
Abstract
Background.
Methods. This randomized control trial employed a 2 X 2 fully-crossed between subjects and tested the effects of
Results. A Factorial ANOVA with repeated measures and a between subjects’ factor (split plot) was used to test for the differences between the means of the outcome variables. Despite having no main or interaction effect our analysis did report a significant main effect of using a pre-post design with the experiment as a stimulus.
Discussion/Conclusion. For experimental data, customizing an
Introduction
Human Papillomavirus (HPV) is a group of 150 related viruses that can result in genital warts as well as cancers of the mouth/throat, cervix, vagina, vulvar, anus and penis ((Centers for Disease Control and Prevention, 2016)). While the body is able to fight most HPV infections resulting in no health problems or consequences, there are 9 that cause the majority of HPV related cancers and diseases. These include types 6, 11,6,18, 31, 33, 45, 52 and 58 (Merck, 2017). But despite public health efforts and the availability of a vaccine, HPV prevalence and incidence rates remain relatively high. HPV is the most common sexually transmitted disease (STD) in the United States (U.S.) with the highest infection rates observed among sexually active adults under the age of 25 with highest risk in adolescents (aged 15 – 19) and young adults (aged 20 to 24) (Gerend & Magliore, 2008; Patel et al., 2012). With over 20 million people currently infected with HPV, and 6.2 million new cases being diagnosed each year in the U.S., HPV- related cancers are now becoming a greater threat to younger generations of Americans (Katz, Krieger, & Roberto, 2011).
HPV-associated diseases in men are often asymptomatic (Gargano, Meites, Watson, Unger, & Markowitz, 2017). The lack of symptoms in men often causes them to seek care at a later stage of the disease process, thus increasing their risk for oropharyngeal, anal and penile cancers (Fontenot, Collins Fantasia, Charyk, & Sutherland, 2014). Despite this, HPV vaccine uptake is low. Men have less basic knowledge about health, are less likely to seek out health information, and are less likely to engage in preventative health-promoting behaviors compared to females (Davies et al., 2000). Low vaccine uptake among men has been related to low perceived threat due to the absence of HPV vaccination information from healthcare providers, parents, peers, public health officials, prevention campaigns and the media (Daley et al., 2011; Ratanasiripong, 2015). This is of great concern, since males are the highest carriers and transmitters of HPV virus yet are so instrumental to herd immunity (Hosseini, Munoz, Lakon, & Brown, 2014). Herd immunity occurs when a critical part of the community is immunized from a contagious disease because of their increased risk, allowing for most members of the community to be protected against that disease (National Institute of Allergy and Infectious Diseases, 2010). Because of the herd immunity effect, there are compelling arguments to make in favor of male vaccination against HPV, such as taking a gender neutral approach to vaccination which has not been traditionally adopted since recommendations were released by the Centers for Disease Control and Prevention (Zimet & Rosenthal, 2010).
Despite the obvious health benefits of male vaccination against HPV, there are no screening procedures nor vaccine prevention campaigns specifically for males (Crosignani et al., 2013). With several countries including the US exclusively focusing their efforts towards only educating the female population, HPV risk perception among males is low (No et al., 2011). According to National Health and Nutrition Examination Survey (NHANES) data, HPV infection prevalence was almost 50% for men 18 – 59 years old, equating to nearly 34.8 million men (Han, Beltran, Song, Klaric, & Choi, 2017). College males have a higher risk of contracting HPV, due to their riskier sexual behaviors such as having multiple sexual partners and having sex while intoxicated (Hittner, Owens, & Swickert, 2016). Furthermore, college males are reluctant to seek care from a healthcare provider due to social expectations to avoid extreme pain and pressures to conceal any vulnerabilities (Davies et al., 2000). Although the HPV vaccine is expected to reduce healthcare costs and decrease the fear associated with treatment of genital warts, there are key barriers that have affected vaccine uptake (M. Jones & Cook, 2008). These barriers include the stigmatizing nature of HPV, physical discomfort associated with vaccine uptake and the fear of vaccine side effects (Anic & Giuliano, 2011; Fontenot et al., 2014; G. Jones, Perez, Huta, Rosberger, & Lebel, 2016).
Serious Digital Games and Character Customization
Digital games may be an ideal platform to deliver HPV interventions to college males. About seven in ten men younger than 30 (72%) say they play video games often or sometimes, compared with 49% of women in the same age group (Pew Research Center, 2016). Games for health have emerged as a personalized, entertaining and informative means to health promotion. These games not only impact attitudes and beliefs, but have been shown to increase knowledge, skills and changes in behavior (Thompson, 2012). Therefore, video games can be marketable to a vast range of population subgroups including college students as they are a powerful channel to deliver health messages.
Customizing digital games provides increased opportunities for interventions to focus on the individual and ensures that messages (a combination of content, source, graphics, channel, etc.) the audience receives reflect relevant individual characteristics that matches the self (Kalyanaraman & Sundar, 2006). Based on self-concept theory “the self”” has been operationally defined as “a person’s representation or description of his or her personal and social characteristics” (Leary, Estrada, & Allen, 2009, p. 148). These characteristics can reflect people’s ideal, actual and feared selves and can even extend into the ecological, interpersonal, extended, private and conceptual selves (Benson, 2002; Leary et al., 2009). As the digital landscape evolves however, the idea of self has been extended to online communication technologies such as the internet, smartphones, virtual worlds, and video/ digital games (Belk, 2014). The “extended self” occurs when external objects, possessions and identities become viewed as part of the “self” because of the power or control that can be forced upon them (Belk, 1988). Role playing games are popular because they allow an individual immerse into the game narrative through personalizing and controlling the selected avatar character (Turkay & Kinzer, 2014). Through this customization, the player becomes more immersed in the game, which increases the saliency of messages due to its personal relevance (Vanhatupa, 2011). Using the avatar customization to attract a player’s attention, role playing games initiate information processing which is pivotal to facilitating sustained behavior change (Thompson, 2012). Because research has pointed to differences in preferences among gamers, customization may enhance the effectiveness of digital games developed for sexual health (DeSmet, Shegog, Van Ryckeghem, Crombez, & De Bourdeaudhuij, 2015).
Simulations and Role Playing
Simulation games could be of great benefit to sexual health education because real-world activities are mimicked and practiced in a safe gaming environment (DeSmet et al., 2015). Simulation and role playing games allow players to participate in a virtual representation of a real world situation and maneuver through game activities without any real-world consequences (Thompson, 2012). Through using the combination of emotional storytelling and character immersion, role playing increases a player’s personal stake in a video game’s outcome. Although some believe that using simulations and role playing can diminish the perceived seriousness and impact of the activity on health, others suggest that gaming strategies increase intrinsic motivation, behavioral self-efficacy and adoption rates (McCallum, 2012).
Avatar Self-Representation, Projection & Relatedness
Avatars are becoming a constant presence within digital and virtual world realities because they are malleable objects that allow users to customize self-presentation in diverse ways, while maintaining the user’s privacy (Yee & Bailenson, 2007). Avatars allow for expressive freedom over an otherwise static online identity and are especially important for gamers who are still forming their own in person and online personal identities (Vasalou, Joinson, Banziger, Goldie, & Pitt, 2008). Because young people are in these early stages of identity formation, they engage in wishful identification and may choose avatars with characteristics they would like to possess themselves (Konijn & Bijvank, 2009). The player behind the avatar regularly experiences the emotions attached to achievement or failure in the gaming situation, which often leads to continued adoption of the avatar’s identity (Li, Liau, & Khoo, 2013).
Self- representation is defined as an individual’s ability to express their own self-image (Park & Chung, 2011). In digital gaming environments, self-representation is more flexible and easy to transform as users can customize their own avatar to form a digital and animated representation of themselves (Yee & Bailenson, 2007). Gamers benefit from the opportunity to select a ready-made character with physical attributes to express individual identity (Jin, 2009; Kim & Sundar, 2012). Research suggests that the representations that people make of themselves online are an amalgamation of their actual and ideal selves (Bessière, Seay, & Kiesler, 2007). Actual self is the way in which a person sees himself or herself now, whereas ideal self is the way in which a person would like to see himself or herself (Abel, Buff, & O’Neill, 2013).
Proteus Effect suggests that users in online environments conform to the expectations and stereotypes related to the individual identity cues of their avatars (Yee & Bailenson, 2007). Because digital games simulate real-world environments how a gamer identifies himself/herself may influence the actions they choose to participate in and outcomes they achieve during the digital game. Additionally, because avatar users and gamers often feel connected to their self-representations (ideal vs. actual), real world behaviors can also be impacted (Kim & Sundar, 2012). The repetitive internalization of the identity of the avatar is a powerful and seductive strategy of identification that influences the player to treat the avatar as if it was himself/herself (Cohen, 2001; Li et al., 2013).
Consistent with Proteus Effect, it is hypothesized that college-aged men playing as their ideal self will feel more self-efficacious towards the targeted behavior and therefore have a greater intent to get the HPV vaccine due to their increased confidence playing the game as who they would want to be. Alternatively, those playing the game with an avatar representing their “actual self” will have increased experiential learning and engagement and thus an increased risk perception of the HPV virus and greater intent to get the HPV vaccine. This is because they are visualizing their character as they really are in real life. This mergence or alignment of their self-image will make the game experiences more relatable and therefore the in game consequences more salient and applicable to their real life. Therefore, our research hypotheses for this study are:
Customizing an avatar character based on an individual’s perception of their actual self will be associated with an increase in one’s perceived risk of the HPV virus.
Customizing an avatar character based on an individual’s perception of their ideal self will be associated with an increase in one’s self–efficacy to receive the HPV vaccine.
Customizing an avatar character based on an individual’s perception of their actual and ideal selves will be associated with an increase in behavioral intention to receive the HPV vaccine.
Theoretical Framework
The Health Belief Model (HBM) has been used extensively to study vaccination beliefs and behaviors (Glanz, Rimer, & Viswanath, 2008). According to Krieger and Sarge (2013), health messages are only salient when perception of threat (risk) is aroused in relation to perceived severity and perceived susceptibility. Research has also indicated that perceived risk/threat and self-efficacy has been identified as theoretical constructs that can impact HPV vaccination intention uptake in males (Fontenont et al., 2014). According to Grace-Leitch and Shneyderman (2016), vaccine acceptability among men is high when perceived susceptibility to HPV and self – efficacy is high. This mirrored a similar study that concluded that HPV vaccine acceptability being associated with perceived severity, barriers and HPV vaccine self-efficacy (Mehta, Sharma, & Lee, 2014).
Although behavior change is often measured in research studies and is included in the Health Belief Model as an outcome, behavioral intention was used as a proxy for this study as it is the most important antecedent of health behavior (Fogel & Ebadi, 2011). Behavioral intention is defined as a person’s the subjective probability that one will choose to engage in a given behavior. Behavioral intention is the hallmark construct of the Theory of Reasoned Action and Planned Behavior (Ajzen, 1991; Gutierrez et al., 2013). In health communication research and practice, behavioral intention is one variable that is often targeted due to its high predictive validity in relation to willingness and motivation to adopt a specific behavior (National Library of Medicine, n.d.).
Methodology
Participants
This study was conducted at a large research-intensive university in the southeastern United States. To be included in the study, males had to be enrolled as full-time students, between the ages of 18-26 and non-recipients of the HPV vaccine. After IRB approval was received for the study, the University’s registrar office provided a database of male undergraduate and graduate college students meeting the study’s age and enrollment requirements. Of the 16,365 males enrolled at the University, a simple random sample of 6,000 men was generated using computer software. This sample represented 36% of the male population at the University. Researchers intentionally oversampled men to account for the trend of low participation rates of college age men in research studies related to HPV (Priest & Knowlden, 2015).
Recruitment emails were sent out to the sample of 6,000 men. SuperSaaS (2018) scheduling software was used to facilitate participant enrollment, and participants were asked to sign up for a 1-hour (60 minute) appointment to participate in the study. Although the software enabled automatic generic reminders to confirm session times for participants, researchers also emailed all enrolled study participants an appointment confirmation, with their Participant ID number and a link to an electronic informed consent and survey.
Procedure
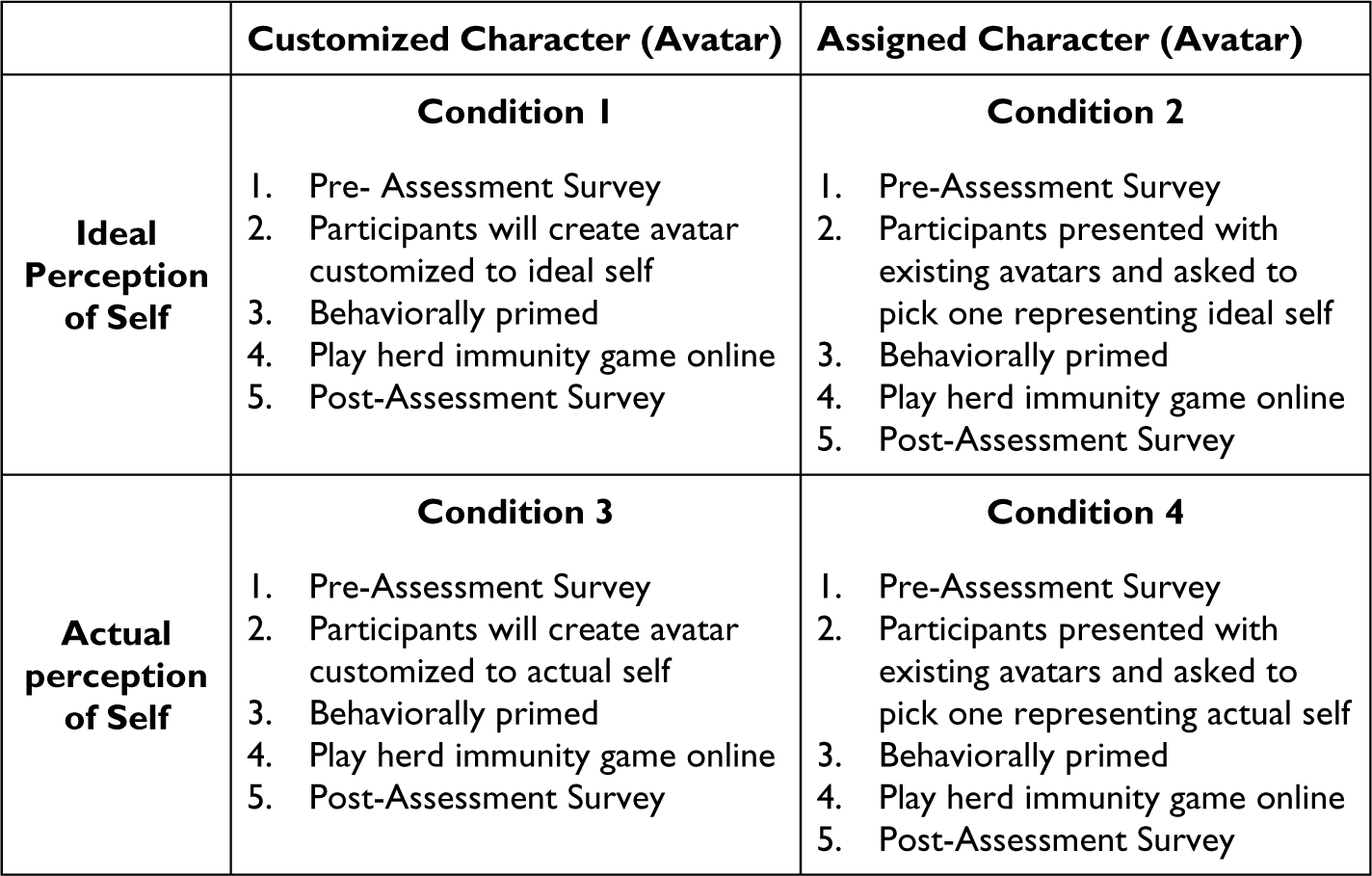
Once participants completed the electronic informed consent and pre-assessment survey administered using Qualtrics, they were randomly assigned into one of the four condition groups (see Figure 1). During the experimental study, two gaming stations were used. Each station was equipped with a Lenovo laptop, gaming mouse, thought listing exercise, and pen.
Experimental design conditions.
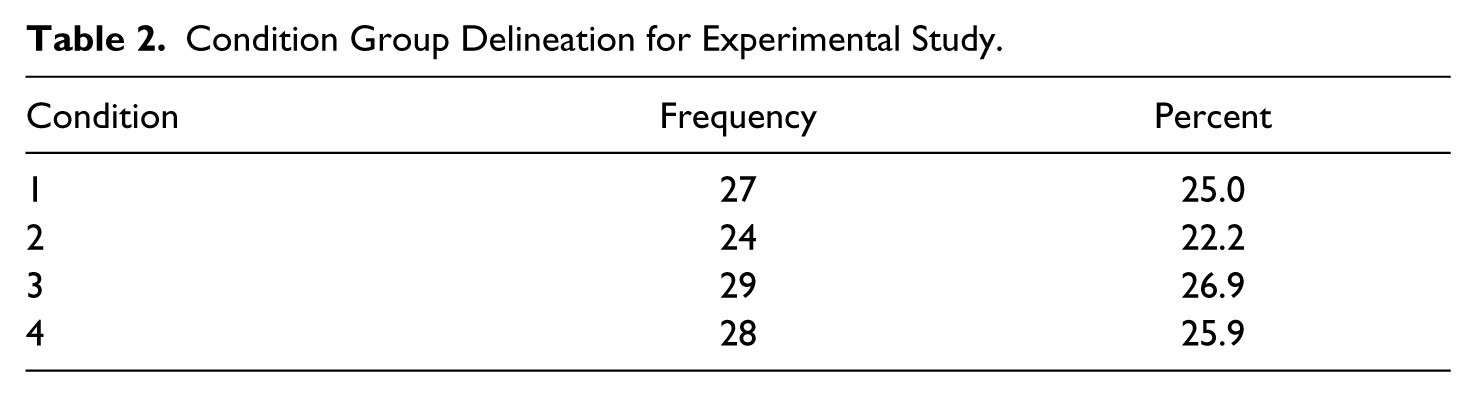
Participants were randomly assigned into 4 experimental conditions (see Table 2). Each condition group played the game as a different avatar character. The lead researcher provided participants with specific instructions on how to customize or select from a group of pre-set avatar profiles in Sitepal to use during the gaming experiment (A_HPV1 to A_HPV6) (see Figure 2). Condition 1 participants (n=27) were asked to customize their avatar character to represent how they would ideally like to look. Condition 2 participants (n=24) was asked to pick one of the existing avatar characters that best represented how they ideally would like to look. Condition 3 participants (n=29) was asked to customize their avatar character to represent how they actually looked. Condition 4 (n=28) was asked to pick one of the existing avatar characters that best represented how they actually looked (Oddcast Company, 2018).

SitePal assigned avatar profiles.
Following avatar selection, participants were behaviorally primed using the thought listing method often used in persuasion studies to measure elaboration (Cacioppo, Von Hippel, & Ernst, 1997). Using this method, students were given a paper form that asked them to “List 3 reasons why male college students should take precautions to prevent HPV” and “List 3 ways that male college students can prevent the spread of the HPV virus.” Participants were behaviorally primed to think about HPV prevention, because the VAX game used as the stimulus for this study did not include HPV-specific messages during the actual gaming experience. Rather, the thought listing exercise was conducted to encourage users to associate the spread of the infectious disease during the game as the spread of the HPV virus If the VAX-HPV association was not organically made during this thought listing activity, instructions were also included after the exercise to inform participants that they would be playing a HPV video game as their designated avatar character.
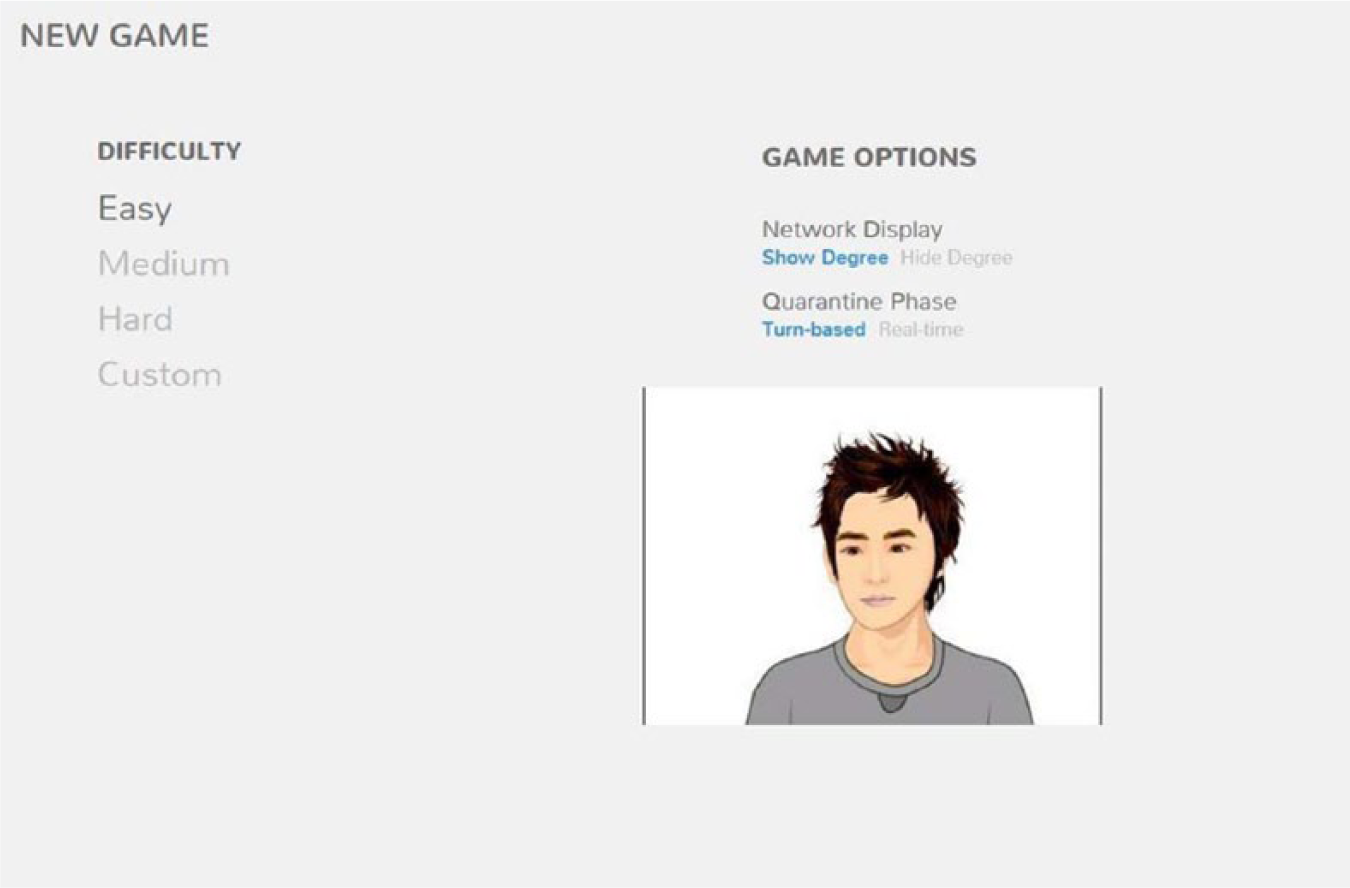
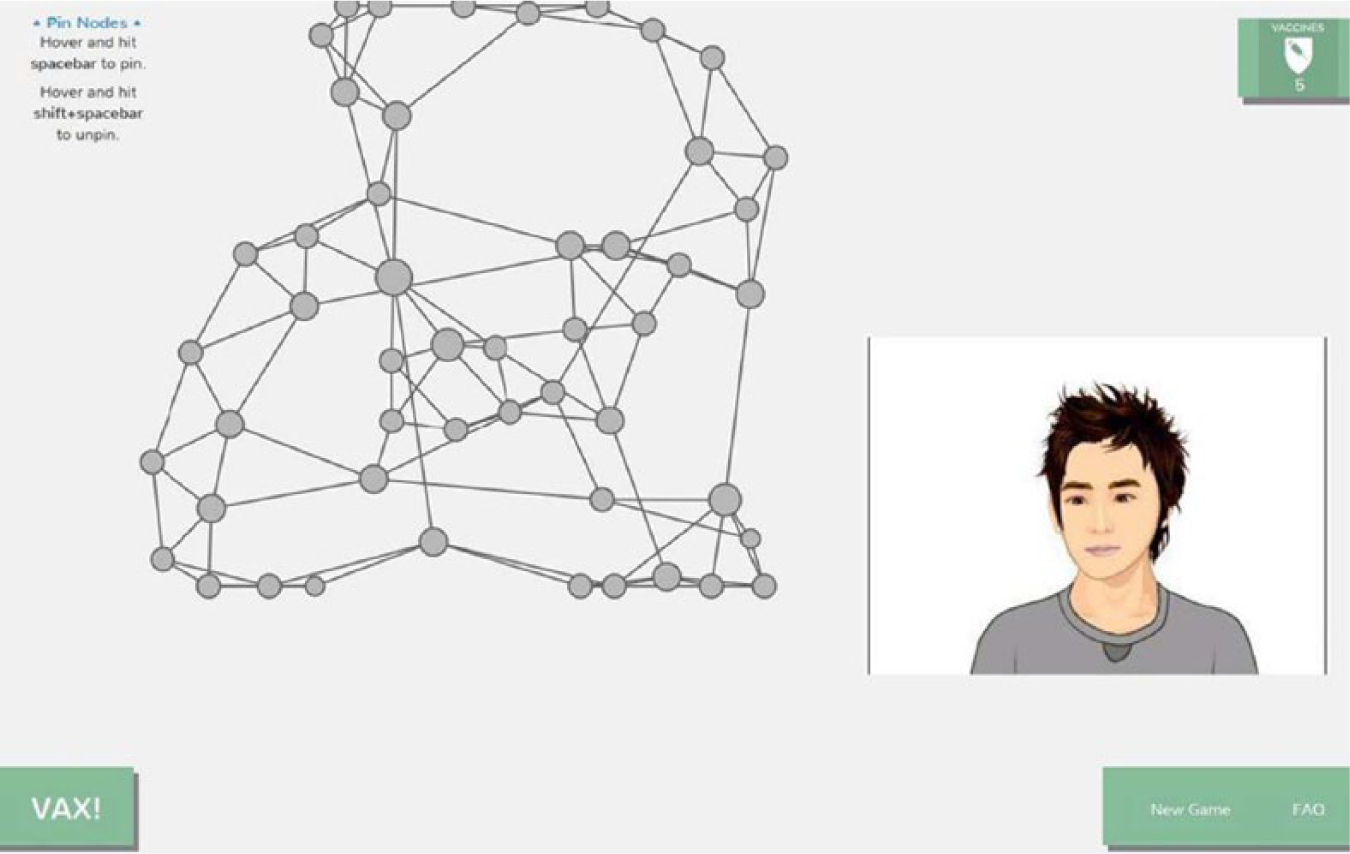
While the participant was completing the thought listing exercise, the research staff embedded the code of the participant’s avatar into the game so that they could see the avatar and assume the role of the avatar while playing the game. An existing digital game called Vax! (http://vax.herokuapp.com/) was used in this study. Developed in 2014 by Ellsworth Campbell, a doctoral student affiliated with Penn State University’s Salathe Group, the Vax! game presents an interactive learning environment by which users are immersed into contagion scenario within which a disease is spread across a network of individuals. According to the instructions, “players are tasked to prepare for an outbreak by vaccinating a network that resembles human social networks. After distributing vaccines, an infectious outbreak begins to spread, and the player is tasked to quell the epidemic by quarantining individuals at risk of becoming infected. Vax! is a puzzle-game infused with chance that was inspired by real-world challenges, infectious disease modeling, and addictively rewarding gameplay” (Salathe Group, 2014, p. 1). Before playing the Vax! Game, participants were instructed to complete a “tour” activating the avatar to appear on the “gaming option” screen (see Figure 3). The avatar remained present during the game (Figure 4) and only disappeared once results were presented to gamers at the conclusion of the Vax! gaming sessions. Post-assessment surveys were administered to participants immediately following gameplay using Qualtrics online survey software. Participants were compensated with a $10 Visa debit card for their participation in the study.
Game play screen.
Gaming option screen.
Measures
The independent variables (IVs) in this study were categorical: (a) avatar character (assigned/customized) and (b) perception of self (ideal/actual (Abel et al., 2013; Bailey, Wise, & Bolls, 2009; Sah, Ratan, Tsai, Peng, & Sarinopoulos, 2017). The dependent variables (DVs) included the following continuous variables: (a) risk perception (b) self-efficacy and (c) HPV vaccine intention. Behavioral intention was used as a proxy to behavior change. Scale items included on the survey were adapted from a scale used in previous HPV studies (Katz, Kam, Krieger, & Roberto, 2012). Three items measured risk perception, three items measured self-efficacy, and four items measured behavioral intention. The questions in the survey measured dependent variables using a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree). The total score for each of the constructs of interest (risk perception, self-efficacy and behavioral intention) was computed by summing up the scores of each statement used to measure that construct. This was done at both pre- and post-assessment. There were three statements used to measure risk perception, thus a minimum score possible was 3 and maximum score possible was 21. There were three statements used to measure self-efficacy, thus a minimum score possible was 3 and maximum score possible was 21. There were four statements used to measure behavioral intention, thus a minimum score possible was 4 and maximum score possible was 28. The scales were within the acceptable range with respect to internal consistency for self-efficacy (α = 0.812) and intention (α= 0.836). Although risk perception was a variable of interest for the previous study the scale was used in, Cronbach’s alpha was not reported. In our study however Cronbach’s alpha of 0.910 was reported for risk perception which indicated an excellent level of internal consistency. Other questions collected data on age, race, ethnicity, student status/classification, health insurance coverage, religious/spiritual affiliation, and current sexual health practices and beliefs (Division of STD Prevention, 2015; Ward, Dahlhamer, Galinsky, & Joestl, 2014).
Data Analysis
All statistical analyses were conducted using SPSS v24.0 software. Pearson correlation coefficients were calculated to examine the relationships between the pre and post-test score for risk perception, self-efficacy and behavioral intention. A descriptive analysis was conducted to collect measures of central tendency and variation for each variable. Pearson’s r correlation coefficients were calculated to determine the relationship between pre- and post-test scores for each dependent variable (risk perception, self-efficacy and behavioral intent) (see Table 3). A Between-Subjects (split plot) Factorial Analysis of Variance (ANOVA) with repeated measures was used to test differences between the means on the outcome variables across our experimental conditions. Condition group was treated as a between-subject factor with pre- and post-test scores treated as two levels of the within-subject variable. Main and interaction (type of avatar X perception of self) effects were computed.
Results
Demographics
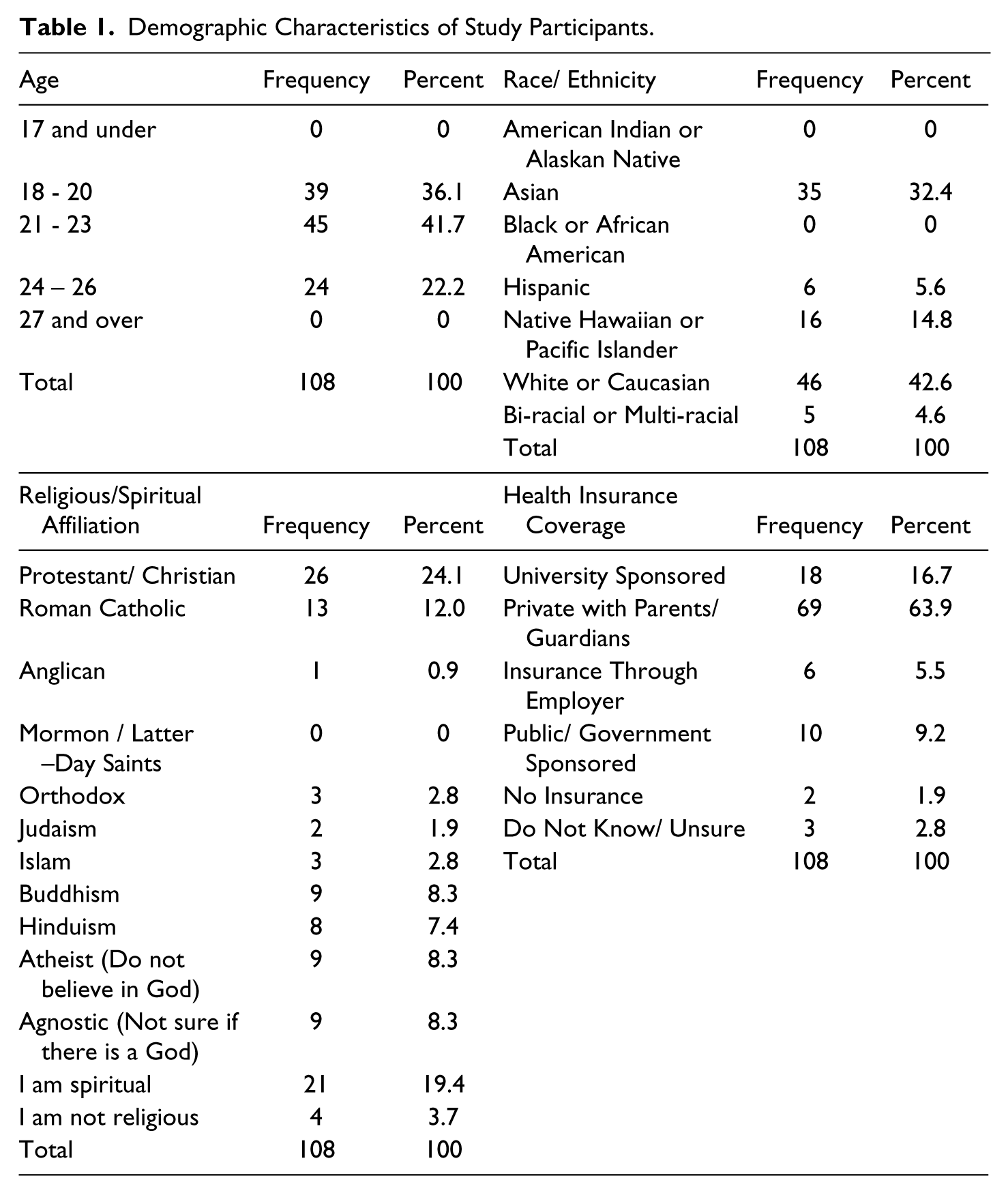
A total of 168 participants initially enrolled in the experiment, with 108 (64.29%) completing the protocol. Study participants were about evenly distributed with respect to age: 18-20 years old (n=39; 36.1%), 21-23 years old (n=45; 41.7%) and 24-26 years old (n = 24; 22.2%). Participants self-identified as being White or Caucasian (n=46; 42.6%), Asian (n=35; 32.4%), Native Hawaiian or Pacific Islander (n=16; 14.8%), Hispanic (n=6; 5.6%) and Bi-racial or Multi-racial (n=5; 4.6%). None of the respondents of this study identified as Black/African American or American Indian/Alaskan Native. Our sample group did not match the demographics of the institution, with the exception to the higher level of involvement of Caucasian males in the study. Of the total number of students enrolled at the institution, demographics for males were White or Caucasian (n=12,491; 23.9%), Asian (n=1,690; 3.2%), Native Hawaiian or Pacific Islander (n=72; 0.13%), Hispanic (n=3,695; 7.0%) and Bi-racial or Multi-racial (n=480; 0.9%) (College Tuition Compare, 2017). When asked about their spiritual or religious affiliation, 24.1% were Protestant or Christian (n=26) and 19.4% self-identified as spiritual (n=21). Most of the participants reported having health insurance through a private plan under their parents/guardians (n=69; 63.9%) and of that amount 19.4% (n=21) agreed that cost or health insurance coverage would not stop them from getting the HPV vaccine (see Table 1).
Demographic Characteristics of Study Participants.
Condition Group Delineation for Experimental Study.
Correlations Between Pre- and Post- Test Scores for Risk Perception, Self - Efficacy and Behavioral Intention.
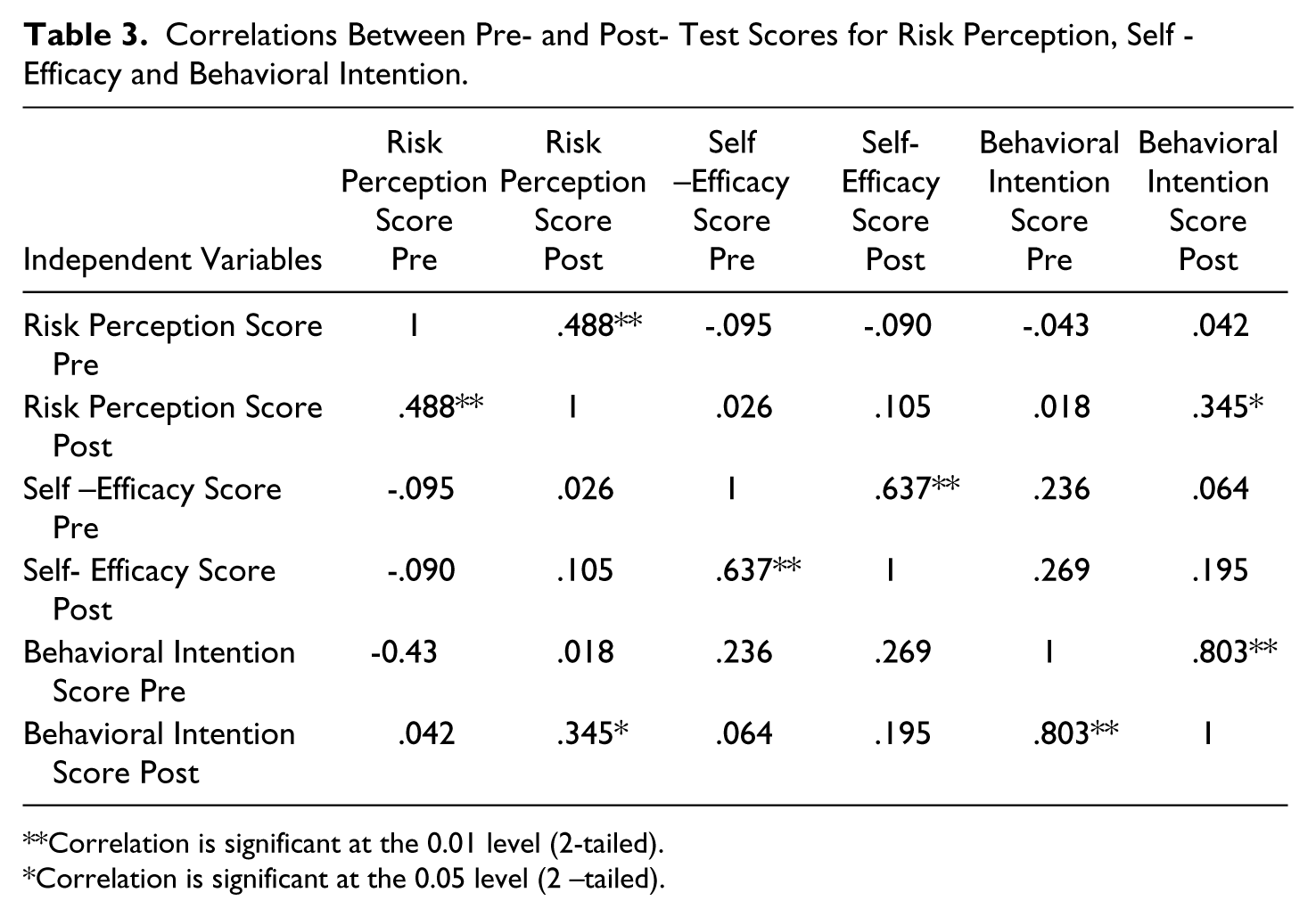
Correlation is significant at the 0.01 level (2-tailed).
Correlation is significant at the 0.05 level (2 –tailed).
Participants in this study identified as freshmen (n=14; 13%), sophomores (n=18; 29.6%), juniors (n=24; 22.2%), seniors (n=22; 20.4%), graduate students (n=29; 26.9%), and professional students (n=1, 0.9%). The majority of participants pursued majors in the College of Engineering (n=37; 34.3%), College of Liberal Arts and Sciences (n=35; 32.4), and College of Business Administration (n=13; 12%).
Current Sexual Health Practices
Overall, 88% of our study sample self-identified as straight (n=95), whereas 4.6% self-identified as gay (n=5) and bisexual (n=5). When asked about sexual activity in the last 6 months, 55.6% indicated that they had been sexually active (n=60). More than half of the study participants (n=88; 81.4%) had less than 5 total lifetime sexual partners. Nearly 48% (n=52) reported between 1 and 4 sexual partners. When asked about condom practices in the last 6 months, 25.9% (n=28) always used condoms, 19.4% (n=21) sometimes used condoms and 16.7% (n=18) never used condoms. The majority of the sample reported never being diagnosed with an STD (n=104; 96.3%).
Digital Gaming Practices
Most of the participants in our study played video games prior to the study (n=95; 88%). Of those who played video games, the top three genre played most frequently were Role Playing Games (n=20; 18.5%), Sports (n=16; 14.8%) and First Person Shooter (n=15; 13.9%). Of our study participants, 20.4% played video games less than 1 hour per week (n=22), 23.1% played 1-3 hours per week (n=25) and 21.3% played 3-6 hours per week (n=23). Additionally, almost half of the participants preferred to play video games using a dedicated game console such as an Xbox, PlayStation Wii™ (n=49; 45.4%). Laptops or Personal Computers (PCs) were identified as the second most preferred platform (n=34; 31.5%) with smartphones ranking third (n=12; 11.1%).
Thirty-one percent (n=34) of our participants indicated that they had received health messages while playing a video game; 68.5% (n=74) indicated that they had not. Despite previous exposure, 87% (n=94) of gamers indicated that they would be receptive to receiving health messages while playing a video game. Nearly 40.7% of respondents indicated that they were ‘likely’ to be receptive to playing an existing video game embedded with HPV messages (n=44) as well as a game developed to increase knowledge and awareness of HPV (n=44). However, 53.7% (n=58) of respondents indicated that they were ‘extremely likely” to be receptive to HPV information presented in a HPV game in lieu of a lecture/assignment within a college sexual health course.
Risk Perception
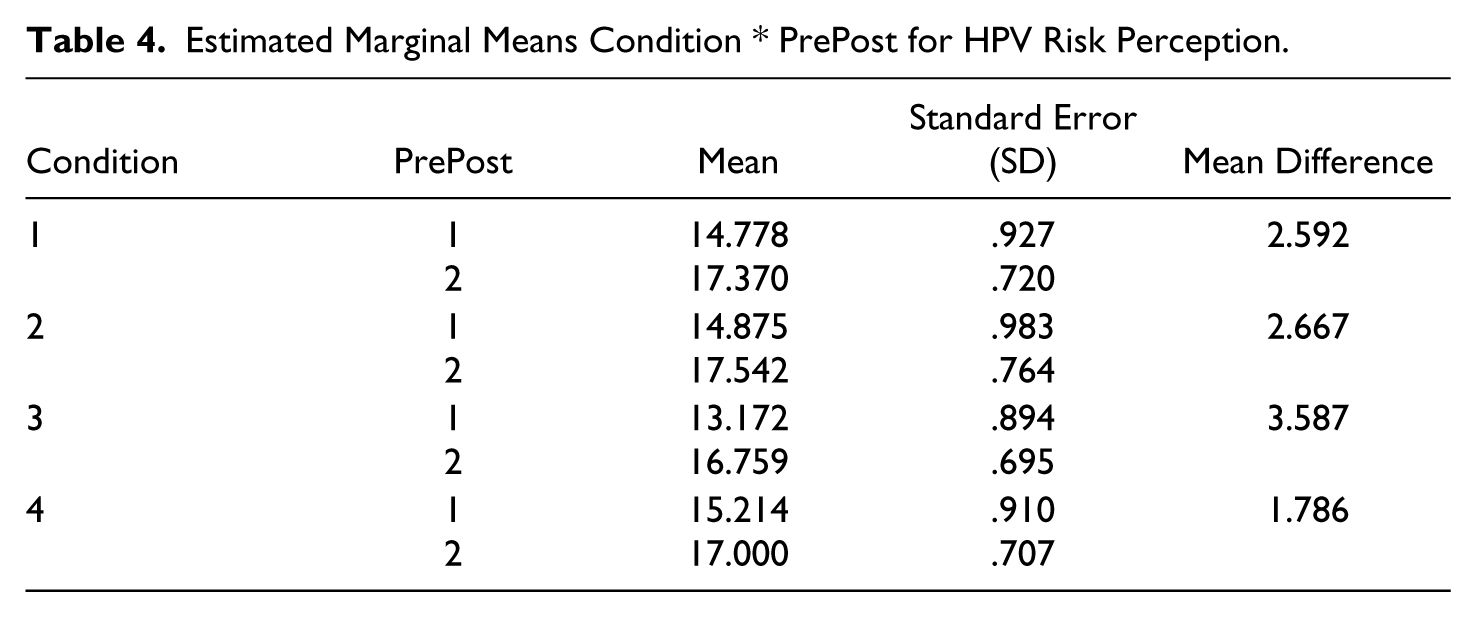
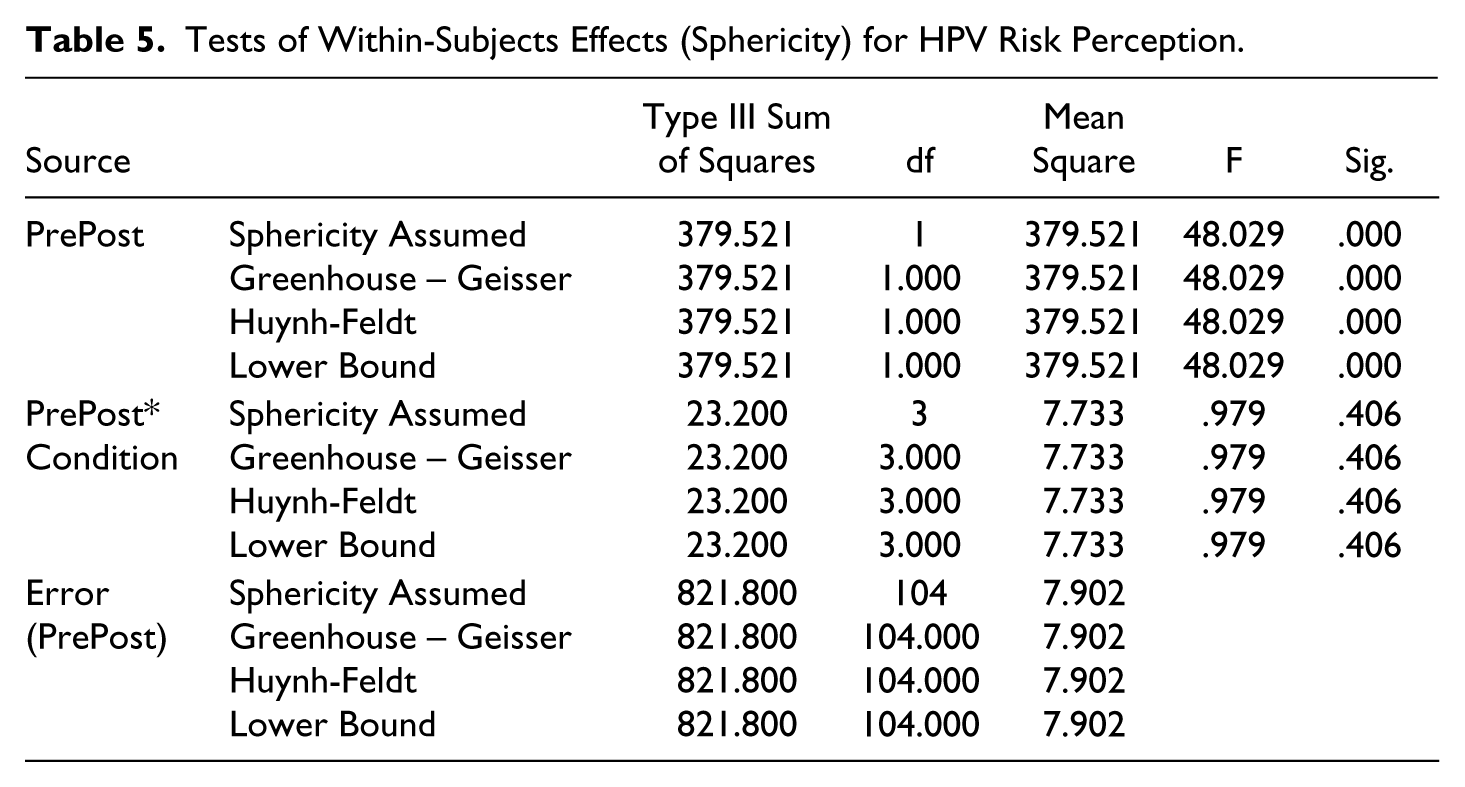
There was not a statistically significant interaction between avatar type and perception of self (F (3,104) = 0.979, p=.406) in the model and no significant main effects for condition group (F (3,104) = .657, p=.581). Therefore, we cannot support our hypothesis. Despite having no main or interaction effect for risk perception, our analysis did report a significant main effect for the experimental game with avatar (regardless of type) as a stimulus (F (1,104) = 48.029, p<0.001). Participants in Condition 3 (customized avatar, actual self-perception) showed the largest mean difference (3.587) in risk perceptions for the HPV virus (see Table 4 and 5).
Estimated Marginal Means Condition * PrePost for HPV Risk Perception.
Tests of Within-Subjects Effects (Sphericity) for HPV Risk Perception.
Self-Efficacy
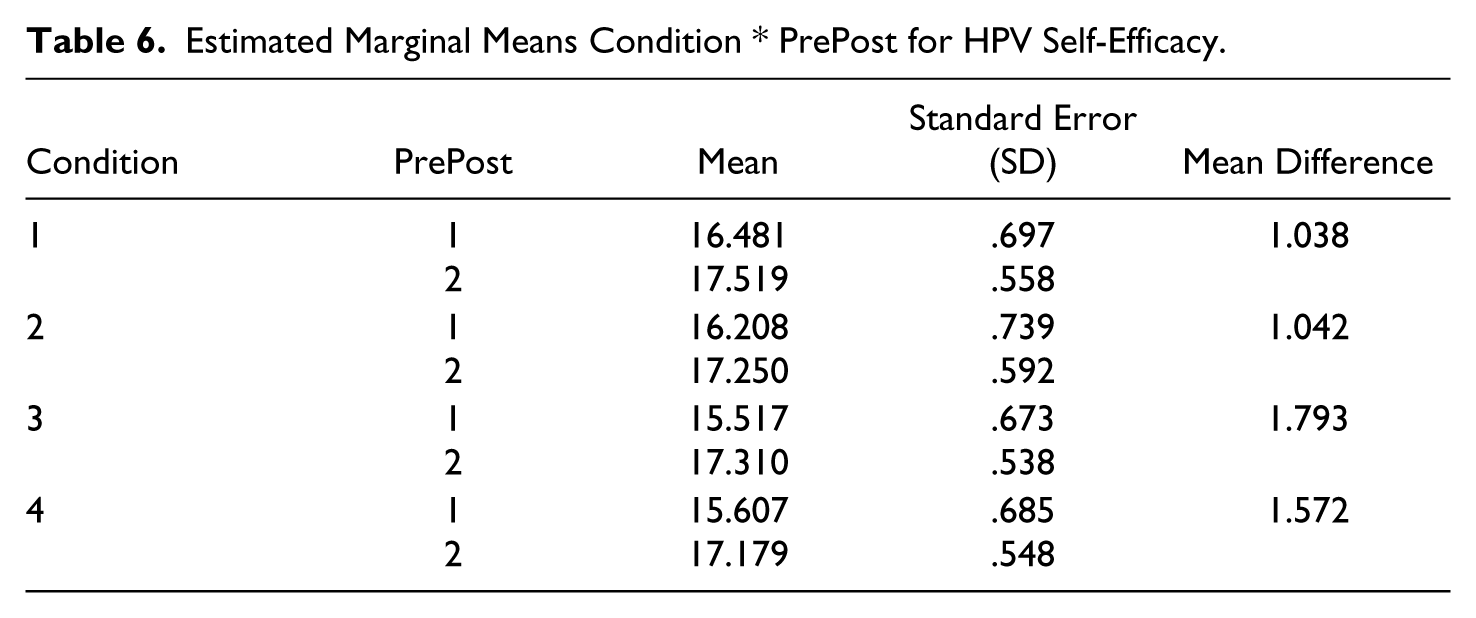
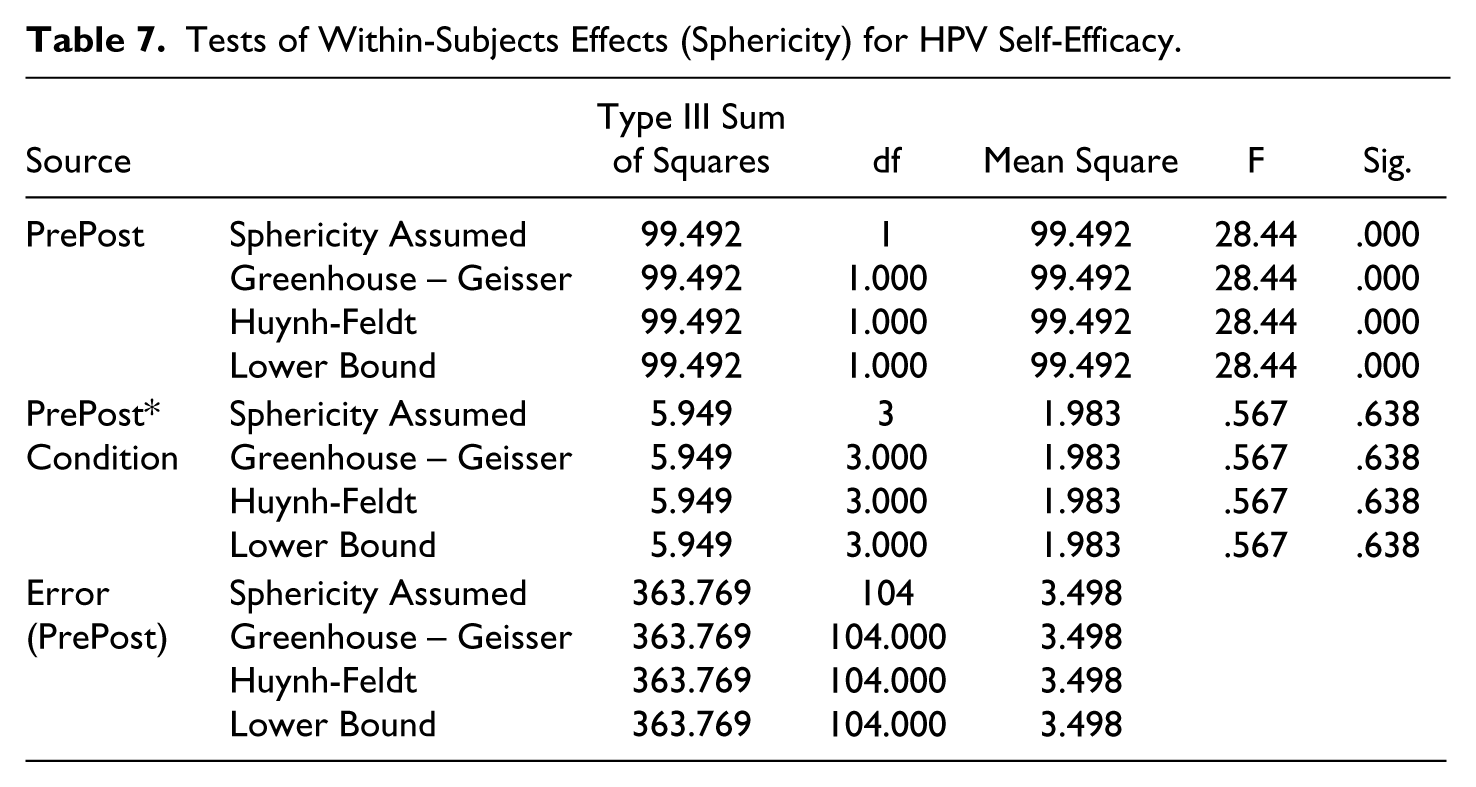
There was not a statistically significant interaction between avatar type and perception of self (F (3,104) = 0.567, p =.638) in the model and no significant main effects for condition group (F (3,104) = .254, p =.859). Therefore, we cannot support our hypothesis. Our analysis did report a significant main effect for the experimental game with avatar (regardless of type) as a stimulus (F (1,104) = 28.44, p<0.001). Condition 3 (customized avatar, actual self-perception) had the largest mean difference (1.793) demonstrating that for experimental data, having a customized avatar most representative of one’s actual self is most indicative of an increased level of self-efficacy or confidence to receive the HPV vaccine (see Table 6 and 7).
Estimated Marginal Means Condition * PrePost for HPV Self-Efficacy.
Tests of Within-Subjects Effects (Sphericity) for HPV Self-Efficacy.
Behavioral Intention
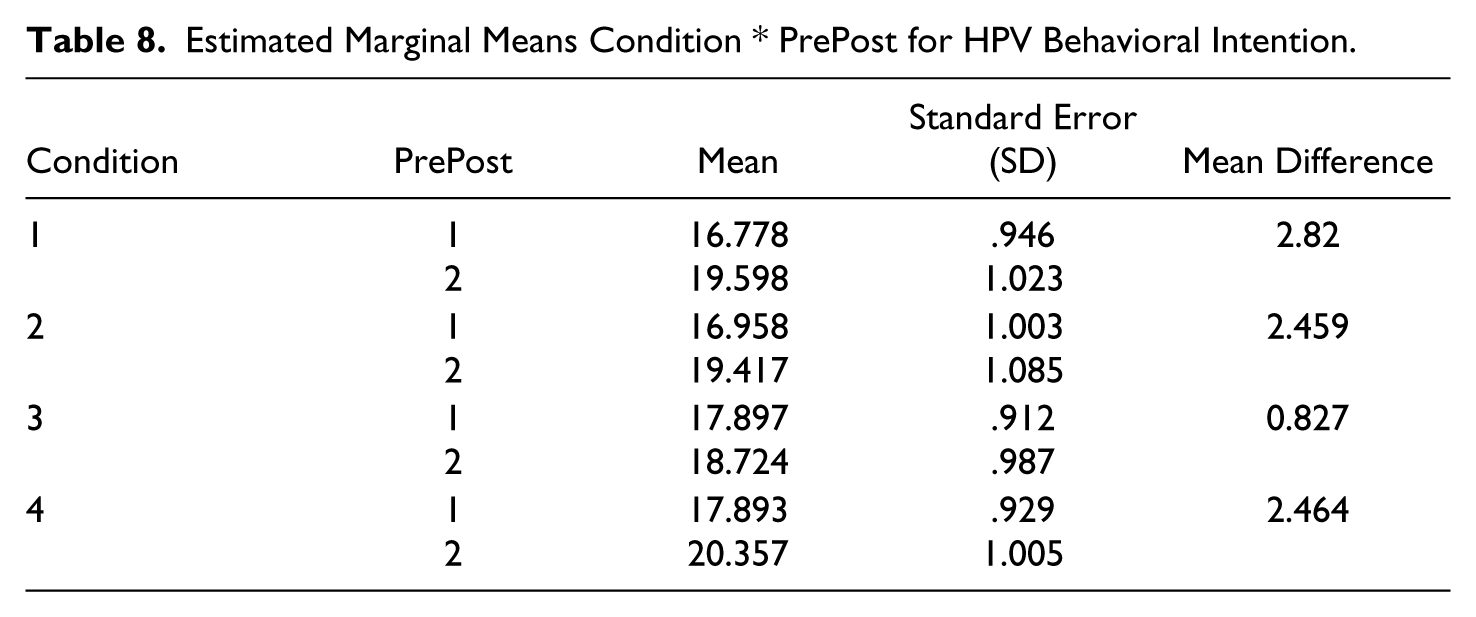
There was not a statistically significant interaction between avatar type and perception of self (F (3,104) = 1.549, p=.206) in the model and no significant main effects for condition group (F (3,104) = .249, p=.862). Therefore, we cannot support our hypothesis. Despite having no main effect (condition group) or interaction effect for behavioral intention, our analysis did report a significant main effect for the experimental game with avatar (regardless of type) as a stimulus (F (1,104) = 33.907, p<0.001). Condition 1 (customized avatar, ideal self-perception) had the largest mean difference (2.82); whereas, Condition 3 (customized avatar, actual self-perception) had the lowest mean difference (0.827) demonstrating that for experimental data customizing an avatar to represent your ideal self was the most indicative of an increased level of behavioral intention to receive the HPV vaccine (see Table 8 and 9).
Estimated Marginal Means Condition * PrePost for HPV Behavioral Intention.
Tests of Within-Subjects Effects (Sphericity) for HPV Behavioral Intention.

Discussion
Digital gaming shows promise as a communication tool for delivering health interventions and improving sexual health behavior among the digital native population. This study is the first to our knowledge that explores use of digital gaming to improve HPV and HPV-related vaccine outcomes among college men. Although our results were not statistically significant, our data analysis did indicate an increase in gain score for risk perception, self –efficacy and behavioral intention when participants were able to customize their avatar to look like their ideal or actual self. This reflected similar research that indicates that playing as their actual self would lead to higher perceptions of physical risks, such as HPV risk (Kim & Sundar, 2012). Our results were comparable to previous research that identified that, “the more they visualized their ideal body through their desired avatar, the more motivated they were to engage in preventative behaviors” (Kim & Sundar, 2012, p. 1363). Results for self-efficacy however, proved to be significantly different to research previously conducted. According to Kim and Sundar (2012), the greater the risk perceived by players playing as their actual self, the less motivated they would be engage in proactive behaviors.
Limitations and Implications for Future Research
Although results are promising, there are limitations to our study. First, the use of avatars with the Vax! Game may not have been an appropriate or automatic fit. In conversation with gamers, participants indicated that they saw Vax! as more of a strategy game. Additionally, although an adequate range of customization options was available to users, the SitePal software limited extensive creativity in changing physical features or attributes. Compared to the vivid graphics of today’s role playing games, the avatars appeared “cartoony” in nature which could have affected the perception of the avatar truly looking like one’s ideal or actual self. Lastly, the “assigned” and “customized” avatars may not have been significantly different in appearance to produce any treatment or interaction effects among experimental groups.
As part of the experiment, research staff had to provide instructions to participants so that they could progress and complete the study as planned. Detailed instructions were necessary due to limitations in being able to alter the existing Vax! Game to allow for the avatar customization, behavioral priming exercise, and game to be housed in one space and naturally flow as one stimulus. Because of this, participants may not have been able to immerse themselves in the Vax! Game and achieve a constant level of flow while playing, which could have affected the results.
It can be concluded from our study that the use of an avatar is important; however, the type of avatar may not be as important when discussing games related to the HPV virus and HPV vaccine. To explore this idea further, studies should look at the use of more advanced avatar customization software similar to the vivid imagery and graphics often found in off-the-shelf video games. Future studies should also consider utilizing a game where the customization of the avatar and priming exercise is integrated in the game as one system rather than via separate software and experimental components used in our study.
This study did not include a true control group to truly measure impact of the independent variables. Therefore, future research should include a true control to further test effects and include background variables (sexual protection/condom use, orientation, identity) in the analysis due possibly mediating the interaction. Apart from background variables, future researchers should also look at the possibility of using full body avatars customized to ideal and actual perceptions of self since HPV is a sexually transmitted disease affecting the sexual organs. Since sexuality, manhood and overall appearance extend beyond the face, full body avatars may be more salient for men.
Because two of the constructs measured in this study came from the Health Belief Model (i.e., perceived threat, self-efficacy) with another being derived from the Theory of Planned Behavior (i.e., behavioral intention), future HPV studies for college age men should investigate the impact of digital gaming that leverages all HBM constructs, including perceived benefits and perceived barriers of taking action. Although this study measured behavioral intention as a proxy for behavior change, future research should also directly measure completion of the 3 shot HPV vaccination series by the target population. A gap still exists in the literature on HPV vaccination studies among college age men measuring vaccine series completion.
Lastly, there was limited racial/ethnic diversity in the participants of the digital gaming study. None of the study participants identified as Black or American Indian/Alaskan Native. Placing an emphasis on vaccinating males from racial/minority groups can protect females from those circles and communities as young adults tend to have sexual partners from within their own community (Jeudin, Liveright, Del Carmen, & Perkins, 2014). Since research shows that racial/ethnic minorities account for a disproportionate number of HPV-related cancers) cultural differences could affect vaccine uptake (Okafor, Hu, & Cook, 2015. Future research should expand this study to be replicated among specific isolated racial and ethnic groups (Anderson, 2015; Daley et al., 2011). Such studies could demonstrate positive improvements in in preventing HPV-related cancers and conditions among males from various minority groups. This approach could prove to be a strategic way to achieve herd immunity among risky sexual networks and thereby reduce the disproportionately high rates of cancer in female minority groups such as Blacks and Hispanics.
Conclusion
Research on the human papillomavirus (HPV) and vaccine is still lacking among college age males. However, extensive opportunities exist to utilize information communication technologies like digital gaming change HPV knowledge and impact HPV vaccine. Despite the fact that a large percentage of college age men play video games, video gaming interventions have been used heavily in other aspects of health promotion such as physical activity, diabetes prevention and management, anxiety and depression. Few interventions and research studies have explored the application to sexual health and specifically as it relates to HPV prevention. The digital game or video game presents itself as the optimal platform to communicate and educate college age men about a topic that could be very stigmatizing and uncomfortable to discuss. Furthermore, using a digital game can have direct impact on HPV risk perception increasing the likelihood of vaccine uptake. The team that contributed to our study included researchers in public health, health communication, media psychology, computer engineering, research methodology and evaluation. Therefore, an interdisciplinary team of stakeholders involved in the HPV vaccine conversation should all partake in the development of a digital game that would be most receptive by college age men.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the NIH/NCATS Clinical and Translational Science Award to the University of Florida UL1 TR000064.