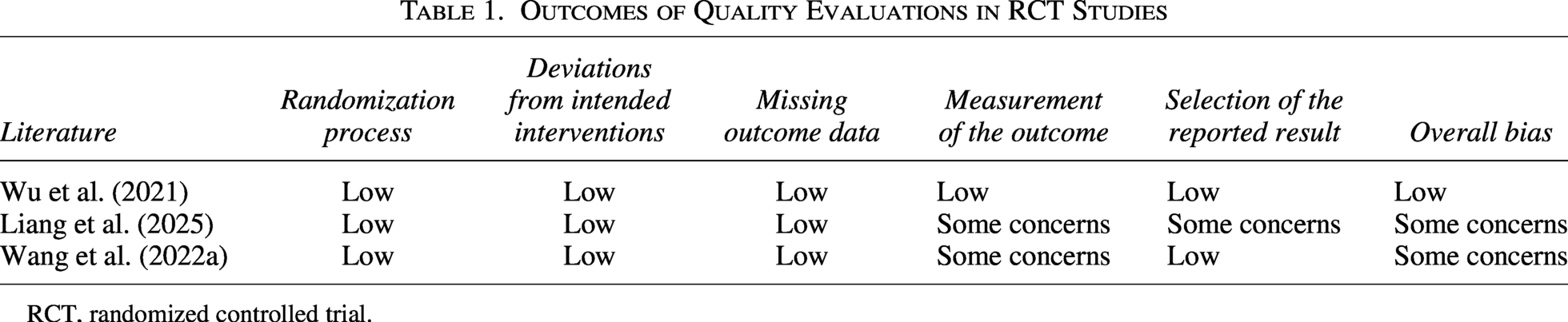
RCT, randomized controlled trial.
Outcomes of Quality Evaluations in Non-Randomized Intervention Studies
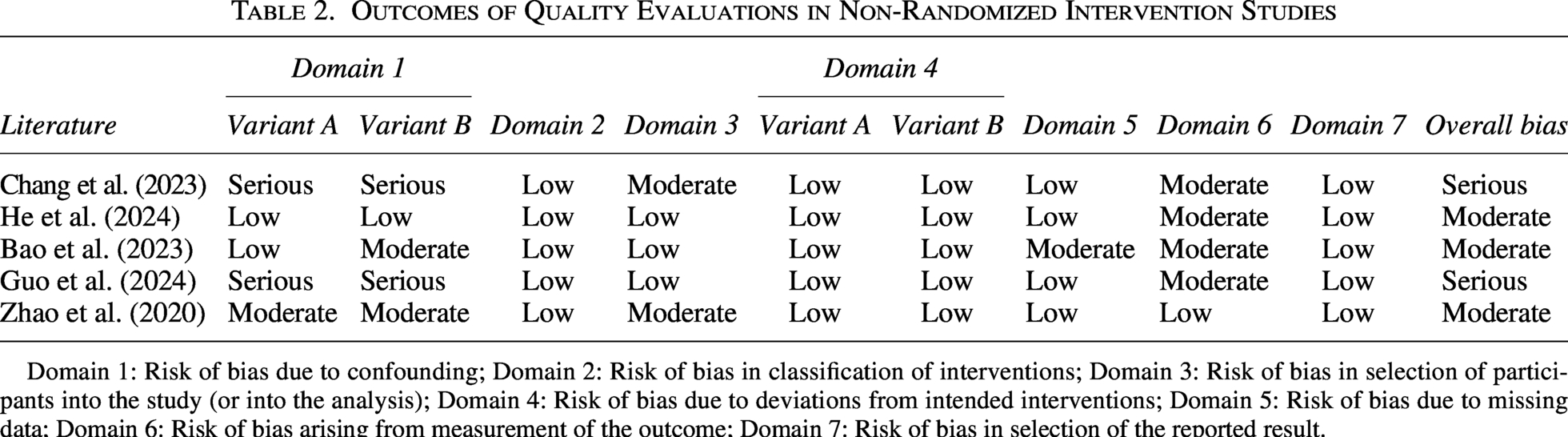
Domain 1: Risk of bias due to confounding; Domain 2: Risk of bias in classification of interventions; Domain 3: Risk of bias in selection of participants into the study (or into the analysis); Domain 4: Risk of bias due to deviations from intended interventions; Domain 5: Risk of bias due to missing data; Domain 6: Risk of bias arising from measurement of the outcome; Domain 7: Risk of bias in selection of the reported result.
Outcomes of Quality Evaluations in Cross-Sectional Studies
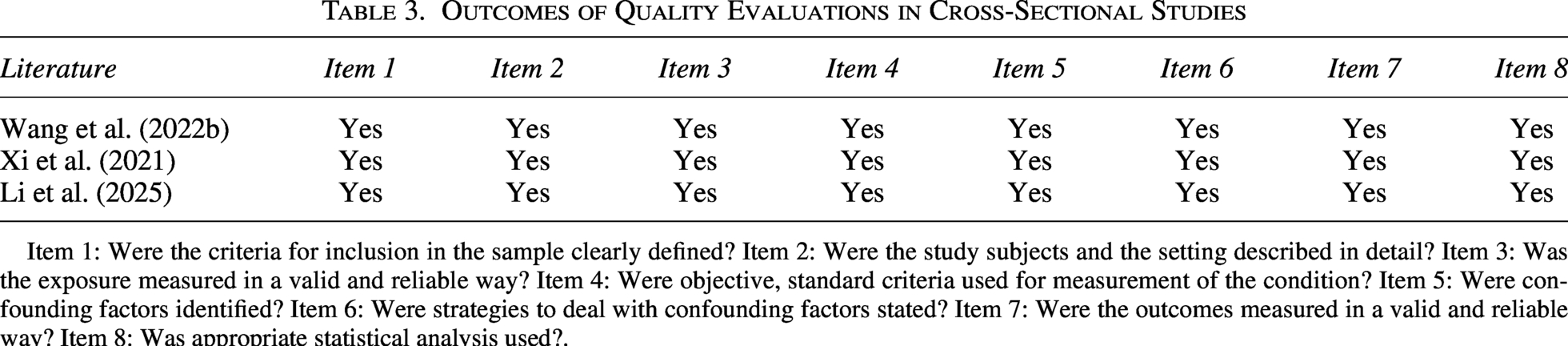
Item 1: Were the criteria for inclusion in the sample clearly defined? Item 2: Were the study subjects and the setting described in detail? Item 3: Was the exposure measured in a valid and reliable way? Item 4: Were objective, standard criteria used for measurement of the condition? Item 5: Were confounding factors identified? Item 6: Were strategies to deal with confounding factors stated? Item 7: Were the outcomes measured in a valid and reliable way? Item 8: Was appropriate statistical analysis used?.
Study data collection and heterogeneity testing
Differences in gut microbiota diversity between patients with TD and HC
Five studies included a control group of HC and all reported on α-diversity and β-diversity (Bao et al., 2023; Chang et al., 2023; Wang et al., 2022b; Xi et al., 2021; Zhang et al., 2024a). Two studies provided specific data on α-diversity, while the remaining three presented results graphically without reporting numerical values. Among the two studies with quantitative data, one reported results as medians (Zhang et al., 2024a), and the other indicated that the TD group had significantly lower microbial richness based on Chao1 (mean difference (MD) = −54.52, 95% confidence interval (CI): [−92.08, −16.96], p = 0.004), Sobs (MD = −56.67, 95% CI: [−87.53, −25.81], p = 0.0003), Ace (MD = −50.28, 95% CI: [−86.88, −13.68], p = 0.007), and Shannon (MD = −0.53, 95% CI: [−0.73, −0.33], p < 0.00001) indices; however, no statistically significant difference was observed for the Simpson index (MD = 0.02, 95% CI: [0.00, 0.04], p = 0.05). The other four studies showed no significant between-group differences in α-diversity (Bao et al., 2023; Wang et al., 2022b; Xi et al., 2021; Zhang et al., 2024a). β-diversity was assessed visually in all studies: three reported significant group differences using principal coordinates analysis (PCoA) (Bao et al., 2023; Chang et al., 2023; Wang et al., 2022b), while two found no differences—one using PCoA (Xi et al., 2021) and the other using principal component analysis (PCA) (Zhang et al., 2024a).
Current comparative studies on gut microbiota diversity between TD and HC exhibit substantial heterogeneity, primarily due to inconsistent data reporting and methodological variations. Although one high-quality study indicates significantly reduced α-diversity in the TD group, this finding has not been replicated in other studies, and results for β-diversity remain inconsistent. Therefore, the existing evidence does not support a definitive conclusion that gut microbiota diversity is consistently altered in patients with TD, and further standardized, transparent, and large-scale studies are needed to clarify this issue.
Differences in gut microbiota composition at the phylum levels between patients with TD and HC
Three studies analyzed microbial phyla (Chang et al., 2023; Wang et al., 2022b; Xi et al., 2021), focusing on three main phyla: Firmicutes, Bacteroidetes, and Actinobacteria. Two studies reported an increased relative abundance of Firmicutes in TD children (Wang et al., 2022b; Xi et al., 2021), while one study showed a decreased abundance (Chang et al., 2023). Two studies indicated a reduced relative abundance of Actinobacteria (Wang et al., 2022b; Xi et al., 2021), whereas another study found no statistically significant difference in Actinobacteria abundance between TD and HC groups before treatment but a marked increase in the TD group after effective treatment. One study reported an elevated relative abundance of Bacteroidetes.
Differences in gut microbiota composition at the genus levels between patients with TD and HC
Six studies analyzed differences at the genus level (Bao et al., 2023; Chang et al., 2023; Li et al., 2025; Wang et al., 2022b; Xi et al., 2021; Zhang et al., 2024a), and two of them discussed the relationship between disease severity and microbial abundance (Li et al., 2025; Xi et al., 2021). The most frequently mentioned genera were Bacteroides, Bifidobacterium, Faecalibacterium, Ruminococcus, and Prevotella.
Bacteroides (Bao et al., 2023; Chang et al., 2023; Xi et al., 2021), Faecalibacterium (Bao et al., 2023; Li et al., 2025; Wang et al., 2022b), and Ruminococcus (Wang et al., 2022b) showed increased relative abundance in TD children. Moreover, the abundance of Faecalibacterium (MD = 0.70, 95% CI: [0.49, 0.91], p < 0.00001) and Ruminococcus (MD = 0.73, 95% CI: [0.54, 0.92], p < 0.00001) was higher in children with severe TD than in those with mild TD. The relative abundance of Bacteroides was positively correlated with the total score of the Yale Global Tic Severity Scale (YGTSS) (R = 0.39, p = 0.005). After treatment, the abundance of these three genera decreased in TD children (Bao et al., 2023; Chang et al., 2023; Xi et al., 2021; Zhang et al., 2024a).
Bifidobacterium exhibited reduced relative abundance in TD children (Bao et al., 2023; Li et al., 2025; Wang et al., 2022b), and its abundance was lower in children with severe TD than in those with mild TD (MD = −1.41, 95% CI: [−1.71, −1.11], p < 0.00001). Prevotella showed decreased abundance in TD children (Bao et al., 2023; Xi et al., 2021), but this finding was inconsistent across studies, and no correlation with disease severity was reported (Supplementary Table S1).
Probiotic administration and YGTSS scores
YGTSS is the most widely used instrument in clinical practice for assessing tic severity. It evaluates the number, frequency, intensity, complexity, and interference of motor and vocal tics over a one-week period, reflecting their impact on daily life (Szejko et al., 2022). Three probiotic administration studies reported specific YGTSS scores but exhibited high heterogeneity among them (p = 0.0006, I2 = 86%) (Liang et al., 2025; Wang et al., 2022a; Wu et al., 2021). No statistically significant difference was found between the probiotic intervention group and the positive drug or placebo groups (standardized mean difference (SMD) = 0.25, 95% CI: [−0.55, 1.06], p = 0.54). In these three studies, the intervention in the experimental group was administered orally, but the probiotic strains and treatment durations varied, which were the main sources of heterogeneity.
Probiotic administration and SNAP-IV (parent) scores
The Swanson, Nolan, and Pelham Rating Scale, Version IV (SNAP-IV) is primarily used to assess symptoms of attention-deficit/hyperactivity disorder in children and adolescents and can also be used to evaluate symptoms of oppositional defiant disorder (Zhang et al., 2024b). Two studies used SNAP-IV as an additional outcome measure (Liang et al., 2025; Wu et al., 2021). One study collected parent-reported data (Liang et al., 2025), while the other provided data from both parents and teachers (Wu et al., 2021). When referencing the parent-reported data from the two studies, low heterogeneity was observed (p = 0.38, I2 = 0%). No statistically significant difference was found between the probiotic intervention group and the positive drug or placebo groups (SMD = −0.18, 95% CI: [−0.56, 0.19], p = 0.34).
Gut microbiota and neurotransmitters
Bifidobacterium treatment not only reduced YGTSS scores but also decreased the levels of neurotransmitters Glu and Asp (Glu: MD = 13.05, 95% CI: [11.67, 14.43], p < 0.00001; Asp: MD = 5.29, 95% CI: [3.91, 6.67], p < 0.00001) (Wang et al., 2022a). Some studies have suggested through bioinformatics analysis that alterations in gut microbiota following therapeutic intervention in children with TD and their effects on neuro-metabolic pathways such as GABA (Bao et al., 2023; Xi et al., 2021) (Table 4, Supplementary Table S2).
Summary of Findings: GRADE Assessment

Item 1: Risk of bias. Item 2: Inconsistency. Item 3: Indirectness. Item 4: Imprecision. Item 5: Publication bias. Item 6: Large effect. Item 7: Plausible confounding would change the effect. Item 8: Dose response gradient.
GRADE, Grading of Recommendations, Assessment, Development and Evaluation; HC, healthy children; SNAP-IV, Chinese version of the Swanson, Nolan, and Pelham IV scale; TD, Tic disorder; YGTSS, the Yale global tic severity scale.
Discussion
Gut microbiota characteristics in children with TD
Regarding the overall characteristics of gut microbiota in children with TD, conclusions from different studies on α-diversity, β-diversity, and phylum-level analyses are inconsistent. This inconsistency may be attributed to the lack of uniform standards in sample collection, storage, DNA extraction, sequencing platform selection, and bioinformatics analysis workflows across studies, which affects the comparability and reproducibility of research results.
However, some more consistent trends have been observed at the genus level. Multiple studies have shown that the relative abundances of Bacteroides, Faecalibacterium, and Ruminococcus in the gut microbiota of TD children are increased, while the relative abundances of Bifidobacterium and Prevotella are decreased. This phenomenon suggests that gut microbiota alterations associated with TD may be more prominently reflected in the imbalance of these key functional genera rather than in macroscopic changes in the overall community structure.
Dysregulation of short-chain fatty acid metabolism and barrier injury
Ruminococcus is one of the most important butyrate-producing bacterial families in the gut, while Prevotella is a core gut microbiota that ferments dietary fibers to produce short-chain fatty acids (SCFAs), with a predominant role in propionate synthesis. These SCFAs serve not only as the primary energy source for colonic epithelial cells but also as key substances that maintain the structural integrity of the intestinal barrier (Calzadilla et al., 2022; Fusco et al., 2023; Liu et al., 2024).
In addition to their local effects in the gut, SCFAs can enter the bloodstream through the portal venous circulation or lymphatic system. Some small-molecular-weight SCFAs can cross the blood–brain barrier (BBB) and directly act on the CNS (Fusco et al., 2023). Butyrate and propionate inhibit histone deacetylases and activate G protein-coupled receptor 43, thereby promoting the differentiation and function of regulatory T (Treg) cells and suppressing excessive inflammation (Fock and Parnova, 2023; Fusco et al., 2023; Zhang et al., 2023). In a TD mouse model, characteristic alterations in intestinal barrier dysfunction have been observed: the expression levels of tight junction proteins ZO-1, Occludin, and Claudin-1 in the intestinal mucosa are significantly downregulated, accompanied by severe dysbiosis of the gut microbiota (Zhu et al., 2026). Combining clinical research findings, it is speculated that changes in the abundance of key SCFA-producing bacterial genera in the gut of TD children may reduce the synthesis of protective SCFAs, weaken their anti-inflammatory effects and barrier-maintaining functions, and thus create pathological conditions for intestinal barrier injury and the subsequent development of neuroinflammatory responses.
Intestinal barrier injury and neuroinflammation
Disruption of the intestinal barrier facilitates the translocation of pathogenic factors into the bloodstream. Pathogen-associated molecular patterns and microbe-associated molecular patterns are recognized by pattern recognition receptors (PRRs). This activation triggers the excessive secretion of pro-inflammatory cytokines, including IL-1β, IL-6, and TNF-α (Fusco et al., 2023; Liu et al., 2024; Wei et al., 2023). Pro-inflammatory cytokines directly act on cerebrovascular endothelial cells, leading to downregulation of tight junction proteins and compromising the selective permeability of the BBB. This barrier dysfunction subsequently activates microglia and astrocytes, initiating neuroinflammatory cascades (Liddelow et al., 2017; Ortiz-Samur et al., 2025; Zhao et al., 2021). The excessive activation of microglia further amplifies the release of pro-inflammatory mediators, exacerbating oxidative stress, neuronal apoptosis, and consequent brain tissue damage (Ortiz-Samur et al., 2025). Administration of SCFAs corrects microglial morphological and functional abnormalities in germ-free mice, exerting neuroprotective effects through dual modulation of TNF-α suppression and IL-10 upregulation (Jameson et al., 2020; Patnala et al., 2017). Among them, butyrate can specifically inhibit the NF-κB signaling pathway, thereby blocking the cascade amplification effect of pro-inflammatory factors (Fock and Parnova, 2023).
Gut microbiota and its metabolites can modulate the Glu/GABA balance
Glu is the primary excitatory neurotransmitter in the CNS, exerting excitatory effects by binding to receptors on postsynaptic neurons. However, excessive accumulation of Glu in the synaptic cleft induces neurotoxicity. GABA is an inhibitory neurotransmitter that binds to GABA receptors on postsynaptic neurons, regulates the opening state of ion channels, promotes membrane hyperpolarization, thereby reducing neuronal excitability, and plays a crucial role in modulating human emotions and excitatory behaviors (Hao et al., 2023; Xu et al., 2025).
In patients with TD and animal models, Glu levels in the extracellular fluid of the striatum/caudate putamen and plasma are significantly elevated, while GABA levels show a decreasing trend (Fan et al., 2025; Hao et al., 2023; Wang et al., 2025). Moreover, the degree of Glu elevation in the striatum is positively correlated with the severity of tics (Hao et al., 2023). This imbalance between the two key neurotransmitters disrupts the flux of the Glu/GABA-Gln metabolic cycle, which uses glutamine (Gln) as an intermediate metabolite, leading to excitatory amino acid neurotoxicity. This subsequently causes degeneration and death of dopaminergic neurons in the striatum, ultimately triggering TD (Hao et al., 2023; Xu et al., 2025).
Studies have shown that exogenous GABA can alleviate tic-like behaviors in TS model rats by modulating gut microbiota composition and restoring the GABA-Glu metabolic balance in the striatum (Xu et al., 2025). Preliminary clinical studies included in this review have found an association between Bifidobacterium and Glu, Asp levels. Although current research on GABA is mostly based on indirect evidence such as bioinformatics analysis, and the conclusions require further validation, the complex interactions between the Glu/GABA system and its cross-talk with the dopamine system remain central to understanding the dysfunction of the CSTC circuit that leads to tics (Fig. 2).
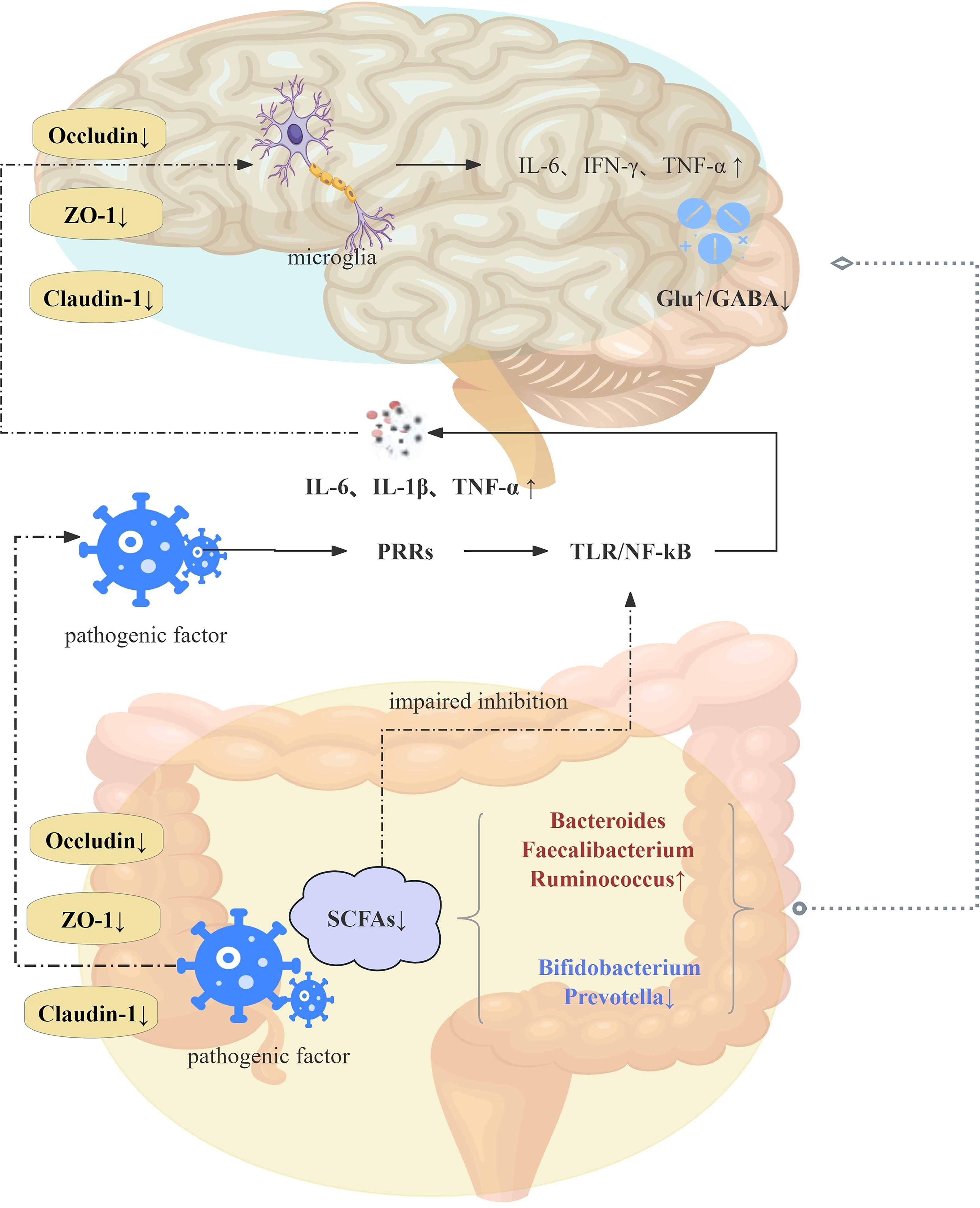
Proposed mechanisms of gut microbiota in tic disorders. SCFAs: short-chain fatty acids, PRRs: pattern recognition receptors, Glu: glutamic acid, GABA: γ-aminobutyric acid.
Efficacy of probiotic intervention: preliminary exploration and uncertainties
Within the studies included in this review, both fecal microbiota transplantation (FMT) and specific probiotic strains (e.g., Limosilactobacillus reuteri, PS128, and Bifidobacterium triple viable powder) demonstrated efficacy in alleviating tic symptoms, though with notable variations in their underlying mechanisms and duration of therapeutic effects (Liang et al., 2025; Wang et al., 2022a; Wu et al., 2021; Zhao et al., 2020). Emerging research further delineates the intricate associations between gut microbiota interventions and neurotransmitter modulation, as well as inflammatory pathways (Wang et al., 2022a; Zhao et al., 2020), providing critical mechanistic insights into the role of the GBA in neuropsychiatric disorders. A systematic analysis and evaluation were conducted to assess the effects of probiotics as an intervention on core symptoms of TD (YGTSS score) and comorbid symptoms (assessed by SNAP-IV). Currently, limited evidence does not support the notion that a single probiotic formulation can universally and significantly improve tic symptoms or common comorbid symptoms in children with TD. This conclusion does not negate the potential effectiveness of microbiota-based intervention strategies, but rather suggests that future research needs to design more rigorous RCTs with larger sample sizes, and provide detailed reports on key parameters such as the specific strains of probiotics used, intervention dosage, and treatment duration, in order to obtain more reliable evidence-based medical data.
Limitations
Study design and causal inference
Included studies vary widely in design and quality. Two high-risk NRSIs failed to control confounders (e.g., antibiotic/probiotic use), undermining causal inference reliability. CSSes can only reveal associations, not causal relationships, between microbial changes and TD.
Protocol heterogeneity and evidence quality
Significant inconsistencies in treatment protocols (e.g., probiotic strains and dosages) across studies impede direct effect comparisons. The overall body of evidence was rated as very low to moderate certainty using the GRADE framework.
Sample representativeness and generalizability
All samples were sourced exclusively from China, mostly from local populations. Geographic and dietary influences on gut microbiota may limit the generalizability of findings to other populations.
Data depth and functional inference
Current evidence relies primarily on 16S rRNA sequencing, providing only taxonomic profiles. Inferences about microbial function remain indirect; multi-omics approaches (metagenomics, metabolomics) are needed for direct validation.
Systematic search limitations
Despite adhering to PRISMA guidelines, evolving microbiome terminology may have caused retrieval bias, potentially missing studies using nonstandard or highly specific terms.
In summary, findings from this review should be interpreted with caution. While holding significant reference value for future research, they are suggestive rather than definitive evidence, constrained by methodological limitations, heterogeneity, and limited generalizability.
Future Directions
To advance understanding of the GBA in TD and accelerate clinical translation, future research should prioritize the following key directions:
Clarify causal relationships
Conduct large-scale, multicenter prospective cohort studies to establish temporal associations between gut microbiota alterations and the onset/progression of TD, addressing the limitations of cross-sectional designs in inferring causality.
Standardize research methodologies
Develop consensus-based standardized research protocols, including unified core outcome measures (e.g., YGTSS scores, validated microbiota profiling techniques) and shared data platforms, to enhance comparability across studies and facilitate meta-analyses.
Facilitate clinical trial participation
Encourage eligible patients with TD to enroll in ongoing clinical trials investigating microbiome-targeted interventions (e.g., probiotics, fecal microbiota transplantation), while ensuring transparent communication about the exploratory nature of such treatments.
Deepen mechanistic insights
Employ integrated multi-omics approaches (metagenomics, metabolomics, metatranscriptomics) combined with functional validation models (e.g., germ-free mice, organoid systems) to elucidate the specific roles of key bacterial genera (e.g., Ruminococcus, Faecalibacterium, Prevotella, Bifidobacterium) and their metabolites (e.g., SCFAs) in TD pathophysiology.
Accelerate clinical translation
Translate mechanistic findings into clinical applications, including the development of microbiota-based biomarkers for early diagnosis and subtype classification and the validation of safe, effective microbiota-modulating therapies for TD.
Integrate gut health into clinical practice
Incorporate assessment of dietary patterns and gastrointestinal symptoms into routine clinical evaluations of patients with TD, recognizing their potential as modifiable factors influencing both gut microbiota and tic severity.
Authors’ Contributions
B.C.: Writing—original draft, funding acquisition, visualization, and data curation. X.Z.: Writing—review and editing. X.C.: Writing—review and editing. J.S.: Data curation. C.L.: Data curation. B.Y.: Validation.
Footnotes
Disclosures
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.