
Abstract
Objective:
Early behavioral dysregulation places children at elevated risk for later psychopathology. Maternal emotion dysregulation during pregnancy is a transdiagnostic vulnerability that may shape child regulatory development through both prenatal biological influences and postnatal caregiving. However, less is known about the specific postnatal mechanisms through which prenatal emotion dysregulation confers risk for toddler behavioral dysregulation. This study examined whether prenatal maternal emotion dysregulation was associated with toddler behavioral dysregulation indirectly through infant parasympathetic regulation (baseline respiratory sinus arrhythmia; RSA) and postnatal parenting stress.
Methods:
Participants were 385 mothers and their infants recruited during the third trimester. At the third trimester, maternal emotion dysregulation was assessed using the Difficulties in Emotion Regulation Scale. At 7 months postpartum, parenting stress was measured using the Parenting Stress Index, and infant parasympathetic regulation was assessed using baseline RSA during a neutral resting period. At 18 months, toddler behavioral dysregulation was evaluated using the Infant–Toddler Social Emotional Assessment. We tested direct and indirect pathways among prenatal maternal emotion dysregulation, postnatal parenting stress, infant baseline RSA, and toddler behavioral dysregulation with structural equation models.
Results:
Higher prenatal maternal emotion dysregulation was associated with greater postnatal parenting stress and lower infant baseline RSA. Postnatal parenting stress was concurrently associated with higher infant baseline RSA and higher toddler behavioral dysregulation. Infant RSA was not directly associated with toddler behavioral dysregulation. Parenting stress partially accounted for associations between prenatal maternal emotion dysregulation and toddler behavioral outcomes.
Conclusion:
This study provides evidence for prospective indirect pathways in which maternal emotion dysregulation during pregnancy contributes to elevated parenting stress in infancy, which is linked to both infant parasympathetic regulation and toddler behavioral dysregulation. Although prenatal maternal emotion dysregulation was associated with infant baseline RSA, infant RSA was not associated with toddler dysregulation, suggesting partly distinct pathways of physiological and behavioral regulation development. These findings highlight pregnancy and infancy as important periods in early child development.
Introduction
Early behavioral dysregulation in infancy and toddlerhood is associated with an increased risk of developing internalizing and externalizing problems later in development (Hyde et al., 2012; Winsper and Wolke, 2014). Behavioral dysregulation encompasses various dimensions, such as heightened negative emotionality, feeding difficulties, and sleep disturbances. These factors are not only markers of immediate distress but also predictors of stable, trait-like dysregulation that can persist across childhood (Winsper and Wolke, 2014). Understanding antecedents and developmental pathways to early behavioral dysregulation is important for determining potential intervention targets for later dysregulation and psychopathology.
During early development, maternal psychopathology and parenting-related stress are salient risk factors for the development of toddler psychopathology risk (Glover et al., 2018). Specifically, maternal mental health symptoms during pregnancy have important implications for the development of child regulatory systems. Prenatal maternal emotion dysregulation is a core transdiagnostic vulnerability that has been associated with infant and toddler outcomes related to psychopathology risk (Ostlund et al., 2019). However, less work has examined developmental influences from prenatal emotion dysregulation to toddler behavioral dysregulation via different indirect pathways. Drawing from developmental psychopathology frameworks, risk factors may influence the emergence of psychopathology through cumulative or progressive effects across levels, domains, and systems (Masten and Cicchetti, 2010). Relatedly, models of intergenerational risk for psychopathology (Goodman and Gotlib, 1999) posit multiple mechanisms that link maternal and child psychopathology symptoms, including prenatal programming of biological systems underlying regulation, as well as environmental transmission through the postnatal parenting stress context and related caregiving demands. Integrative models of intergenerational self-regulation further suggest that children’s emerging regulation is shaped by the combined influences of prenatal programming, genetic liability, and postnatal caregiving (Bridgett et al., 2015; Morris et al., 2007). However, few studies have empirically tested these proposed mechanisms by examining both postnatal parenting stress and infant physiological regulation as pathways linking prenatal maternal emotion dysregulation with toddler behavioral dysregulation.
Prenatal maternal emotion dysregulation
Emotion dysregulation is conceptualized as emotional experiences and expressions that are labile, intense, rigid, and prolonged, and that may interfere with goal-directed behavior and increase suffering (Crowell et al., 2020). During the perinatal period, maternal emotion dysregulation has been associated concurrently with elevated psychopathology and self-injurious thoughts and behaviors and prospectively with poorer sleep and a diminished desire to live (Kaliush et al., 2024; Lin et al., 2019; Molina et al., 2025). Additionally, maternal emotion dysregulation has been associated with lower concurrent observed parental sensitivity 6 months postpartum (Leerkes et al., 2020). Together, this literature suggests that maternal emotion dysregulation may have important implications not only for maternal functioning but also for parents’ experiences of parenting demands, which may in turn be associated with children’s emerging regulatory capacities.
While previous studies have focused on the effects of prenatal maternal diagnostic symptoms on child outcomes (Madigan et al., 2018; O’Donnell et al., 2014; Rees et al., 2019), a transdiagnostic marker of maternal psychopathology, such as emotion dysregulation, may provide a more robust understanding of the antecedents of child transdiagnostic risk (Brown et al., 2023). Emerging evidence indicates that maternal emotion dysregulation during pregnancy is associated with newborn neurobehavioral profiles characterized by lower arousal and attention, suggesting that downstream effects may be evident at birth (Ostlund et al., 2019). More recent work further suggests that perinatal emotion dysregulation prospectively predicts infant negative emotionality and toddler socioemotional difficulties, with evidence for indirect pathways through infant temperament and direct effects on later behavioral dysregulation (Zhou et al., in press; Laifer et al., 2025). In addition, developmental research outside the perinatal period suggests that parental emotion regulation difficulties are associated with children’s emotion regulation and internalizing risk, with some evidence of bidirectional, transactional influences between parent and child emotion regulation over time (Bariola et al., 2012; Han and Shaffer, 2013; Morris et al., 2011). Relatedly, maternal emotion dysregulation has been shown to associate with emotion socialization practices, which in turn may influence child affect and psychopathology risk (Price and Kiel, 2022; Binion and Zalewski, 2018). These findings align with broader developmental models of intergenerational transmission, which emphasize that prenatal programming and postnatal parenting jointly contribute to children’s emerging self-regulation capacities (Bridgett et al., 2015). Together, this literature supports perinatal emotion dysregulation as an early vulnerability that may confer downstream risk through both infant-level regulatory pathways and postnatal contextual mechanisms.
Postnatal parenting stress
Postnatal parenting stress is a possible proximal developmental context by which maternal emotion dysregulation can contribute to later child regulation (Goodman et al., 2020). Defined as the distress that arises when parenting demands exceed a parent’s perceived resources, parenting stress is a well-established risk factor for both parental mental health and child outcomes (Abidin, 1992; Fang et al., 2024). Recent longitudinal research demonstrates that elevated parenting stress predicts later child internalizing and externalizing difficulties, with evidence for both parent-driven and transactional associations across early childhood (Kochanova et al., 2022; Pan et al., 2025). Conceptually, parenting stress reflects parents’ appraisals of their caregiving capacity (Abidin, 1992). Widely used measures such as the Parenting Stress Index (PSI) operationalize this construct through domains of perceived parenting competence, role restriction, and attachment-related strain (Anhalt et al., 2007; NICHD Early Child Care Research Network, 2005).
Higher parenting stress, particularly when parents experience caregiving as overwhelming, ineffective, or constraining, has been associated with disruptions in sensitive parenting and reduced emotional availability, processes central to early regulatory development (Crnic and Greenberg, 1990; Jones and Prinz, 2005; Morris et al., 2007; Planalp et al., 2022). In the postnatal period, high parenting stress is also linked to increased symptoms of depression and anxiety and greater difficulty interpreting and responding to infant cues (Crnic and Greenberg, 1990; Khalsa et al., 2022; Leerkes, 2010; Leigh and Milgrom, 2008; Morris et al., 2007). Parental emotion regulation capacities may shape how these later caregiving demands are experienced and managed (Dix, 1991; Morris et al., 2007). Empirical work demonstrates that maternal emotion dysregulation is associated with higher parenting stress and that parenting stress can mediate associations between maternal emotion dysregulation and child physiological outcomes (Cao et al., 2017). Additionally, studies have shown that parenting stress can mediate associations between parental negative affect and later harsh parenting (Le et al., 2017). Building upon this literature, there is a body of work that demonstrates that these early caregiving experiences can shape child stress regulation (Hane and Fox, 2016; Luecken and Lemery, 2004). However, less work has examined whether postnatal parenting stress, as operationalized through processes such as attachment, competence, and role restriction, may represent a possible pathway through which prenatal emotion dysregulation is associated with both child physiological and behavioral dysregulation.
Parasympathetic nervous system activity and behavioral dysregulation
Measures of parasympathetic nervous system (PNS) activity during infancy have been associated with dimensions of behavioral dysregulation as well as later psychopathology symptoms (Graziano and Derefinko, 2013; Zhou et al., 2023). Therefore, it may be possible that individual differences in PNS functioning underlie behavioral dysregulation. The PNS responds very quickly to environmental cues as a first-response coping system, allowing individuals to mobilize resources to achieve homeostasis (Porges, 2007). One measure of PNS activity is respiratory sinus arrhythmia (RSA), an index of an individual’s capacity to self-regulation when engaging with environmental demands (Beauchaine, 2001). At the biological level, RSA indexes parasympathetic (vagal) control of arousal and is theorized to support restoration, recovery, and flexible physiological engagement with environmental demands. Chronic stress exposure may therefore disrupt the development of RSA and stress responsivity (Beauchaine, 2001; Thayer and Lane, 2009; Porges, 2007). Under optimal stimulus conditions, baseline RSA can provide insight into parasympathetic functioning and regulatory capacity. Generally, higher levels of baseline RSA have been associated with better emotion regulation, as well as fewer internalizing and externalizing symptoms during childhood (Graziano and Derefinko, 2013). Additionally, emerging evidence shows that infant baseline RSA may be associated with toddler dysregulation, although this association may be moderated by maternal sensitivity (Brown et al., 2023).
However, less work has examined whether the development of infant RSA is a potential pathway through which parental risk factors may be associated with toddler dysregulation and increased psychopathology risk. Emerging work shows that prenatal maternal factors can shape the development of infant RSA (Gao et al., 2022; Propper and Holochwost, 2013), thereby suggesting that disruptions in parental emotional or physiological functioning may be transmitted to the infant via early autonomic regulation. Such alterations in parasympathetic functioning may compromise the infant’s ability to regulate stress and emotion, thereby increasing vulnerability to later behavioral dysregulation and psychopathology.
Present study
Although both conceptual and empirical work suggests multiple mechanisms that may link prenatal maternal emotion dysregulation to toddler behavioral dysregulation, few studies have explicitly tested indirect pathways such as parenting stress and infant autonomic regulation. Drawing on models of the intergenerational transmission of psychopathology (Goodman and Gotlib, 1999) and self-regulation (Bridgett et al., 2015), there are multiple mechanisms by which maternal emotion dysregulation may be associated with child behavior dysregulation and psychopathology risk. Thus, the present study tested if prenatal maternal emotion dysregulation may be associated with 18-month behavioral dysregulation via 7-month postnatal parenting stress and 7-month infant autonomic regulation. Infant age at 7 months was selected because this period reflects a sensitive window for emerging self-regulation, making it optimal for assessing an early physiological pathway to toddler behavioral dysregulation. First, we hypothesized that we would find direct effects of prenatal maternal emotion dysregulation on infant baseline RSA and toddler dysregulation. Specifically, we expected that higher levels of prenatal maternal emotion dysregulation would be associated with lower levels of infant resting RSA and higher levels of toddler behavioral dysregulation. Second, we hypothesized a positive association between prenatal maternal emotion dysregulation and postnatal parenting stress, consistent with findings from prior studies. We also predicted that higher levels of postnatal parenting stress would be associated with higher toddler behavioral dysregulation levels. Thus, we hypothesized indirect pathways from prenatal maternal emotion dysregulation to child behavior regulation outcomes via parenting stress. Lastly, we hypothesized that lower baseline RSA would serve as an early risk marker for higher levels of dysregulation during toddlerhood and that infant baseline RSA may be a pathway by which prenatal maternal emotion dysregulation and parenting stress are associated with toddler dysregulation.
Materials and Method
Participants
This longitudinal study involved 385 mothers and their infants, 52% of whom were assigned female at birth. The participants were engaged in a research project aimed at exploring the intergenerational transmission of emotion dysregulation (Gao et al., 2021; Lin et al., 2019). We conducted recruitment in two phases: the first cohort was enrolled from 2016 to 2019, and the second from 2019 to 2024, reflecting separate funding mechanisms. The average age of expectant mothers was 29.40 years (standard deviation [SD] = 4.9), ranging from 18 to 40 years. Recruitment occurred during the third trimester through OB/GYN clinics, media advertisements, and referrals.
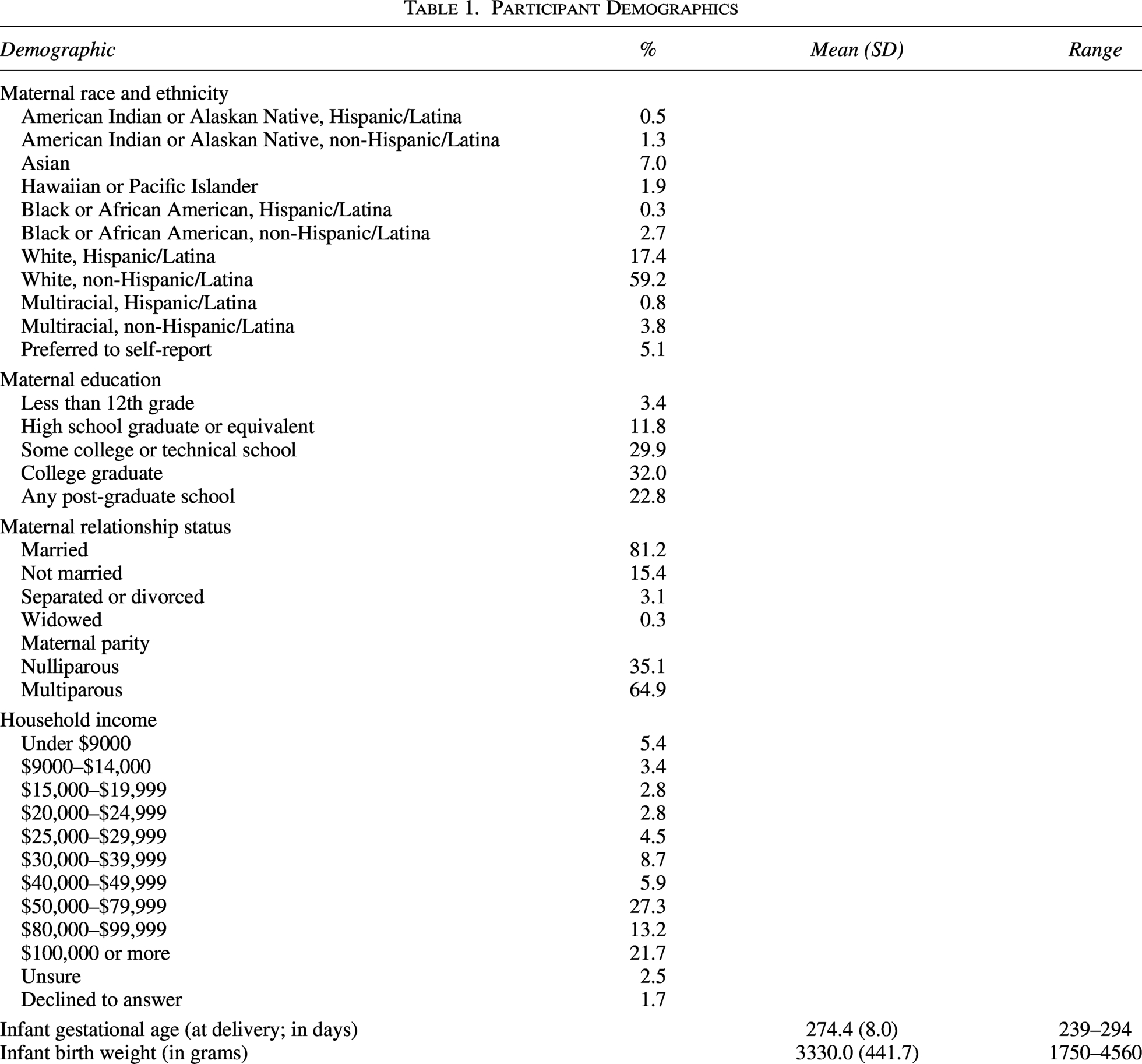
Participants were recruited based on their scores on the Difficulties in Emotion Regulation Scale (DERS; Gratz and Roemer, 2004), with a focus on including both high and low scorers to ensure a representative distribution of emotion dysregulation. We screened a total of 1860 pregnant individuals across both cohorts; we excluded 890 women based on low or moderate DERS scores as part of the stratification process. We also excluded expectant mothers carrying multiples, those who reported substance use during pregnancy, or those diagnosed with gestational diabetes or pre-eclampsia to minimize health-related variability in our analysis. In the current study, data collection occurred at the third trimester, and again at 7 and 18 months postpartum. Participation rates declined over time, partly due to pandemic-related disruptions, with 84% at 7 months and 74% at 18 months. Participant demographic details are presented in Table 1. Participants were compensated $25 for completing questionnaires at each time point and $50 for completing the laboratory visit at 7 months postpartum.
Participant Demographics
Procedures
Pregnant individuals who were interested in participating completed a two-step screening process, which involved completing the DERS and additional questions pertaining to eligibility criteria. After enrollment and upon providing written informed consent, expectant mothers completed questionnaires using an online link during their third trimester of pregnancy. At the 7-month laboratory visit, infant electrocardiogram data were collected when infants were in a neutral state (i.e., the resting phase). Infants were seated either in a high chair or on their mother’s lap while watching a Baby Einstein video clip (2 minutes) and were not allowed to interact with toys (Conradt and Ablow, 2010). Mothers were asked to limit interactions with their child during this time. Prior to attending the 7- and 18-month visits, mothers completed a series of online questionnaires about themselves and their children. Of interest to the current study, mothers self-reported their parenting stress level at 7 months (PSI) and their toddlers’ socioemotional development at 18 months (The Infant and Toddler Socioemotional Assessment). All study procedures were approved by the institutional review board at the University of Utah.
Measures
Maternal emotion dysregulation
The Difficulties in Emotion Regulation Scale (DERS; Gratz and Roemer, 2004), a self-report measure of emotion dysregulation, was administered during the third trimester. The DERS consists of 36 questions that are scored on a 5-point Likert scale, ranging from 1 (Almost Never) to 5 (Almost Always). A total score is computed, as well as scores for six subscales (nonacceptance of emotional responses, difficulty engaging in goal-directed behavior, impulse control difficulties, lack of emotional awareness, limited access to emotion regulation strategies, and lack of emotional clarity). There was good internal consistency for this measure in our study (α = 0.96). Higher scores (e.g., 90+) in adult samples are often seen in clinical populations and are associated with significant regulatory impairment.
Parenting stress
Parents reported their parenting stress at 7 months postpartum using a 25-item survey adapted from the PSI, consisting of items from the subscales of Attachment, Competence, and Role Restriction from the parent domain that were previously validated (Abidin, 1992; Anhalt et al., 2007; NICHD Early Child Care Research Network, 2005). The survey assessed various aspects of parenting stress using a 5-point Likert scale ranging from 1 (Almost Never/Strongly Disagree) to 5 (Almost Always/Strongly Agree). Higher scores indicate greater parenting stress. As this measure was adapted rather than administered in its full standardized form, established PSI clinical cutoffs are not directly applicable; thus, parenting stress was treated as a continuous variable. Previous research showed associations between the adapted scale and maternal sensitivity, children’s behavioral problems, and children’s language skills (Mulsow et al., 2002; Oxford and Lee, 2011). In our data, there was good internal consistency for this measure (α = 0.84). Although clinical cutoffs are not available for this measure, mean levels in the current sample appear higher than those reported in earlier cohorts using similar measures (Anhalt et al., 2007). However, such comparisons should be interpreted cautiously given differences in postpartum timing, sample composition, and historical context.
Infant RSA
Electrocardiogram data were collected from infants at the 7-month time point for 2 minutes at 500 Hz with pediatric spot electrodes placed immediately below the child’s right clavicle and on the lower left and right rib cage. MindWare Technologies’ BioLab and HRV Editor softwares (both 3.1) were used to acquire and process the signal, respectively (MindWare Technologies, Ltd., Gahanna, OH). The editing software automatically identifies R peaks within the heart rate signal and flagged interbeat intervals (IBIs) outside the expected range for review. Data were examined for aberrant IBIs by trained research assistants and analyzed in contiguous 30-second segments. Ambiguous waveforms were reviewed by a senior researcher and excluded from analyses when necessary. RSA values were defined as the high-frequency band of the power spectrum (0.24–1.04 Hz) following application of the Fast Fourier Transform algorithm. A mean baseline score was calculated as the average of up to four available RSA data segments from the 2-minute baseline. Of the participants with data, 95.6% had all four segments available, and none had fewer than two segments available. Due to the COVID-19 pandemic, data collection occurred during at-home visits for 48% of participants (Gao et al., 2021). An analysis of variance showed that there were significantly more epochs of RSA data missing from at-home collection than in-lab, F(1, 272) = 50.79, p < 0.001, suggesting that data collected in the home setting may have been more susceptible to noise. Although at-home recordings contained a greater number of missing epochs, all data were subjected to rigorous and standardized cleaning procedures. Artifact rejection criteria were consistent across settings, and only epochs meeting established quality thresholds were retained for analysis.
Toddler behavior dysregulation
The Infant and Toddler Socioemotional Assessment (ITSEA; Carter et al., 2003) is a 166-item questionnaire designed to assess social and emotional problems and competencies in children aged 12–35-months-old. Parents completed this questionnaire at the 18-month timepoint. Each item assesses different behaviors on a 3-point scale ranging from 0 (Not True) to 2 (Very True/Often). The ITSEA contains 17 subscales that capture four broad domains: internalizing behaviors (α = 0.78), externalizing behaviors (α = 0.83), dysregulation (α = 0.83), and competence (α = 0.87). The dysregulation domain includes negative emotionality, sleep, eating, and sensory sensitivity. We computed T scores that are standardized based on child age and sex, with higher scores indicating more behavioral dysregulation problems. T scores ≥ 63 are considered as clinically significant, and around 7% of children in our sample met this threshold.
Data analytic plan
Missing data
Due to participant attrition and challenges around retention during the COVID-19 pandemic, we had some missing data at all follow-up time points. Full-information maximum likelihood can produce less biased estimates when accounting for missing data when appropriate auxiliary variables are selected and included (Graham, 2003). First, we examined missing data using the naniar package in R 4.4.1. Data were completely missing at random, χ² = 158.71, p = 0.623. We then conducted logistic regression analyses to examine if demographic variables (maternal age, maternal education, gestational age of infant at birth, and infant sex) were associated with missingness and to identify appropriate auxiliary variables to include in our models. Analyses showed that lower maternal education was associated with missingness in parenting stress scores. Additionally, we accounted for data collection method for RSA (i.e., in-lab or remote data collection) in our analyses as parenting stress scores, F(1, 265) = 5.59, p = 0.019, and infant baseline RSA (F(1, 227) = 8.22, p = 0.005) were significantly higher for remote data collection.
Path modeling
Path modeling was conducted using the lavaan package (Rosseel, 2012) in R 4.4.1. We tested direct associations between prenatal maternal emotion dysregulation, 7-month parenting stress, 7-month infant baseline RSA, and 18-month toddler dysregulation T scores. We examined correlations between sociodemographic variables and key study variables to identify potential covariates. Household income was significantly associated with prenatal maternal emotion dysregulation scores (r = −0.22, p < 0.001); therefore, we included it in all models as a covariate. All regression coefficients reported are standardized. Our estimates and standard errors were computed using bias-corrected bootstrapping with 1000 draws. Model fit was evaluated using χ2, the comparative fit index (CFI), the Tucker–Lewis index (TLI), standardized root mean square residual (SRMR), and root mean square error of approximation (RMSEA). Good model fit was indicated by p > 0.05, CFI ≥ 0.95, TLI ≥ 0.95, SRMR ≤ 0.08, RMSEA ≤ 0.06 (Hu and Bentler, 1999). We evaluated three indirect pathways: (1) prenatal maternal emotion dysregulation to infant RSA via postnatal parenting stress, (2) prenatal maternal emotion dysregulation to toddler behavioral dysregulation via postnatal parenting stress, and (3) prenatal maternal emotion dysregulation to toddler behavioral dysregulation via postnatal parenting stress and infant RSA. Indirect effects were evaluated using bootstrapped estimates with bias-corrected 95% confidence intervals; indirect effects were considered statistically significant when the confidence interval did not include zero.
Results
Table 2 contains the means, standard deviations, and correlations between the main variables of interest. Of note, prenatal maternal emotion dysregulation was positively associated with 7-month parenting stress (r = 0.35) and 18-month toddler dysregulation (r = 0.17), but not with 7-month infant baseline RSA. Additionally, parenting stress was positively associated with toddler dysregulation (r = 0.31).
Means, Standard Deviations, Sample Sizes, And Correlations With Confidence Intervals
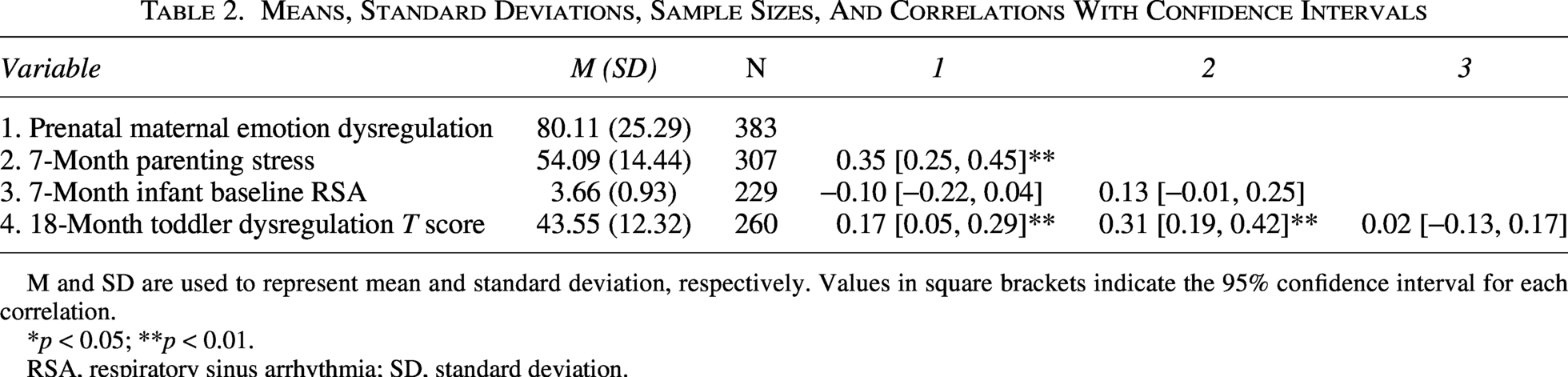
M and SD are used to represent mean and standard deviation, respectively. Values in square brackets indicate the 95% confidence interval for each correlation.
*p < 0.05; **p < 0.01.
RSA, respiratory sinus arrhythmia; SD, standard deviation.
To test our hypotheses, we examined a path model with prenatal maternal emotion dysregulation, 7-month parenting stress, 7-month infant baseline RSA, and 18-month toddler dysregulation T scores. There was an acceptable fit (χ2 = 104.01, p < 0.001, CFI = 1.00, TLI = 1.00, SRMR = < 0.001, RMSEA < 0.001). Figure 1 depicts the path model. First, higher prenatal maternal emotion dysregulation was significantly associated with higher levels of postnatal parenting stress at 7 months (b = 0.37, p < 0.001, 95% CI [0.25, 0.48]). Higher levels of prenatal maternal emotion dysregulation were also associated with lower levels of infant baseline RSA (b = −0.19, p = 0.012, 95% CI [−0.34, −0.03]). Higher parenting stress at 7 months was associated with higher infant baseline RSA (b = 0.16, p = 0.026, 95% CI [0.02, 0.30]). Higher parenting stress was also associated with higher toddler dysregulation (b = 0.31, p < 0.001, 95% CI [0.17, 0.45]). Neither prenatal maternal emotion dysregulation (b = 0.02, p = 0.756, 95% CI [−0.12, 0.17]) nor infant baseline RSA (b = −0.01, p = 0.845, 95% CI [−0.15, 0.12]) was associated with toddler dysregulation.
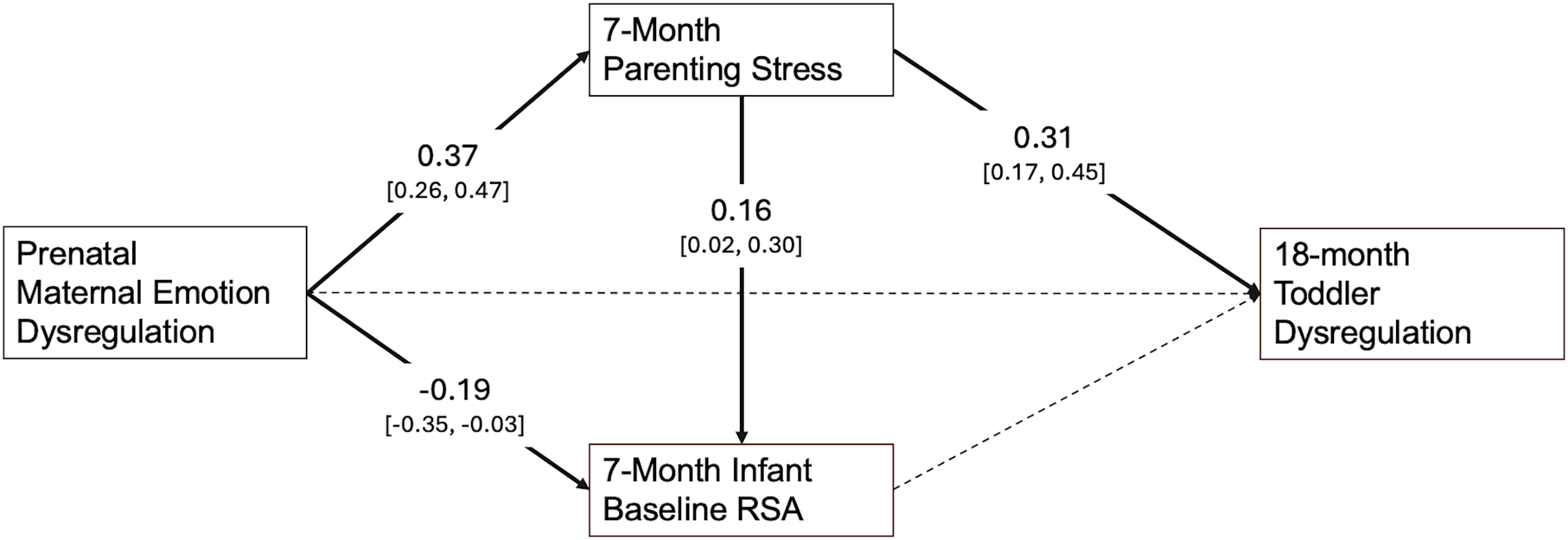
Path model examining associations among prenatal maternal emotion dysregulation, 7-month parenting stress, 7-month infant baseline RSA, and 18-month toddler dysregulation (T scores). All estimates are standardized, with 95% confidence intervals. Solid lines are significant (p < 0.050), while dashed lines are not significant (p ≥ 0.050). RSA, respiratory sinus arrhythmia.
There were also significant indirect paths from prenatal maternal emotion dysregulation to child outcomes via postnatal parenting stress. Prenatal maternal emotion dysregulation was significantly associated with infant baseline RSA via parenting stress (b = 0.06, p = 0.030, 95% CI [0.01, 0.11]). Similarly, prenatal maternal emotion dysregulation was significantly associated with toddler dysregulation via parenting stress (b = 0.11, p = 0.001, 95% CI [0.05, 0.18]). In other words, higher prenatal maternal emotion dysregulation was associated with higher parenting stress, which, in turn was related to child outcomes at 7 and 18 months postpartum.
We further conducted post hoc analyses to test if associations remain after accounting for postnatal maternal emotion dysregulation (assessed at 7 months postpartum), as well as potential moderating associations among the key variables of interest. An extended model with postnatal emotion dysregulation at 7 months (Fig. 2) showed significant continuity in maternal emotion dysregulation from third trimester to 7 months postpartum (b = 0.73, p < 0.001, 95% CI [0.66, 0.79]). We found that the association between prenatal maternal emotion dysregulation and infant RSA was no longer significant after the inclusion of postnatal maternal emotion dysregulation. However, associations with parenting stress remained even after accounting for postnatal maternal emotion dysregulation. Additional models with interaction terms showed no significant associations with child outcomes (see Supplementary Material).
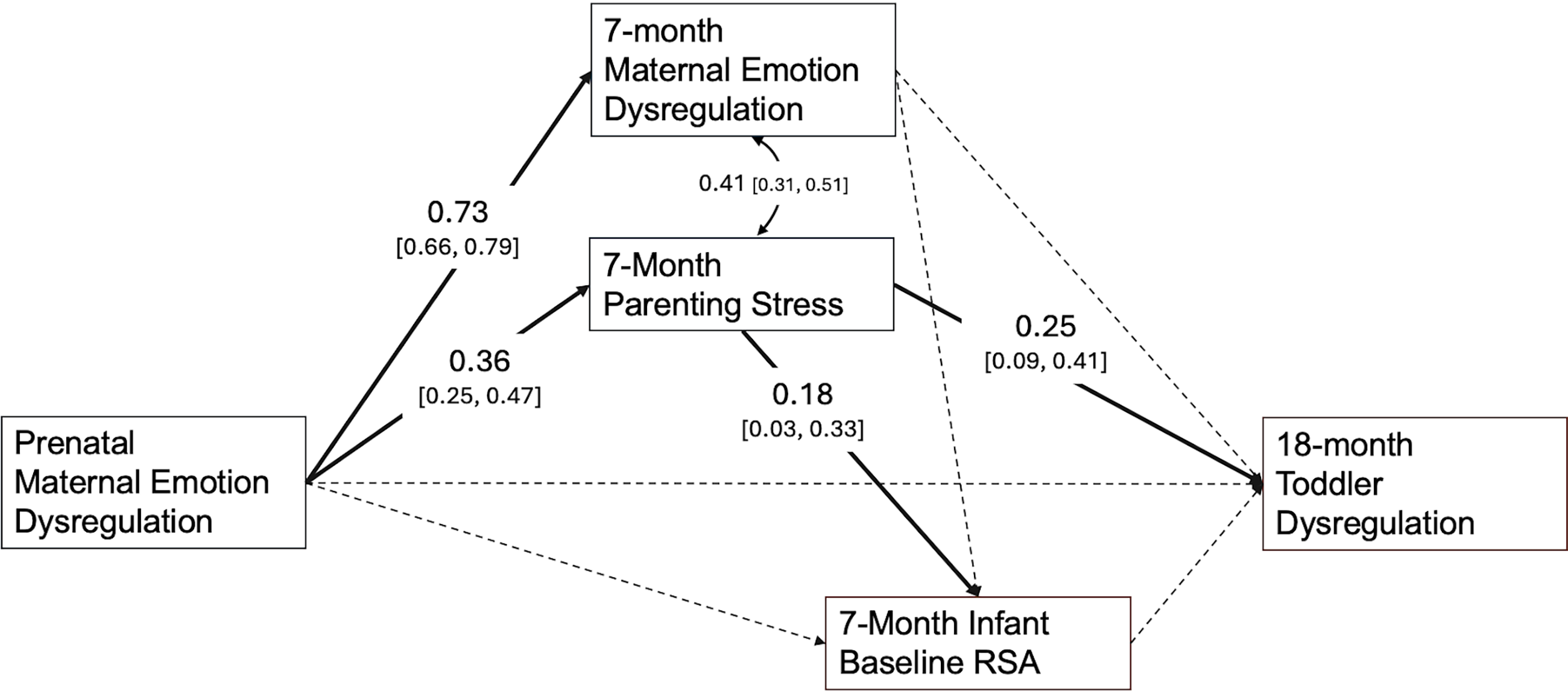
Path model examining associations between prenatal maternal emotion dysregulation, 7-month maternal emotion dysregulation, 7-month parenting stress, 7-month infant baseline RSA, and 18-month toddler dysregulation (T scores). All estimates are standardized, with 95% confidence intervals. Solid lines are significant (p < 0.050), where dashed lines are not significant (p ≥ 0.050). RSA, respiratory sinus arrhythmia.
Additionally, given that parenting stress and infant RSA are assessed at the same time point, we also constructed an additional model where parenting stress and infant RSA are concurrently associated (see Supplementary Material). We find the same indirect path from prenatal maternal emotion dysregulation to toddler behavioral dysregulation via 7-month parenting stress.
Discussion
The present study examined whether prenatal maternal emotion dysregulation was associated with behavioral dysregulation in toddlerhood through postnatal maternal parenting stress and infant autonomic functioning, or RSA. The results provide evidence of cross-domain associations across early development, such that higher maternal emotion dysregulation at third trimester was associated with more parenting stress at 7 months postpartum, which, in turn, was associated with differences in infant baseline RSA and toddler behavioral dysregulation. The indirect pathways were consistent with the possibility that prenatal maternal emotion dysregulation is associated with child regulatory outcomes through higher levels of postnatal parenting stress. Together, these findings suggest that regulatory challenges during pregnancy may be associated with higher levels of parenting stress associated with children’s emerging physiological and behavioral regulation during a sensitive developmental window.
In our full model, we found that prenatal maternal emotion dysregulation was not significantly associated with toddler behavioral dysregulation. Although this null direct effect may be surprising, it is also important to note that there was a significant positive bivariate correlation between prenatal maternal emotion dysregulation and toddler behavioral dysregulation when postnatal parenting stress and infant RSA were not included. This finding suggests that the association between prenatal maternal emotion dysregulation and toddler behavioral dysregulation may be accounted for by shared variance with postnatal parenting stress and infant RSA, consistent with the possibility that these postnatal factors were associated with the attenuation of the observed bivariate relationship.
We found that prenatal maternal emotion dysregulation and toddler behavioral dysregulation was associated via postnatal parenting stress. This pattern suggests that difficulties in maternal emotion regulation during pregnancy may carry forward into the postnatal period in ways that heighten parenting-related stress, which, in turn, contributes to greater dysregulation in toddlers. Notably, this indirect pathway remained even after accounting for postnatal maternal emotion dysregulation, suggesting that associations between prenatal maternal emotion dysregulation and toddler behavioral outcomes operate, in part, through stress associated with early caregiving, above and beyond mothers’ concurrent emotion regulation difficulties. This finding highlights the potential impact of prenatal emotional processes on the postnatal caregiving environment and indicates that postnatal parenting stress may be a key mechanism linking early maternal vulnerabilities to child behavioral dysregulation.
Our findings are also consistent with theoretical models and empirical work suggesting that early exposure to stress is associated with emerging regulatory vulnerabilities during infancy and toddlerhood (Nicolaides et al., 2024; Propper and Holochwost, 2013). Notably, we found a direct association between higher prenatal maternal emotion dysregulation and lower infant baseline RSA, aligning with prior research indicating that prenatal stress exposure can shape infant parasympathetic functioning (Propper and Holochwost, 2013). However, this association was no longer significant after accounting for postnatal maternal emotion dysregulation; therefore, this finding should be interpreted with caution.
Although higher prenatal maternal emotion dysregulation was associated with lower infant baseline RSA, the positive association between postnatal parenting stress and infant baseline RSA was unexpected, although it was consistent across models. There was also an unexpected positive indirect effect from prenatal maternal emotion dysregulation to infant baseline RSA via postnatal parenting stress. One possibility is that the indirect effect reflects how shared variance among predictors is accounted for in the model rather than a developmental mediation process. In the context of our model, this pattern is consistent with a suppression effect (Mackinnon et al., 2000), wherein the inclusion of postnatal parenting stress in our model increased the magnitude of the negative association between prenatal maternal emotion dysregulation and infant baseline RSA. In a model without parenting stress, there was no significant association between prenatal maternal emotion dysregulation and infant baseline RSA (b = 0.11, p = 0.169). In contrast, this was a significant negative association when postnatal parenting stress was included in the model (Fig. 1). Conceptually, this suggests that parenting stress may capture variance in infant parasympathetic functioning that is distinct from prenatal maternal emotion dysregulation. Within the context of our mediation model, this pattern represents a residual association between parenting stress and infant RSA after accounting for prenatal maternal emotion dysregulation. That is, among mothers with comparable levels of prenatal dysregulation, those experiencing more parenting stress had infants with higher baseline RSA.
Although this finding was unexpected within our model, it aligns with prior studies that have found positive associations between postnatal maternal internalizing symptoms and infant baseline RSA (Zhou et al., 2023). Thus, several speculative developmental explanations could also be considered. One possibility is that infants exposed to parents experiencing high levels of stress engage more in self-regulatory processes, thus developing higher levels of baseline RSA to meet contextual stressors and demands. In this context, higher RSA may reflect a compensatory regulatory response to caregiving stress rather than a uniformly adaptive physiological profile. Another possibility is that reports of higher parenting stress, for some families, may reflect greater parental investment or monitoring, which may also support the development of stronger parasympathetic regulation. Mothers who are more attuned to the stress in their life may also be more attuned to their infants’ distress, which may lead to higher engagement in behaviors that promote their infants’ physiological regulatory capacities. These potential mechanisms underlying the positive association between parenting stress and infant RSA will require future empirical testing.
Additionally, infant baseline RSA was not directly associated with toddler behavioral dysregulation, suggesting that physiological and behavioral regulatory systems may follow partially independent developmental trajectories. Behavioral dysregulation is a complex, multi-determined phenotype that likely emerges from the interplay of biological, environmental, and psychosocial factors. For example, studies have shown that child baseline RSA may moderate associations between environmental risk factors and child socioemotional outcomes (Blandon et al., 2008). Thus, the effects of parasympathetic functioning on later toddler behavioral dysregulation may be context dependent. For example, in a partially overlapping sample, lower infant baseline RSA was associated with greater toddler dysregulation for infants who experienced lower levels of maternal sensitivity (Brown et al., 2025). This pattern suggests that associations between early parasympathetic functioning and later behavioral regulation may depend on caregiving processes. Although our post hoc analyses did not show evidence for moderation between parenting stress and baseline infant RSA on later toddler dysregulation, future studies could test statistical interactions between baseline RSA and other dimensions of parenting processes to inform our understanding of intergenerational mechanisms. Additionally, studies have shown that there is variability in developmental trajectories of parasympathetic functioning during infancy, and that contextual factors may shape developmental change in parasympathetic regulation (Lytle et al., 2025; Wagner et al., 2021). Therefore, the lack of predictive validity of baseline RSA at 7 months on toddler behavioral dysregulation may reflect the timing of assessment, as the developing PNS may be sensitive and shaped by exposure to contextual factors. Future research could test if trajectories of baseline RSA across early development may be a better indicator of later behavioral dysregulation.
Limitations and future directions
This study has several strengths, including a longitudinal design, a multi-level assessment of both physiological (infant RSA) and behavioral (toddler dysregulation) outcomes, and the examination of prenatal and postnatal pathways within a single model. Several limitations should also be noted. First, prenatal maternal emotion dysregulation, postnatal parenting stress, and toddler dysregulation were all measured using maternal self-report, raising the possibility of shared method variance, which could inflate associations among these constructs. Although studies show lack of reporter bias of child behaviors by maternal psychopathology (Olino et al., 2020), integrating multi-method assessments of behavioral dysregulation that do not rely on maternal report, such as observed ratings of child emotionality or sleep actigraphy could strengthen this line of work. We also only had a single assessment of maternal emotion dysregulation during pregnancy. Prior studies have shown that maternal emotion dysregulation is, on average, elevated during the third trimester compared to the postnatal period (Zhou et al., 2025). However, fewer studies have investigated maternal emotion dysregulation prior to the third trimester. Some emerging evidence suggests that prenatal maternal distress at different gestational timing may have differential effects on fetal and infant outcomes (Liou et al., 2016). Future work should examine if timing of elevated maternal emotion dysregulation plays a differential role on offspring autonomic development. In addition, genetic transmission represents a plausible mechanism linking maternal and child emotion dysregulation that cannot be disentangled in the current study. We also assessed parenting stress and infant physiological regulation concurrently. While the test of this pathway was informed by conceptual models of intergenerational transmission of psychopathology and self-regulation (Bridgett et al., 2015), it is plausible that there may be child-directed associations on parenting stress. Longitudinal research with repeated measures may elucidate and clarify the directionality of these associations. We also acknowledge that there were some differences in the amount of usable RSA data based on data collection method; however, at-home data collection was necessary in order to retain families at precise developmental intervals even amid the COVID-19 pandemic. Additionally, another methodological consideration is that there was significantly higher infant baseline RSA for infants where data collection occurred in the home, which may be due to comfort and being in a familiar context. Researchers should consider the methodological impact of data collection method on physiological indices of regulation.
It will be critical to replicate the current study to ensure that the findings regarding infant RSA are reliable, generalizable, and informative for both developmental science and practical assessment protocols. For instance, study variables fell largely within the normative range, which may limit generalizability and attenuate effect sizes relative to more clinically elevated samples. Consistent with this, the observed effect sizes were modest but are in line with those commonly observed in psychological and developmental research and remain meaningful, particularly in longitudinal contexts in which small effects may accumulate over time (Funder and Ozer, 2019; Masten and Cicchetti, 2010). Repeated measures across the perinatal period and toddlerhood will be needed to more rigorously test developmental cascade processes as defined in the developmental psychopathology literature. Future research should examine moderators of these pathways, including infant temperament and health status, maternal trauma exposure, and contextual factors shaping parenting stress (e.g., socioeconomic resources, social support, and access to mental health care). Future work should also examine cultural contexts, because emotion regulation strategies vary across cultures (Chen et al., 2025), and cultural norms may shape caregiving expectations and access to community-based parenting support (Falzarano et al., 2022). Given the sample demographics in the present study, it will be important to consider contextual factors in order to understand generalizability of findings as well as identifying families who may be at heightened risk due to sociodemographic factors. Understanding these sociocultural contexts is an important next step for clarifying how regulatory processes unfold across generations.
Conclusions
In summary, this study highlights the potential cascading influence of maternal emotion dysregulation during pregnancy on early child regulatory outcomes. Prenatal maternal emotion dysregulation was associated with higher postnatal parenting stress, which, in turn, was associated with both infant physiological regulation and toddler behavioral dysregulation. Additionally, there was a direct pathway from prenatal maternal emotion dysregulation to infant physiological regulation, suggesting that these associations may be, in part, due to genetic and/or prenatal processes. These findings underscore the importance of considering both prenatal and postnatal pathways for understanding early developmental risk and resilience. Interventions that support maternal emotion regulation during pregnancy and reduce parenting stress postnatally may have meaningful benefits for children’s emerging self-regulation both on a physiological and behavioral level, emphasizing the value of early, preventive approaches to promote healthy developmental trajectories.
Clinical significance
Prenatal maternal emotion dysregulation was associated with higher parenting stress, which was linked to both infant autonomic regulation and toddler behavioral dysregulation. Our findings support the importance of early screening for maternal mental health during pregnancy, especially screening for emotion dysregulation, to identify families who may be at risk for postnatal parenting stress and toddler behavioral dysregulation. While we utilized a 36-item emotion dysregulation scale in the present study, a validated 18-item version (Kaufman et al., 2016) may be more feasible for implementation in medical settings.
Building on the emerging literature demonstrating the efficacy of perinatal interventions for maternal and child outcomes, future work should examine if supporting maternal emotion regulation and coping capacity during pregnancy and early infancy is associated with parenting stress and more adaptive regulatory development. Given that early childhood interventions are often parent focused, transdiagnostic supports that strengthen maternal coping and reduce parenting stress may represent a promising pathway for shaping toddlers’ regulatory profiles and reducing downstream behavioral risk.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.