
Abstract
Background
In recent years, serious games have been used as an educational method in various fields such as economy, marketing, military, education, and health as a training method. Pressure injuries (PIs) are a significant health problem and clinical quality improvement issue throughout the world. Implementation of prevention strategies has gained importance in all healthcare settings due to the negative effects of PIs. Educating patient relatives on PI prevention is essential.
Aims
This study aimed to develop a serious game for the training of patient relatives on PI prevention and evaluate the game in terms of knowledge acquisition and its features.
Methods
The study was carried out as a single-group quasi-experimental pre-test and post-test design in three stages between August 1, 2020-April 30, 2022. In the first stage educational content, knowledge assessment test, and game evaluation questionnaire were prepared. A web-based serious game (PreSore: Pressure Injury Prevention Game) was developed in the second stage. The participants played the game in the third stage, and data was collected. The study sample consisted of patient relatives (n=55). A knowledge assessment test (pre-test, post-test, and re-test) and a game evaluation questionnaire were administered for the data collection.
Results
It was determined that there was a significant increase in knowledge scores after the PreSore game implementation (p < .001). Most of the participants indicated that the information in the game was easy to understand (98.2%), they wanted to share their educational experience with others with the digital game method (96.4%), and they found the game was authentic (94.5%).
Conclusions
The study revealed that the PreSore game is a method that could be used to train patient relatives on PI prevention. Integrating the PreSore into daily practice in healthcare institutions and conducting prospective studies are recommended.
Introduction
Thanks to the advancement of technology, there have been innovations and developments regarding the education methods employed in the healthcare field (Friesgaard et al., 2017; Yao et al., 2016). In recent years, one such technology, digital platform games, have been used as an educational method in various fields such as economy, marketing, military, education, and health as a training method in addition to its use for entertainment purposes (Boyle et al., 2016; Gentry et al., 2019). The basis of these educational games is gamification, which involves applying game design elements, features, and benefits to real situations and problems. Accordingly, these games have a clearly stated educational purpose and simulate real-world events or processes designed to solve a problem (Gentry et al., 2019; Nacke & Deterding, 2017; Stepanovic & Mettler, 2018).
The primary purpose of using games as educational material is to give the learner a more interactive, engaging, easily accessible, and understandable educational experience where the learner manages the process (Rutledge et al., 2018). Players of these games work to achieve the game objectives or reward systems by performing various simple or challenging activities offered to them in a subject-specific, virtually simulated environment in line with the game's flow. Therefore, the players make discoveries and trials of their free will, make decisions, and experience success or failure due to these decisions. The players can repeat these experiences consecutively until they achieve the desired result (Garris et al., 2002).
It has been reported that serious games support the player's learning by providing interactivity, being interesting and immersive with in-game reward opportunities, enabling discovery by guiding the player, and being a method of knowledge transfer (Pourabdollahian et al., 2012). In addition, it is pointed out that using games would have beneficial effects such as providing education without time and place restrictions, increasing patient satisfaction, improving health behaviors by educating the society, promoting health culture, increasing motivation, reducing the negative physical and psychological consequences of the disease, ensuring lifestyle change and maintaining well-being (Safdari et al., 2016).
In a systematic review (n = 30) on serious games in health profession education, it was determined that these games contribute to the development of knowledge and skills of health professionals (such as surgical skills, drug administration, first aid, and patient safety) and further studies examining their contribution to patient outcomes and health economic were recommended (Gentry et al., 2019). A systematic review and meta-analysis of randomized controlled trials, which evaluates the effectiveness of serious games in improving knowledge and self-management behaviors in young people with chronic diseases (n = 9), reported that there was an increase in knowledge scores (n = 7) and self-management scores (n = 2) in study groups in which serious games were used (Charlier et al., 2016). In an interventional study with pre-test and post-test design investigating the effect of serious games on awareness and behavioral change about lifestyle-related diseases in different age groups (adults aged 23-67, n = 22; university students, n = 76; and high school students, n = 24) in Japan, participants were asked to answer evaluation questions consisting of 16 items before, immediately after and two to four weeks after the game. It was reported that there was a significant relationship between perceived behavioral control and behavioral intention in adult participants, university students, and high school students before and after the game. The study concluded that serious games contribute to the development of learning and perception, which promotes the improvement of certain lifestyle behaviors (Egashira et al., 2022).
Pressure injuries (PIs) are a significant health problem and clinical quality improvement issue throughout the world due to their negative effects, such as increasing mortality and morbidity and healthcare costs, prolonged hospital stay, and decreasing quality of life of patients and their families. A pressure injury is defined as localized tissue damage to the skin and/or subcutaneous tissues over bony prominences and under medical devices. Although the prevalence of PIs varies across countries and clinical care settings, they are common (European Pressure Ulcer Advisory Panel-EPUAP, National Pressure Injury Advisory Panel-NPIAP, & Pan Pacific Pressure Injury Alliance-PPPIA, 2019). In the systematic review and meta-analysis study on acute care (n = 42), the global prevalence was 14.8%, and the hospital-acquired prevalence was 8.4% (Li et al., 2020). In the systematic review and meta-analysis study on intensive care units (n = 22), the global cumulative incidence of PI in intensive care unit patients was 10.0%-25.9%, and the prevalence was 16.9%-23.8% (Chaboyer et al., 2018).
Implementation of prevention strategies has gained importance in all healthcare settings due to the negative effects of PIs (Ayello & Sibbald, 2019; Ellis, 2017). Prevention areas include risk assessment, skin assessment and care, measures to reduce the impact of pressure, friction, and shear, nutritional management, and continuous education. Training patient relatives as informal caregivers is critical in implementing prevention strategies and ensuring adherence to these strategies (EPUAP, NPIAP & PPPIA, 2019). On the other hand, preventing PIs becomes challenging, especially in home care, due to limited access to resources and educational opportunities (Ellis, 2017). In home care, patients' relatives take on significant roles as informal caregivers (Kokorelias et al., 2019; Probst et al., 2014). Therefore, including patient relatives in the care team and obtaining their cooperation supports the continuity of care and the success of person-centered PI prevention strategies (Pokorna et al., 2019; Kokorelias et al., 2019; Lor et al., 2016). In this context, educating healthcare professionals and patient relatives in implementing PI prevention strategies is crucial, as well as ensuring adherence to these strategies in all healthcare settings (EPUAP, NPIAP & PPPIA, 2019). Moreover, it is necessary to provide training and awareness of patient relatives by using new educational methods in line with current knowledge for their effective involvement in care processes (Pokorna et al., 2019; Vuolo, 2014).
In a scoping review study on evidence-based prevention and management of PIs in home care (n = 4); in studies conducted on patients receiving services from home care agencies in the United States and Belgium, it was determined that although 54.3% of the agencies provided educational materials to the patient relatives and more than 85% of agencies taught the repositioning, only 22.2% of the patient relatives caring for the patient with a high risk of PI were encouraged by the home care nurse to participate in care, and 21.4% participated in repositioning practices (Karadağ & Çakar, 2022). In a descriptive online survey study conducted with patients’ informal caregivers from 27 countries, it was determined that caregivers' most important care goal for the individual they provided care for was preventing PIs. The educational topics that caregivers rated as important or very important in the study included how PIs occur, preventing PIs during immobility, risk factors, skin care and being knowledgeable about PIs (Haesler et al., 2022).
Although there are numerous materials and methods for training healthcare professionals regarding PI prevention (Beeckman et al., 2010; Bredesen et al., 2016), a recent systematic review reported that approaches toward patient relatives are very limited and insufficiently focused on their training on that topic (O'Connor et al., 2021). However, since patient relatives play crucial roles in the care of patients and are significant members of the care team, educating them on PI prevention is essential. In this regard, developing understandable, easily accessible, and scientific knowledge-based technological educational approaches is a significant need in contemporary healthcare (Fleming et al., 2017; Satterfield, 2015). When the relevant literature was examined, no study was available concerning the training of patient relatives on preventing PIs by using serious games (Krath et al., 2021; O'Connor et al., 2021). Additionally, considering the abovementioned positive effects of these games on learning and the easy accessibility of game-providing technological tools, it was thought that this educational approach could be used to train patient relatives on PI prevention. In this regard, this study intended to develop and evaluate a serious game for individuals other than health professionals on PI prevention.
Materials and Methods
Aim
This study aims to develop a web-based serious game incorporating gamification, three-dimensional modeling, and animation to train patient relatives on PI prevention. The primary objective is to evaluate the effect of the developed game on knowledge acquisition by focusing on the knowledge level related to PI prevention and its features according to the participants' opinions.
Research Questions
In this study, answers were sought to the following questions: 1. What is the serious game's effect on patient relatives' knowledge level regarding PI prevention? 2. How do the descriptive characteristics of patient relatives affect their knowledge level regarding PI prevention? 3. What are the opinions of patient relatives about the features of the serious game?
Design
This study was carried out as a single-group quasi-experimental pre-test and post-test design. The study population consisted of patient relatives. The purposive sampling method was employed in determining the sample size due to the lack of specific numbers on patients at risk for PI in acute care hospitals and home care, as well as the absence of structured studies in the literature on the education and knowledge levels of patient relatives regarding PI prevention (Erdoğan et al., 2018). Therefore, the Cohen effect size (d-value) method was used to calculate the sample size. A medium effect size was determined for the test group, where the difference between the pre-test and post-test would be measured (McConnell et al., 2019). In this context, participants (n = 55) were included in the study according to medium effect size (d = 0.5), 95% confidence level, and 95% test power.
Inclusion criteria for the participation were as follows: a) being 18 years of age or older, b) being literate, c) being a patient's relative at any PI risk level, d) ability to use a computer, and volunteering to participate in the study. Individuals who did not meet these criteria were not included in the study.
The researchers reached the study participants living in different provinces in Turkey through wound care professionals (nurses and physicians) in terms of inclusiveness. Accordingly, a detailed information message about the study was prepared and sent to the nurses and physicians working in wound care who are already in the researchers' professional network through social media platforms (e-mail, WhatsApp, Facebook, and LinkedIn). They were asked to refer volunteers among the patient relatives they cared for to the researchers. One researcher interviewed those referred patient relatives, providing information about the study, and evaluating their eligibility according to the sample selection criteria. Those patient relatives who volunteered to participate were included in the study after obtaining written and verbal consent.
Data Collection Tools
The researchers created the Question Form on the Descriptive Characteristics of the Participants, the Pressure Injuries Knowledge Assessment Test, and the Educational Serious Game Evaluation Questionnaire for data collection.
Question Form on the Descriptive Characteristics of the Participants
This form examined sociodemographic information, previous PI care and training experiences, and computer game experiences of the participants.
Pressure Injuries Knowledge Assessment Test
This test evaluated participants' knowledge levels. In the literature, there are no available valid and reliable standard knowledge assessment tools developed to evaluate the knowledge levels of patient relatives regarding PI prevention. Therefore, a knowledge assessment test was prepared based on the current literature and the researchers' experiences following the learning objectives and the characteristics of the target group of the study. A content validity study was conducted to evaluate the adequacy and suitability of the Pressure Injuries Knowledge Assessment Test (PIKAT) before its use. The knowledge test was created with three sub-dimensions: 1) Conceptual Knowledge, 2) Etiology and Physiopathology, and 3) Prevention Interventions. While the Conceptual Knowledge sub-dimension included questions related to the definition, importance, and various conceptual topics on PIs, the Etiology and Physiopathology sub-dimension questions covered the mechanism of PI formation and risk factors, and the Prevention Interventions sub-dimension questions included preventive measurements.
PIKAT consisted of 20 questions with triple-response options (test items), 16 questions in the test had one correct answer, and four had more than one correct answer (Conceptual Knowledge: Four questions with six test items, Etiology and Physiopathology: Eight questions with 10 test items, Prevention Interventions: Eight questions with 12 test items). In the scoring, the answers to the questions with a single answer were evaluated as one item, and each correct answer to the questions with more than one answer was evaluated as one item. Correct answers were scored one (1), and incorrect answers scored zero (0). Accordingly, while the maximum score (number of correct answers) that can be obtained from the test was 28, the total score for the Conceptual Knowledge sub-dimension was six, the total score for the Etiology and Physiopathology sub-dimension was 10, and the total score for the Prevention Interventions sub-dimension was 12 (Supplementary File 1).
Educational Serious Game Evaluation Questionnaire
This questionnaire aimed to evaluate game features developed within the research scope. When relevant literature was examined, it was determined that specific evaluation questions tailored to the developed game were utilized. Therefore, test items were created using the literature on digital education methods (Diehl et al., 2017; Márquez-Hernández et al., 2019; Tan et al., 2017). This questionnaire consisted of thirteen questions to evaluate the game's features. The response options of each test item were designed on a 3-point Likert scale (Disagree, Undecided, Agree) (Junne et al., 2016; Streiner et al., 2015). A content validity study was conducted to evaluate the adequacy and suitability of the Educational Serious Game Evaluation Questionnaire (ESGEQ) before its use. The evaluation had no scoring system, and number and percentage calculations were made for each question according to the participants' responses.
Statistical Analysis
Data was analyzed using the IBM® SPSS® for Windows, Version 28.0 (Armonk, NY, USA, IBM Corp., 2021). Descriptive statistics were reported as a number, percentage, mean, median, and standard deviations. The Shapiro-Wilk Test was employed as a statistical method to assess the normal distribution of the data. Non-parametric tests such as the Mann-Whitney U, Kruskal-Wallis, and Wilcoxon Signed Rank Test were preferred for comparisons involving quantitative data without normal distribution (Hayran & Özbek, 2017). p < .05 was considered as statistically significant.
Ethical Considerations
This study was approved by the university’s Biomedical Research Ethics Committee (Approval Date: April 22, 2020, Decision Number: 2020.164.IRB2.054) was obtained before the study. In addition, written and verbal consent were received from the participants by being informed, including on issues of ensuring confidentiality.
Study Procedure
The study was carried out in three stages between August 1, 2020-April 30, 2022 (Figure 1). Study Flow Chart.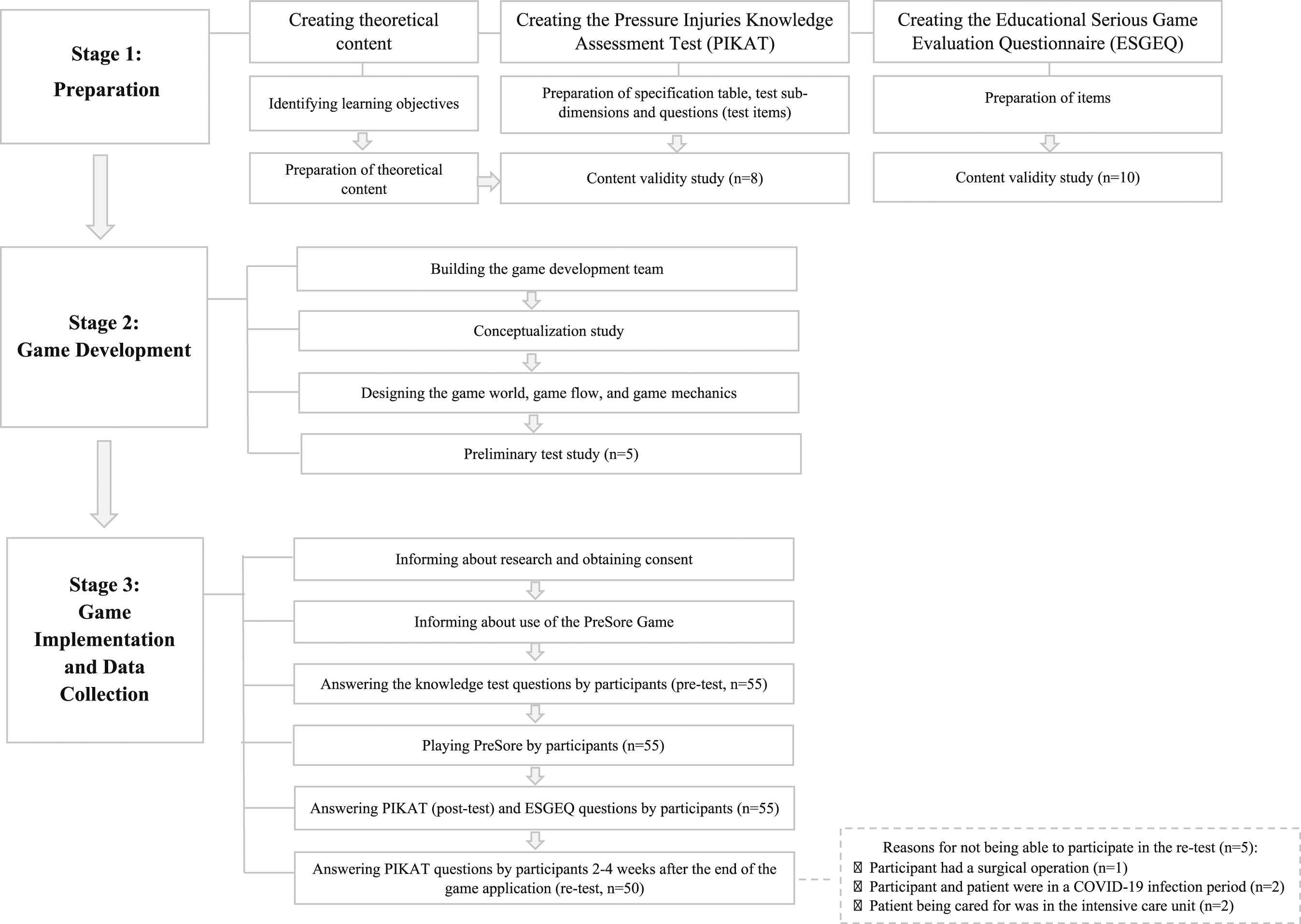
Stage 1: Preparation
Theoretical content, PIKAT, and ESGEQ were prepared within this stage. The studies performed in this context include creating learning objectives, creating theoretical content, creating PIKAT questions, and content validity study.
Since the game is an educational material, learning objectives were identified in accordance with Bloom's Taxonomy to cover the knowledge dimension (factual, conceptual, procedural, and metacognitive knowledge) and the cognitive process dimension (remembering, understanding, and applying). Bloom's Taxonomy was originally developed by Bloom in 1956 to ensure a systematic approach to learning and teaching processes. In the updated taxonomy by Anderson and Krathwohl in 2001, the knowledge dimensions (factual, conceptual, procedural, and metacognitive knowledge) and cognitive process dimensions (remembering, understanding, applying, analyzing, evaluating, and creating) have been redefined (Krau, 2011).
Theoretical content was prepared, including the definition, importance, etiology, physiopathology, risk factors, classification, and prevention practices of PIs by using current literature (EPUAP, NPIAP & PPPIA, 2019; Wound, Ostomy, and Continence Nurses Society-WOCN, 2017). The methodology for content validity studies was followed to assess the adequacy and appropriateness of the learning objectives and field knowledge (Polit & Beck, 2006). In this context, the theoretical contents and PIKAT questions were submitted to the expert opinion of eight people. Experts consisted of five nursing faculty members working in the field of PIs, one faculty member working in the field of educational methods, measurement, and evaluation in education, and two patient relatives.
In addition, ESGEQ questions were submitted to the expert opinion of 10 people. Experts consisted of two faculty members working in the field of digital education, one computer engineering faculty member, two computer engineers, one faculty member working in the field of educational methods, measurement, and evaluation, two nursing faculty members working in the field of education, and two patient relatives.
Expert Opinion Forms were prepared for each evaluation topic (learning objectives, theoretical content, PIKAT, and ESGEQ), and the forms were shared with the experts via e-mail. The experts were asked to evaluate each area and section on a scale of one to four (1: Not appropriate, 2: Somewhat appropriate, 3: Appropriate, 4: Very appropriate). Expert opinions were analyzed by the researchers, the learning objectives, theoretical content, and assessment tools were finalized, and Content Validity Index values were calculated (Polit & Beck, 2006). Content Validity Index values are as follows: a) 0.96 for learning objectives, b) 0.99 for theoretical content, c) 0.91 for PIKAT, and d) 0.95 for ESGEQ.
Stage 2: Game Development
In this stage, a web-based computer game was developed. The game has both Turkish and English language options. During this stage, the following steps were performed:
Building the Game Development Team
A team comprised of one computer engineer academic specializing in modeling and simulation, one graphic design specialist, one software development specialist, one nursing academic specializing in PIs, and one wound care nurse.
Conceptualization Study
The brand and logo of the game (PreSore: Pressure Injury Prevention Game) were designed.
Designing the Game World, Game Flow, and Game Mechanics
The game was created using the Unity three dimensional simulation development platform and the c# programming language. A patient profile (virtual patient) with a risk of PI was created. Care practices within the scope of prevention practices that should be included in a patient's daily care routine with the virtual patient's characteristics were determined. The game world (virtual game simulation environment) was designed to reflect the patient receiving care at home and the care environment. The player's main task in the game world was to complete patient care tasks, preventing PI development in the virtual patient within the 12-minute game cycle (Supplementary File 2). At the end of each game cycle, the player could see a graphical report of the realization rates and scores of the care tasks and evaluate their game performance. According to this report, the player could aim to complete incomplete tasks or replay the entire game. In this context, patient care tasks and all materials to guide the player during these tasks (e.g., instructions, task list, task tools, or materials) were placed in the game world.
Game flow was based on the fact that the player could navigate freely around the game world in the designated time frame, exploring the tasks and materials, making decisions while doing the tasks, and completing the tasks. While the players were performing their tasks in the game, when the game time was over, they could replay the whole game as many times as they wanted and have the opportunity to experience all the tasks repetitively in a virtual simulation environment by trial and error. In addition, the theoretical content, for which special graphic work was done so that the player could read at any time, was placed as a guide information booklet in the library integrated into the game world (Supplementary File 2).
Preliminary Test Study
Before the PreSore was made available to the research participants, preliminary testing was conducted with five patient relatives aged 20-69. Participants were asked to evaluate the ease of play, the use of icons, and in-game instructions. Three visuals and the speed of the click icon have been improved according to preliminary test study.
Stage 3: Game Implementation and Data Collection
During this study stage, the PreSore game was implemented, and data was collected.
An appointment was made with the study participants. The way of participation in the study (face-to-face: n = 13 or online participation: n = 42) was decided by the participants depending on COVID-19 precautions and their preferences. Voluntary participants (n = 55) were given detailed information about the research process, and their consent was obtained. Researchers worked one-to-one with each participant for the implementation of the game.
Before implementing the PreSore, participants were asked to answer PIKAT questions (pre-test). After the pre-test, the participant who accessed PreSore via the web link was registered to the game system. They were informed about the use of the game, and the participants read the instructions in the game if they wanted to. The basic expectation from participants was to complete the tasks given in the game by playing it as much as they wanted. When the participants stated they were ready for the knowledge test after playing the game as many times as they wanted, playing was concluded, and PIKAT (post-test) and ESGEQ were administered.
Two weeks after PreSore implementation, PIKAT (re-test) was shared with all participants (n = 55) on a web link via social platforms (WhatsApp and e-mail). No participant had access to PreSore during this period. The re-test was answered by volunteer participants within two to four weeks after the end of PreSore implementation, depending on the participant's home and work conditions and the burden of caring for the patients in their care. The re-test was answered by 50 participants. Five participants could not answer the re-test because one participant had a surgical operation, two participants were in the COVID-19 active infection period, and two participants' patients were in the intensive care unit.
Results
Descriptive Characteristics of the Participants and Information on the Game Use
Information on the Participants’ Descriptive Characteristics and Game Use.

Knowledge Level of the Participants on Pressure Injuries
Participants’ Pressure Injury Knowledge Assessment Test Scores.
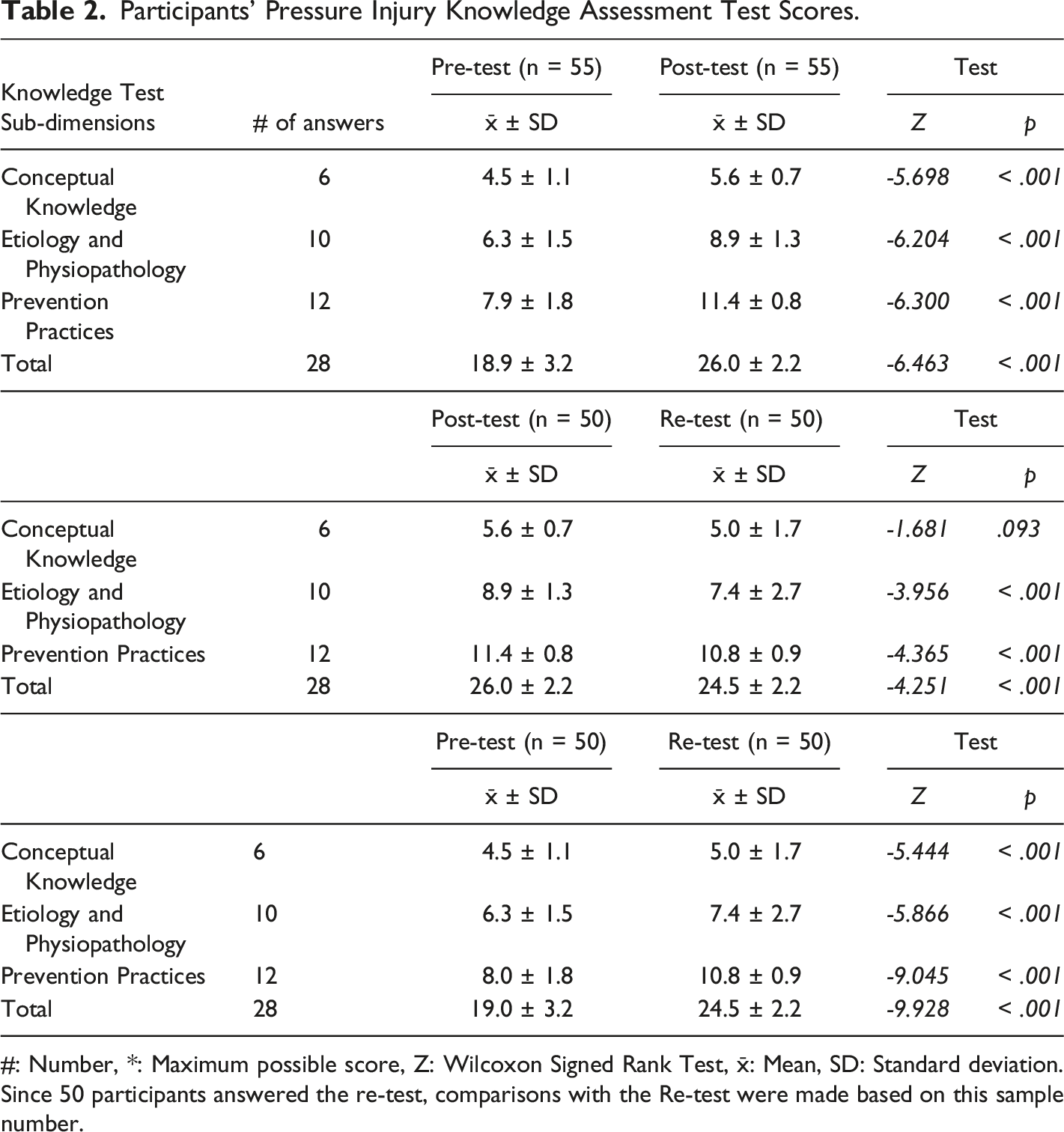
#: Number, *: Maximum possible score, Z: Wilcoxon Signed Rank Test, x̄: Mean, SD: Standard deviation.
Since 50 participants answered the re-test, comparisons with the Re-test were made based on this sample number.
While there was no statistically significant difference between the knowledge scores related to the Conceptual Knowledge sub-dimension in the post-test and re-test, (post-test: x̄ = 5.6 ± 0.7, re-test: x̄ = 5.0 ± 1.7, p = .093), there was a statistically significant decrease in the Etiology and Physiopathology (x̄ = 7.4 ± 2.7, p < .001), Prevention Interventions (x̄ = 10.8 ± 0.9, p < .001) sub-dimensions and total knowledge scores (x̄ = 24.5 ± 2.2, p < .001) in the re-test compared to the post-test (Table 2).
According to the evaluation made according to the correct response rates of the total and sub-dimensions of PIKAT, an increase of 22.1% in Conceptual Knowledge, 41.1% in Etiology and Physiopathology, 43.8% in Prevention Interventions, and 37.8% in total were determined in the post-test compared to the pre-test. Although there was a statistically significant decrease in the post-test and re-test scores, it was found that there was an increase of 21.3% in Conceptual Knowledge, 29.1% in Etiology and Physiopathology, 35.3% in Prevention Interventions and 29.9% in total in the correct response rates between the pre-test and re-test (Figure 2). Correct Response Rates of the Pressure Injuries Knowledge Assessment Test.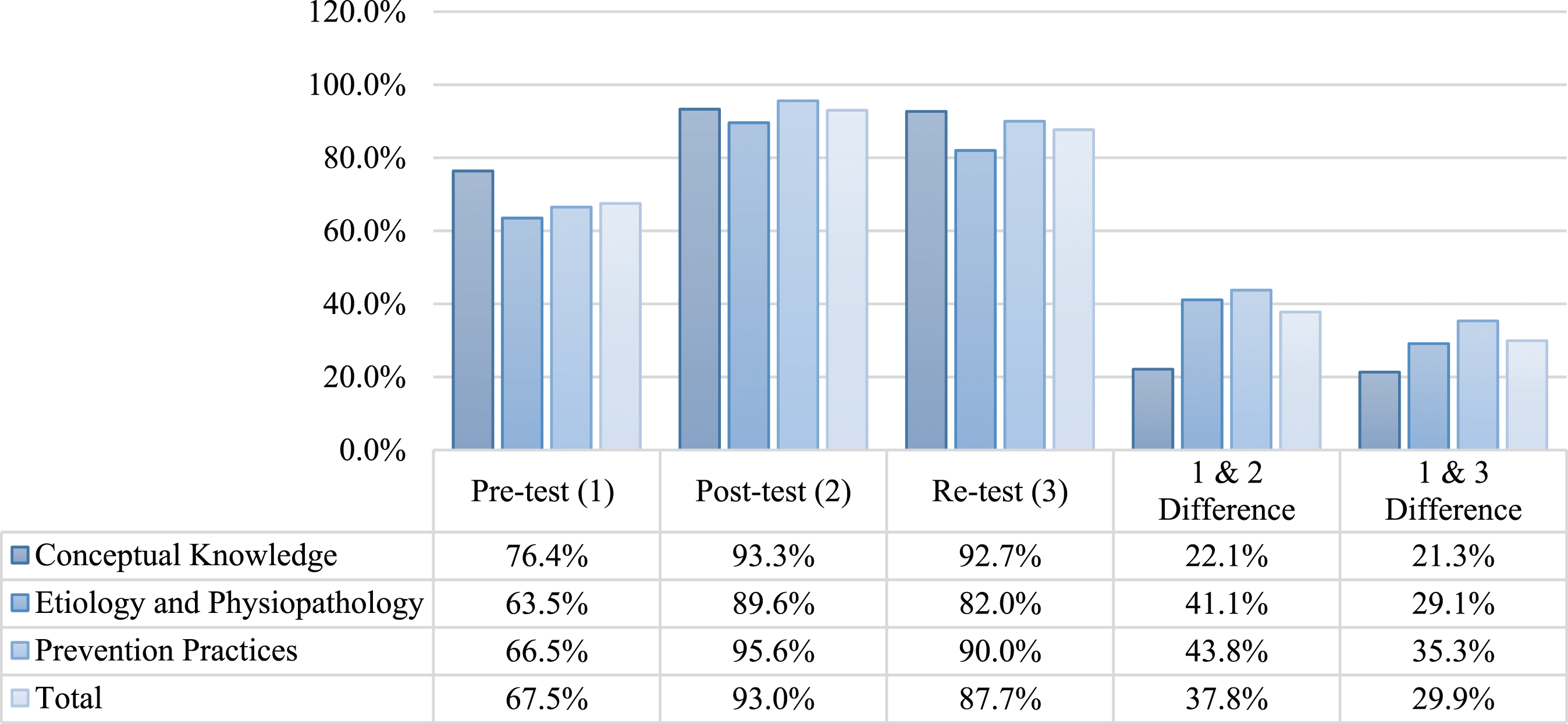
Correct Answer Rates Based on the Pressure Injuries Knowledge Assessment Test.

Participants’ Knowledge Scores according to the Descriptive Characteristics and Game Use.

Participants' Responses on Features of the Game
Participants’ Responses on the Educational Serious Game Evaluation Questionnaire Regarding Features of the PreSore Game.

Discussion
In this study, a serious game (PreSore) was developed to train patient relatives on PI prevention, and its effect on knowledge acquisition and game features were evaluated. A statistically significant increase was found in study participants' total and sub-dimension scores. Although there was a decrease in the re-test and post-test scores, it was determined that the increase in the pre-test and re-test continued.
In a randomized controlled study in which a 30-minute serious game developed for the knowledge and skills of second-year nursing students on blood transfusion was evaluated (control group, n = 46; intervention group, n = 57), an improvement was found in the intervention group participants' post-test knowledge scores and self-confidence scores. The study concluded that gaming technologies have the potential to enable learning and improve learners' knowledge and confidence in safe blood transfusion practice (Tan et al., 2017).
In a randomized controlled study on tracheostomy care of first-year nursing students (control group, n = 43; intervention group, n = 43), it was determined that the post-test scores of tracheostomy aspiration and peristomal skin care were significantly higher than the intervention group. The study recommended using game-based applications in psychomotor skill training (Bayram & Çalışkan, 2019).
A randomized controlled study evaluated the knowledge of family physicians (control group, n = 65; intervention group, n = 69) regarding insulin administration using a computer game. A significant increase was found in the first post-test scores of the intervention group participants. Although the second post-test scores of the intervention group participants were higher, this increase was not statistically significant. The study recommended the intervention as an educational method to improve knowledge (Diehl et al., 2017).
In a randomized controlled study (control group, n = 13; intervention group, n = 14) for primary healthcare education of medical students, a web-based game was used. In the study, the post-test scores of the control and intervention group participants were found to be significantly higher. Although there was a decrease in the second post-test scores of both groups compared to the first post-test scores, it was pointed out that the game may contribute to improving knowledge (Tubelo et al., 2019).
In the literature, the results of studies with similar or different methodological approaches on different topics (e.g., knowledge, skills, behavior, and attitude) and different groups in the healthcare field (Bayram & Çalışkan, 2019; Diehl et al., 2017; Tan et al., 2017; Tubelo et al., 2019) support the findings of this study regarding knowledge levels. Accordingly, it could be argued that the increase in the knowledge scores of patient relatives participating in this study indicated that this method had a positive contribution to knowledge acquisition, and the PreSore might have a supportive role in the training of patient relatives. In the study, the re-test was sent to the participants online two weeks after the PreSore was applied, and the participants were asked to answer the test when they were available. Considering that the participants did not have access to the PreSore game or any other information material prepared by the researchers during this process, the decrease in the knowledge scores between the post-test and re-test is an expected result. On the other hand, the increase in the knowledge scores between the pre-test and re-test leads to the argument that this approach may allow the learners to update their knowledge in case of continuous game use. When the knowledge scores of the participants were evaluated with respect to their descriptive characteristics, it was determined that the post-test knowledge scores increased significantly in all groups. Accordingly, it was interpreted that PreSore is a training material that can be used for training people of all ages, with different educational levels and professions, with and without PI experience, and computer game experience.
In this study, there was an increase in the number of people who answered those questions, which were answered correctly at a low rate in the pre-test and correctly in the post-test. These questions were among the essential information that the participants aimed to gain within the scope of the knowledge and cognitive process dimensions of Bloom's Taxonomy in line with the learning objectives. In addition, these correct answers seemed to cover the most basic etiological factors in the occurrence of PIs and prevention practices (EPUAP, NPIAP & PPPIA, 2019; WOCN, 2017). This was interpreted as PreSore was supportive of the participants' improvement in the dimensions of knowledge and cognitive process targeted to be gained on PI prevention.
In this study, while the entertainment aspect of the game was mentioned as the least agreed upon game characteristic among relevant results, the authenticity of the game, its characteristics related to knowledge, willingness to share game experience, and happiness with the game were the most agreed upon characteristics. Based on this information, it was argued that the educational aspect of PreSore was found appropriate by participants, and it was accepted as an education method. In addition, in the study, the suitability of its duration was determined as the least agreed-upon characteristic. This result was not surprising, concerning participants who did not have computer game-playing experience.
When the relevant literature is examined, although there are studies examining the effect of serious educational games on knowledge, attitude, or behavior, there are limited studies evaluating the effect of the time spent in the game or the number of repetitive games in replayable games directly on the result. On the other hand, considering the assumptions of the Cognitive Load Theory (Krath et al., 2021), it is assumed that games with repetitive game cycles will significantly contribute to learning processes. In addition, considering that most of the participants played the game two times, a player spent approximately 24 minutes in a 12-minute PreSore game cycle just playing the game, allowing for a constructive educational experience. Moreover, it could be argued that the game would help players reinforce their knowledge by repeating or experiencing in-game tasks determined for the subject with repetitive game cycles.
Limitations of the Study
Since the study is a one-group pre-test and post-test design study, this should be considered in the interpretation and generalization of the research results. The fact that participants could access PreSore only on the computer via internet access was experienced as a technical limiting factor. On the other hand, the research's implementation and data collection process coincided with the COVID-19 pandemic conditions. This situation limited face-to-face interaction due to the participants' concern about carrying the infection to their patients, and interviews with a group of participants were conducted online. One of the limitations of the study, coinciding with the pandemic period, was that access to hospitals was limited due to isolation practices, which made it difficult to contact the relatives of patients being treated in acute care institutions. Therefore, the support of nurses and physicians working in the wound care field was needed to reach the study sample. Accordingly, the fact that the re-test application of the knowledge test was conducted in a short period, such as two to four weeks after the end of the PreSore implementation, was another limitation of the study.
Recommendations for Future Research
It is recommended to conduct prospective observational studies on the cognitive and behavioral effects of PreSore with a larger sample group by including caregiver relatives of all patients at risk of PI. Besides, it is recommended that the knowledge assessment test, which was used to evaluate the knowledge levels of participants, be developed as a standardized knowledge level measurement tool for individuals other than healthcare professionals regarding PIs by conducting construct validity and reliability studies.
Conclusion
The data of this study showed that the PreSore game, which was developed within the scope of this study, significantly contributed to increasing the knowledge of patient relatives on PI prevention. The study results showed that the participants acquired essential knowledge that is critical in PI prevention in line with the defined learning objectives. This meant that the PreSore game was an educational method suitable for training the patient relatives and the community on this issue and raising social awareness. In this context, it was recommended that the PreSore should be integrated into daily practice in healthcare institutions (hospitals, palliative care, long-term care, and home care). Moreover, conducting international studies using the PreSore game's English version will help ensure its global use.
Supplemental Material
Supplemental Material - Development and Evaluation of a Serious Game on Pressure Injury Prevention for the Training of Patient Relatives: A Quasi-Experimental Study
Supplemental Material for Development and Evaluation of a Serious Game on Pressure Injury Prevention for the Training of Patient Relatives: A Quasi-Experimental Study by Vildan Çakar, and Ayişe Karadağ in Simulation & Gaming
Footnotes
Acknowledgements
The authors thank all volunteered participants and the European Wound Management Association.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.