
Abstract
Objectives:
This study aimed to describe changes in psychotropic medication use over time in commercially insured children with autism spectrum disorder (ASD) across age groups and characterize the comorbidity burden in patients with more complex treatment regimens.
Methods:
Using deidentified administrative claims from the Workpartners Research Reference Database, we conducted a retrospective cohort study of employee dependents aged 0–17 years with ASD followed for 3 years. Psychotropic medication use was analyzed across three age groups (0–4, 5–9, and 10–17 years). In a subgroup with high treatment complexity, defined as polypharmacy (≥3 drug classes) and/or antipsychotic use, the prevalence of various co-occurring conditions associated with ASD was also described.
Results:
Among 2747 children with ASD, psychotropic medication use and polypharmacy were more common in older age groups. At Year 1, 32.8% of children aged 10–17 used ≥2 drug classes concurrently, compared with 0.9% and 15.3% in the 0–4 and 5–9 age groups, respectively. From Year 1 to Year 3, medication use increased in younger children but declined in the 10–17 age group. High treatment complexity was observed in 20.5% of children (n = 562) over the entire 3-year study period, most frequently in the 10–17 age group. A higher prevalence of comorbidities, including attention-deficit hyperactivity disorder, mental health conditions, conduct disorders, and irritability and agitation, was observed in those with high treatment complexity compared with those without.
Conclusions:
Pharmacologic treatment patterns varied by age in children with ASD, and higher treatment complexity was associated with more frequent diagnoses of co-occurring psychiatric and behavioral conditions. Further understanding of longitudinal treatment trajectories should be explored in future research, such as by contextualizing treatment changes with symptom assessment and evaluating the social impact of treatment complexity.
Introduction
Autism spectrum disorder (ASD) is a common neurodevelopmental disorder characterized by the core deficits in social communication and interactions and restrictive, repetitive patterns of behavior (Hyman et al., 2020). Standardized screening for ASD begins as early as 18 and 24 months of age (Hyman et al., 2020), and clinical presentation of features can vary largely across ages and developmental stages (Shulman et al., 2020). Children with ASD may receive psychotropic medication treatment and/or nonpharmacological interventions for the management of core ASD symptoms and co-occurring behavioral challenges (Hyman et al., 2020). Currently, only risperidone and aripiprazole are Food and Drug Administration (FDA)-approved for irritability associated with ASD. However, various pharmacotherapy options are available for managing common co-occurring conditions such as attention-deficit hyperactivity disorder (ADHD), anxiety, mood disorders, sleep disorders, and seizures, as well as behavior challenges such as aggression, irritability, and self-injurious behavior (Hyman et al., 2020; Manter et al., 2025). As a result, children with ASD may be treated with multiple drug classes over time: Polypharmacy, generally defined as the use of at least two or three drug classes in the context of ASD treatment, has been reported to vary in 6.8%–87% of children with ASD (Ritter et al., 2021). The use of multiple psychotropic medications not only elevates pill burden and adherence challenges in children but can also increase the risk of side effects and drug–drug interactions, highlighting the importance of comprehensive analysis of treatment patterns in this population. However, nonpharmacological treatment options include educational practices, developmental therapies, and behavioral interventions, such as applied behavior analysis (Hyman et al., 2020). Psychotropic medication use patterns may thus also be influenced by patient access and response to psychosocial services and behavioral interventions (Wiggins et al., 2021).
Although several previous U.S. insurance claims studies have characterized psychotropic treatment patterns in youths with ASD, many utilized cross-sectional designs, examining different cohorts of children in different calendar years (Feroe et al., 2021; Plourde et al., 2024; Rast et al., 2025), or utilized limited data from a single year (Houghton et al., 2017). Few studies have compared the longitudinal changes in prescription patterns following a cohort of children with ASD. One Canadian study following individuals with ASD from initial diagnosis reported an increase in psychoactive drug use between the first and fifth year since diagnosis across all pediatric age groups under the age of 18, but it did not distinguish different drug classes and may not reflect the prescribing practice in the United States (Croteau et al., 2019). In the United States, a claims analysis of newly diagnosed individuals with 3 years of follow-up reported that pharmacotherapy options varied highly and therapy switching was common, with some individuals advancing through four lines of therapy within the 3 years (Shoaib et al., 2022). Although this study described subsequent lines of therapy, the study did not characterize the duration of each therapy change, creating a gap in evidence regarding the overall medication pattern at different timepoints since diagnosis.
To build on limitations of previous studies and further evaluate the medication use in ASD treatment, this study aimed to describe the 3-year changes in medication use in different age groups of children with ASD based on a sample of commercially insured dependents of employees in the United States. Additionally, as polypharmacy is associated with disruptive features such as self-injurious behaviors, physical aggression, and psychiatric comorbidities (Ritter et al., 2021), a secondary objective was to characterize treatments in a subgroup of patients with higher treatment complexity, defined as polypharmacy or antipsychotic use, and the prevalence of co-occurring conditions in this subgroup.
Methods
Data source and study population
This study utilized administrative data from the Workpartners Research Reference Database, a propriety database containing deidentified medical and prescription claims data of over 3.5 million employees and their covered dependents as well as employment information such as job type, employment status, salary, and company type (Judy et al., 2024). The database includes over 500 private sector employers in a variety of industries, including health care, insurance, retail, manufacturing, technology, and energy, across 50 states in the United States.
Minor dependents of employees were included if they had two medical claims with an International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM) diagnosis code of F84.0 (autistic disorder) between January 1, 2016, and December 31, 2023. The first claim with diagnosis code F84.0 was defined as the index claim. Dependents were required to have 3 years of continuous data post-ASD diagnosis within the study timeframe to minimize misclassification bias of medication utilization patterns due to incomplete claims data. Supplementary Figure S1 summarized the study design. Psychotropic medication utilization patterns in the 3-year postindex period were characterized in three groups of patients, aged 0–4 years, 5–9 years, and 10–17 years at baseline.
Baseline characteristics
Demographic information and characteristics of the employee and dependents included age at the time of diagnosis, race, gender, geographic region, salary (inflation-adjusted to 2023 U.S. dollars), and full-time/part-time status. Baseline clinical characteristics were also evaluated in the preindex period of up to 12 months, including psychotropic medication use and prevalence of six prespecified co-occurring conditions: ADHD (ICD-10-CM code, F90.x), anxiety disorder (F40.x and F41.x), conduct disorder (F91.x), depressive disorder (F32.x and F33.x), bipolar disorder or other mood disorders (F30.x, F31.x, F34.x, and F39.x), seizure disorder (G40.x and R56.x), and sleep disorder (G47.x and F51.x).
Psychotropic medication use
Six psychotropic drug classes were evaluated, including (1) antipsychotics, (2) anti-seizure medications including benzodiazepines, (3) antidepressant/anxiolytic agents, (4) alpha agonists, (5) stimulants, and (6) sleep medications. Pharmacy claims for these drug classes were characterized in each age group at Year 1 (baseline to first year postindex), Year 2 (first to second year postindex), and Year 3 (second to third year postindex). Different drug classes with at least 30 days of prescription overlap were considered concurrent use.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) categorizes ASD into three severity levels, with the highest level described as “requiring very substantial support” and the lowest level “requiring support” (American Psychiatric Association, 2022). The severity defined by DSM-5-TR is based on severity of core symptoms in diagnostic criterion A, social communication impairment, and criterion B, restricted, repetitive patterns of behavior (American Psychiatric Association, 2022). However, since ASD severity cannot be captured directly with claims data and ICD-10-CM codes alone, we chose a subgroup of children with high medication burden (polypharmacy of three or more psychotropic medications) and/or those treated with antipsychotics as a surrogate for patients exhibiting greater overall neuropsychiatric and behavioral complexity. We chose this composite definition as we hypothesized that patients receiving multiple psychotropic drugs likely experienced multiple co-occurring psychiatric or behavioral conditions, given that polypharmacy has been associated with self-injurious behaviors, physical aggression, and psychiatric comorbidities (Ritter et al., 2021). Moreover, antipsychotic use could potentially suggest irritability, aggressive behavior, and self-injurious behavior since it is the only drug class approved by the FDA, recommended by the American Academy of Pediatrics for the treatment of irritability and severe disruptive behavior (Hyman et al., 2020), and supported by randomized trials demonstrating the efficacy of risperidone and aripiprazole for these symptoms (McCracken et al., 2002; Owen et al., 2009). In addition, patients with polypharmacy also face increased risks of drug–drug interactions and adverse effects, underscoring the clinical relevance of this subgroup. It is important to note that this subgroup based on pharmacological complexity was not intended to be a direct proxy of autism severity defined by the severity of impairment in core diagnostic domains outlined by the DSM-5-TR, which is based on direct assessment of social communication and restricted, repetitive patterns of behavior. Rather, we hypothesized that this group of individuals has high clinical complexity, reflected by cumulative management of multiple co-occurring symptom domains. We acknowledge that polypharmacy and/or antipsychotics use may also be used in those with greater severity of core diagnostic symptoms, but since insurance claims data do not capture data on severity assessment data, our analysis focused on characterizing comorbidity burden.
Prior studies have defined polypharmacy in autism as at least two or three drug classes used concurrently (Ritter et al., 2021). The rates of patients using at least two drug classes were reported to be 35%–53% depending on study design and patient sample variability (Houghton et al., 2017; Logan et al., 2015; Martin et al., 1999). Given this high prevalence, defining polypharmacy as two or more drug classes would likely capture a subset of patients that is too broad and heterogeneous to meaningfully reflect clinical complexity. However, a threshold of four or more drug classes was rarely used in existing literature and would likely reduce the sample size substantially. We, therefore, selected concurrent use of at least three drug classes, consistent with prior studies (Madden et al., 2017; Mandell, 2008; Rosenberg et al., 2010), to better identify patients with higher clinical complexity while keeping an adequate sample size.
Therefore, the clinical characteristics of a subgroup of dependents using any antipsychotic or at least three concurrent drug classes were explored by identifying the prevalence of co-occurring psychiatric and behavioral conditions, including conduct disorder, irritability, and agitation associated with ASD, compared with those who do not fall within this subgroup. These co-occurring conditions were identified by the presence of at least one ICD-10-CM code for the corresponding condition during the study period (Supplementary Table S1). We also conducted a sensitivity analysis using alternative definitions based on antipsychotic use alone, polypharmacy alone, and requiring both criteria (antipsychotics and polypharmacy) with results reported in the Supplemental Data.
Statistical analysis
Descriptive statistics were used to summarize medication use patterns (including combinations of medications) and characteristics of the study population. The proportion of patients using concurrent drug classes was compared across the three age groups using a chi-squared test. Pairwise comparisons between 0–4 years and 5–9 years and between 5–9 years and 10–17 years age groups were performed using two-sample z test for proportions. Within each age group, the proportions of patients using no versus at least one psychotropic drug class were also compared between Year 1 and Year 3 using the McNemar test. The statistical significance threshold of p values was adjusted for multiple comparisons using Bonferroni correction.
Results
Baseline characteristics
A total of 2747 children with ASD met inclusion criteria in the final sample based on diagnostic and three-year postindex continuous enrollment requirements, with 77.5% male and a mean age of 9.3 years at the first diagnosis (Table 1). The majority of children were under the age of 10, with 23.3% aged 0–4 years, 32.5% aged 5–9 years, and 44.2% aged 10–17 years. Race information was only available for 42.4% of the employees, of which the majority was white (26.5% of the entire sample). Most employees with dependents included in this analysis held full-time employment (88.4%) and had a mean annual salary of $125,404 (adjusted to 2023). The most common co-occurring conditions at baseline were ADHD (20.2%) and anxiety disorder (12.7%). Stimulants, antidepressants/anxiolytics, and alpha agonists were used in 17.2%, 13.4%, and 12.3% of patients, respectively, at baseline.
Baseline Characteristics of Dependents and Employees

Concurrent use of multiple drug classes
At Year 1, more children in the older age groups were treated with psychotropic medications and multiple concurrent psychotropic classes (Fig. 1). In the youngest age group of 0–4 years, the majority (90.3%) were not treated with any psychotropic medication in Year 1. However, the older age groups 5–9 years and 10–17 years, had a larger proportion of children with ASD using at least 1 psychotropic medication: In the 5–9 age group, 15.3% used two or more medication classes concurrently in Year 1, and this number increased to 32.8% in the 10–17 years age group. At Year 1, the proportions of children with at least two or more concurrent medications were significantly different between the 10–17 age group and 5–9 age group (p < 0.000001) and between the 5–9 age group and 0–4 age group (p < 0.000001).
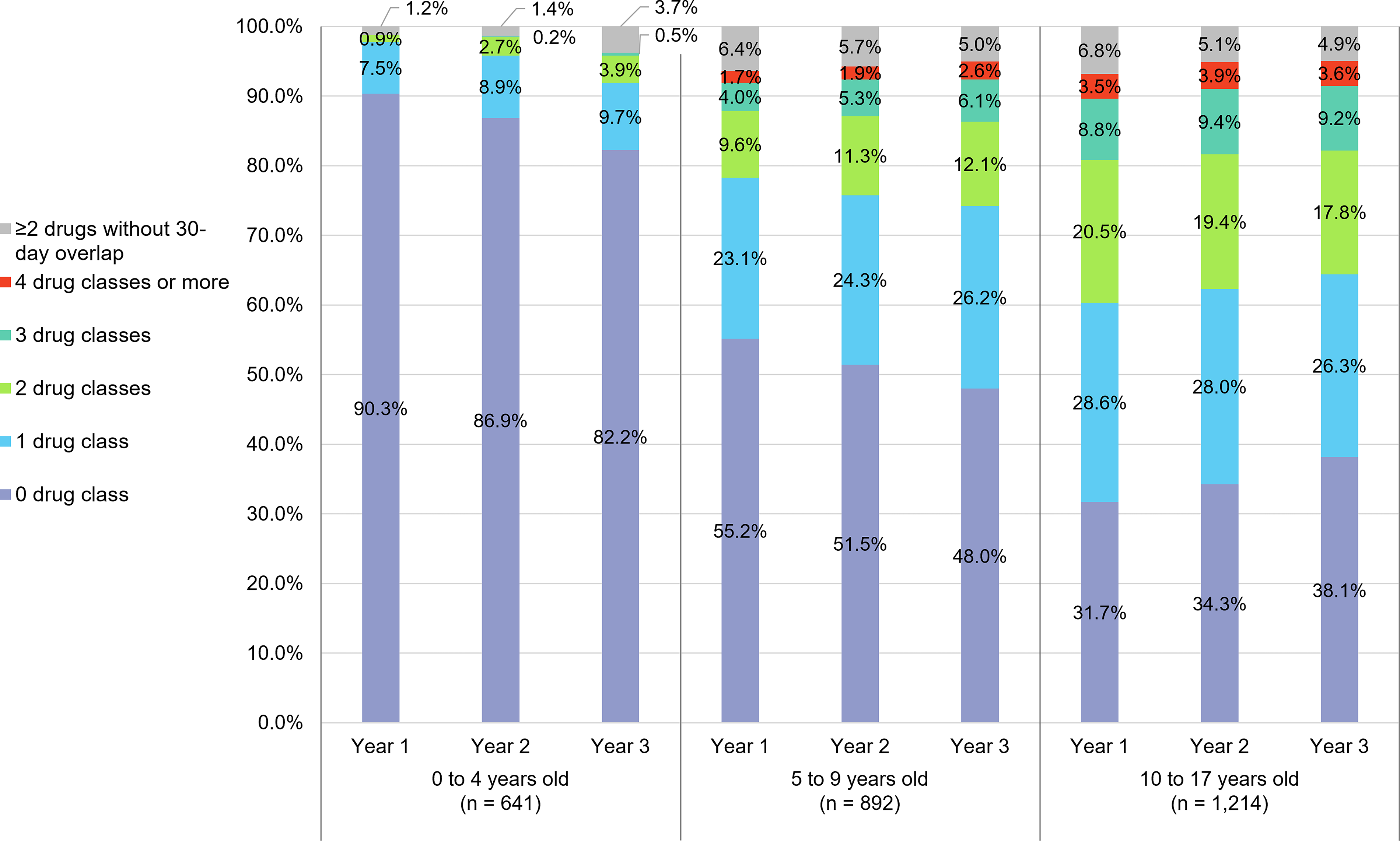
Percentage of children using different numbers of concurrent drug classes.
From Year 1 to Year 3, an increase in medication utilization was observed in the 0–4 and 5–9 age groups (Fig. 1 and Supplementary Table S2). The proportion of those using at least 1 drug class increased from 9.7% to 17.8% from Year 1 to Year 3 in the 0–4 age group (p < 0.000001). The proportion of those using at least 2 concurrent drug classes increased from 15.3% to 20.8% from Year 1 to Year 3 in the 5–9 age group (p < 0.000001). However, this trend was reversed in the 10–17 age group, where the proportions of adolescents with ASD treated with at least 1 medication reduced from 68.3% to 61.9% (p = 0.000001).
Utilization by drug class and drug type
At Year 1, the most commonly used drug classes in the 5–9 and 10–17 age groups were stimulants, alpha agonists, and antidepressants/anxiolytics (Fig. 2 and Table 2). The use of stimulants and alpha agonists was comparable between the age groups, with 28.3% stimulant use and 20.2% alpha agonist use in 5–9 years compared with 34.0% stimulant use and 24.1% alpha agonist use in the 10–17 age group. However, the use of antidepressants/anxiolytics saw a large difference between the 5–9 age group (12.4%) and the 10–17 age group (34.8%). Antipsychotic and anti-seizure medication use was also more common in the 10–17 age group. When comparing the temporal changes, utilization of all six drug classes increased from Year 1 to Year 3 in the 0–4 and 5–9 age groups. In contrast, between Year 1 and Year 3, in the 10–17 age group, the use of stimulants, alpha agonists, and antipsychotics declined from 34.0% to 28.4%, from 24.1% to 21.5%, and from 20.8% to 18.9%, respectively, but the use of antidepressants/anxiolytics, anti-seizure medications, and sleep medications remained stable. At Year 1, the most used drug agents were methylphenidate (11.7%), guanfacine (10.8%), sertraline (7.8%), clonidine (7.0%), and amphetamine-dextroamphetamine (6.6%; Table 2). The most used antipsychotics were risperidone (5.8%) and aripiprazole (5.6%). The most common combinations of drug classes were combinations of the most utilized drug classes, including stimulants + antidepressants/anxiolytics (n = 201), stimulants + alpha agonists (n = 180), antidepressants/anxiolytics + alpha agonists (n = 178), and antidepressants/anxiolytics + antipsychotics (n = 148; Supplementary Table S3).
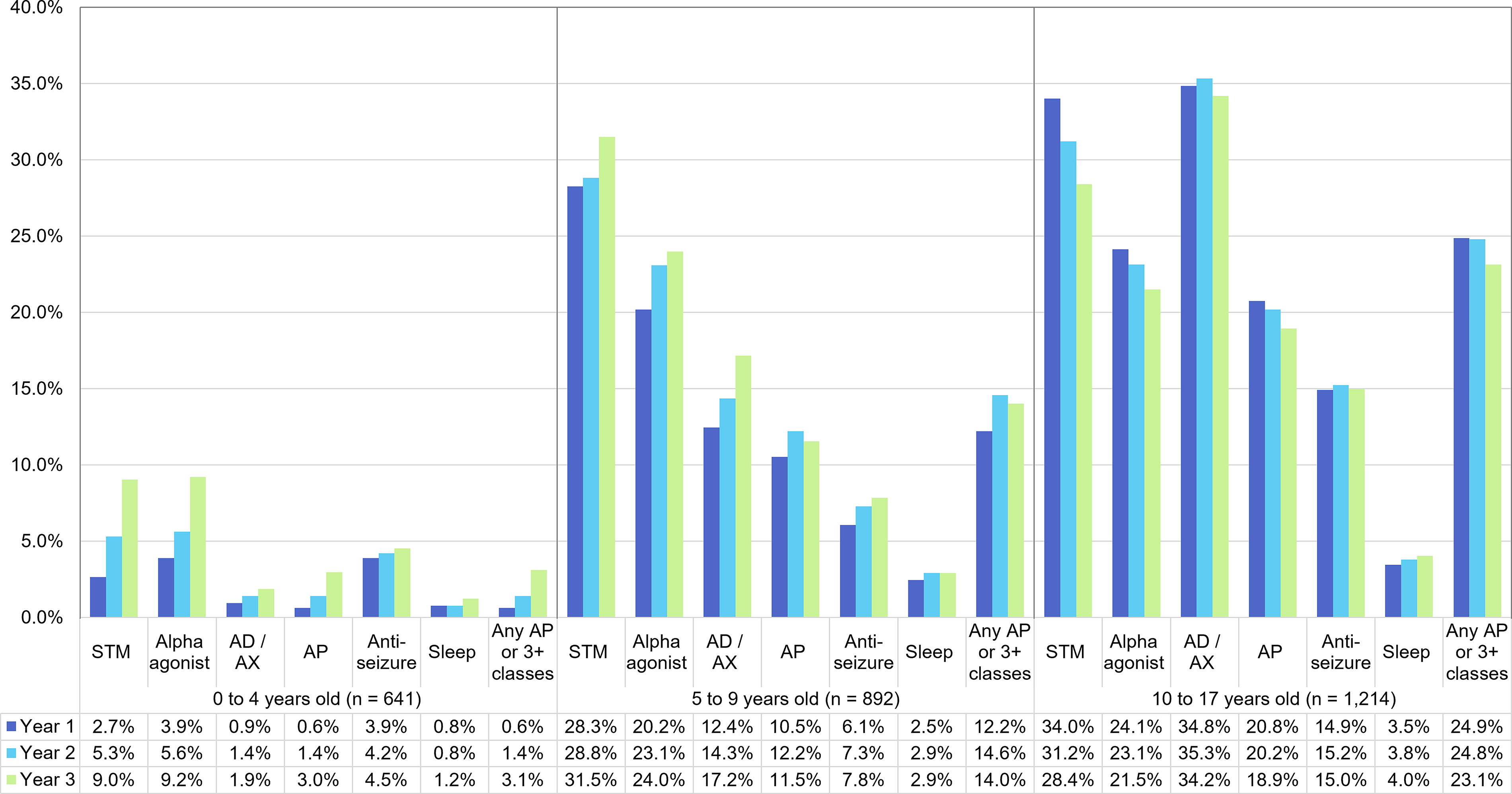
Percentage of children using stimulants, alpha agonists, antidepressants/anxiolytics, antipsychotics, anti-seizure medications, and sleep medications and the use of any antipsychotic or three or more concurrent drug classes in Year 1 to Year 3. AD/AX, antidepressant/anxiolytic; AP, antipsychotic; STM, stimulant.
Psychotropic Medication Utilization by Drug Class at Year 1
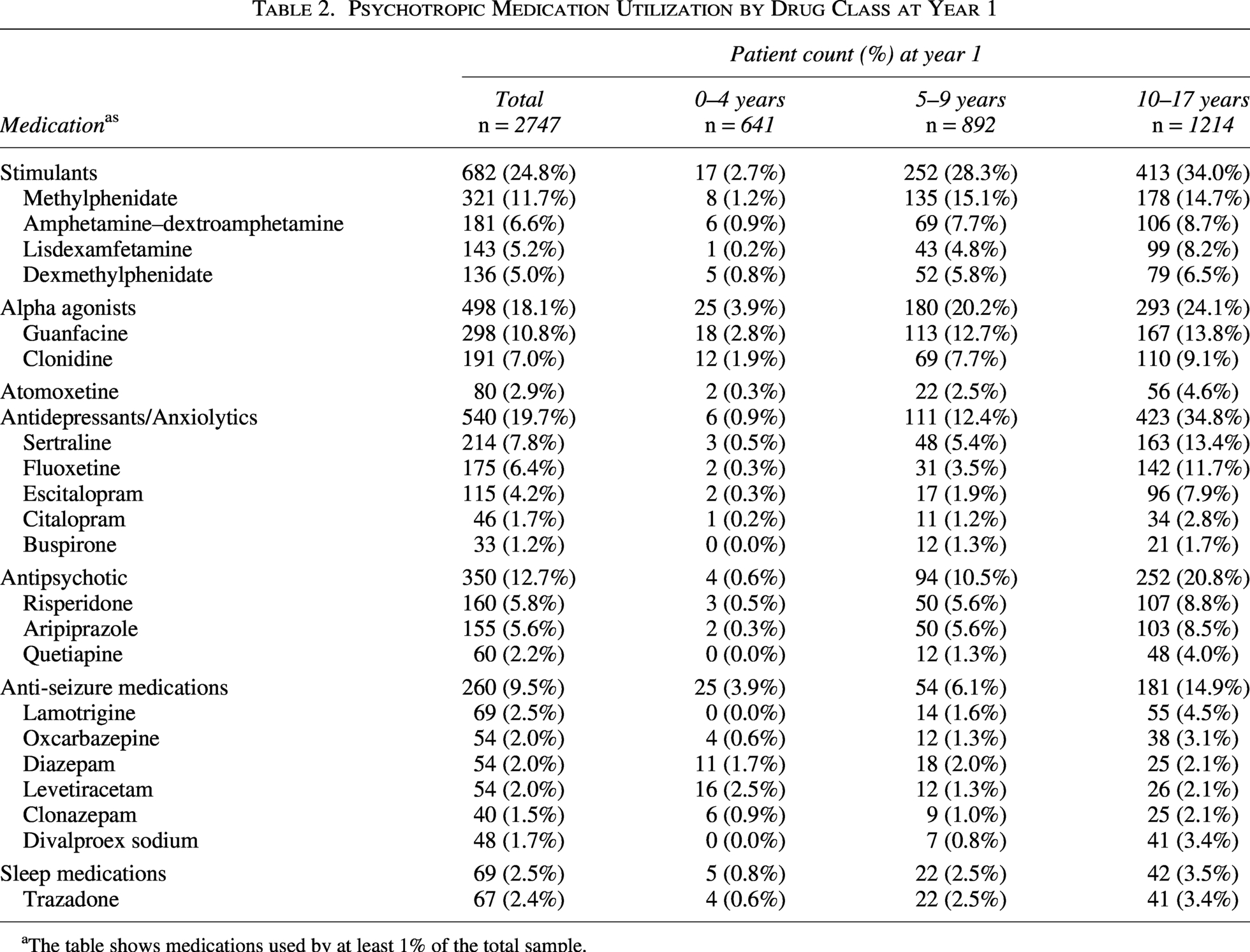
The table shows medications used by at least 1% of the total sample.
High-complexity subgroup
At Year 1, across all age groups, there were a total of 415 children (15.1%) who used an antipsychotic and/or at least three concurrent drug classes (Supplementary Table S2). At Year 1, the prevalence was the highest in the oldest age group, with 24.9% in the 10–17 years cohort, followed by 12.2% in the 5–9 years cohort and only 0.6% in the 0–4 years cohort. Significantly more children aged 10–17 were classified in the high-complexity group than those aged 5–9 (p < 0.000001), and more children aged 5–9 than children aged 0–4 years (p < 0.000001). In the high-complexity subgroup, the most common combinations were antidepressants/anxiolytics + antipsychotics, alpha agonists + antipsychotics, and stimulants + antipsychotics (Supplementary Table S4).
Over the entire follow-up period, 562 individuals (20.5%) were categorized as having high treatment complexity in any of the 3 years. The high-complexity subgroup had a notably higher prevalence of prespecified co-occurring conditions compared with those who never used any antipsychotics and were not treated with three or more concurrent drug classes (noncomplex subgroup; n = 2185; Fig. 3). The categories with the largest differences between the high-complexity group and noncomplex group include ADHD (72.1% vs. 39.3%), anxiety disorders (58.7% vs. 28.9%), bipolar disorder or other mood disorders (36.3% vs. 5.0%), and conduct disorder (31.0% vs. 9.0%). Additionally, conditions such as irritability/agitation and schizophrenia/psychotic disorders were rare in the noncomplex subgroup (2.4% and 0.5%, respectively) but had much higher prevalence in the high-complexity subgroup (14.6% and 9.6%, respectively). When complexity was defined with alternative criteria, such as antipsychotic use only, using three or more drug classes only, or requiring both of these criteria, the pattern of comorbidities among complex individuals was similar to those with either antipsychotics or three or more drug classes (Supplementary Table S5).

Distribution of co-occurring conditions in the individuals classified as complex at any point of the 3 years (complex subgroup) compared with those not classified as complex for the entire 3-year follow-up (noncomplex subgroup). ADHD, attention-deficit hyperactivity disorder; AP, antipsychotic.
Discussion
We believe that our study provides important insights into the treatment trajectories in children with ASD. Our descriptive analysis examined psychotropic medication use and polypharmacy patterns across different age groups in children with ASD using a large sample of commercially insured employee dependents in the United States. We found that older children exhibited higher rates of antipsychotic medication use, and treatment complexity was observed with a higher prevalence of mood disorders and other behavioral disorders associated with disruptive behaviors. Notably, a decline in medication use over time among adolescents suggests treatment de-escalation or refinement due to potential symptom improvement, side effects, or transition of care in adolescents. Our findings of higher rates of polypharmacy in older age groups were consistent with prior observational studies. A Canada-based study also found that compared with those aged 1–5 years, children with autism aged 6–12 years, 13–17 years, and 18–25 years had higher odds of using any psychoactive drug (Croteau et al., 2019). Another study on youth with ASD also reported similar proportions of individuals using two or more medications concurrently for at least 60 days in a year, with only 1.5% in 0–5-year-olds, 13.5% in 12–17-year-olds, and 29.6% in 6–11-year-olds (Rast et al., 2025). Specifically, we observed a marked increase in utilization of antidepressants/anxiolytics in the 10–17 age group, which more than doubled the prevalence of use in the 5–9 age group (34.8 vs. 12.4%). This rise in antidepressants/anxiolytic treatment in the 10–17 age group may be attributed to increased prevalence of depression in adolescence as well as more common screening and identification given the American Academy of Pediatrics (AAP’s) recommendation of depression screening beginning at age 12 (Hyman et al., 2020). Other factors may also contribute to the infrequent utilization of psychotropic medications in children <5 years old, including the FDA-indicated minimum age for medications such as aripiprazole and risperidone and diagnostic uncertainty in very young children leading to the decision to delay pharmacologic treatment.
Although older cohorts had a higher prevalence of medication use, interestingly, we observed a reverse in the longitudinal trend of psychotropic medication use between Year 1 and Year 3 in the 10–17 age group, with a small reduction in medication use in Year 3. In contrast, a Quebec study reported an increase in the mean number of medications at 5 years postdiagnosis in those aged 13–17 years (Croteau et al., 2019). However, in the older, early adult age group, the number of medications was unchanged in those aged 18–25 years (Croteau et al., 2019). Therefore, the findings from both analyses suggest that in individuals diagnosed at a higher age (18–25 age group in the Croteau et al. study and 10–17 age group in this study), medication use stabilized in subsequent years after diagnosis. This downward trend in medication use, specifically for stimulants and alpha agonists, has also been observed in adolescents with ADHD. In a U.S. claims analysis in individuals with ADHD aged 16–21, the percentage of patients receiving ADHD pharmacotherapy significantly decreased as patients aged, and the median time to treatment discontinuation was 2.94 years (Farahbakhshian et al., 2021). The observed decline in several medication classes in older adolescents may reflect a combination of developmental changes, treatment refinement, and transition from pediatric to adult care. Moreover, the observed decline could also be attributed to the nature of our sample, which most likely included both incident and prevalent cases. In clinical practice, psychotropic regimens in youth with ASD often evolve over time as clinicians and families evaluate the balance between symptom improvement and medication-related adverse effects. In some cases, medications initially prescribed during periods of severe behavioral dysregulation may be reduced or discontinued as symptoms stabilize or as treatment goals shift during adolescence. Possible stabilization of behavioral symptoms was supported by changes in different drug classes in the 10–17 age group, with a decline in antipsychotics use (indicated for irritability and severe disruptive behavior) along with stimulants and alpha agonists (indicated for hyperactivity, impulsivity, and inattention) but stable trends in antidepressants/anxiolytics and anti-seizure medication use. Age-related improvement in behavioral symptoms associated with ASD has been reported in previous longitudinal studies: One study on children with autism, aged 11.8 years on average, found that aggressive behavior observed in 61.6% of children at baseline only persisted in 30% of participants over 10 years (Laverty et al., 2023). Another study also found that autism symptoms and maladaptive behaviors in adolescents and adults with ASD were observed to improve over the 8.5-year study period (Woodman et al., 2015). Similarly, in a French longitudinal survey study, caregivers of children with ASD reported a significant decline in the hyperactivity domain between adolescence (13–17 years of age) and early adulthood (18–23 years), although irritability/aggressiveness and stereotypy domains did not change significantly (Rattaz et al., 2018). Besides symptom stabilization improvement, adolescents and their caregivers may discontinue medications in response to side effect burden, such as weight gain, sedation, or metabolic effects associated with antipsychotics, especially since this age group had the highest rate of polypharmacy in Year 1. Additionally, youth with autism may also develop behavioral coping strategies, potentially reducing the need for pharmacological management and deprescribing of psychotropic medications. Lastly, teenagers aged 16 or more at index may also transition from pediatric to adult health care providers within the study follow-up, which could lead to changes in prescribing patterns between the pediatric specialists who initiated treatment and the adult primary care provider.
However, it is important to contextualize these longitudinal findings with this study’s limitations using an administrative database: First, given that the average age of ASD diagnosis is 4.9 years in the United States (Autism Speaks, 2025), many in the 10–17 age group likely received an ASD diagnosis earlier in life but entered this claims dataset later, resulting in a higher age at index diagnosis in this study. These individuals may represent both incident and prevalent cases; more likely, they represent prevalent cases with established ASD diagnoses and potentially are already on treatment for a longer duration compared with new cases of ASD. As a result, the observed decline in psychotropic medications in the 10–17 age group may also reflect a later stage in treatment trajectories, where medications tried earlier in life were being discontinued due to inadequate prior response or cumulative side effects, compared with younger age groups, who likely represented newly diagnosed individuals. Second, the inclusion criterion of 3 years of continuous insurance enrollment likely had a confounding effect on medication utilization. Caregivers of children with more persistent and severe presentations of autism might have left the workforce within the 3-year period to focus on caregiving responsibilities, thereby losing employer-sponsored commercial insurance. Consequently, these dependents with higher needs would have been excluded from this sample, leading to an underestimation of treatment burden compared with the true population with ASD.
Although the ICD-10-CM diagnosis codes do not distinguish between severity levels, we utilized a composite marker of antipsychotic use or concurrent use of three or more drug classes as an indicator of autism with higher treatment complexity suggestive of cumulative management of multiple co-occurring psychiatric and behavioral comorbidities. We found that those classified as high treatment complexity also had a notably higher prevalence of mental health and behavioral conditions compared with the noncomplex subgroup, highlighting the high burden of co-occurring conditions among patients with antipsychotic use or polypharmacy. Besides clinical mental health conditions such as depression and bipolar disorders, aggression and disruptive behaviors are also clinically important, as they not only drive treatment decisions but also contribute substantially to health care resource utilization, including psychiatric hospitalization (Mandell, 2008) and increased caregiver strain (Bradshaw et al., 2021). While symptoms of aggressive behaviors could not be measured directly, we found that diagnoses of conduct disorder and irritability and agitation in the high treatment complexity group were more than twice as prevalent as in the noncomplex group. Additionally, the medication combination patterns observed in this analysis also aligned with common clinical approaches to symptom management in ASD. For example, stimulant and alpha agonist combinations are recommended to address ADHD, hyperactivity, and impulsivity, while antidepressant or anxiolytic agents may be added for anxiety, mood symptoms, or rigidity (Manter et al., 2025). Antipsychotic medications are typically reserved for more severe irritability, aggression, or behavioral dysregulation (Manter et al., 2025). These patterns suggest that the treatment-complexity marker may reflect the accumulation of pharmacologic strategies targeting multiple symptom domains rather than a single underlying condition. When we used alternative definitions of treatment complexity (based on antipsychotic use alone, having three or more drug classes alone, or requiring both criteria), sample sizes of complex individuals differed, but similar patterns of co-occurring conditions were observed. This was likely due to overlap in patients who fit these definitions; for example, most of the patients with at least three or more drug classes (n = 335) were also treated with an antipsychotic (n = 231). Our findings suggested that in claims-based research where symptom scores are absent, the use of antipsychotics or three or more drug classes may be a useful, though imperfect, indicator for identifying a subgroup with greater clinical complexity and need. It is important to highlight that higher medication burden may also be related to underlying disease severity, which was not assessed directly in this analysis due to the lack of symptom-specific severity data in administrative claims data. Future analyses may further investigate alternative proxies of ASD severity and explore patient and caregiver outcomes among individuals with autism who face high medication treatment complexity. Our study’s sample of only commercially insured children limits generalizability to the U.S. population and may underestimate medication burden. As our sample consisted of dependents of commercially insured employees, with an average salary above that of the general U.S. population, it is not representative of children with lower socioeconomic status, those with Medicaid insurance or those without insurance, and those with unemployed or disabled parents. Additionally, medications excluded from coverage by private insurance but covered secondarily by Medicaid were also not captured in this claims database. Prior studies reported that Medicaid enrollees with autism reported more prevalent polypharmacy (Houghton et al., 2017) and higher health care resource expenditure and utilization, including higher total and ASD-specific health care costs, more frequent speech therapy visits, and more frequent behavioral modification and social skill visits (Wang et al., 2013). As such, our study likely underestimated medication use compared with a nationally representative sample. Nevertheless, this study’s findings remain highly relevant for employer groups and commercial insurance payers. We found that even among children of employed caregivers, medication burden and comorbidity burden are substantial, highlighting the importance of medication coverage and other workplace policy and benefits to best support employees of children with ASD.
Another limitation of this analysis is the inclusion of both incident and prevalent autism cases, as the first available diagnosis in claims data may not necessarily reflect the true time of initial diagnosis. While the average age of autism diagnosis is 4.9 years in the United States and ranges from 2.8 to 7.6 years in different states (Autism Speaks, 2025), the average age at index in this study was 9.3 years. Younger children are thus more likely to represent new diagnoses, whereas many individuals in the older age group are likely to reflect prevalent cases and ongoing treatment. However, since the purpose of this study was descriptive in nature rather than to infer causality, we included all individuals with a recorded autism diagnosis at baseline to provide a more comprehensive depiction of utilization patterns at different ages. Additionally, administrative data has poor capture of over-the-counter products such as melatonin, likely leading to the findings of low utilization of sleep medications in our analysis. Furthermore, while there is racial disparity in the diagnosis of ASD and treatment (Liu et al., 2023), race and ethnicity information was only available for 42.4% of patients in this dataset, which limited the completeness of demographic characterization and ability to generalize our study’s findings to racial minorities. Lastly, this study’s follow-up period was limited to 3 years, as requiring longer continuous enrollment in claims data would have substantially reduced the sample size. A longer longitudinal study can more definitively characterize long-term medication utilization changes through different developmental stages in children. However, as discussed, requiring three years of continuous enrollment also could have excluded caregivers who left the workforce due to caring for children with greater ASD-related needs, thus likely underestimating the true burden of treatment in the ASD population. Although our study focused on characterizing treatment utilization over a defined observation period, future studies could examine time to benefit disenrollment to better understand how ASD severity and treatment burden may relate to insurance loss and caregiver burden.
Future research should aim to build on these findings by incorporating longer follow-up periods to better capture the evolution of pharmacologic treatment across developmental stages in ASD. Additionally, integrating clinical data sources such as electronic health records data or caregiver-reported outcomes could provide more granular insights into symptom severity, functional outcomes, and the rationale behind medication changes. Given the observed association between antipsychotic use/polypharmacy and behavioral symptoms such as agitation and irritability, future research should also examine whether claims-based indicators of treatment complexity are associated with caregiver burden and family outcomes. Youth with ASD requiring antipsychotic treatment and/or three or more concurrent psychotropic medication classes may represent families experiencing greater day-to-day management demands related to behavioral dysregulation, psychiatric comorbidity, and functional impairment. Understanding how treatment complexity relates to caregiver stress and health outcomes may provide important insight into the broader impact of ASD on family systems.
Conclusions
This U.S. claims-based analysis of commercially insured children with ASD found that psychotropic medication use and treatment complexity increased in older age groups, but medication use declined slightly over time in the adolescent age group. The observed stabilization or decline in certain medication classes during adolescence might be highlighting the importance of periodic treatment reassessment during adolescence and potential deprescribing opportunities based on symptom and behavioral changes across developmental transitions. Claims-based measures of treatment complexity also identified a subgroup of youth with substantially higher psychiatric and behavioral comorbidity burden, suggesting the possibility of using such measures for recognizing patients who may benefit from closer clinical monitoring. Although treatment burden may be underestimated due to the continuous enrollment requirement in a commercially insured population, these findings might underscore the complexity of psychotropic medication use over time. Future work examining how treatment complexity relates to family-level outcomes, including caregiver burden and functional impairment, may provide further insight into the broader clinical and societal impact of ASD.
Clinical Significance
This study describes age-related differences in longitudinal psychotropic medication use and treatment complexity among commercially insured children and adolescents with ASD. Higher prevalence of antipsychotic use and polypharmacy were observed in older age groups and reflected a greater burden of comorbidities. From a clinical perspective, pharmacotherapy complexity may serve as a practical signal of increased treatment burden in youth with ASD. While medication complexity should not be interpreted as a direct indicator of autism severity, it may identify individuals with multiple co-occurring psychiatric or behavioral conditions requiring ongoing pharmacologic management. Recognizing this subgroup may help clinicians prioritize periodic structured medication review, reassessment of target symptoms, and careful monitoring of cumulative side-effect burden.
The reduction in certain medication classes during adolescence suggests that psychotropic treatment needs evolve across developmental stages, highlighting the importance of periodic treatment reassessment at key transitions such as entry into adolescence during shifts from pediatric to adult care. Clinicians and caregivers should engage in shared decision-making regarding ongoing medication needs, including consideration of structured deprescribing based on symptom and adverse effect assessments. Future research should examine work productivity and caregiver outcomes among employees with dependents with ASD, alongside qualitative investigation into the drivers of adolescent medication reduction, to inform both workplace policy and deprescribing practices in clinical care.
Authors’ Contributions
C.M.C.: Investigation, formal analysis, methodology, project administration, validation, visualization, and writing—original draft. K.M.S.: Data curation, investigation, formal analysis, resources, software, and writing—review and editing. S.K.P. and C.B.G.: Conceptualization, methodology, supervision, validation, writing—review and editing. E.M.R.: Data curation, formal analysis, resources, and writing—review and editing. J.N.P.: Conceptualization, methodology, validation, and writing—review and editing.
Ethics Approval
Data used for this study were deidentified and in full compliance with the Health Insurance Portability and Accountability Act; therefore, the University of Pittsburgh Institutional Review Board granted an exemption.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.