
Abstract
Introduction:
Neurodevelopmental disorders (NDDs), including Autism Spectrum Disorder (ASD), Fragile X syndrome (FXS), and Rett Syndrome (RTT), share impairments in cognitive and behavioral functioning and may involve an altered excitatory/inhibitory balance modulated by the endocannabinoid system. This systematic review evaluated the safety and efficacy of cannabinoid-based products (CBPs) in these pediatric NDDs.
Methods:
We conducted a systematic review according to Preferred Reporting Items of Systematic Reviews and Meta-Analyses (PRISMA) 2020, including randomized and nonrandomized studies of patients under 18 years treated with cannabidiol (CBD), cannabidivarin (CBDV), tetrahydrocannabinol (THC), or their combinations. Outcomes were adverse events (AEs) and treatment discontinuation, seizure reduction, and behavioral and cognitive changes. Study quality and certainty of evidence were assessed using design-specific risk-of-bias tools and the GRADE approach.
Results:
Seventeen studies (two randomized controlled trials, observational studies, and case series) met the inclusion criteria. Across diagnoses, CBPs were generally associated with mild-to-moderate AEs and low discontinuation rates. Descriptive pooled proportions suggested behavioral improvements in ASD and FXS and seizure reduction in RTT, with exploratory analyses indicating differential effects of CBD versus CBD + THC on behavioral and cognitive outcomes in ASD.
Conclusion:
CBPs may offer potential benefits for selected behavioral symptoms and comorbid epilepsy in pediatric NDDs, but current evidence is insufficient to support routine clinical use. High-quality randomized controlled trials with standardized outcome measures and long-term follow-up are needed to clarify efficacy, safety, and syndrome-specific effects.
Introduction
Neurodevelopmental disorders (NDDs) constitute a group of conditions that manifest early in life, significantly impairing personal, social, academic, and occupational functioning (American Psychiatric Association, 2013).
Although the etiopathogenesis of these disorders is complex and varies depending on the specific phenotype, one of the most widely discussed hypotheses involves a disruption in the excitatory/inhibitory (E/I) balance. This imbalance is thought to result from increased levels of excitatory neurotransmitters and/or decreased levels of inhibitory neurotransmitters, particularly γ-aminobutyric acid (Rubenstein and Merzenich, 2003). Such imbalance is associated with altered synaptic plasticity and connectivity—hallmarks of many NDDs—as well as an increased risk of epilepsy due to heightened cortical excitability (Sohal and Rubenstein, 2019).
In recent years, the endocannabinoid system has gained increasing attention as a potential therapeutic target in NDDs. Both endogenous cannabinoids and phytocannabinoids have been shown to modulate excitatory and inhibitory synaptic transmission through the activation of cannabinoid receptors (CB1 and CB2), with potentially beneficial effects on social behavior, communication, and cognitive functions (Mechoulam and Parker, 2013). In parallel, cannabis derivatives have emerged as a well-established adjunctive treatment for drug-resistant epilepsies and developmental and epileptic encephalopathies, exerting anticonvulsant, neuroprotective, and anti-inflammatory effects, partly through the downregulation of pro-inflammatory cytokines (Foiadelli et al., 2023; Pesántez Ríos et al., 2025; Rice et al., 2024).
Based on this evidence, medical cannabis and its derivatives—such as cannabidiol (CBD), cannabidivarin (CBDV), and tetrahydrocannabinol (THC)—have been investigated in pharmacological trials involving adults with neuropsychiatric conditions to assess their safety and efficacy (Black et al., 2019). More recently, the use of cannabinoid-based products (CBPs) has been extended to pediatric populations with NDDs, although for most conditions, the evidence remains limited and largely based on nonrandomized or uncontrolled studies (Rice et al., 2024).
Among the CBPs most commonly investigated in this context, CBD, THC, and CBDV show distinct pharmacodynamic profiles. CBD, one of the most prominent components of cannabis, was initially utilized as an analgesic. It functions as an allosteric modulator of the CB1 receptor and a weak antagonist at the CB2 receptor, as well as interacting with the 5-HT1A, vanilloid receptor type 1, and D2 receptors. THC acts primarily as a partial agonist of the CB1 receptor in the brain, exhibits psychoactive effects, and may lower seizure threshold (Whalley et al., 2019). The two interacting compounds are involved in the regulation of numerous cognitive and behavioral processes (Szkudlarek et al., 2019). CBDV is a non-hallucinogenic analog of CBD that can cross the blood–brain barrier and has a weak affinity for CB1 receptors. It acts by reducing intracellular calcium and thus neuronal excitability (Hurley et al., 2022).
The aim of this review was to systematically summarize and critically appraise studies evaluating CBPs in pediatric patients with Autism Spectrum Disorder (ASD), Fragile X Syndrome (FXS), or Rett Syndrome (RTT). Specifically, we sought to describe: (1) safety outcomes, including the type and frequency of adverse events (AEs) and treatment discontinuation; and (2) efficacy outcomes, including reduction in the frequency of seizures and changes in behavioral and cognitive functioning, as measured by standardized tools or caregiver/clinician reports. Despite their distinct clinical phenotypes, these conditions share an altered E/I balance, as demonstrated in preclinical studies using animal models (Dani et al., 2005; Gibson et al., 2008; Rubenstein and Merzenich, 2003). This common pathophysiological substrate provides a plausible rationale for targeting the endocannabinoid system with CBPs in ASD, FXS, and RTT.
Methods
Search strategy
A systematic search of MEDLINE (PubMed), Scopus, Embase, and Cochrane Library was performed by two authors independently in June 2025, with no restriction on publication date. We restricted inclusion to articles published in English, which may have introduced language bias. This systematic review was conducted and reported in accordance with the PRISMA 2020 statement. The PRISMA flow diagram is provided as Supplementary Data.
This review was focused on the administration of CBPs in children and adolescents with a diagnosis of ASD, FXS, or RTT.
The search syntax used the following keywords: (“cannabis” OR “medical cannabis” OR “medicinal cannabis” OR “Epidiolex” OR “THC” OR “Tetrahydrocannabinol” OR “cannabidiol” OR “CBD” OR “cannabidivarin” OR “CBDV” OR “cannabinoid”) AND (“neurodevelopment* disorder” OR “autism” OR “autism spectrum disorder” OR “autistic disorder” OR “Asperger” OR “Intellectual disability” OR “Rett syndrome” OR “Rett” OR “Fragile X Syndrome” OR “Fragile X”).
Protocol and registration
The protocol for this systematic review was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number CRD420261306831).
Inclusion and exclusion criteria
The following eligibility criteria were used:
Inclusion criteria: pediatric patients up to the age of 18 years with a diagnosis of ASD according to DSM-5, or intellectual disability genetically determined consistent with FXS or RTT; administration of CBD, or THC, or CBD and THC, or CBDV. Articles eligible for inclusion were randomized controlled trials (RCTs), observational studies, open-label trials, uncontrolled trials, case series, and case reports. Exclusion criteria: texts not in the English language; articles not peer-reviewed; papers including adults and children where the exact number of subjects under the age of 18 could not be determined.
Study selection
Two authors (S.B. and L.B.) blindly extracted the clinical information. Discrepancies were resolved through discussion until consensus was reached; in cases of disagreement, a third reviewer (G.P.) resolved the issue.
Risk of bias and study quality were independently assessed by both reviewers (Supplementary Fig. S1).
Outcomes
We evaluated outcomes of safety and efficacy. Safety outcomes included the presence and type of AEs and discontinuation of treatment. Efficacy outcomes were estimated based on behavioral and cognitive improvements (as assessed by neuropsychological testing and caregivers’ impressions) and reduction in the frequency of seizures, evaluated by impressions of parents or clinicians. Due to the substantial heterogeneity across studies, behavioral and cognitive outcomes could not be evaluated or compared using uniform assessment tools. Furthermore, efficacy results were extracted and reported as originally defined by the primary studies, which were often based on the impressions of caregivers or physicians and on different assessment scales that were difficult to compare. The only standardized instruments used across studies were the Aberrant Behavior Checklist (ABC), the Clinical Global Impressions scale (CGI), the Rett Syndrome Behavior Questionnaire (RSBQ), the Home Situations Questionnaire (HSQ), and the Autism Parenting Stress Index (APSI), each applied only in a minority of studies and exclusively to assess behavioral or emotional outcomes rather than cognitive functioning. As a result, behavioral and cognitive outcomes could not be grouped into a single standardized quantitative measure, and any comparisons between groups should therefore be interpreted with caution.
Quality assessment
The quality of evidence and risk of bias for each included study were evaluated using
JBI Critical Appraisal Checklist for Case Reports (Moola S et al., 2017) NIH Quality Assessment Tool for Case Series Studies (Moola S et al., 2017) NIH Guidance for Assessing the Quality of Observational Cohort and Cross-Sectional Studies (National Heart, Lung, and Blood Institute, 2014) A revised Cochrane risk-of-bias tool for randomized trials (RoB-2) (Sterne et al., 2019) GRADE (Grading of Recommendations Assessment, Development, and Evaluation) approach for overall evidence quality (high, moderate, low, very low) (Guyatt et al., 2008)
Statistical analysis
For each diagnostic group (ASD, FXS, RTT), we calculated pooled proportions for key outcomes (AEs, treatment discontinuation, seizure reduction, and behavioral or cognitive improvement) by summing the number of participants with a given outcome over the total number of enrolled participants across all included studies within that group. These pooled proportions were derived irrespective of study design (randomized controlled trials, observational studies, case reports), risk of bias, or outcome measurement tools, and should therefore be interpreted as descriptive and exploratory. Statistical analyses were then conducted on the entire cohort using pairwise comparisons across the three main groups (ASD vs. FXS, ASD vs. RTT, FXS vs. RTT) for these outcomes, as well as within the ASD group to compare different CBPs. Descriptive statistics were provided for all variables: continuous variables were reported as mean, median, and range (minimum–maximum), while categorical variables were summarized using absolute and relative frequencies. Group comparisons for categorical variables were performed using Fisher’s exact test. Given the substantial heterogeneity in study design, sample size, and outcome definitions, the resulting p-values are intended only to highlight potential patterns and must be interpreted with great caution. No continuous variables were subjected to inferential testing, and formal statistical tests of heterogeneity and nonparametric analyses were not performed. All statistical analyses were conducted using Python (version 3.x) and appropriate statistical libraries, with a two-tailed p-value <0.05 considered statistically significant.
Results
Preliminary research yielded a total of 2692 articles. After the elimination of duplicates, 1378 articles remained. Two authors (S.B. and L.B.) selected articles by title and abstract independently; 274 articles were selected for screening. A total of 17 articles satisfied the inclusion criteria. The articles excluded from the study met one or more of the following criteria: they were not pertinent to the research, included populations of adults and children that were difficult to discriminate, were not written in English, or had not undergone the peer-review process (Supplementary Figure S1; Fig. 1).
Comparative analysis across study groups and cannabinoid-based products (CBPs).
We report the main safety and efficacy characteristics noted in the studies, subdivided by pathology.
Autism spectrum disorder: Safety and efficacy
Regarding ASD, 11 articles met our inclusion criteria. In nine studies, the CBP administered was a combination of CBD and THC (CBD + THC), (Aran et al., 2019; Bar-Lev Schleider et al., 2019; David et al., 2024; Fleury-Teixeira et al., 2019; Ma et al., 2022; Mazza et al., 2024; Ponton et al., 2020; Siani-Rose et al., 2023; Silva et al., 2024), while in the remaining studies only CBD was used (Bilge and Ekici, 2021; Raz et al., 2022). In all studies, the proportion of males was markedly higher than that of females.
With regard to safety, CBPs were generally well tolerated. The only randomized, double-blind, placebo-controlled trial of CBD + THC in ASD reported no treatment discontinuations and only minor AEs in 15% of participants, none of which interfered with study continuation (Silva et al., 2024). Across observational studies, the percentage of discontinuation was minimal and exceeded 25% of the sample in only one study (David et al., 2024). AEs, although frequent in some cohorts (e.g., 72% in Fleury-Teixeira et al.), showed predominantly mild-to-moderate severity (Bar-Lev Schleider et al., 2019; Bilge and Ekici, 2021; Fleury-Teixeira et al., 2019; Mazza et al., 2024; Siani-Rose et al., 2023; Silva et al., 2024). A single serious AE (SAE), a psychotic episode leading to treatment discontinuation, was reported in the study by Aran et al. (2019). In most studies, at least half of the participants were receiving concomitant pharmacological treatments (antiepileptic drugs or psychotropic medications) at the time of CBPs administration, which may have influenced both tolerability and safety profiles (Aran et al., 2019; Bar-Lev Schleider et al., 2019; Bilge and Ekici, 2021; Fleury-Teixeira et al., 2019; Ma et al., 2022; Mazza et al., 2024; Ponton et al., 2020; Raz et al., 2022; Silva et al., 2024).
In terms of efficacy, observational studies and case reports consistently documented improvements in behavioral symptoms, particularly reductions in aggression, irritability, and anxiety (Bilge and Ekici, 2021; David et al., 2024; Ma et al., 2022; Mazza et al., 2024; Ponton et al., 2020; Raz et al., 2022; Siani-Rose et al., 2023). Improvements in social and/or verbal communication were reported in four studies (Bilge and Ekici, 2021; Fleury-Teixeira et al., 2019; Ponton et al., 2020; Raz et al., 2022), whereas three studies described reductions in repetitive behaviors (David et al., 2024; Mazza et al., 2024; Siani-Rose et al., 2023). These findings support the hypothesis that modulation of the endocannabinoid system may influence core or associated symptoms of ASD. A reduction in sleep–wake rhythm dysregulation was also described in five studies in which CBD + THC formulations were administered (Bar-Lev Schleider et al., 2019; David et al., 2024; Fleury-Teixeira et al., 2019; Ma et al., 2022; Ponton et al., 2020). Patients with comorbid epilepsy were included in three reports (Bar-Lev Schleider et al., 2019; Fleury-Teixeira et al., 2019; Ponton et al., 2020), and two of these described reductions in seizure frequency; however, due to differences in study design and outcome reporting (only Fleury-Teixeira et al. quantified seizure reduction as a percentage), robust conclusions regarding antiseizure efficacy cannot be drawn (Bar-Lev Schleider et al., 2019; Fleury-Teixeira et al., 2019).
Among the 11 ASD studies, 1 was a randomized, double-blind, placebo-controlled trial, 7 were observational (including one prospective study), and 3 were case reports. The trial by da Silva et al. showed significant improvements in social interaction, anxiety, and psychomotor agitation in the active-treatment group, but raised some concerns regarding randomization procedures and outcome assessment, leading to a moderate risk of bias (Silva et al., 2024). The observational studies were limited by small sample sizes, lack of blinding, and heterogeneous, often poorly defined outcome measures, with more rigorous assessment only in the studies by Mazza et al. (Mazza et al., 2024) and Siani-Rose et al. (Siani-Rose et al., 2023).
The case reports provided detailed clinical descriptions but, owing to their anecdotal nature and infrequent use of validated scales, contributed very low-certainty evidence. GRADE assessments for each ASD study are reported in Table 1.
Characteristics, Efficacy, and Safety of Studies on Cannabinoid-Based Products (CBP) in the Treatment of Autism Spectrum Disorder in Children and Adolescents
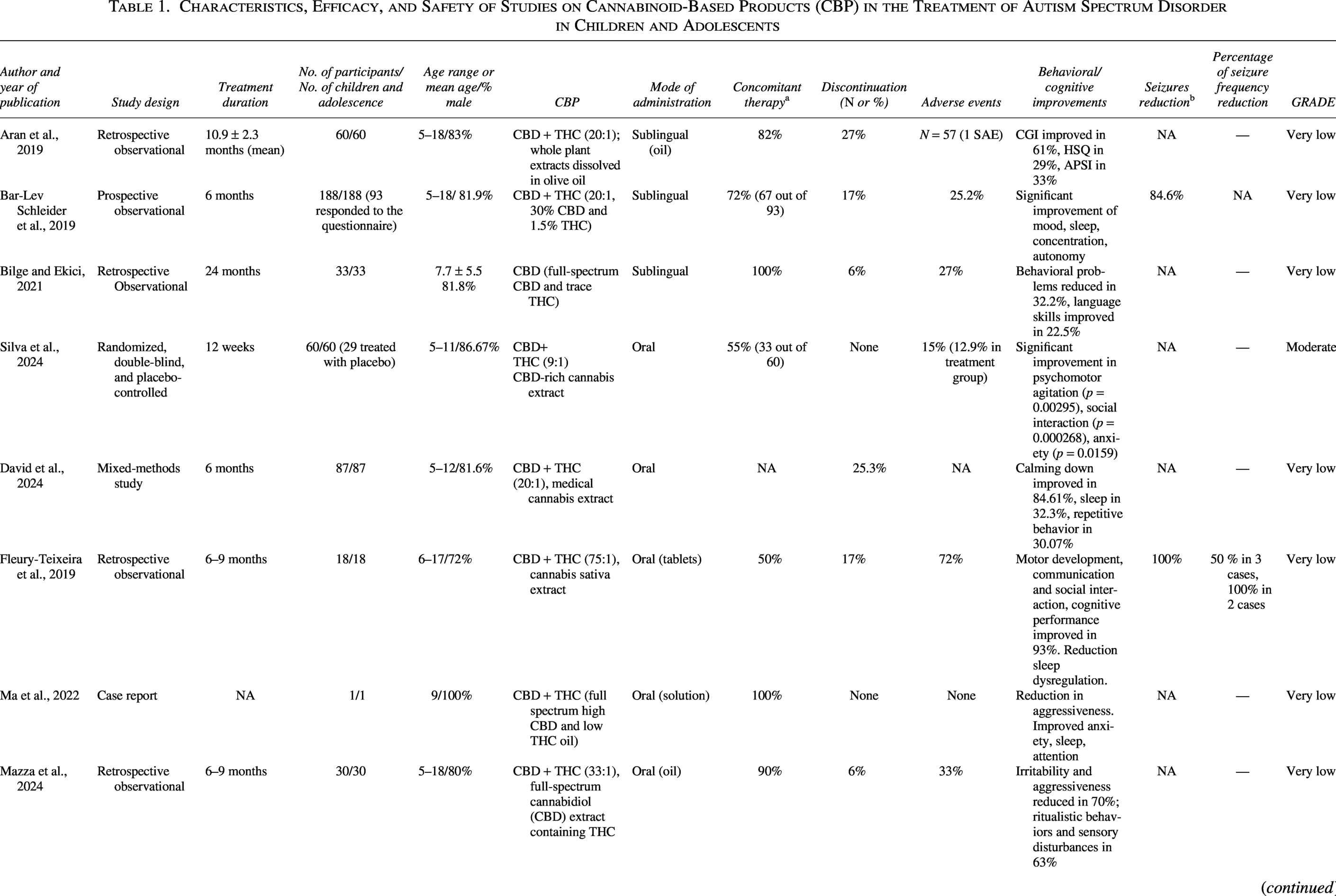
Percentage of patients who were taking concomitant therapy.
Percentage of patients who demonstrated a reduction in seizure frequency.
APSI, Autism Parenting Stress Index; CBD, cannabidiol; CGI, Clinical Global Impression; GRADE, Grading of Recommendations Assessment, Development and Evaluation; HSQ, Home Situations Questionnaire; NA, not available; THC, tetrahydrocannabinol.
Rett syndrome: Safety and efficacy
Our analysis revealed three papers that satisfied the inclusion criteria for RTT (Desnous et al., 2024; Divisic et al., 2021; Hurley et al., 2022). The samples of all three studies consisted exclusively of female patients, which is consistent with the known sex distribution of RTT, although sporadic male cases have been reported (Neul et al., 2019). Across studies, patients exhibited complex clinical pictures characterized by severe cognitive impairment and drug-resistant epilepsy, typically managed with antiseizure medications (ASM) (Desnous et al., 2024; Divisic et al., 2021; Hurley et al., 2022).
From a safety perspective, CBPs were generally well tolerated. No treatment discontinuation was reported in any study (Desnous et al., 2024; Divisic et al., 2021; Hurley et al., 2022). AEs, including infections, somnolence, and gastrointestinal disturbances, occurred in all patients receiving CBDV (Hurley et al., 2022), and in the RTT patient treated with CBD + THC in the case series by Divisic et al. (Divisic et al., 2021), whereas only one patient experienced AEs in the study by Desnous et al. (Desnous et al., 2024). In all cases, these events were mild and did not lead to treatment cessation. The absence of control groups and the small sample sizes, however, limit the precision with which safety can be characterized.
In terms of efficacy, all three studies reported some degree of seizure reduction associated with CBP treatment (Desnous et al., 2024; Divisic et al., 2021; Hurley et al., 2022). Desnous et al. described a reduction in seizure frequency greater than 50% in six patients, with one participant achieving a seizure-free period during treatment with CBD (Epidiolex®) (Desnous et al., 2024). Hurley et al. also observed decreases in seizure frequency, defined as reductions >50% in seizure diaries across the treated cohort (Hurley et al., 2022). Beyond seizure control, two studies noted improvements in spasticity (Desnous et al., 2024; Divisic et al., 2021), and in the case series by Divisic et al., the RTT patient additionally showed better sleep and quality of life (Divisic et al., 2021). Nonetheless, the strength of these efficacy signals is constrained by important methodological limitations. The studies by Hurley et al. and Desnous et al. were observational, with benefits rated by parents or physicians without blinded assessment, and in Desnous et al., seizure outcomes were not systematically captured with diaries, reflecting the retrospective design (Desnous et al., 2024; Divisic et al., 2021; Hurley et al., 2022). The third study was a small case series in which only one RTT patient met our inclusion criteria, and outcome reporting for domains such as spasticity, sleep, and behavior was nonstandardized and incomplete (Divisic et al., 2021). Consequently, the overall quality of evidence for RTT is low to very low, as reflected in the GRADE assessments summarized in Table 2.
Characteristics, Efficacy, and Safety of Studies on Cannabinoid-Based Products (CBP) in the Treatment of Rett Syndrome in Children and Adolescents
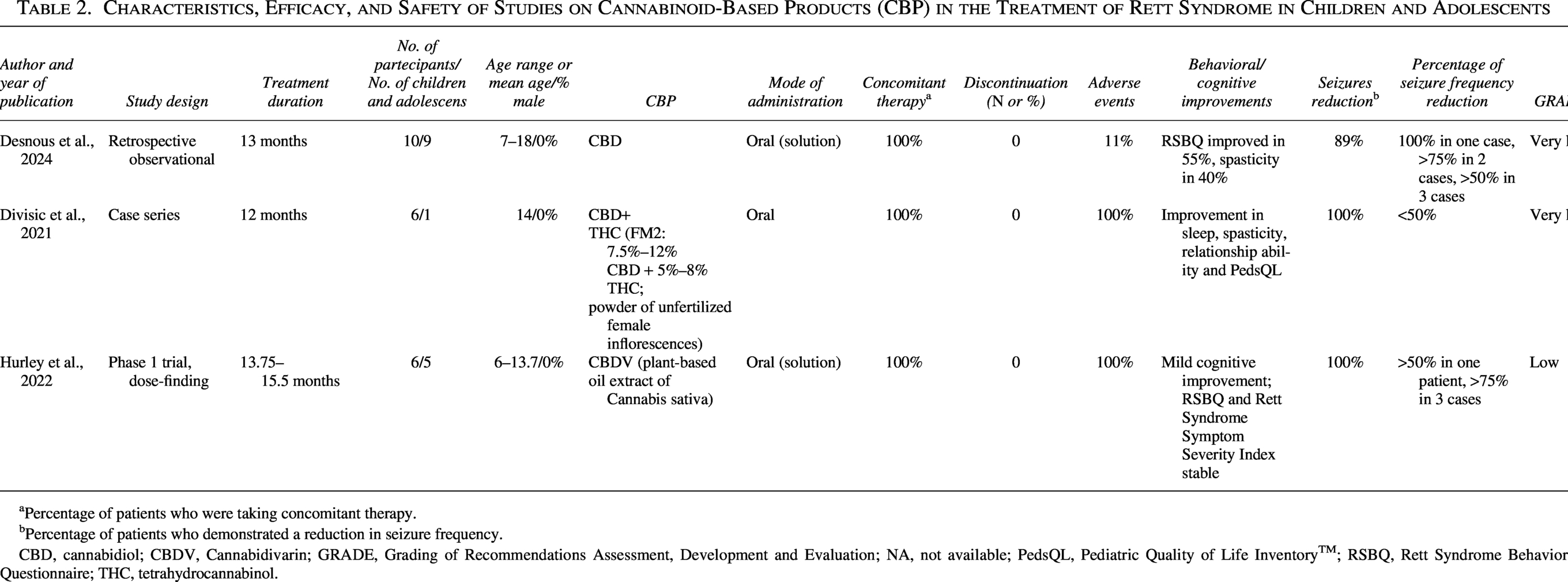
Percentage of patients who were taking concomitant therapy.
Percentage of patients who demonstrated a reduction in seizure frequency.
CBD, cannabidiol; CBDV, Cannabidivarin; GRADE, Grading of Recommendations Assessment, Development and Evaluation; NA, not available; PedsQL, Pediatric Quality of Life InventoryTM; RSBQ, Rett Syndrome Behavior Questionnaire; THC, tetrahydrocannabinol.
FXS: Safety and efficacy
We identified three papers that met our inclusion criteria for FXS: a randomized, placebo-controlled trial, a phase 1/2 open-label trial, and a case series (Berry-Kravis et al., 2022; Heussler et al., 2019; Tartaglia et al., 2019). In all studies, the CBP used was CBD-based (Berry-Kravis et al., 2022; Heussler et al., 2019; Tartaglia et al., 2019), and the proportion of male patients was consistently high, accounting for at least 75% of participants in each cohort (Berry-Kravis et al., 2022; Heussler et al., 2019; Tartaglia et al., 2019). CBD administration was generally well tolerated, with minimal withdrawal rates. In the randomized trial by Berry-Kravis et al., only one patient discontinued treatment, and in the open-label trial by Heussler et al., two patients withdrew (Berry-Kravis et al., 2022; Heussler et al., 2019). In the Tartaglia case series, the single patient who met our criteria continued treatment without experiencing adverse events. (Tartaglia et al., 2019). Across the two trials, more than half of CBD-treated patients reported at least one adverse event, with rates up to 85% in the Heussler study, but these were predominantly mild to moderate and did not lead to study interruption (Berry-Kravis et al., 2022; Heussler et al., 2019). Reported events were frequently skin reactions related to the transdermal gel formulation (Berry-Kravis et al., 2022; Heussler et al., 2019). No SAEs were documented in any of the FXS studies (Berry-Kravis et al., 2022; Heussler et al., 2019; Tartaglia et al., 2019).
Regarding efficacy, all three studies described improvements in behavioral domains among CBD-treated patients (Berry-Kravis et al., 2022; Heussler et al., 2019; Tartaglia et al., 2019). In the trials by Berry-Kravis et al. and Heussler et al., standardized rating scales demonstrated overall clinical improvement from the caregivers’ perspective as well as reductions in aberrant behaviors on the Aberrant Behavior Checklist–Community (ABC–C) (Berry-Kravis et al., 2022; Heussler et al., 2019). In Berry-Kravis et al., these effects were particularly pronounced in the subgroup of individuals with promoter methylation of the FMR1 gene >90%, suggesting a potential genotype–phenotype interaction (Berry-Kravis et al., 2022). Heussler et al. additionally reported reductions in psychiatric symptoms commonly associated with FXS, including anxiety and depressive features, alongside gains in quality of life measures (Heussler et al., 2019). Nevertheless, the certainty of these efficacy findings varies. The Berry-Kravis trial showed a low risk of bias according to RoB-2 across all domains (Berry-Kravis et al., 2022), whereas the open-label trial and the case series were limited by the absence of control groups, lack of blinded outcome assessment, and small sample sizes (Heussler et al., 2019; Tartaglia et al., 2019). Consequently, GRADE ratings ranged from moderate for the randomized trial to very low for the noncontrolled studies, as detailed in Table 3.
Characteristics, Efficacy, and Safety of Studies on Cannabinoid-Based Products (CBP) in the Treatment of Fragile X Syndrome in Children and Adolescents
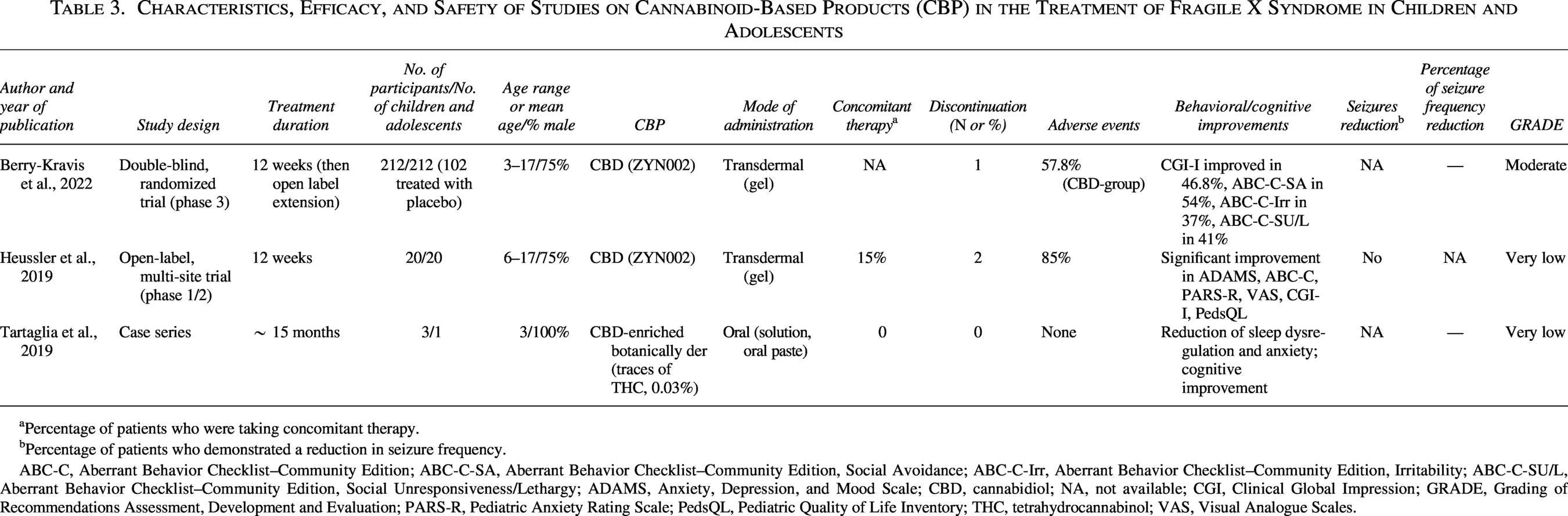
Percentage of patients who were taking concomitant therapy.
Percentage of patients who demonstrated a reduction in seizure frequency.
ABC-C, Aberrant Behavior Checklist–Community Edition; ABC-C-SA, Aberrant Behavior Checklist–Community Edition, Social Avoidance; ABC-C-Irr, Aberrant Behavior Checklist–Community Edition, Irritability; ABC-C-SU/L, Aberrant Behavior Checklist–Community Edition, Social Unresponsiveness/Lethargy; ADAMS, Anxiety, Depression, and Mood Scale; CBD, cannabidiol; NA, not available; CGI, Clinical Global Impression; GRADE, Grading of Recommendations Assessment, Development and Evaluation; PARS-R, Pediatric Anxiety Rating Scale; PedsQL, Pediatric Quality of Life Inventory; THC, tetrahydrocannabinol; VAS, Visual Analogue Scales.
Comparison among populations and CBPs
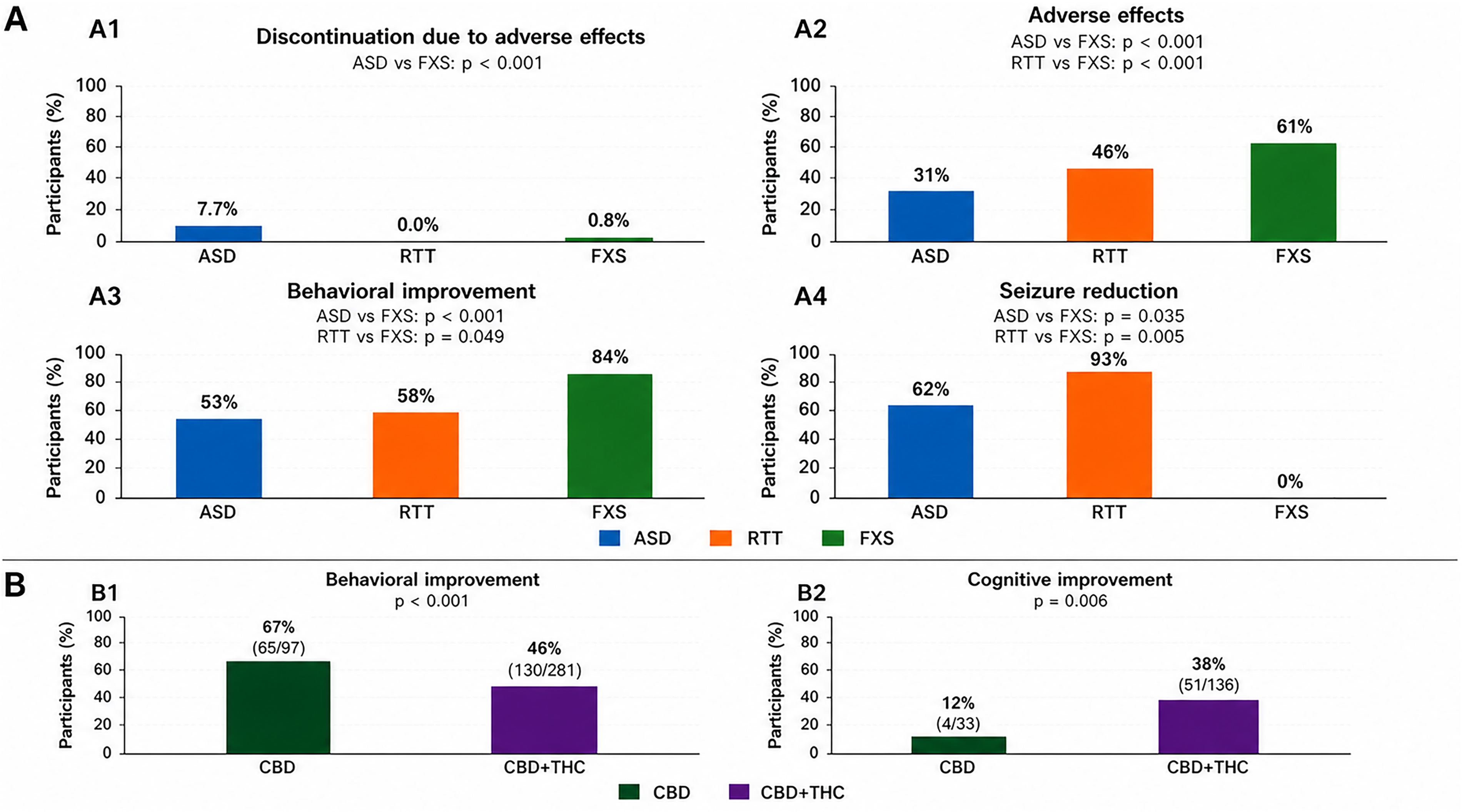
A statistical analysis (pooled proportions) revealed that subjects with ASD exhibited a higher rate of discontinuations secondary to AE compared to subjects in the FXS group (7.7% vs. 0.8%, p = 0.002). However, no significant differences were observed when comparing ASD and RTT (7.7% vs. 0%) or FXS and RTT (0.8% vs. 0%). Discontinuation rates were calculated as the proportion of participants who discontinued intervention (discontinuation/total enrolled subjects) for each diagnostic group across included studies (Fig. 1-A1). Nevertheless, the FXS group exhibited a higher prevalence of AE in comparison to the ASD and RTT groups (61% vs. 31% and 46%, respectively; p < 0.001) (Fig. 1-A2).
Behavioral improvement was higher in the FXS population compared to RTT and ASD groups (84% vs. 58% and 53%, respectively; p = 0.049 and p < 0.001, respectively), whereas no significant difference was observed between ASD and RTT (53% vs. 58%, p = 0.78) (Fig. 1-A3).
The use of CBPs was found to be effective in the treatment of epilepsy when present in comorbidity. Seizure reduction rates were calculated as the percentage of participants who showed improvement in seizures out of the total number of participants enrolled in each diagnostic group. A statistically significant higher proportion of seizure reduction was observed in RTT compared with ASD (93% vs. 62%, p = 0.035) and FXS (93% vs. 0%, p = 0.005), with no difference between ASD and FXS (62% vs. 0%) (Fig. 1-A4).
Within the ASD group, we explored whether efficacy and safety differed according to the type of CBPs, distinguishing between CBD and CBD + THC. Regarding behavioral outcomes, CBD alone was associated with a higher proportion of reported improvement in behavioral issues (e.g., irritability, aggression) compared with CBD + THC (67% [65/97] vs 46% [130/281], p < 0.001; Fig. 1-B1). In contrast, for cognitive outcomes, CBD + THC was associated with a higher proportion of reported improvement than CBD alone (38% [51/136] vs. 12% [4/33], p = 0.006: Fig. 1-B2). No substantial differences were observed between CBD and CBD + THC in terms of AE incidence or withdrawal rates in the ASD group.
Quality of evidence
The quality of evidence was low to very low for most outcomes. For ASD and RTT, most included studies were observational designs or case reports, often with small samples, lack of blinding, and heterogeneous, frequently subjective outcome measures.
Importantly, only two randomized controlled trials were identified across the included literature -one in ASD and one in FXS- and both reached a moderate level of certainty according to the GRADE framework. The remaining evidence was derived predominantly from observational studies, case series, and case reports, resulting in overall low to very low certainty of evidence. Consequently, the current data should be interpreted cautiously and cannot yet support firm clinical recommendations regarding the use of CBPs in pediatric NDDs.
Discussion
The objective of this review was to critically assess the utilization of CBPs in pediatric patients diagnosed with NDDs, specifically ASD, and intellectual disabilities associated with FXS and RTT .
The role of the endocannabinoid system in these disorders is now better recognized and supported by an expanding body of evidence. Indeed, the endocannabinoids anandamide (AEA) and 2-arachidonoyl glycerol (2-AG) appear to be implicated in the maintenance of E/I balance, and thus in synaptic plasticity, the disruption of which is believed to be a potential cause of NDDs, particularly ASD (Mechoulam and Parker, 2013). Studies in mouse models for ASD and FXS have demonstrated that increasing AEA may enhance aspects of socialization by reducing repetitive behaviors. Based on this evidence, clinical trials were initiated to evaluate the efficacy of CBPs by increasing endogenous endocannabinoid levels (Poleg et al., 2019; Wei et al., 2016).
Similarly, RTT has been demonstrated to be associated with increased cortical arousal, as evidenced by the frequent association with epilepsy (Hurley et al., 2022). Studies in mouse models for RTT have demonstrated that the use of CBPs (particularly CBDV) acts on excitability and acts as a 2-AG antagonist, reducing seizures and improving motor and social aspects, which are severely impaired in patients with this diagnosis (Hurley et al., 2022; Mouro et al., 2019). These encouraging results from animal research have led to clinical trials.
Notwithstanding the preliminary constraints and initial skepticism about the utilization of CBPs in many countries, their use has been approved in the adult population. In recent years, studies and approvals are increased in the pediatric population.
Among the reviewed studies, the main compounds investigated were CBD, THC (alone or associated), and CBDV. Their distinct mechanisms of action may help to explain the differential effects we observed on behavioral, cognitive, and seizure outcomes.
The available evidence suggests that CBPs may be generally well tolerated in pediatric patients with NDDs, with mostly mild-to-moderate AEs and low rates of treatment discontinuation; however, the certainty of this evidence is low, and SAEs, although rare, have been reported. In the study conducted by Aran et al. in children and adolescents with ASD, a single SAE was observed (Aran et al., 2019). Notably, ASD patients exhibited a statistically higher rate of discontinuation due to AE compared to the FXS group (p = 0.002). The AE reported in the other studies were classified as mild-to-moderate, consistent with the findings of previous reviews on pediatric case series (Rice et al., 2024). The most frequently documented AE across studies included gastrointestinal disturbances, drowsiness, and airway infections. In FXS patients, skin reactions associated with transdermal formulations were also reported; however, this group exhibited a higher incidence of AE (Berry-Kravis et al., 2022).
In addition to differences in active compounds, variability in route of administration and galenic preparation is likely to have influenced both efficacy and tolerability across studies. In our review, most pediatric patients received oral formulations, with a minority treated with transdermal preparations. Pharmacokinetic data in humans indicate that oral THC exhibits slow and highly variable absorption, with low systemic bioavailability because of extensive first-pass metabolism and its poor aqueous solubility, whereas alternative formulations such as oromucosal or transdermal products can yield distinct and sometimes more sustained exposure profiles (Kaszewska et al., 2025; Lucas et al., 2018). Similarly, CBD is a highly lipophilic compound with low and variable oral bioavailability, largely due to incomplete intestinal absorption and extensive first-pass metabolism, and its systemic exposure is substantially affected by formulation (Kaszewska et al., 2025; Lucas et al., 2018). These differences in the absorption of THC and CBD, which depend on formulation and route of administration, may partly explain the variability in clinical response and adverse-event rates observed across studies and limit the generalizability of findings when different formulations is used.
In most studies, a substantial proportion of participants were receiving concomitant antiepileptic or psychotropic medications at the time of CBPs administration, which may have influenced both the observed tolerability and safety profiles. Several studies, mainly conducted in epileptic encephalopathies, have highlighted the pharmacokinetic and pharmacodynamic impact of CBPs when used in combination with ASM (Roberti et al., 2025).
Regarding efficacy, results suggest a different impact depending on the compound used, and direct comparison across studies is limited due to the heterogeneity of the products administered. Although there are positive outcomes, it is difficult to establish the effect of CBPs on the core symptoms of ASD. Our review found that CBD administration would improve behavioral issues, while the combination of CBD and THC seemed to offer greater benefit on cognitive parameters. This finding, albeit preliminary, is in line with previous studies that have shown significant improvement in socialization with the use of CBD alone, but no significant cognitive gains (Hacohen et al., 2022). Regarding the pharmacological association between THC and CBD, a clear effect on cognitive aspects has not yet been proven, despite this association being very commonly used. The review by Boggs et al. on the interaction of CBD and THC in preclinical and clinical studies showed discordant data with potential negative effects of THC on memory and concentration, apparently decreased by CBD (Boggs et al., 2018). However, the study by Suliman et al. conducted in mouse models showed that THC could be implicated in neurogenesis and cognitive processes. In fact, it appears to increase the expression of brain-derived neurotrophic factor (BDNF) with a consequent increase in synaptic plasticity, promoting memory and learning processes (Suliman et al., 2018). Such results have not been confirmed in human studies, where an exposure exclusively to THC, primarily for recreational purposes, has been shown to cause impairments in executive function, attention, memory, and decision making, deficits limited by CBD coadministration (Boggs et al., 2018).
In the FXS population, where only CBD was administered, outcomes were consistently positive regarding anxiety, depression, and autism-related behaviors, as reported in preclinical studies (Wei et al., 2016). Interestingly, patients with more severe phenotypes, defined by higher promoter methylation of the FMR1 gene, appeared to benefit the most (Berry-Kravis et al., 2022). However, the clinical relevance of these improvements should be interpreted cautiously, given the limited data.
The effectiveness of CBPs in the treatment of seizures is now well known, as evidenced by the approval of CBD (Epidiolex®) for certain epileptic syndromes and by more recent evidence of its use in Rett syndrome and cyclin-dependent kinase-like 5 (CDKL5) deficiency disorder (Arzimanoglou et al., 2020; Vignoli et al., 2025; Wechsler et al., 2024). Consistently, in our review, good seizure control was observed in patients who had epilepsy in RTT. Specifically, 14 out of 15 RTT patients experienced significant seizure reduction (9 of them showed a reduction of >50%), alongside gains in communication and motor functions.
Conclusions
These outcomes, although encouraging, are primarily based on uncontrolled studies and small samples. The heterogeneity and poor quality of many studies (with GRADE ratings very low or low for most outcomes, except for the two double-blind RCTs, which reached moderate quality) prevent the efficacy and tolerability profiles of CBPs from being established with confidence. In addition, our pooled proportions and statistical comparisons across diagnostic groups are derived from heterogeneous studies with differing designs, outcome definitions, CBPs administered, and risk of bias; therefore, these analyses should be regarded as exploratory and cannot support firm inferences about comparative efficacy or safety.
Methodological considerations regarding the two randomized controlled trials deserve further attention.
The ASD randomized, double-blind, placebo-controlled trial was strengthened by its controlled design and structured outcome assessment; however, limitations included relatively small sample size, short treatment duration, and some concerns regarding allocation procedures and heterogeneity of outcome measures.
The FXS phase 3 randomized controlled trial represented the largest and methodologically most robust study included in this review, with adequate blinding and standardized behavioral scales. Nevertheless, subgroup effects (e.g., promoter methylation status), variability in clinical phenotype, and the relatively short, blinded phase limit the generalizability of findings.
Overall, although these trials provide the highest-quality evidence currently available, longer term, and independently replicated studies remain necessary to confirm efficacy and safety profiles.
Clinical Significance
In summary, preliminary data indicate that CBPs could be a useful adjunctive option to antiseizure or psychotropic medication for seizure control in RTT and for behavioral and emotional symptoms in ASD and FXS. The cognitive gains observed with CBD + THC in individuals with ASD are based on preliminary data and cannot yet be generalized. The overall quality of evidence is low to very low, with only two moderate-quality randomized trials. Robust, adequately powered randomized controlled trials with standardized outcome measures and long-term follow-up are urgently needed before definitive recommendations can be made regarding the use of CBPs in pediatric NDDs.
Authors’ Contributions
Research idea and study design: S.B. and L.N.; Data acquisition: S.B. and L.B.; Data analyses/interpretation: S.B., L.B., and G.P.; Article drafting and revising: S.B., T.A.B., P.S., and L.N. All authors contributed to the article and approved the submitted version.
Footnotes
Author Disclosure Statement
The authors have stated that they had no interests that might be perceived as posing a conflict or bias.
Funding Information
No funding was received for this article.