
Abstract
Background:
Down syndrome (DS) is a major genetic cause of intellectual disability. In an animal model of DS, fluoxetine was shown to restore brain architecture and cognitive performance, acting primarily on the hippocampus, with effects persisting after treatment discontinuation. In this translational study, we assessed the safety and tolerability of fluoxetine at the standard labeled dose and explored selected efficacy endpoints to inform future clinical trials.
Methods:
The study was approved as a phase I, open-label study. Participants with full trisomy 21 received fluoxetine (10 mg/day) for 6 months, followed by a 6-month observation period. The primary endpoint, safety and tolerability, was evaluated through clinical examinations, biochemistry, plasma fluoxetine and norfluoxetine levels, electroencephalography, and electrocardiography at multiple time-points. As a secondary efficacy endpoint, we selected a set of cognitive tests to explore hippocampus-dependent functions and adaptive behavior.
Results:
Fourteen children with DS (8.1 ± 1.24 years; range 6–10) were enrolled, and 12 completed the 12-month study. No serious or severe adverse events (AEs) occurred. All AEs resolved without sequelae. Short-term terminal insomnia was observed in two patients. Neuropsychological assessments revealed improvements in visuospatial processing tasks during the study. Analysis of adaptive behavior suggested enhanced expression skills.
Conclusions:
These findings indicate that fluoxetine is safe in children with DS. The association with terminal insomnia warrants specific investigation in future trials and strategies to optimize tolerability are discussed. Efficacy analyses highlight the visuospatial processing domain as potentially responsive to treatment, supporting further research.
Keywords
Introduction
Down syndrome (DS) is a major genetic cause of intellectual disability. From early infancy, children with DS exhibit weakness in verbal communication, learning processes, and memory, while nonverbal cognitive functions are generally less affected (Marino et al., 2019; Onnivello et al., 2022; Pulina et al., 2019). Accumulating evidence indicates that intellectual disability in DS primarily arises from alterations in neurogenesis and dendritogenesis (Stagni and Bartesaghi, 2022). In the human brain, cortical neurogenesis is completed before birth around gestational week 24–25, whereas neurogenesis in the hippocampus and cerebellum continues after birth. Specifically, cerebellar neurogenesis ceases around 5 months of age, while hippocampal neurogenesis persists at a slow rate throughout life. Dendritic maturation continues during infancy and concludes by late adolescence (Stagni and Bartesaghi, 2022). Considering the timeline of cerebral differentiation and maturation, interventions aimed at improving cognitive abilities should begin as early as possible. Preclinical studies in DS animal models have examined whether pharmacological interventions may promote brain development and enhance cognitive performance in DS (Gardiner, 2015; Stagni et al., 2015a ; Stagni and Bartesaghi, 2022). In human studies, clinical trials of memantine (Hanney et al., 2012), donepezil (Kishnani et al., 2010), intranasal insulin (Rosenbloom et al., 2020), basmisanil (Goeldner et al., 2022), and simvastatin (Cooper et al, 2016) have not demonstrated clear cognitive benefits in adults with DS. More recently, a pilot open-label trial involving seven men with DS treated with pulsatile gonadotropin-releasing hormone for 6 months reported improvements in visuospatial function, executive function, and attention (Manfredi-Lozano et al., 2022). In children aged >10 years and adolescents with DS, intervention with memantine (Costa et al., 2022), donepezil (Kishnani et al., 2010), and basmisanil (Goeldner et al., 2022) did not show improvement in cognitive functions. In previous mice studies, we demonstrated that perinatal treatment with fluoxetine, a selective serotonin reuptake inhibitor (SSRI), restores hippocampal neurogenesis, dendritogenesis, neural connectivity, and long-term memory in the Ts65Dn mouse model of DS, with effects persisting after treatment discontinuation (Bianchi et al., 2010; Guidi et al., 2013; 2014; Stagni et al., 2013; 2015b). A recent independent study further showed that chronic fluoxetine administration in adult Ts65Dn mice corrects synaptic abnormalities and prevents aberrant proteomic changes related to synaptic vesicular traffic, endocytosis, assembly, and maturation (Fatemi et al., 2024).
The finding that fluoxetine improves key neurodevelopmental processes in a DS model suggests that early treatment with fluoxetine may enhance brain development and cognitive outcomes in DS. In clinical practice, fluoxetine, like other SSRIs, is used to treat major depressive disorder. Previous studies have shown that the brains of depressed patients treated with SSRIs (including fluoxetine) exhibit an increased number of progenitor and proliferating cells and an enlarged hippocampal dentate gyrus compared with those of untreated depressed and nonpsychiatric patients (Boldrini et al., 2009; 2012; 2013; Cobb et al., 2013; Huang et al., 2013). These data demonstrate that the human hippocampus, like the rodent hippocampus, is sensitive to the neuroplastic effects of antidepressants. In pediatric populations, fluoxetine is approved for the treatment of moderate to severe major depressive episodes, at the starting dose of 10 mg/day. Although no studies have specifically assessed fluoxetine safety in children with DS, case reports describe adults with DS treated with SSRIs for cognitive decline or behavioral disturbances, reporting favorable safety profiles and clinical improvement (Akahoshi et al., 2012; Geldmacher et al., 1997; O’Dwyer et al., 1992; Raitasuo et al., 1998; Tsiouris et al., 2014). In other neurodevelopmental conditions, including autism spectrum disorder, fluoxetine has been tested in clinical trials involving participants older than 5 years to target repetitive behaviors. The daily doses ranged from 10 to 40 mg, and adverse event (AE) rates were comparable to placebo (Alcamí Pertejo et al., 2000; Geller et al., 2001; Hollander et al., 2005; Makkonen et al., 2011). Based on this evidence, the present study aimed to translate the preclinical finding from DS animal models to pediatric individuals with DS. The primary objective of this study was to assess the safety and tolerability of fluoxetine in children with DS aged 5–10 years. We also aimed to collect preliminary evidence of efficacy on hippocampus-dependent functions and adaptive behavior in this age range and to identify potentially modifiable cognitive domains that could inform future research.
Materials and Methods
The study was approved by the Italian regulatory authorities as a single-center, phase I, open-label, one-arm clinical trial. The trial is registered in the EudraCT database (ARIDDS2; EudraCT n. 2017-000687-16). The study was approved by the Italian Institute of Health (ISS, n. 30891(17)-PRE21-1580), the Italian Medicines Agency (AIFA, n. 134021), and the Institutional Ethics Committee (n. 222/17). Written informed consent was provided by parents or legal guardians, and children gave assent (when possible) after the study information sheet was explained in age-appropriate language. The trial was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines.
Study population
Children with DS were recruited at the Down’s Syndrome Clinic, Department of Maternal and Child Health of the Federico II University Hospital, Naples, Italy. According to the study protocol, recruitment lasted 12 months. Inclusion criteria were (1) diagnosis of DS by karyotype analysis; (2) age between 5 and 10 years, either sex; (3) written informed consent from parents or legal guardians; (4) euthyroid status (reference value: FT4), with or without
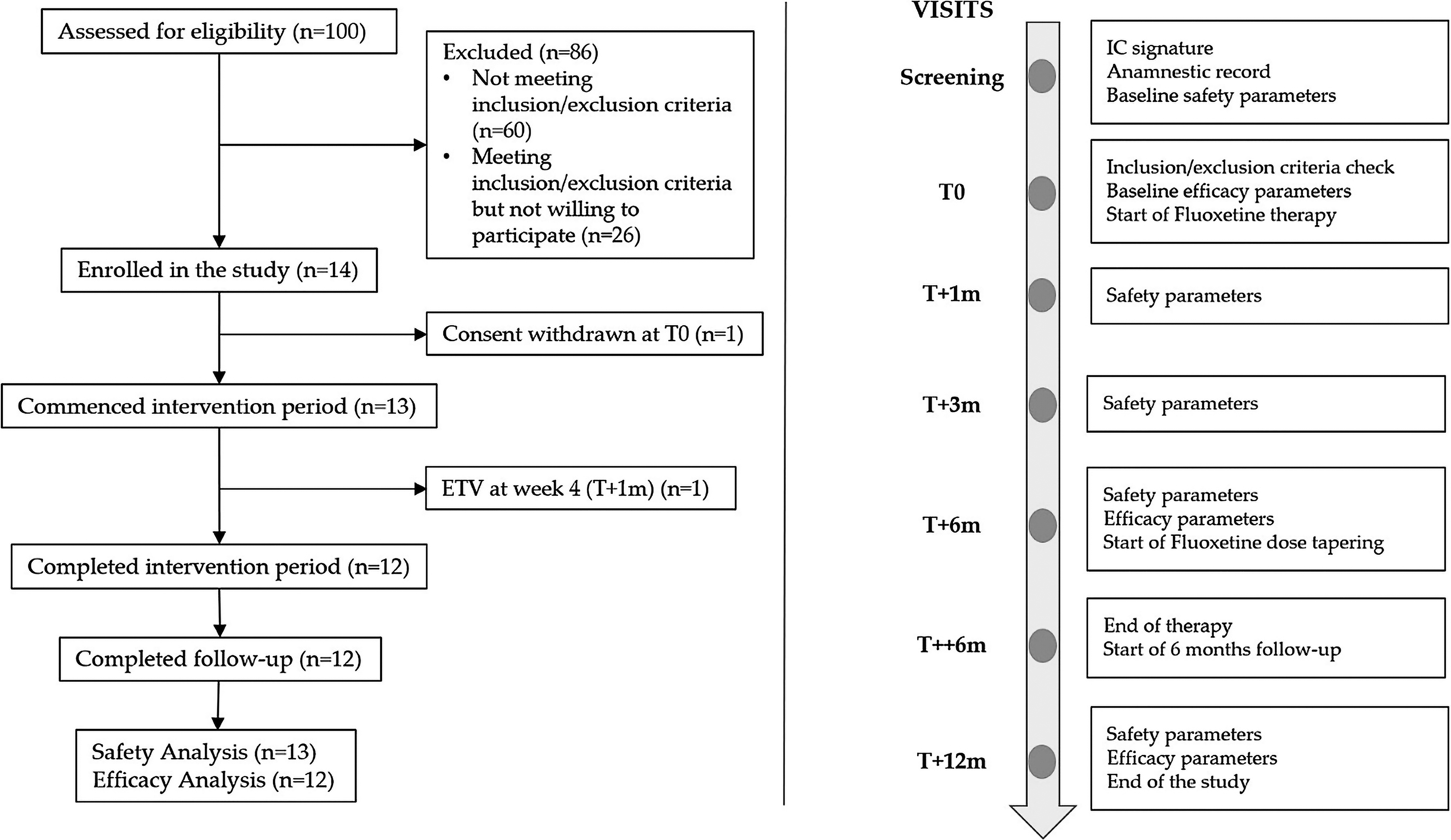
Study flow diagram. ETV, early termination visit; IC, informed consent; T++6m visit, 16 days of fluoxetine dose tapering; T+12m, 12 months after T0; T+1m visit, 1 month after T0; T+3m visit, 3 months after T0; T+6m visit, 6 months after T0; T0, baseline visit.
Experimental plan
Each subject attended seven visits: screening (within 15 days prior to T0), T0 (baseline), T+1m (1 month post-T0), T+3m (3 months post-T0), T+6m (6 months post-T0), T++6m (6 months and 16 days post-T0), and T+12m (12 months post-T0). Fluoxetine dose tapering started at T+6m to end after 16 days (T++6m). Details are provided in Supplementary Table S2. AEs were recorded at each visit. The tolerance window of ±1 week was permitted for visit scheduling. Participants discontinuing early underwent an ETV equivalent to the T+12m visit.
Experimental medication
Fluoxetine oral solution (20 mg/5 mL) was administered at 10 mg/day. The dose was selected based on preclinical findings and on the dosage specified in the Summary of Product Characteristics (SPC) for pediatric patients (Agenzia Italiana del Farmaco, 2013). At T0, a 3-day titration at 5 mg/day was followed by maintenance at 10 mg/day until T+6m. After T+6m, treatment was discontinued through a tapering protocol (dose reduction by 2 mg every 4 days over 16 days; T++6m), followed by a 6-month observation phase until T+12m.
Safety and tolerability
AEs, severe AEs (SAEs), and suspected unexpected serious adverse reactions were classified as unrelated or related to treatment, with causality assessed per WHO-UMC criteria (certain, probable/likely, possible, unlikely) (Edwards and Biriell, 1994). Preliminary evidence of safety required the absence of any serious AEs or SAEs that were possibly, probably, or definitely related to fluoxetine. Tolerability was evaluated based on treatment retention (at least 80% of participants exposed to fluoxetine completing treatment without discontinuation due to AEs) and the incidence of AEs. At all visits except T0, fasting blood samples were collected for biochemistry and fluoxetine/norfluoxetine plasma levels. The therapeutic range (fluoxetine + norfluoxetine) was 120–500 ng/mL (Hiemke et al., 2018). Electrocardiograms (ECGs) were obtained for QTc evaluation. Electroencephalograms (EEGs) were performed at screening, T+3m, T+6m, and T+12m. Anthropometric data (height, weight, body mass index [BMI], occipitofrontal circumference ) and pubertal stage were recorded at each visit. The potential effect of fluoxetine on appetite was monitored through parents' interviews and weight assessments. Risk of mood disorders was assessed using Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime version; K-SADS-PL) (Kaufman et al., 2004). Neurological examination evaluated (1) state of consciousness, orientation, and cooperation; (2) presence/absence of expressive language and of language impairments; (3) cranial nerves integrity; (4) coordination deficit; (5) reflexes; and (6) gait.
Psychometric testing
Hippocampus-dependent functions were assessed using memory, learning, and visuospatial tasks. Of the Wechsler scales (Wechsler, 2012), WPPSI was chosen for children <6 years, and WISC-IV for those ≥6 years; however, no participants were younger than 6 years. The analyzed subscales included: (1) NEPSY-II “Memory for Faces” and “Narrative Memory” (memory and learning domain); (2) NEPSY-II “Route Finding” and “Arrows” (visuospatial processing domain) (Korkman et al., 2007); (3) WISC-IV “Digit Symbol” (processing speed index), “Digit Span” (working memory index), “Vocabulary” and “Information” (verbal comprehension index), and “Block Design” (visual spatial index). Fluid intelligence was evaluated with the Leiter-R (Roid and Miller, 2002), generating weighted scores for “Figure Ground,” “Form Completion,” “Sequential Order,” and “Repeated Patterns,” from which a short-IQ score was derived. The short-IQ is a recognized and validated method for the assessment of fluid intelligence in individuals with verbal impairments and/or susceptible to distractibility and fatigue, like children with DS (Channell et al., 2014; Glenn and Cunningham, 2005; Phillips et al., 2014). Adaptive behavior was assessed using the Vineland-II scale (Sparrow et al., 2016). All the selected tests were repeatable after 6 months without the risk of “learning bias,” according to the tests’ specific instructions. We analyzed (1) the increase in the raw scores of the NEPSY-II and WISC-IV subtests; (2) positive differences in short-IQ score and its subtests (weighted scores); and (3) positive differences in the Vineland-II scale weighted scores. A significant change in any subtest was considered an achieved endpoint.
Statistical analysis
The safety analysis was conducted using a modified intention-to-treat approach, including all participants who received at least one dose of the treatment. To assess efficacy, a per-protocol analysis was performed, including only those participants who completed the study. Descriptive characteristics were provided using medians and interquartile ranges (IQR) or mean and standard deviation, minimum and maximum values for continuous variables, and frequencies and percentages for categorical variables. The comparisons of continuous variables at two different time-points were performed using the paired Wilcoxon signed-rank test, and the mean and median difference were calculated compared to baseline value or screening value according to protocol. Regarding categorical variables, the comparisons of proportions at two different time-points were made by nonparametric McNemar test. During the study, not all participants were able to complete every test; therefore, the number of comparisons varies depending on the test. The p Value was considered significant if lower than 0.05 (two-sided). The incidence rate of AEs was calculated as the number of AEs divided by the total number of person-months of follow-up and was expressed per 100 person-months. The statistical analysis was performed using STATA 15.1 software.
Results
Participant characteristics
Fourteen Caucasian children (9 males, 5 females; mean age 8.1 ± 1.24 years; range 6–10 years) with full trisomy 21 were enrolled. All were born at term or late preterm (mean 37.4 ± 1 gestational weeks; range 35–39) with normal APGAR scores (≥7) (Supplementary Table S3). Rehabilitation therapies remained unchanged during the study.
Safety and tolerability
Growth parameters were evaluated at each visit (except T++6m). At T+6m, there was a significant increase in weight and height due to children’s growth, but not in BMI. At T+12m, BMI increased compared with screening (p = 0.011) but not compared with T+6m, when treatment was discontinued (Table 1). All BMI values remained <95th percentile. Pubertal development followed age-appropriate trajectories. Vital signs remained within the normal ranges according to age. Serial ECGs did not show abnormalities, and QTc was normal in all patients. No abnormalities in EEGs were observed. No seizures were reported. No clinically significant biochemical abnormalities were detected (Supplementary Table S4). Fluoxetine and norfluoxetine levels were within the therapeutic range (Fig. 2).
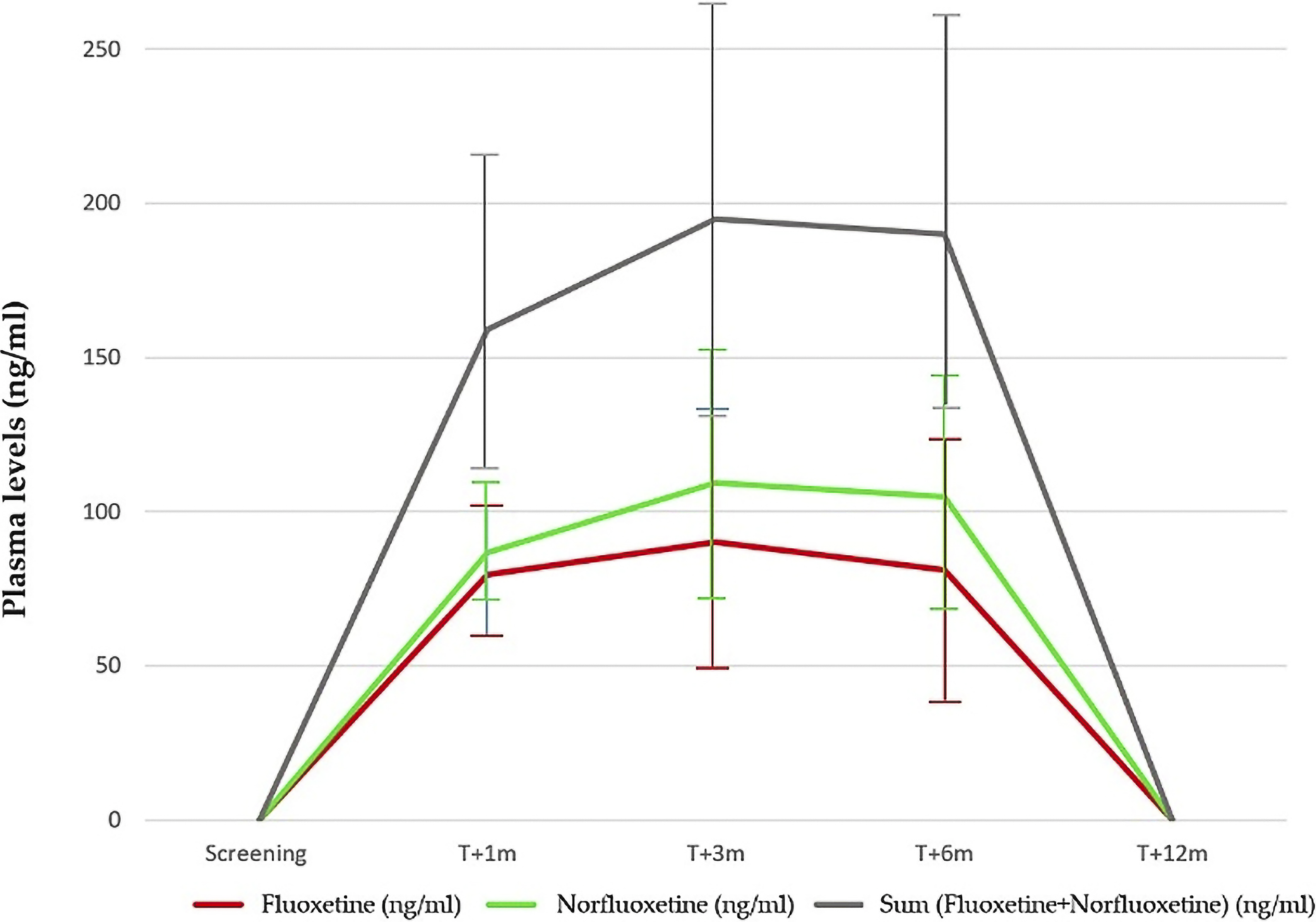
Fluoxetine and norfluoxetine plasma levels.
Growth and Vital Signs Variation
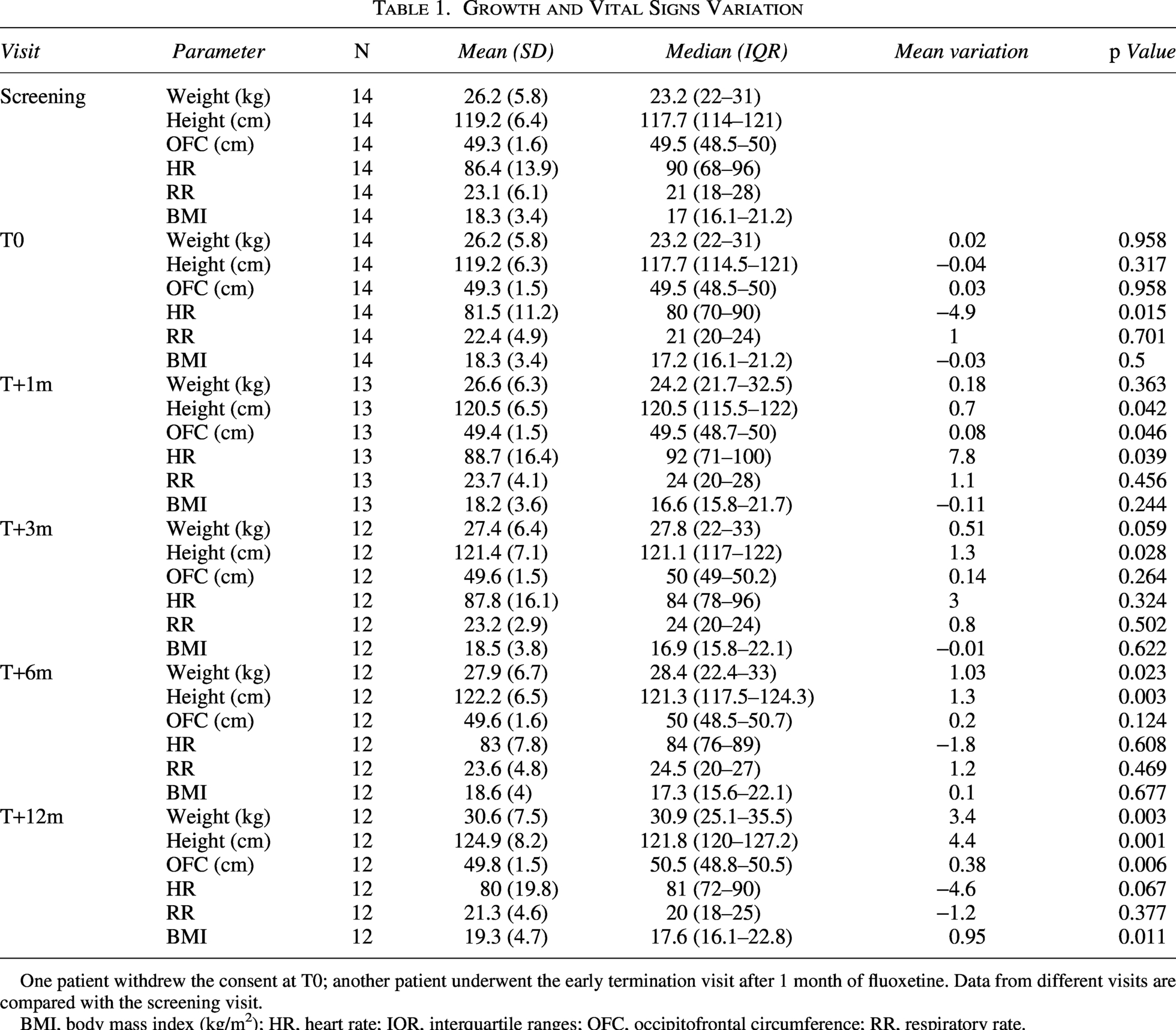
One patient withdrew the consent at T0; another patient underwent the early termination visit after 1 month of fluoxetine. Data from different visits are compared with the screening visit.
BMI, body mass index (kg/m2); HR, heart rate; IQR, interquartile ranges; OFC, occipitofrontal circumference; RR, respiratory rate.
K-SADS-PL interview was administered to intercept mood disorders: at screening, one participant (7.1%) reported transient sadness; at T+1m and T+3m, no mood disorders were reported; at T+6m, transient and mild irritability symptoms were present in two participants (16.7%) (p = ns); at T+12m, no symptoms were reported (Table 2).
Psychopathological Risk Assessed by K-SADS-PL

One patient withdrew the consent at T0; one patient underwent early termination visit after 1 month of fluoxetine. Data from different visits are compared with the screening visit.
None of the examined neurological areas showed worsening throughout the study (Supplementary Table S5).
Adverse events
Ten AEs were registered (Table 3), none serious or severe, all resolving without sequelae. Five were unrelated to fluoxetine: four infections (patients #2, #5, #6, #12) and one irritability episode (patient #10) 7 weeks post-withdrawal. Considering that, according to fluoxetine SPC, both fluoxetine and norfluoxetine are completely eliminated after 5–6 weeks from withdrawal, the AE was judged as not related to the medication. One urticaria episode at week 4 (patient #1), treated with cetirizine, was judged as probably related as urticaria and itching are possible side effects of fluoxetine according to SPC. The same patient developed dermatillomania during fluoxetine tapering, with onset 6 days after T+6m at the dose of 5 mg/day, resolving without intervention after 18 days. The symptom is not listed among the known fluoxetine AEs but was judged as possibly related because the patient was still exposed to the medication. In all cases but one, no modification of fluoxetine treatment was required. In patient #2, the occurrence of lack of appetite, headache, and diarrhea was classified as possibly related to fluoxetine because of the reasonable time-relationship with fluoxetine intake, but confounded by the concurrent helminthic infection and antihelminthic therapy. In this case, the family decided to stop the treatment. Lack of appetite was not observed in the other patients. Two patients (15%) presented short-term terminal insomnia, defined as premature awakenings over a period <3 months according to DSM-5 criteria. In patient #1, a 6-year-old girl, the reduction of sleep hours (from 9–10 h to 7–8 h) occurred between T0 and T+1m, lasted for 18 days, and spontaneously resolved without medications. In patient #9, an 8-year-old girl, after 10 weeks of treatment, mean nocturnal sleep hours gradually decreased from 7–8 h at baseline to 5–6 h/night until T+6m, improving with melatonin (3 mg before bedtime). The family decided to continue the treatment. Insomnia resolved upon fluoxetine discontinuation at T++6m. Fluoxetine plasma levels were within the normal range and were not different compared to those of children without insomnia.
Summary of Adverse Events and Incidence Rate
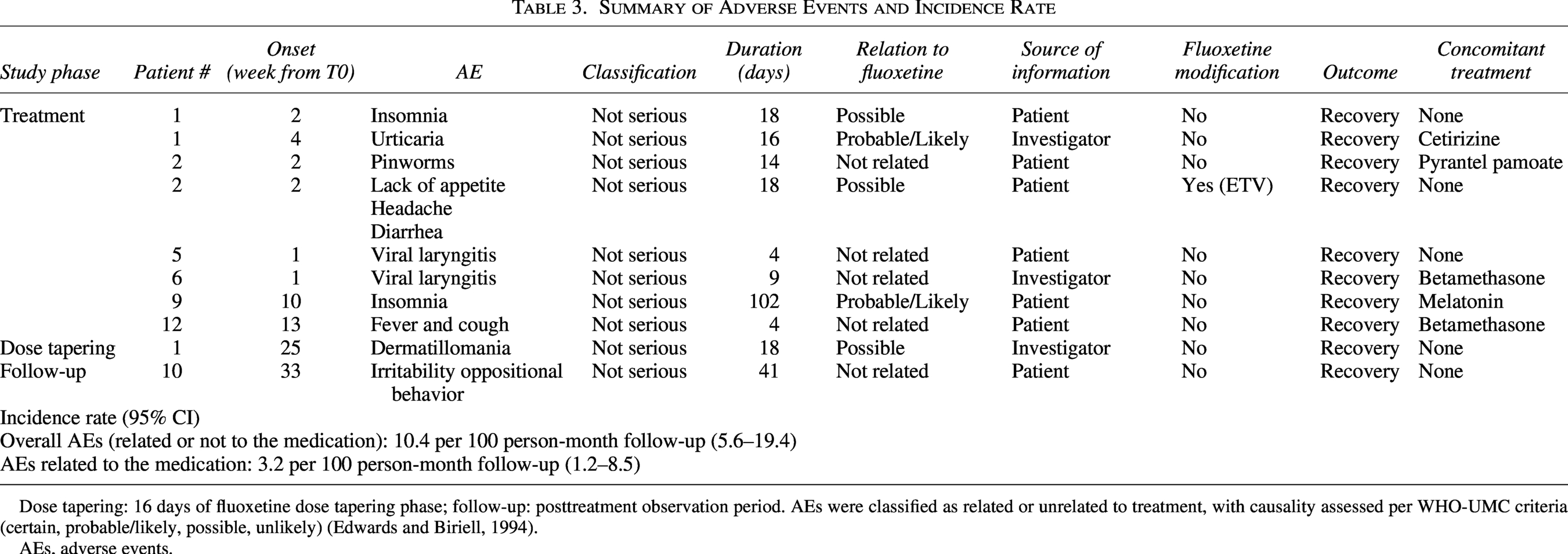
Dose tapering: 16 days of fluoxetine dose tapering phase; follow-up: posttreatment observation period. AEs were classified as related or unrelated to treatment, with causality assessed per WHO-UMC criteria (certain, probable/likely, possible, unlikely) (Edwards and Biriell, 1994).
AEs, adverse events.
The treatment retention rate was 92%. The incidence rate of the overall AEs registered during the study, whether or not related to fluoxetine, was 10.4 for 100 person-month follow-up (95% CI: 5.6–19.4). The incidence rate of AEs related to the medication was 3.2 for 100 person-month follow-up (95% CI: 1.2–8.5).
Psychometric outcomes
Nonverbal intellectual functioning
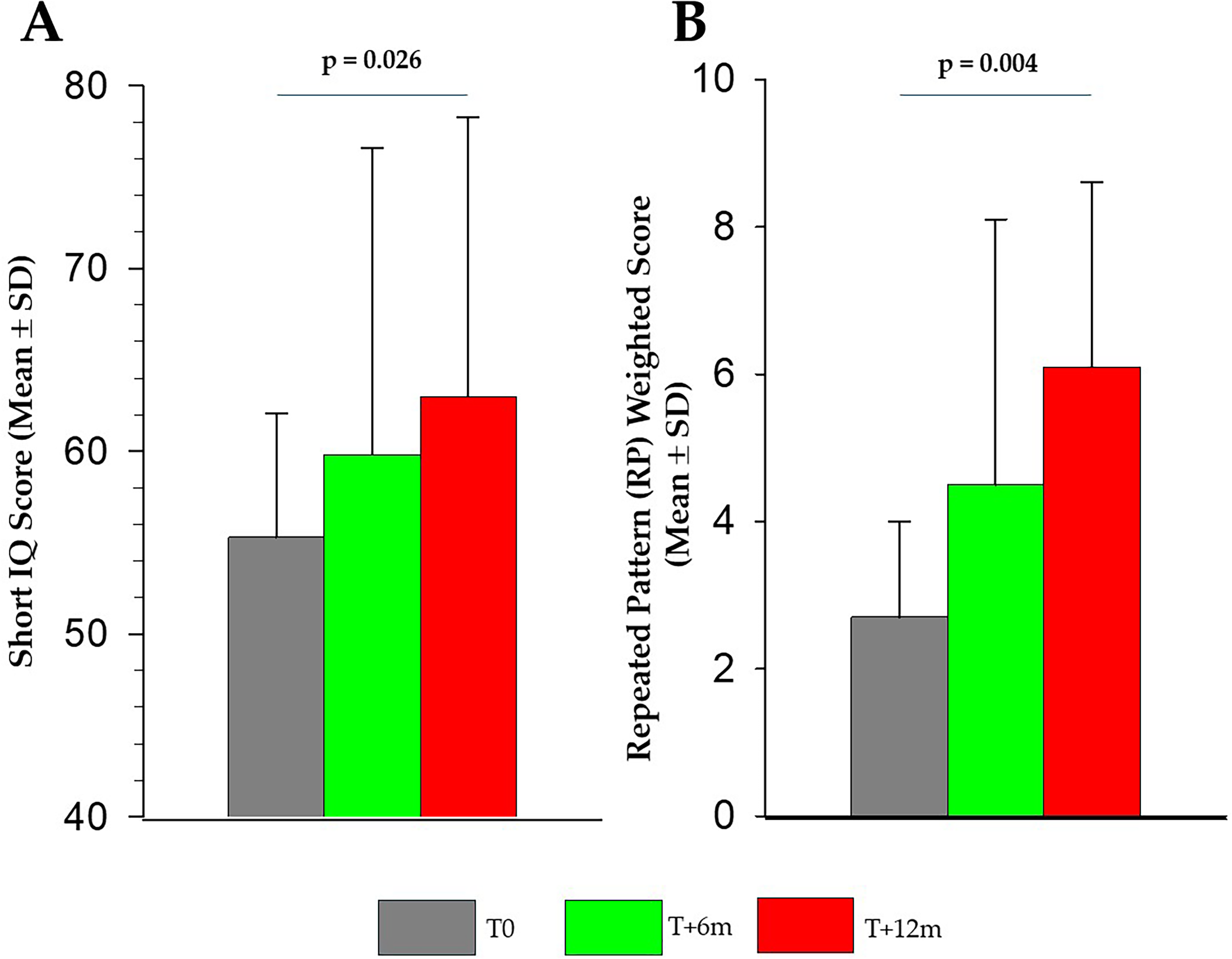
Results from the Leiter-R scale showed an improvement in short-IQ, driven by better performance in the “Repeated Pattern” weighted scores, an index of logical reasoning based on visual stimuli (Fig. 3; Supplementary Table S6). Mean short-IQ improved from 55.3 ± 6.8 (T0) to 59.8 ± 16.8 (+4.5 points) (T+6m; p = 0.373) and to 63 ± 15.3 (+8.4 points) (T+12m; p = 0.026) (Fig. 3). “Repeated Pattern” mean scores were 2.7 ± 1.3 at T0, 4.5 ± 3.6 at T+6m (p = 0.07), and 6.1 ± 2.5 at T12m (p = 0.004) (Fig. 3).
Results of the Leiter-R test (N = 11): short-IQ
Hippocampus-dependent tasks
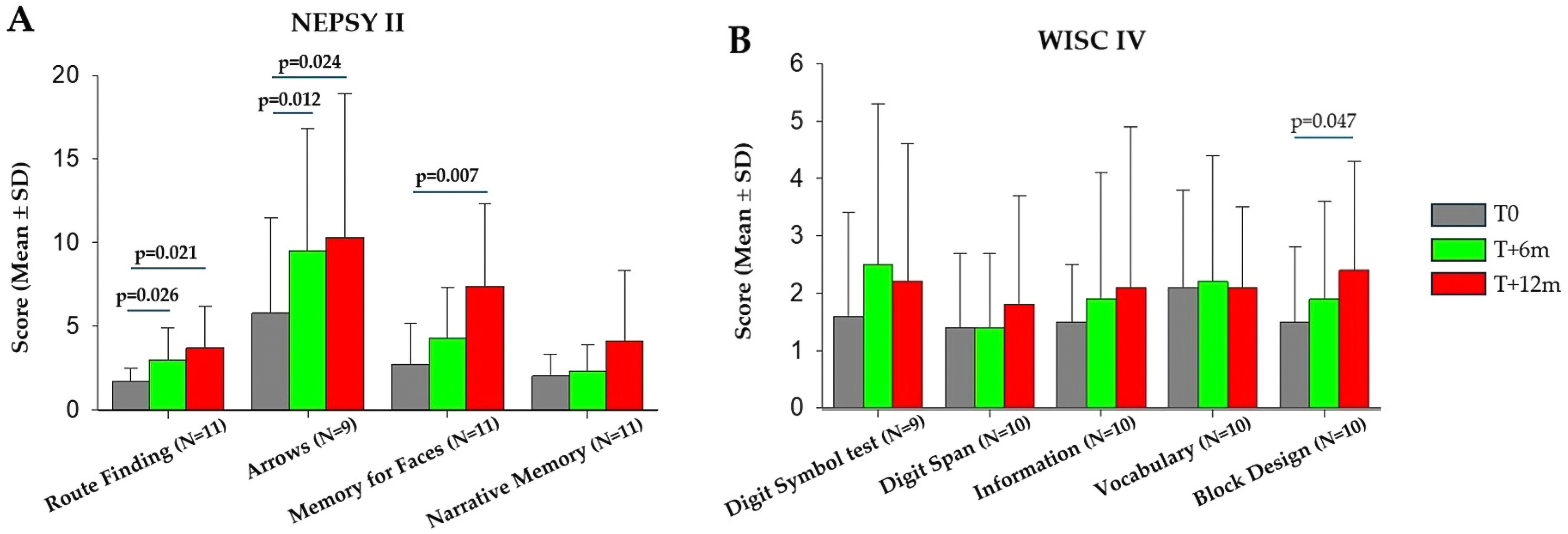
NEPSY-II subtests indicated significant improvements in visuospatial processing both at T+6m and at T+12m. The “Route finding,” an index of knowledge of visuospatial relationships and orientation, improved at T+6m (p = 0.026) and at T+12m (p = 0.021) (Fig. 4; Supplementary Table S7). “Arrows” test, an index of the ability to judge the orientation and distance of lines in a two-dimensional space, improved at T+6m (p = 0.012) and at T+12m (p = 0.024). Memory and Learning domain showed improvements only at T+12m in the “Memory for faces” subtest, an index of immediate retrieval skills of short and long-term memory (p = 0.007) (Fig. 4; Supplementary Table S7). Regarding WISC-IV, none of the subtests analyzed showed differences during the study, with the exception of the “block design” test, in which we observed an improvement of the scores during the study, although the difference was significant only at T+12m but not at T+6m (Fig. 4; Supplementary Table S7).
Results of the NEPSY-II
Adaptive behavior
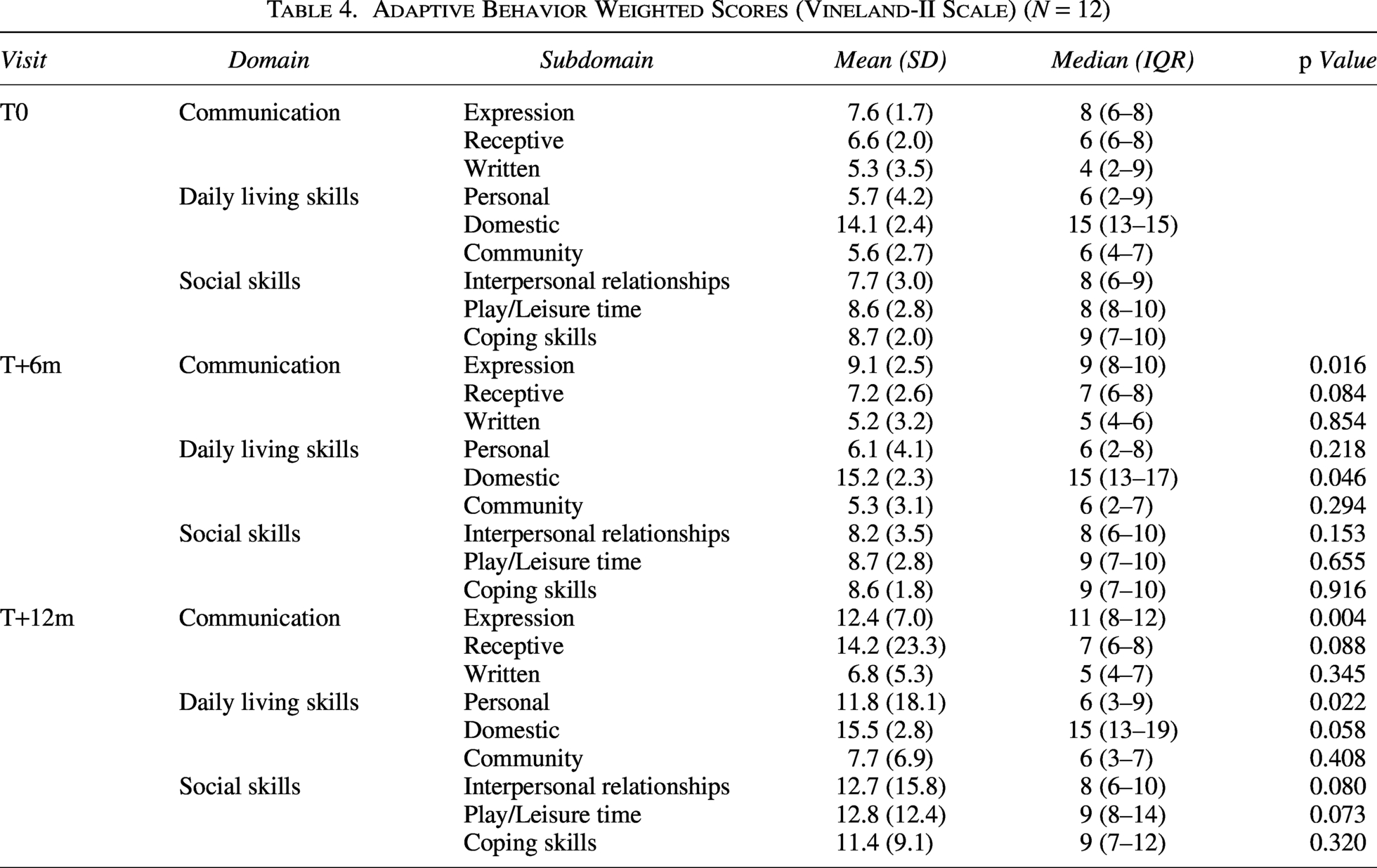
Vineland-II scores improved for verbal expression (T+6m, p = 0.016; T+12m, p = 0.004), domestic (T+6m, p = 0.046), and personal domains (T+12m, p = 0.022) (Table 4).
Adaptive Behavior Weighted Scores (Vineland-II Scale) (N = 12)
Discussion
Over the past two decades, studies in mouse models have demonstrated that pharmacological interventions can ameliorate abnormalities in neurogenesis, dendritogenesis, and myelination (Fatemi et al, 2024; Lindberg et al., 2023; López-Hidalgo et al., 2024; Manfredi-Lozano et al., 2022; Stagni and Bartesaghi, 2022; Vázquez-Oliver et al., 2025). These preclinical findings have paved the way for the first translational studies in humans. Beyond the extensive cognitive stimulation programs implemented in rehabilitation settings, researchers are now investigating whether it is possible to pharmacologically enhance psychomotor development in infancy, counteract the decline in IQ scores from childhood through adolescence, and mitigate neurodegeneration in adulthood. Few studies in adults or adolescents with DS have addressed cognition using pharmacological or nutraceutical approaches (Cieuta-Walti et al., 2022; Costa et al., 2022; de la Torre et al., 2016; Goeldner et al., 2022; Manfredi-Lozano et al., 2022; Mircher et al., 2020; Rafii et al., 2022; Rosenbloom et al., 2020; Spiridigliozzi et al, 2016). As pioneering experiences, these studies remain heterogeneous regarding both the investigational medications and the cognitive outcome measures employed. The patients’ age is another important consideration. It is known that the gaps in learning skills and performance compared to typically developing individuals widen over lifespan (Carr, 1995, 2012; Carr and Collins, 2018; Pulina et al., 2019). Early pharmacological intervention may therefore be essential to achieve meaningful cognitive benefits. Also, cognitive profiles within DS are themselves highly variable. Despite these limitations, a small number of pilot studies and placebo-controlled trials suggest that certain aspects of cognition can be modulated by pharmacological or nutraceutical treatments (Cieuta-Walti et al., 2022; de la Torre et al, 2016; Manfredi-Lozano et al., 2022). Importantly, across all studies, AEs were generally mild, with no indication of serious AEs specifically depending on trisomy 21 (Cieuta-Walti et al., 2022; Costa et al., 2022; de la Torre et al., 2016; Goeldner et al., 2022; Manfredi-Lozano et al., 2022; Mircher et al., 2020; Rafii et al., 2022; Rosenbloom et al., 2020; Scala et al., 2021; Spiridigliozzi et al, 2016). In preclinical studies using the Ts65Dn mouse model, perinatal, neonatal, and adult fluoxetine administration enhanced neurogenesis and synaptogenesis (Bianchi et al., 2010; Fatemi et al., 2024; Guidi et al., 2013; 2014; Stagni et al., 2013; 2015b), supporting the rationale for translational research.
This exploratory study reports findings on the safety and tolerability of fluoxetine in children with DS. Regarding safety, administration of fluoxetine 10 mg/day for 6 months did not produce any serious AEs or SAEs. Regarding tolerability, the overall retention rate was high (92%). AEs included symptoms that may have been related to fluoxetine and warrant specific investigation and mitigation strategies in future trials. In particular, terminal insomnia—defined as early-morning awakening with inability to resume sleep—was observed in two female participants (#1, #9; Table 3). Although no protocol modifications were required and the symptom resolved spontaneously in one case, insomnia may affect the quality of life of both children and their families. One of these participants (#1) also experienced transient urticaria between weeks 4 and 6 of the treatment and developed dermatillomania during fluoxetine tapering phase, when the dose was 5 mg/day. These two children did not differ from other participants in fluoxetine or norfluoxetine plasma levels, body weight, psychopathological risk, or sleep apnea history (which was an exclusion criterion). However, retrospective review of baseline data revealed that patient #9 slept fewer hours nightly (7–8 h vs. 9–10 h in other children), suggesting that a specific subgroup of children with DS might be more sensitive to the effects of SSRIs on sleep. One additional participant (#2) reported decreased appetite, headache, and diarrhea, although interpretation was complicated by a concurrent intestinal infection. Besides these 3 patients, the other children remained asymptomatic during the treatment. To enhance tolerability in future studies, several strategies may be considered: (1) a longer dose tapering period, (2) specific evaluation of sleep habits and of predisposing factors that this study was unable to intercept, (3) doses of fluoxetine lower than 10 mg/day. Although 10 mg/day represents the lowest labeled dose and previous studies in adults with DS and in children >5 years with autism have demonstrated good tolerability at 10–40 mg/day, lower doses may be better tolerated in some children with DS.
We also examined performance with a battery of cognitive tests designed to assess hippocampus-dependent functions. A previous study highlighted hippocampal dysfunction in children and adolescents with DS (Pennington et al., 2003). Although our study was not powered to assess efficacy, we aimed to identify potential endpoints for future trials. Psychometric testing showed a nonsignificant increase of mean short-IQ scores after 6 months of fluoxetine, which became statistically significant after the 6-month follow-up (T+12m). This improvement was primarily driven by gains in the “Repeated Patterns” subtest, which assesses logical reasoning. Significant enhancement of visuospatial and orientation skills was observed after 6 months of fluoxetine, as reflected by the visuospatial domain of the NEPSY-II scale. The improvement was retained after 6 months of follow-up. We hypothesize that the observed improvement in short-IQ, driven by the Repeated Pattern task, reflects a broader enhancement of visuospatial and nonverbal cognitive functions. This interpretation is supported by concurrent gains in visuospatial subtests (Leiter-R Repeated Patterns; NEPSY-II Route Finding and Arrows). Such domain-specific improvement may be grounded in the neuropsychological profile of individuals with DS, characterized by relatively stronger visuospatial abilities (Marino et al., 2019; Onnivello et al., 2022; Pulina et al., 2019). These findings suggest that visuospatial performance and visuoperceptive reasoning may be modulated by fluoxetine. With regard to adaptive behavior, it is noteworthy that the “Expression” subdomain improved at both T +6 and T +12 months, reflecting an enhanced ability among the children to convey their thoughts, needs, and ideas verbally. In contrast to the improvements observed in the Leiter-R and NEPSY-II, no significant gains were found in WISC-IV subtests (with the only exception of the Block design task at T+12m). This discrepancy may reflect the greater reliance of WISC-IV tasks on verbal reasoning mediated processes and auditory attention—functions that are relatively vulnerable in DS—compared with the predominantly visuospatial demands of the other measures. We also observed that mean scores on certain psychometric tests improved at T+12m compared with T+6m (Figs. 3 and 4). Several hypotheses may explain this pattern. (1) The improvement may reflect the effects of ongoing conventional rehabilitative therapies during the trial. However, prior studies of IQ trajectories in DS report stability or decline, with improvement being uncommon (Carr, 1995, 2012; Carr and Collins, 2018; Liogier d’Ardhuy et al., 2015). (2) Fluoxetine, even at the low doses used here, may have reduced anxiety during testing or increased mood activation, allowing better abilities in daily activities and practical reasoning. This hypothesis, however, does not fully explain the persistence of gains during the follow-up. (3) The observed improvements may reflect “practice effect.” While the absence of a control group precludes ruling out potential learning effects associated with repeated task exposure, the retest interval was established in line with standardized test manuals, which recommend a minimum interval of 6 months between assessments to reduce this source of bias (Korkman et al., 2007; Roid and Miller, 2002; Sparrow et al., 2016; Wechsler, 2012). (4) Consistent with animal data (Bianchi et al., 2010; Stagni et al., 2013; 2015b), fluoxetine may promote hippocampal plasticity, thereby improving cognitive performance. This hypothesis should be addressed in future double-blind, placebo-controlled trials, including a follow-up period of at least 6 months.
This study presents limitations and strengths. The main limitations include the small sample size and the absence of a placebo group. Recruitment was challenging due to exclusion criteria (reflecting common DS comorbidities) and parental hesitancy toward psychopharmacological research. The challenges associated with recruiting patients with DS for psychopharmacological trials, compared to other neurogenetic syndromes, were recently highlighted in the paper by Gracias et al. (2025). In their open-label trial investigating fluoxetine for depression in adults with DS, the authors failed to meet their recruitment target: only 3 subjects completed the study out of the 25 patients originally planned over a 25-month recruitment period. Interestingly, the authors compared this experience with a parallel, successful trial of buspirone for anxiety in Williams syndrome (Thom et al., 2025). The authors suggested that challenges may arise from limited foundational research, underestimation of the small eligible population, and weak partnerships with patient associations. In our case, more extensive foundational and clinical research on cognitive profiles and developmental trajectories within specific age windows would have strengthened trial design, improved communication with families and advocacy groups, and fostered engagement with medical communities. We also underestimated the impact of comorbidities. This limitation could be mitigated in the future by multicenter clinical trials. This study also has strengths. (1) It provides novel data on the safety and tolerability of fluoxetine in children with DS younger than 10 years—the youngest cohort investigated to date in pharmacological trials. (2) The exploratory efficacy endpoints specifically targeted hippocampus-dependent functions, aligning with preclinical evidence. (3) The study addressed visuospatial reasoning and adaptive behavior, key domains for improving daily functioning in individuals with DS.
Conclusions
This pilot study demonstrates that fluoxetine at 10 mg/day is safe in children with DS aged 6–10 years and outlines strategies to optimize tolerability in future clinical trials. The exploratory efficacy findings suggest potential improvements in visuospatial abilities, reasoning, and expression. These results provide a rationale for future placebo-controlled studies designed to confirm and extend these observations. Until such further research is conducted, the use of fluoxetine to treat the intellectual disability in children with DS is not yet supported.
Clinical Significance
Habilitative therapies are the mainstay for improving cognition in DS, but they are not curative. Pharmacological treatments targeting pathophysiological mechanisms may promote cognitive development. The present study stems from preclinical evidence of abnormalities in serotonergic systems in DS and the beneficial effects of fluoxetine. Although preliminary, these results show that fluoxetine may improve visuospatial and reasoning performance and provide a translational rationale for future studies.
Authors’ Contributions
Literature search: I.S., M.M., M.P.R., E.C., R.B., and P.S.; study design: I.S., R.B., C.B., M.M., and P.S.; conceptualization: I.S., R.B., C.B., and M.M.; data collection: I.S., O.S., V.M., and G.T.; data analysis: I.S., O.S., and V.M.; funding acquisition: R.B.; investigation: I.S., C.B., M.M., O.S., V.M., M.P.R., G.T., D.C., E.C., R.B., and P.S.; methodology: I.S., R.B., C.B., and M.M.; supervision: I.S., C.B., R.B., and P.S.; validation: I.S., M.P.R., and R.B.; writing—original draft: I.S. and R.B.; writing—review and editing: I.S., R.B., V.M., G.T., E.C., and P.S. All authors have read and agreed to the published version of the article.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and approved by the ISS (n. 30891(17)-PRE21-1580), the Italian Medicines Agency (AIFA, n. 134021), and the Institutional Ethics Committee (n. 222/17). Written informed consent was provided by parents or legal guardians, and children gave assent (when possible) after the study information sheet was explained in age-appropriate language. All data were collected at the Department of Maternal and Child Health, Federico II University Hospital.
Footnotes
Acknowledgments
The authors wish to express our gratitude to the patients and their families whose participation made this study possible.
Data Availability Statement
Disclosures
The authors declare no conflict of interest.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.