
Abstract
Background:
Management of acute agitation in youth frequently involves intramuscular (IM) antipsychotics; however, little is known about how treatment strategies vary across care settings. Differences between emergency and inpatient psychiatric environments may influence medication selection and dosing.
Methods:
This retrospective secondary analysis included youth (<18 years) who received IM antipsychotics for agitation across multiple emergency departments and inpatient psychiatric units within a large urban health system (2019–2023). Comparisons between settings examined antipsychotic selection, coadministration of adjunctive medications, and dosing. To account for differences in medication selection, dosing comparisons were conducted within each antipsychotic agent. Secondary outcomes included repeat IM administration and restraint or seclusion within 24 hours.
Results:
The sample included 158 youth (86 emergency, 72 inpatient). Antipsychotic selection differed significantly by setting, with greater use of haloperidol in emergency settings and chlorpromazine in inpatient settings (p < 0.001). Midazolam coadministration was more common in emergency settings (10.5% vs. 1.4%, p = 0.020). When examined within agents, chlorpromazine doses were higher in inpatient settings (36.7 mg vs. 30.4 mg, p = 0.035), while haloperidol and olanzapine dosing did not differ. Rates of additional IM administration were similar across settings (p = 0.295), although restraint or seclusion was more common in inpatient settings (p < 0.001).
Conclusions:
Pharmacologic management of pediatric agitation varies by care setting, particularly in antipsychotic selection and adjunctive medication use. Differences in dosing were limited to chlorpromazine, suggesting that variation reflects agent-specific prescribing patterns rather than overall treatment intensity. These findings highlight the influence of clinical context and provider practice patterns in shaping management strategies for pediatric agitation.
Keywords
Introduction
Agitation among youth presenting to the hospital for psychiatric concerns is common across care settings, with agitation being reported in about 7% of emergency department (ED) visits and a history of aggression reported in about a third of youth admitted to psychiatry (John et al., 2023; Salvi et al., 2022). Acute agitation is a high-risk state that can escalate into aggression and violence if not promptly recognized and addressed (Salvi et al., 2022). Agitation can cause significant distress and may lead to injury of the patient, caregivers, or medical staff (Foster et al., 2024). Common interventions for agitation include verbal de-escalation, environmental modification, and oral medications; however, when these fail, intramuscular (IM) medications (often antipsychotics) are frequently used (Gerson et al., 2019; Hoffmann et al., 2023; Mills et al., 2026). Most existing literature focuses on comparing specific IM antipsychotics in terms of clinical outcomes, while relatively little is known about how treatment strategies vary across care settings (Bourke et al., 2023; Gerson et al., 2019; Hoffmann et al., 2023; Mills et al., 2026).
Inpatient psychiatric units and the ED are fundamentally different care environments. The therapeutic goals of parenteral medication in the ED often emphasize rapid stabilization, given the time-sensitive nature of the environment (Isoardi et al., 2026; Kim et al., 2021). In addition, emergency physicians are often expected or required to intervene prior to the patient being seen by a consulting psychiatrist (Brown et al., 2017). In contrast, inpatient units involve more longitudinal care, emphasizing the prevention of agitation and aggression with attention to staffing, staff training, and milieu programming (Saito et al., 2025). Physicians and other staff on inpatient child and adolescent (CAP) psychiatric units may have greater familiarity with pediatric patients in psychiatric crisis, including subpopulations such as those with autism spectrum disorder (ASD) or intellectual disability (ID) (Dean et al., 2007; Salvi et al., 2022).
These differences in care environments may contribute to providers’ medication choices and dosing strategies. Prior work, while able to examine outcomes such as restraints or seclusion, has rarely standardized the severity or nature of agitation (Hoffmann et al., 2023; Saidinejad et al., 2023). Studies have also rarely examined differences in practice patterns across settings (Hoffmann et al., 2023; Saidinejad et al., 2023). Therefore, it remains unclear whether differences in management reflect patient factors, provider practice patterns, or both.
This study aimed to address this gap by examining differences in IM antipsychotic selection, coadministration, and dosing among youth receiving IM antipsychotics for agitation across emergency and inpatient psychiatric settings. By focusing on youth who required IM antipsychotics, the present study examines a cohort with a relatively uniform threshold of agitation severity. We hypothesized that management strategies would differ by setting, reflecting differences in clinical context and provider practice patterns.
Methods
Study design and setting
This study is a secondary analysis of an IRB-approved retrospective chart review conducted within the Mount Sinai Health System (Protocol #24-00101) examining patterns of pharmacologic management of acute agitation across clinical settings. The Mount Sinai Health System is a large, private academic medical network in New York City comprising multiple EDs and inpatient psychiatric units across several campuses, including Mount Sinai Hospital, Mount Sinai Beth Israel, Mount Sinai Brooklyn, Mount Sinai Queens, Mount Sinai Morningside, and Mount Sinai West. The patient population served by this system is demographically diverse and broadly representative of New York City and the surrounding metropolitan area. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Study population
The parent dataset included all pediatric patients under the age of 18 who received an IM antipsychotic medication for the management of acute agitation in any participating ED or inpatient psychiatric unit between January 1, 2019, and December 31, 2023. Eligible encounters were identified through medication administration records and confirmed through manual electronic medical record (EMR) review.
For this secondary analysis, IM antipsychotics included chlorpromazine, haloperidol, and olanzapine. Although olanzapine was infrequently used, it was retained for descriptive analyses. To ensure independence of observations, only the first agitation-related encounter during which an IM antipsychotic was administered was included for patients with multiple encounters during the study period. For youth who received an IM antipsychotic in the ED and were subsequently admitted to inpatient psychiatry, only the initial ED episode was included to maintain a consistent unit of analysis.
Data abstraction and variables
Members of the study team (R.B., A.I.C., C.N., S.T.L.) abstracted data from the EMR using a standardized data collection protocol. Extracted variables included baseline sociodemographic characteristics (age at encounter, gender identity, race) and clinical history variables, including number of prior psychiatric hospitalizations, history of violence, history of ASD or ID, and history of substance use.
Encounter-level variables included the clinical context of care (ED/comprehensive psychiatric emergency program [CPEP] vs. inpatient psychiatry), reason for presentation, and primary billing diagnosis. Medication-related variables included the antipsychotic administered, dose of the administered agent, and coadministration of benzodiazepines (lorazepam or midazolam) or diphenhydramine.
Interrater reliability was assessed across variables on a subset of charts and exceeded 95%. Discrepancies or ambiguous data points were reviewed by the full study team to achieve consensus. Missing data were minimal, and analyses were conducted using available data for each variable.
Outcomes
The primary outcomes of this secondary analysis were patterns of antipsychotic selection, coadministration of adjunctive medications, and dosing of antipsychotics across clinical settings. Antipsychotic dosing was examined both overall and within each agent to account for differences in medication selection.
Secondary outcomes included the need for additional IM antipsychotic administration within 24 hours and the occurrence of restraint or seclusion within 24 hours, which were included to contextualize differences in management strategies across settings.
Statistical analysis
All analyses were conducted using IBM SPSS Statistics for Windows, version 31.0 (IBM, 2025). Descriptive statistics were calculated for all study variables, including means and standard deviations for continuous variables and frequencies and percentages for categorical variables.
Comparisons between emergency and inpatient settings were conducted using independent-samples t-tests for continuous variables and chi-square or Fisher’s exact tests for categorical variables, as appropriate. Effect sizes were reported using Cohen’s d for continuous variables and Cramer’s V for categorical variables.
To account for differences in antipsychotic selection across settings, dosing comparisons were additionally conducted within each antipsychotic agent. All statistical tests were two-tailed, with a significance threshold of p < 0.05.
Results
Sample characteristics
The sample included 158 youth, with 86 treated in emergency settings and 72 in inpatient psychiatry. Patients treated in emergency settings were slightly older than those treated in inpatient settings (mean 12.6 vs. 11.6 years, t = 2.06, df = 156, p = 0.041, d = 0.34). There were no significant differences in gender or race (Table 1).
Baseline Characteristics of Youth Receiving Intramuscular Antipsychotics by Care Setting
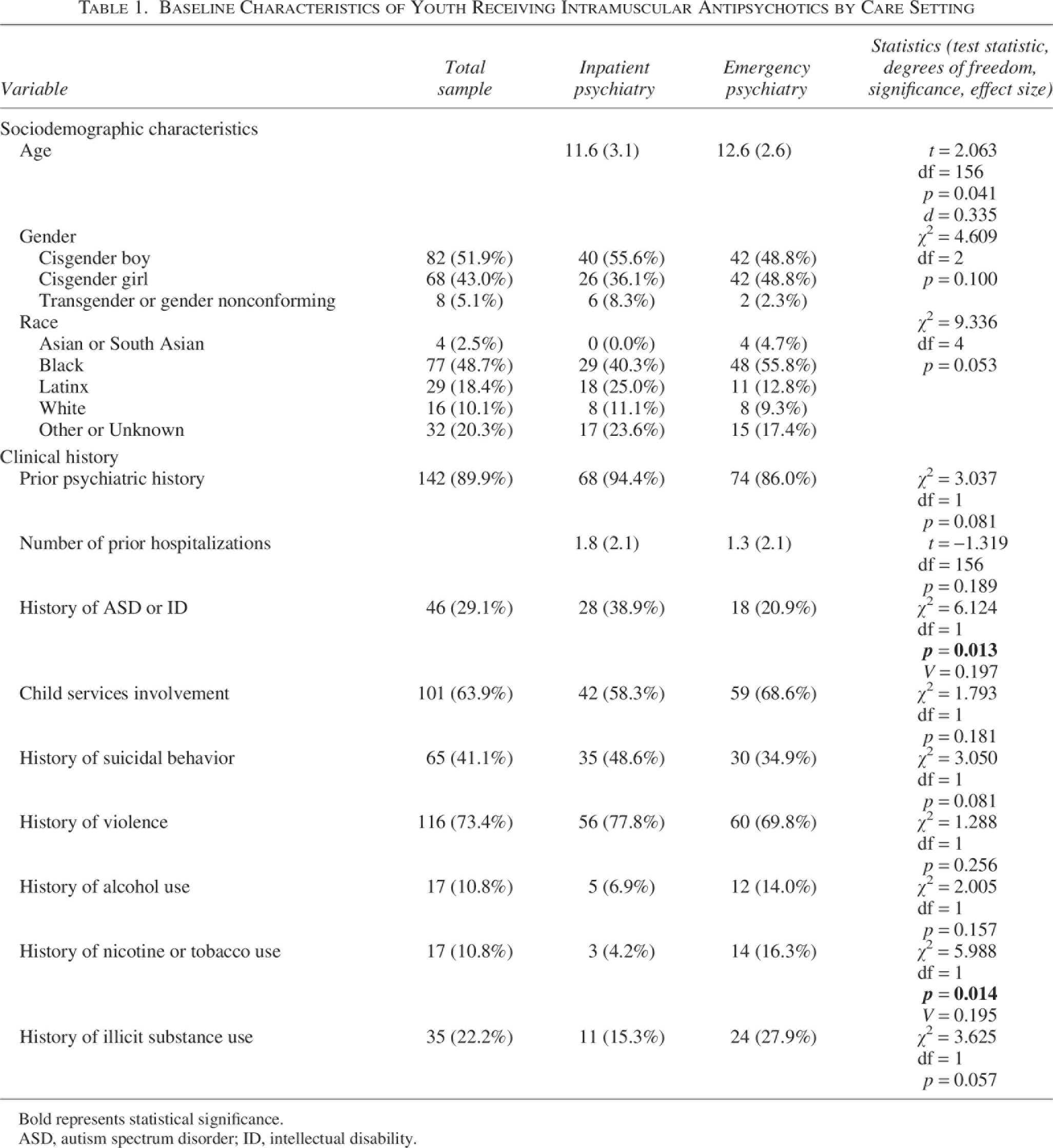
Bold represents statistical significance.
ASD, autism spectrum disorder; ID, intellectual disability.
Clinical characteristics were largely similar across settings. However, youth treated in inpatient settings were more likely to have a history of ASD or ID (38.9% vs. 20.9%, χ2 = 6.12, df = 1, p = 0.013, V = 0.20). History of nicotine or tobacco use was more common in emergency settings (16.3% vs. 4.2%, χ2 = 5.99, df = 1, p = 0.014, V = 0.20) (Table 1). Primary diagnostic categories differed significantly between settings (χ2 = 13.91, df = 3, p = 0.003, V = 0.30), with a higher proportion of mood and anxiety disorders in inpatient settings and a greater proportion of “other” diagnoses in emergency settings.
Antipsychotic selection and coadministration
Antipsychotic selection differed significantly by care setting (χ2 = 17.43, df = 2, p < 0.001, V = 0.33). Haloperidol was more commonly administered in emergency settings (40.7% vs. 11.1%), whereas chlorpromazine was more frequently used in inpatient settings (83.3% vs. 54.7%). Olanzapine use was uncommon in both settings (Table 2).
Clinical Characteristics, Medication Use, and Outcomes by Care Setting
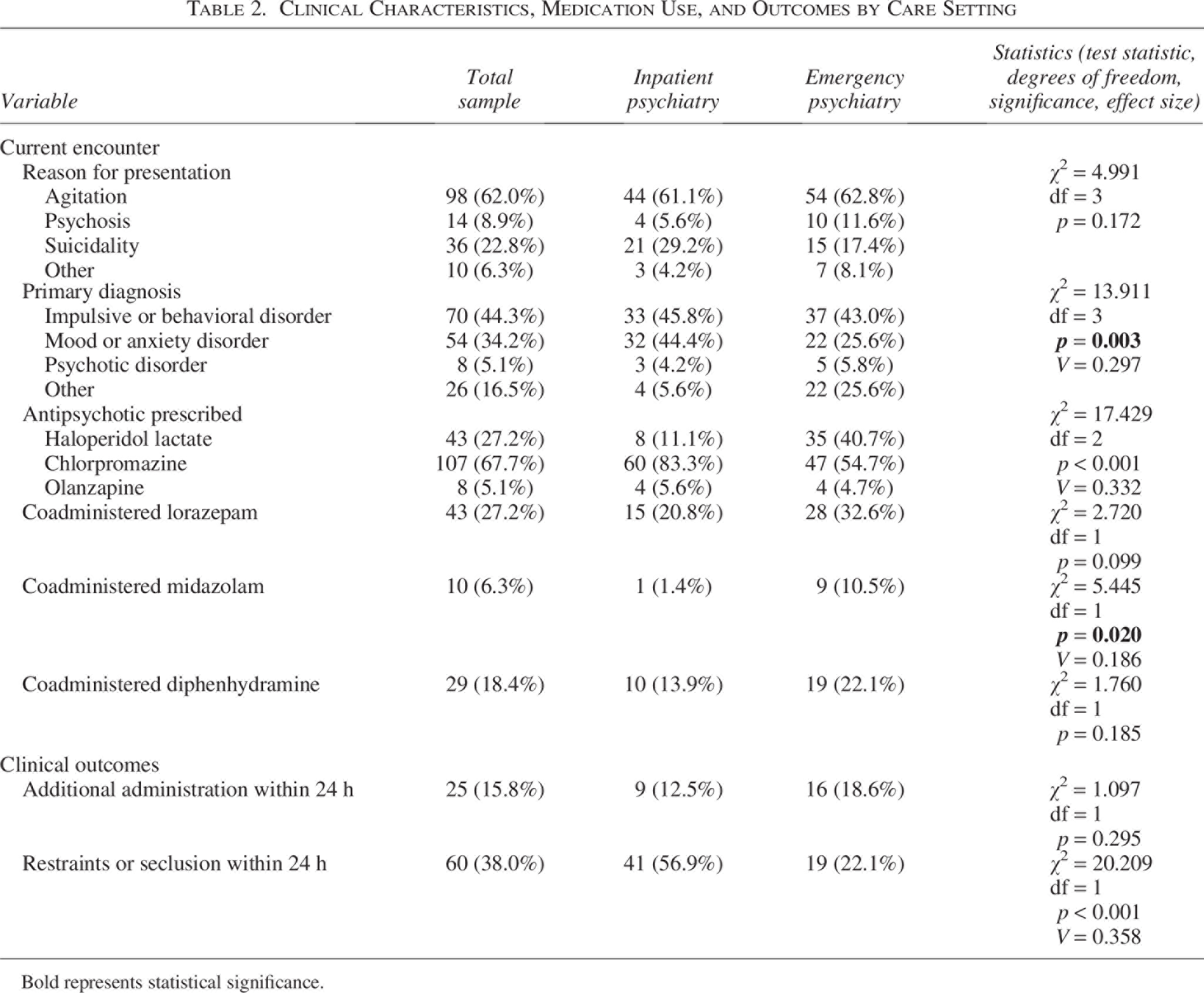
Bold represents statistical significance.
Coadministration patterns also varied. Midazolam was more frequently coadministered in emergency settings (10.5% vs. 1.4%, χ2 = 5.45, df = 1, p = 0.020, V = 0.19), while there were no significant differences in lorazepam or diphenhydramine coadministration (Table 2).
Antipsychotic dosing
To account for differences in antipsychotic selection, dosing comparisons were conducted within each agent. Chlorpromazine doses were significantly higher in inpatient settings compared to emergency settings (mean 36.7 mg vs. 30.4 mg, t = −2.14, df = 105, p = 0.035, d = −0.42). In contrast, there were no significant differences in dosing for haloperidol (4.1 mg vs 4.6 mg) or olanzapine (5.0 mg vs 4.4 mg) between settings (Table 2).
Clinical outcomes
Rates of additional antipsychotic administration within 24 hours did not differ significantly between settings (18.6% emergency vs. 12.5% inpatient, χ2 = 1.10, df = 1, p = 0.295). However, restraints or seclusion within 24 hours were significantly more common in inpatient settings (56.9% vs. 22.1%, χ2 = 20.21, df = 1, p < 0.001, V = 0.36) (Table 2). Exploratory analyses did not identify significant racial differences in antipsychotic selection or restraint/seclusion outcomes.
Discussion
In this retrospective study of youth who received IM antipsychotics for agitation, results indicate significant differences across care setting in the selection of antipsychotic agents as well as coadministration of midazolam. Only chlorpromazine dosing differed between the inpatient unit and the ED, and outcomes were largely similar. Overall, these findings suggest that treatment of pediatric agitation varies substantially by care setting, particularly in medication selection and use of adjunctive agents, while overall short-term outcomes remain similar.
One possible explanation for these differences is variation in clinician familiarity and practice patterns across care settings (Mills et al., 2026; Rettew et al., 2015). Clinicians in the ED may also frequently manage agitation in the adult population and be more comfortable with haloperidol compared to chlorpromazine, compared to inpatient clinicians (Stetson and Osser, 2022; Uribe et al., 2025; Yip et al., 2020). In addition, they may be more familiar with benzodiazepine coadministration (Brown et al., 2017; Stetson and Osser, 2022). This may also explain why chlorpromazine was used at lower doses in emergency settings, potentially reflecting more cautious use or less familiarity with its dosing in pediatric populations (Mills et al., 2026). In contrast, inpatient child and adolescent psychiatry providers may be more accustomed to using chlorpromazine for behavioral dysregulation, particularly in structured settings where ongoing observation and repeated dosing are feasible. Notably, olanzapine use was uncommon across both settings despite increasing literature and consensus recommendations supporting second-generation antipsychotics, particularly olanzapine, in the management of pediatric agitation (Gerson et al., 2019; Hoffmann et al., 2023). Several factors may contribute to this pattern, including institutional prescribing culture, provider familiarity with older agents such as chlorpromazine and haloperidol, historical formulary or order-set practices, and concerns regarding coadministration with benzodiazepines. These findings may reflect the lag that can occur between evolving evidence-based recommendations and real-world prescribing practices across hospital systems.
Differences in treatment strategies may also reflect differences in patient populations, particularly the higher prevalence of neurodevelopmental disorders in inpatient settings, where chlorpromazine is commonly used for behavioral dysregulation (Morris et al., 2025; Neuhaus et al., 2022). However, the persistence of differences in medication selection and dosing suggests that setting-related practice patterns likely play an independent role. Importantly, these findings suggest that both patient-level factors and provider-level factors contribute to treatment decisions and that these influences may be difficult to fully disentangle in observational studies.
Notably, differences in dosing were not observed across all agents. When examined within individual antipsychotics, only chlorpromazine doses differed between settings, while haloperidol and olanzapine dosing were similar. This suggests that there are agent-specific differences tied to how these medications are prescribed across care settings (Hoffmann et al., 2023; Yip et al., 2020). Rather than reflecting a generalized tendency toward higher or lower dosing in one setting, these findings support the interpretation that dosing differences are closely linked to the clinical role and familiarity of specific medications. This highlights the importance of examining dosing within agents, as aggregate comparisons may obscure these more nuanced patterns.
These findings have important clinical implications. The finding that despite significant practice variation, outcomes were largely similar suggests that there may be multiple acceptable strategies for managing agitation in the hospital setting (Gerson et al., 2019; van Schalkwyk et al., 2017; Yip et al., 2020). In addition, it highlights the lack of standardization of agitation management in youth, including guidance on medication selection and dosing across clinical settings (Hoffmann et al., 2023; Mills et al., 2026; Saidinejad et al., 2023). This variability may reflect the absence of consensus guidelines that are specific to pediatric populations and adaptable across care environments. Future work may benefit from developing setting-informed guidelines that account for differences in workflow, patient populations, and provider expertise, while promoting consistency in safe and effective care. Future quality improvement initiatives may also benefit from examining barriers to implementation of evidence-based pediatric agitation pathways and greater standardization of second-generation antipsychotic use across care settings.
This study has several limitations, including its retrospective nature and observational design. In addition, this study relied on the review of the EMR, which introduces the possibility of variability and incompleteness in recorded data, particularly for clinical variables such as agitation severity, behavioral context, and rationale for medication selection. The study period also spanned the COVID-19 pandemic, during which pediatric psychiatric presentations and behavioral acuity changed substantially across many health systems. Because the present study was not designed or powered to evaluate temporal changes in practice patterns, potential pandemic-related effects could not be fully assessed. A key limitation is the potential for confounding by indication, as medication choice and dosing may reflect underlying differences in patient presentation that were not fully captured in the available data. Relatedly, although this study focused on youth receiving IM antipsychotics to approximate a consistent threshold of agitation severity, it was not possible to fully control for differences in the severity, acuity, or etiology of agitation across encounters. Differences in patient populations between settings, including the higher prevalence of ASD/ID in inpatient settings, may also have influenced treatment decisions. Although exploratory analyses did not identify significant racial differences in management strategies or outcomes, the study was not specifically powered to evaluate racial disparities in pediatric agitation treatment. In addition, some subgroup analyses were limited by small sample sizes, particularly for olanzapine and for haloperidol use in inpatient settings, which may reduce statistical power and limit interpretation of within-agent comparisons. Although the overall sample size may appear modest relative to the study period and size of the health system, the cohort was intentionally restricted to pediatric patients who received IM antipsychotic medications specifically for agitation, representing a narrower and more clinically severe subset of psychiatric presentations. In addition, only first encounters were included to preserve the independence of observations. Finally, clinical setting was closely associated with medication selection, such that differences attributed to setting may in part reflect differences in preferred pharmacologic strategies, making it difficult to fully disentangle the independent effects of setting versus medication choice.
Despite these limitations, this study has several notable strengths. It includes a relatively large, multisite sample drawn from a diverse urban health system, enhancing generalizability. By focusing on youth who required IM antipsychotics, the study examines a clinically meaningful population with a relatively standardized threshold of agitation severity. In addition, the analysis of dosing within individual antipsychotic agents represents a methodological strength, allowing for more precise comparison of prescribing practices across settings while minimizing confounding related to differences in medication selection.
Conclusion
In this multisite retrospective study, management of pediatric agitation differed significantly between emergency and inpatient psychiatric settings, particularly in antipsychotic selection and adjunctive medication use. Differences in dosing were limited to chlorpromazine, suggesting that variation in practice is driven more by agent selection than by overall prescribing intensity. These findings underscore the influence of clinical context and provider practice patterns in shaping treatment approaches for pediatric agitation.
Authors’ Contributions
S.T.L.: Conceptualization, data curation, formal analysis, writing (original draft); A.I.C.: Data curation, data interpretation, writing (review & editing); R.B.: Data curation, data interpretation, writing (review & editing); C.N.: Data curation, data interpretation, writing (review & editing); T.R.R.: Supervision, data interpretation, writing (review & editing); A.N..S.: Supervision, data interpretation, writing (review & editing).
Ethical Approval
This study was approved by the Institutional Review Board at the Icahn School of Medicine at Mount Sinai, and a waiver of informed consent was obtained (Protocol #24-00101).
Use of Generative AI
The authors used generative artificial intelligence tools to assist with language editing and stylistic refinement of the article. All content decisions, data interpretation, analyses, and conclusions were made by the authors, who take full responsibility for the accuracy and integrity of the work.
Footnotes
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, S.T.L., upon reasonable request.
Clinical Significance
Management of pediatric agitation requiring intramuscular antipsychotic medication varies substantially across emergency and inpatient psychiatric settings. In this multi-site study, differences were observed in antipsychotic selection, adjunctive medication use, and chlorpromazine dosing, despite generally similar short-term outcomes. These findings suggest that local practice patterns and clinical context may influence treatment decisions as much as patient factors. Greater standardization of evidence-based approaches to pediatric agitation may help reduce unwarranted variation in care while maintaining safe and effective treatment.
Disclosures
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article. The authors alone are responsible for the content and writing of this article.