
Abstract
Healthcare workers regularly face the risk of violent physical, sexual, and verbal assault from their patients. To explore this phenomenon, a collaborative descriptive qualitative study was undertaken by university-affiliated researchers and a union council representing registered practical nurses, personal support workers, and other healthcare staff in Ontario, Canada. A total of fifty-four healthcare workers from diverse communities were consulted about their experiences and ideas. They described violence-related physical, psychological, interpersonal, and financial effects. They put forward such ideas for prevention strategies as increased staffing, enhanced security, personal alarms, building design changes, “zero tolerance” policies, simplified reporting, using the criminal justice system, better training, and flagging. They reported such barriers to eliminating risks as the normalization of violence; underreporting; lack of respect from patients, visitors, higher status professionals, and supervisors; poor communication; and the threat of reprisal for speaking publicly. Inadequate postincident psychological and financial support compounded their distress.
Introduction
–I was working a night shift … He pumped his fist into my mouth. I ended up with a swollen mouth, cut lip and a concussion. I’m still off work.
The findings of Canadian studies share many similarities to those in research conducted across the globe. A study of Alberta and British Columbia nurses, which explored the effects of both physical and emotional abuse, recommended “targeting prevention strategies not only at the nurse but, perhaps more importantly, at the hospital. Overall, the findings suggest that healthcare institutions are not always healthy workplaces and may increasingly be stressful and hazardous ones.” 9
Statistics released by the Ontario Workplace Safety and Insurance Board show that “In 2014, lost-time injuries due to workplace violence in the healthcare sector greatly outnumbered those in other sectors surveyed.” 10 A survey of paramedics in Ontario and Nova Scotia found that 75 percent had experienced violence in the previous year, 67 percent were verbally assaulted, and 26 percent had been subjected to physical assault. 11 A study of violence in long-term care facilities found that Canadian healthcare workers experience six times more incidents of physical violence than their counterparts in Scandinavian countries.12,13
Minimal research was published on the issue of violence against staff in the healthcare sector prior to 2000. A Medline search using the search string “workplace violence against nurses” conducted in February 2017 resulted in 155 international articles, 149 of which were published from 2000 to the time of the search. Another search using “workplace violence hospital” resulted in 703 articles, 630 of which were published since 2000. They represent research conducted in numerous countries. 14 A recent editorial published by a registered nurse stated that “a disheartening trend evident in the healthcare literature is that violence against nurses appears to be a growing problem globally.” 15
Most studies explored Type II violence, which is “physical or verbal assault of an employee by a client/family member or customer.” 16 It is the most common type of workplace violence in the healthcare setting. 17 While many of the published studies are limited to violence against nurses, others include doctors, 18 hospital aides, paramedics, and other patient-care occupations.11,19–21 Importantly, many studies state that data regarding the incidence of violence against healthcare staff are believed to grossly underestimate the incidence due to widespread underreporting.1,9,22
Consulting With Healthcare Staff
The Ontario Council of Hospital Unions (OCHU), whose members include many of the registered practical nurses, personal support workers (PSWs), dietary, housekeeping, and other healthcare staff represented by the Canadian Union of Public Employees (CUPE), grew increasingly concerned with the number of its members being assaulted and abused. Every one of the 150 registered practical nurses from across Ontario attending a conference on violence in Kingston in January 2016 reported that they had experienced violence at work. 23 A telephone survey of healthcare workers in North Bay, Ontario revealed that 60 percent of all respondents (n = 74), which included both direct patient care and auxiliary workers, had experienced physical violence in the past year; in the subset of nurses and PSWs (n = 44), 85 percent had experienced physical violence, 88 percent had experienced nonphysical violence, and 53 percent had experienced sexual harassment or sexual assault. 24
OCHU partnered with academic researchers in a collaborative effort to explore its members’ experiences of violence on the job, validate their perceptions, and document their recommendations for preventing workplace violence. The occupational health researchers conducted group interviews and analyzed the information they gathered. They were assisted by a nurse, a member of OCHU, who was granted a research fellowship by the host university to recruit participants, organize dates and locations, and record interviews. Between June and September 2016, the facilitators conducted thirteen group interviews with fifty-four healthcare workers in seven communities to identify workers’ perceptions of the risks to themselves and their coworkers of being subjected to violence on the job; effects they experienced when subjected to violence; what barriers, if any, exist to addressing the incidence of violence as described in the literature; and whether any prevention strategies can be formulated for use by a range of bodies such as governments, regulatory agencies, administration, and employee bodies that may reduce the incidence of violence perpetrated against healthcare workers.
Ethics approval was provided by the University of Stirling, the institution with which the academic researchers are associated. Participants’ anonymity was of primary importance. Many participants expressed fear that their employer would become aware of their involvement or trace data to them. Most were aware of the recent firing of a healthcare worker in Ontario who had been quoted by the media after commenting on the issue at a conference on violence. We were told, “People get fired when they speak. Look at that nurse who got fired, who lost her job.” “A family member warned me to shut my mouth while I was here (at the group interview). She said, ‘you’d better be quiet or they’ll fire you.’” Before being asked to sign informed consent forms, they were assured that their confidentiality would be protected to the extent possible given that the interviews were carried out in group settings. All participants agreed to protect the privacy of each other and the research team agreed to follow all ethical guidelines laid out in the approved protocol.
This research was designed to explore Type II violence. Because violence of any degree can have negative effects, the study covers the full continuum of violence, ranging from negative verbal comments to sexual or physical assault. The European Agency for Safety and Health at Work states there is no uniform definition for workplace violence. However, it is generally agreed that “Violence is a generic term that covers all kinds of abuse including ‘homicide, assault, threats, mobbing and bullying; in effect, all behavior that humiliates, degrades or damages a person’s well-being, value and dignity.’” 25 The American Academy of Experts in Traumatic Stress includes “near misses” and “fear of assault or witnessing an assault on a co-worker” in its definition. 26 While physical assaults can be devastating, research has found that nurses may be more in need of ongoing support for nonphysical assaults, which can cause “frustration, anger, stress, fear, and anxiety.” 27
Method
A descriptive qualitative research approach was taken to explore the phenomenon of violence against healthcare staff. 28 Open-ended questions were used to gather experiential data from participants in group interviews regarding their experience with violence.
Participants were recruited with the assistance of their local union executives. Some were specifically invited because they had reported violent episodes, but an open invitation was also made to anyone who wished to participate. Because those providing direct patient care are statistically at a higher risk for violence, the researchers prescreened the participants to ensure that direct care staff were sufficiently represented.
Groups ranged in size from two to seven individuals; they averaged four to five individuals per group. The groups were nonhomogeneous as they included individuals representing various healthcare occupations, types of institutions, communities within the province, ages, genders, ethnic groups, and years of experience. This wide range of participants would thereby provide for the identification of similarities and differences in the data collected and would enhance the reliability and transferability of the findings. 29 Overall, the researchers consulted with twenty-seven registered practical nurses, six PSWs, nine administrative and related staff, five cleaners/housekeepers, three dietary staff, two personal care assistants, one physiotherapy assistant, and one maintenance staff. Forty-one participants were women and thirteen were men. Five of the participants self-identified as indigenous, two as Black or African-American, two as Asian, three as Eastern European immigrant, and the remaining forty-two as Caucasian or Canadian. They worked in acute care hospitals, long-term care, forensic, or detoxification centers and had work experiences in a wide range of departments. There were sixteen facilities in communities across the province represented by the participants in a total of thirteen group interviews. In addition, several participants spoke of violence they had experienced during previous employment in other healthcare facilities in Ontario as well as in home healthcare positions. The work experience of all of the participants totaled 1153 years. There was a wide age differential between the youngest at 23 and oldest at 65; the average age was 47 years. The average work experience was twenty-one years and ranged from three to forty-five years. All but one of the participants, a dietary staff person, had personally experienced violence—most on a regular basis. All had witnessed many episodes.
The group interviews, which ranged in length from two to three hours depending on the number of participants, were semistructured to allow for elaboration and exploration. 30 They began with each participant describing an incident or incidents of violence that he or she had experienced or witnessed. The immediate and underlying causes of the incidents were then explored. Subjects were asked not only how they were physically affected by the violence, but also if and how they were psychologically affected. They described and discussed what happened postincident, such as how their employer, coworkers and/or the workplace compensation board responded. Such open exploratory discussion allows for the discovery of information that may not have been previously considered by the researchers. 31
Analysis
The recorded interviews resulted in approximately one thousand pages of transcripts. They were imported verbatim into a qualitative data analysis program, QDA Miner 32 for open-coding 33 and thematic analysis. 34 The two academic researchers who had conducted the group interviews read through the transcripts to identify initial themes and subthemes and create the preliminary coding scheme. Codes for Risk Factors were organized using U.S. Occupational Safety and Health Administration (OSHA) categories: Clinical (patient care), Environmental, Organizational, Social, and Economic. 35 Other broad themes included the Personal Effects of violence on individuals, Barriers to making improvements, and Solutions. The researchers then thoroughly re-read the transcripts and coded statements as they proceeded, adding further codes as they were identified. The list of themes and subthemes was reviewed by each member of the research team, evaluated for completeness, and revised.
Findings
One of the central findings in this study is that violence is experienced as a pervasive and ongoing problem throughout the healthcare system. Because a range of facilities was explored, there were some differences in the risk factors identified from one to the other. For example, twenty-three of the fifty-four participants reported that they are currently or were previously working in forensic, psychiatric, emergency, or dementia care units. They described violent incidents that they perceived to occur on a regular basis, some reporting violence as an “everyday” occurrence. This experience is borne out in previously published literature. 1 The potential for violence was experienced, however, in every area of patient care—including acute and chronic care. Because members of the general public can be unpredictable, patients and their family members or visitors are potential sources of violence at any time. Hospitals and other healthcare facilities can trigger highly emotional reactions. Fear, pain, trauma, and concern for the patients can precipitate aggressive behaviors. It was also revealed that there are considerable inconsistencies in protections provided from one community, facility or department to another.
Risk Factors
The study participants identified numerous risk factors that contribute to violence against healthcare workers. A few participant comments have been included to illustrate key points; some have been edited for clarity as well as to ensure anonymity. Some are composites of comments from multiple individuals.
Clinical risk factors, according to the U.S. OSHA, include “the influence of drugs or alcohol; severe pain; history of violence; cognitive impairment (e.g., dementia); and certain psychiatric diagnoses.”
35
Study participants described factors in their own workplaces that fit within this category. They discussed violent incidents from patients whose judgment was likely impaired by one or more of these factors. Many of these incidents took place in emergency departments, long-term care and geriatric care departments, psychiatric units, detox facilities, and forensic units. –We had a situation where a patient’s family member came through the emergency department with a wooden club. He apparently didn’t feel that the patient was getting the proper care. They now limit access because you never know who’s coming through the door. –Geriatric and dementia patients are probably the ones I find most difficult. You tell them they can’t go home and they’re going to fight you on it. –I had a patient that was withdrawing from heavy drugs and alcohol and he ended up cornering me in the hallway. He picked up his mattress and he threw it at me. –I've pretty much dealt with violence since starting work in mental health. From having to do one-to-ones, five-point restraints, tackling violent people, restraining them. I was assaulted by a patient, and it was a severe assault. I was strangled, I was thrown, I was beaten. –One of my co-workers was in a room tending to a resident, and this man who had dementia, got it into his head that it was his wife in the bed, and that my co-worker was abusing her. He picked her up, threw her across the room, pounded her face and there was blood everywhere. –Whether it’s a psychiatric or medical patient or someone coming into an emergency room—if you don't have the staff to immediately address their issue—if they're kept waiting—they are more likely to escalate in their behavior.
Environmental risk factors, as described by U.S. OSHA, “relate to the physical layout, design, and contents of the workplace.” They include such building features as “unsecured access/egress …; insufficient heating or cooling; irritating noise levels; unsecured items … and lack of personal security alarms …”
35
Participants explained that the building design where they worked was often not protective. “Those hallways are terrible. You work way over there—and you can’t communicate. I would prefer a full roundabout circle.” One hospital worker described a situation in which she and two co-workers were trapped in a room by an aggressive patient and had been unable to call a Code White, which is a request for assistance for violent encounter. –I was trapped in the room and wasn’t able to call a Code White because he had hold of both of my arms. The more I tried to get away, the stronger he got. He slammed me against some walls and pushed me down on the bed. Two of my co-workers came to help me and we ended up on the other side of the door holding it closed. –He punched me in the head a couple times—so I yelled and people came. But we had no place to put him because our only seclusion room was being used as a patient room. –There is a bathroom emergency alarm and then up above the bed with our call system are the patient and staff emergency alarms. There’s no different distinct sound between them. –We were all trying to get her off me and I had my cell phone out to try to call, but I couldn't. And when I went to press zero to call a Code White, the patient kneed the phone out of my hand. So we just had to deal with it ourselves. –We have no alarms. It was funny, people who have alarms—the doctors, the social worker and the occupational therapist—but not the nursing staff. –I didn't know that there was anything wrong with us not having alarms until I was approached at a seminar. An employee from another hospital came up to me and said, “I work laundry and when I walk into the mental health floor, I have to pick up an alarm, and, after taking care of the laundry, I come back and drop it off.” And I said, “We scream. That's the best we can do is scream.” –This is when he grabbed me and hit me with the glass. I slumped to the ground and he was still pounding me. And next thing you know, all I can tell you I remember—I don't remember being on the floor—but I remember my tongue being tingly and then my memory was off. I fought him all the way down the hall. He put my head through the wall. There was blood on the walls from my elbows, my face. Many months later, I still suffer headaches and symptoms of depression. –He’s got the chair above his head. It’s kind of a shock because the nursing station has been smashed two or three times. –After a co-worker was sexually assaulted by a patient, the inspector recommended that they put glass up. The hospital fought them on it. They said it stigmatizes the patients.
Organizational risk factors for violence in healthcare facilities are described by U.S. OSHA as the “policies, procedures, and prevailing culture of the organization related to safety and security.”
35
The study participants identified many factors that could be considered organizational including working alone or short-staffed, inappropriate staff placement, lack of trained security personnel, healthcare workers’ responsibilities during Code Whites, inadequacy of de-escalation and other training, underreporting, and limited use of restraints. It was reported that, in some locations, police have a practice of bringing violent patients into the healthcare setting without sufficient communications or controls. The issue of insufficient staffing levels was heard in every group in every location. –One of the staff was working nights and a patient bashed her head into a piece of equipment. She was by herself. She couldn’t call for help. She didn’t even have a phone. She suffered a concussion and never came back to work. –She could have grabbed someone else and we wouldn’t know. The violence isn’t being charted. Even if it were charted, it might be so far back in the chart that you might not see it.
In some cases, participants felt that staff were inappropriately placed, e.g., assigning a new graduate to a potentially volatile patient without additional staff support. “I work with some nurses up there who are very tiny and young and don't venture too far away from the desk, which sort of gives the appearance that they are afraid of the patients.”
There is inconsistent flagging of potentially violent patients, not only in their chart but also in other visible locations. Some hospitals use colored arm bands, some symbols, or signs on the door or over the patient’s bed. A participant described the flagging policy in the facility where she worked. No sign signaling threatening behavior was put in place until a violent incident had occurred. “Hospital policy is that, if they swing so many times, then you put up a sign. … the sign goes up after incidents have happened.” Other facilities do not use flagging claiming that it would be stigmatizing to the patients. –The assault could well have been prevented with flagging—a white sheet of paper or arm band. But I’ve been told, “That’s too much information, it’s breaching confidentiality—stigmatizing them.” And I think, “Come on! How many people have to get hurt?”
Social risk factors, as described by U.S. OSHA, include the use of “weapons among patients and their visitors; the increasing use of healthcare facilities by authorities as criminal holds; and presence of gang members, drug or alcohol abusers, trauma patients, or distraught family members.”
35
In our data coding, we also included lack of respect for healthcare staff and negative societal attitudes towards women, sexual minorities, and racialized and immigrant workers. –She came in with the police, wasn’t searched by the police or anything. They were trying to get her into restraints because she was throwing stuff at them; she was threatening people. Nobody checked her, nobody patted her down. It turned out she had a six-inch blade. –I notice at the hospital coffee shop they have a sign that says they won’t tolerate any type of verbal abuse. But there’s no signs on our units that say that. We need signs like they have in emerge that say, “We will not tolerate verbal or physical violence.” … There is a poster about if you’re widowed and lonely, here’s a singles web site. But you won’t put up a violence sign for us? –We don’t report sexual violence because it happens so frequently … I have been grabbed many times … Sexual harassment is definitely a problem for women workers. If I go in with a male worker, the patient is not going to pinch his butt. They'll pinch mine or make a sexual comment … A patient referred to the nurses as whores and bitches … You feel disgusted with yourself after someone makes an inappropriate pass. It makes you feel violated.
Cultural and racial differences have become flash points for some patients. A participant reported, “I’ve been called the “N” word many times and I’ve been threatened.” Another participant told us, “My Asian partner got beaten up. She got punched in the face. The patient thought she was a terrorist.”
A participant recalled being warned by a patient’s family member that her parent would likely react if a non-Caucasian healthcare worker tried to treat him. She was told, “My father has a problem with visually-ethnic people. If the doctor is going to be Chinese or whatever, you’re going to see a side of my father that’s going to come out.”
Distraught families and traumatized patients sometimes lash out at healthcare workers—verbally or physically—blaming them for the patients’ discomfort, long waits, etc. –So I go to give the patient an explanation and they rip my head off and want to talk to the doctor—rightfully so—it’s the doctor who changed their orders. Things like that happen all the time and people get agitated with YOU. –This family member was chasing and barricading a co-worker. He was angry over a bruise on his parent’s hand, which we had suspected was from basic blood work. I grabbed his attention and yelled, “You need to leave now. You can’t do this, you need to leave.” Then he starts chasing me, yelling. I finally get away and run to the nurse’s station. I get in and start to close the door fast so I can call 9-1-1. He starts kicking the door and forcing it open.
Economic risk factors, as described by U.S. OSHA, are related to the funding levels of the institutions and decisions regarding allocation of funds, which “can contribute to risk factors on a personal level in the form of stress levels and on an organizational level in the form of short staffing.”
35
The participants—without exception—identified limited resources as a contributing factor to violence. They reported that understaffing contributes to patient frustration, boredom, fear and anger, which can then lead to acting out behaviors. –You don’t really have extra staff to sit with them and calm them down or to help monitor them … Then that upsets the other patients and family members. And it comes back on you. –With everybody just burning out like they are, you've got no one to come in. There's a ridiculous number of staff that are not making their shifts because they can't cope anymore. I was just in a unit where they had three staff out of their seven call in sick. Supervisors were calling from five o'clock in the morning until seven and they couldn't find a single person to come in. –It’s all about the budget … We have no security. When we've brought it to their attention—their answer is, “If we do bring in security, there will be staff layoffs.”
Personal Effects
Violence can have serious physical and psychological repercussions. It was difficult for some of the participants to talk about their experiences. Some were overwhelmed during the interviews and became shaken and tearful as they described assaults they had endured as well as injuries and aftereffects. We heard that violence can also have financial consequences if it leads to uncompensated lost time at work. We learned that even witnessing a violent incident can have profound, long-term effects—as can the fear of violence. Families and friends may suffer along with the victims.
Some sustained chronic or permanent injuries. While some said they had caring supervisors who provided compassion and concern, others expressed frustration that the postincident briefings were not personally supportive and that they felt they were being blamed for the assault. Several participants said that when management is trying to determine the root cause of a violent incident, their first position seems to be that the staff person somehow triggered it by some misstep. –To me it’s accusatory. They're blaming you … especially when they can target the lowest nurse on the totem pole … If I report an incident and my manager brings me into the office, she’s questioning me on what I did wrong. “Did you approach the patient the right way? You came in too fast. You didn’t tell them what you were doing.” … It’s never the patient’s fault. It’s always our fault. What could you have done better? Well maybe the question should be asked, “Well you, as my employer, what could YOU have done to help not have this happen?” –I can tell you from looking at the responses from managers on incident reports, they feel they’re mainly there to defend the patient. You’re the one defending yourself. –I’m pretty close to being back to normal now. But there are such lasting effects. It’s not just over when the bruises heal. And I think that’s something that people don’t necessarily get if they haven’t been through a trauma like that. This has a profound effect.
Experienced healthcare workers described the change in their role over the last decade or so—from caregiver to ad hoc security personnel—particularly during Code Whites. They believe when they have to function as security, their caregiver–patient relationships are adversely affected and they are made to feel professionally less effective. Some nurses expressed fear of losing their license because of the nature of their interactions with violent patients. They felt that a lack of support from management and a lack of acknowledgment of their injuries, including PTSD, compounded the negative effects they were already experiencing. Many said they were frustrated by the effects of insufficient staffing levels on their professional effectiveness and the negative consequences it had on patient care—which they then believe contributes to violence. –I can’t do enough for my patients and it makes me feel like I’m a horrible nurse. I feel like my license is on the line, not because I’m not competent, but because I should have done more and there’s not enough time—because there’s not enough staff. The violence totally escalates when there’s not enough staff.
Barriers
There were numerous barriers identified to eliminating violence. Study participants reported that violence has become normalized in many healthcare settings. Some felt that it is being increasingly viewed as “part of the job.” Some expressed concern that it may be impossible to eliminate the threat of violence. This sense of hopelessness or defeat may be a significant barrier to addressing the problem.
If managers regularly dismiss acts of violence as insignificant, they may view protective changes as unwarranted. “Violent occurrences are made light of by our management. I’ve seen the comments … It’s accepted. It is part of your duties. If you don’t like it maybe you should look at a different type of job in a different type of field.”
Police are often not called when an assault occurs and criminal charges are not consistently laid or upheld. This may send a signal to patients that violence will have no consequences. According to several of the participants interviewed, patients with dementia or mental health issues are often considered not criminally responsible for acts of aggression.
There is an apparent conflict between patient rights and worker rights. For example, participants stated that, since 2001, they have been required to minimize the use of restraints. Reportedly, however, there has not been a corresponding increase in staff or the introduction of comparable protections against violence to accommodate this principle. –So they came out with Patients’ Bill of Rights. It's this pendulum of “this isn’t working anymore, so we've got to try something else,” but there's no medium. The pendulum doesn't stop. It swings way to the opposite end. All we have is a Code of Conduct. –When you’re short staffed, there’s no time to do incident reports. It seems like they make the incident reports so difficult for you to weave through, it just becomes too much to do.
Healthcare workers are hesitant to speak publicly about the issue of violence due to fear of reprisal by their employer or professional governing body. Participants stated that patient confidentiality is cited by their employers as the rationale for prohibiting public commentary. As a result, the public is generally unaware of this widespread failing of worker protection within the healthcare system. The inconsistency of budgets across the healthcare system and chronic underfunding is a significant barrier to implementing protections, such as adequate staffing, programs, engineering controls, environmental design, security, and other identified measures. There are inadequate regulatory and legislative protections to prevent violence. In addition, under Ontario law, healthcare workers’ have only a limited right to refuse work they believe to be unsafe. There are also significant inconsistencies in protection from one facility to another across the province.
It was the participants’ experience that the Workplace Safety and Insurance Board did not recognize or compensate many of the physical and psychological effects of violence. Such serious conditions as PTSD, cumulative stress, and long term effects of concussion are not uniformly recognized. As one participant said, “What’s the point of filing a claim? They don’t do anything about it anyway.”
Solutions
Prevention Strategies Recommended by Study Participants.
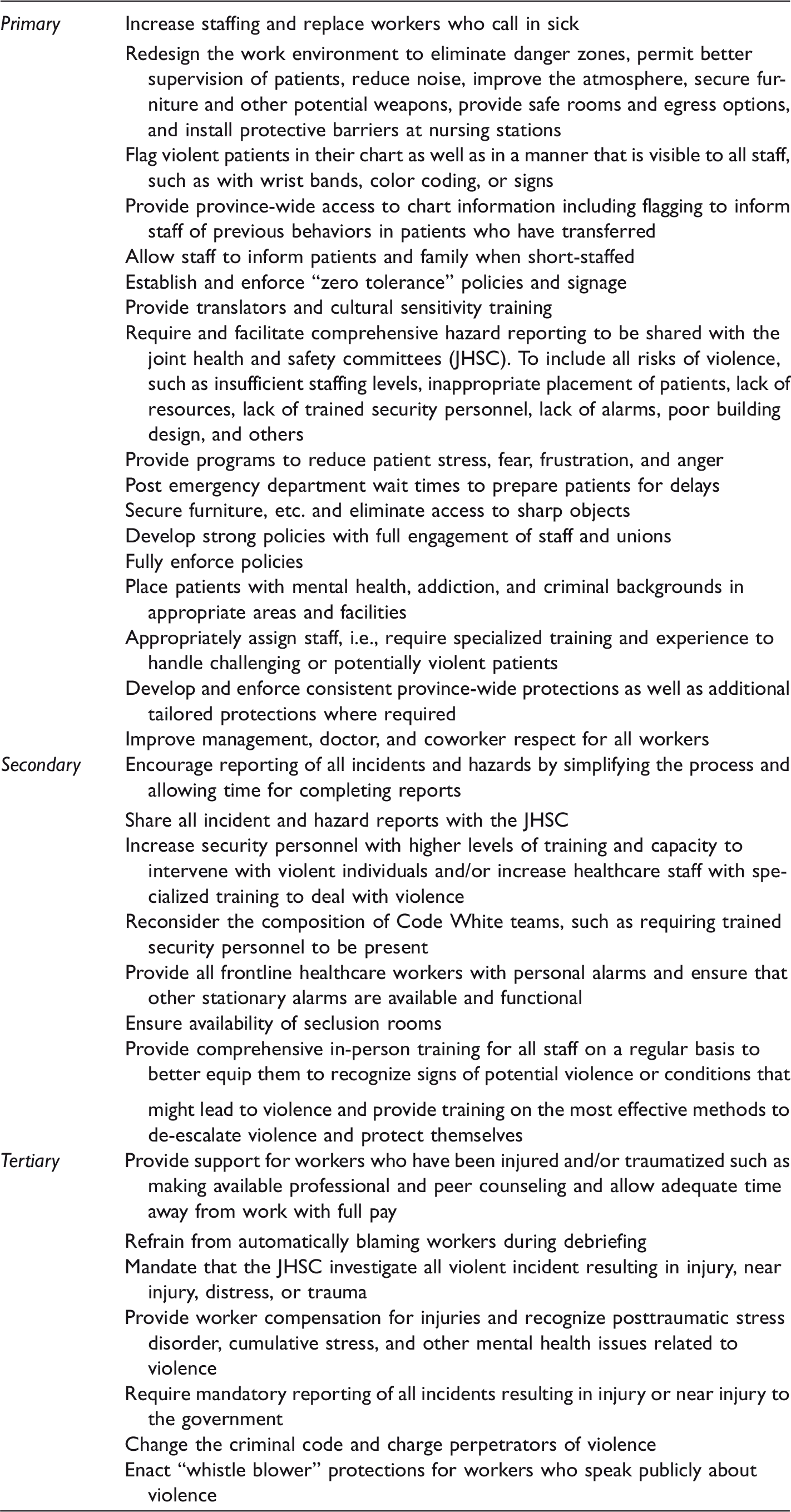
The majority of their proposed solutions fit within the category of Primary prevention. Ensuring adequate staffing levels, a strategy recommended in much of the literature, was cited and emphasized in every group interview. Engineering controls, such as better building design, better communication and identification strategies, increased security, and “zero tolerance” policies were also frequently recommended. Within the category of Secondary prevention, incident reporting, Code White responses, alarms, and training were emphasized. The after-the-fact Tertiary prevention strategies included a wide range of postincident supports and such legislated measures as changes to the Criminal Code and “whistle-blower” protection.
A draft of the findings was presented at a conference sponsored by the participating union council. The experiences of the study participants, the risk factors they identified, the effects they experienced and observed, the barriers they perceived, and the solutions they recommended were shared with the two hundred delegates in attendance. The findings were overwhelmingly validated in plenary discussion and prioritizing exercises. The attendees were asked what strategies might be employed by their union to bring about the recommended improvements, as shown in Table 1. While some issues, such as staffing levels and legislative protections, were given higher priority than others, it was decided that a multipronged campaign would be launched to promote all of the preventative measures brought forward in the study. The campaign would include informing the public, demanding protective language in contract negotiations, and lobbying the government for changes.
Discussion
This study contributes knowledge regarding the issue of violence against healthcare staff, particularly in the Ontario context, where little qualitative research on this subject has previously been done. It included healthcare workers in occupations often left out of studies in that it involved not only direct patient care staff but also allied workers. As a collaborative study, it provides the healthcare workers and their unions with a voice with which to communicate their experiences and ideas. It is important in an environment that has tended to publicly silence healthcare staff about the issue of violence. It also informs their unions’ campaigns aimed at prevention and provides pertinent evidence to support demands for enhanced provincial government regulatory protections.
The study is limited in that it did not include the experiences of healthcare staff in small, remote northern communities nor did it gather data from healthcare professionals, such as physicians and registered nurses. The small number of participants representing various racial and ethnic backgrounds may also have limited the findings with regards to the role of discrimination as a trigger for violence. The findings did not thoroughly differentiate the risks for violence by specific occupation or type of facility.
Despite these limitations, the study was informative. It revealed that, in the experience of the healthcare workers interviewed, violence in Ontario’s healthcare system has come to be seen as normal or as unavoidable—as an inevitable risk. Their perception is supported in research conducted in other jurisdications.1,36,37
The phenomenon of violence against healthcare staff is well documented. For over two decades, research has provided myriad potential solutions.1,4,36 Some would require significant financial investment, such as hospital redesign and increased staffing. Others simply require a change in approach. One of the important recommendations is that all violent or abusive incidents be treated seriously, including verbal comments and threats.
The importance of recognizing verbal assault as a form of workplace violence cannot be overlooked, since verbal assault has been shown to be a risk factor for battery. The “broken windows” principle, a criminal-justice theory that apathy toward low-level crimes creates a neighborhood conducive to more serious crime, also applies to workplace violence. When verbal abuse and low-level battery are tolerated, more serious forms of violence are invited. 1
Many of the recommended solutions remain unimplemented and, as a result, violence continues to harm healthcare workers. Prevention efforts need to address not only immediate safety concerns but also underlying systemic causes. Violence within healthcare settings may reflect broader structural violence12,38 emanating from economic and political factors as well as cultural violence.
39
Structural and cultural violence can be manifest as discrimination and disregard for women, immigrants, racialized workers, and those with different sexual orientation, genders or abilities.27,38–40 As stated in a report jointly released by a coalition that included the International Labor Office and World Health Organization There is growing awareness that confronting stress and violence requires a comprehensive approach. Instead of searching for a single solution good for any problem and situation, the full range of causes which generate stress and violence should be analyzed and a variety of intervention strategies adopted. There is also growing awareness that stress and violence at work is not merely an episodic, individual problem but a structural, strategic problem rooted in wider social, economic, organizational, and cultural factors.
41
“Violence permeates all aspects of our society. In Canada, the majority of healthcare workers are women.” 42 According to the Registered Nurses Association of Ontario, “Nursing continues to be a female-dominated profession, and societal attitudes continue to devalue and sexualize nursing. As a result, violence against nurses can be considered part of the continuum of violence against women.” 43
Occupational health and safety hazards in workplaces predominated by women employees have not received the same attention as those traditionally employing mostly men. 44 As Banerjee et al. suggested that “the failure to adequately address ongoing risk, the normalization of violence and the blaming of victims is characteristic of violence against women. We therefore question why gender has typically been absent in analyses of health-sector violence.” 12
Healthcare workers interviewed for this study reported that they are largely barred from speaking publicly about the assaults they experience. This restriction serves to keep the problem hidden from public view and scrutiny. Legislated safeguards, i.e., “whistle-blower protection,” must be put in place for workers who choose to talk about their experiences, while recognizing the importance of protecting patient confidentiality.
Assaulted workers suffer beyond the violent incidents that occur. Postincident supports must be enhanced. PTSD, a serious and common result of violence, is not always recognized or adequately treated. A U.S. study of emergency department (ED) nurses found Ninety-four percent of nurses experienced at least one post-traumatic stress disorder symptom after a violent event, with 17% having scores high enough to be considered probable for PTSD … Interventions are needed to prevent the violence and to provide care to the ED nurse after an event.
45
Physical and psychological effects need to be mitigated through adequate treatment, recovery time, and specialized counseling. According to US OSHA Victims of workplace violence could suffer a variety of consequences in addition to their actual physical injuries. These may include: short- and long-term psychological trauma; fear of returning to work; changes in relationships with coworkers and family; feelings of incompetence, guilt, powerlessness; and fear of criticism by supervisors or managers.
8
Although verbal and sexual harassment may not result in serious physical injury, these forms of violence must be recognized as harmful and addressed. Ongoing support, such as one-on-one or group counseling, should be offered to anyone who feels they might benefit from it. In addition, supervisors and management personnel should be provided with sensitivity training in order to understand the needs of staff who are, or have been, subjected to violence as well as to appreciate the importance of showing them respect and empathy. Violence training needs to include healthcare worker input, be more comprehensive, and include regular refresher courses. 46
The protections currently in place in the various healthcare facilities represented by the study participants appear to be piecemeal and inconsistent. Universal province-wide protections need to be legislated. The policies developed in each facility as part of their violence prevention programs, must incorporate legislated protections, as well as any additional protections that are needed as a result of the particular character of the facility and the population it serves.
The participants’ sense that patients’ rights supersede healthcare workers’ rights and that they are held, at least somewhat, responsible by their supervisors for violence perpetrated against them may be a reflection of broader social attitudes towards workers and the diminishing of workers’ rights under neoliberalism. 47 In order for system-wide changes to come about, the wellbeing of healthcare workers has to become a priority—for hospitals, consumers, regulators and the society as a whole. Inadequate resources, understaffing, patient wait times, insufficient training, and lack of appropriate resources for patients with mental health needs have been identified in this and numerous other studies as important risk factors for violence. The experience of this study’s participants regarding these factors is borne out by recent reports. Ontario hospitals are operating with less per capita funding than the rest of Canada. 48 Staffing levels are correspondingly lower. 49 Patient wait times are elevated, 50 a significant risk factor for violence that has been identified in the literature. For example, a study of violence in emergency departments states: “Even normally pleasant, well-adjusted people can become irritable after a 3- or 4-hour wait, and those who are already unstable may become dangerous.” 51 There is also a shortage of mental health beds, 52 resulting in the inappropriate placement of patients with particular needs and sometimes a propensity towards violent behavior.
Conclusion
The risk factors for violence against healthcare workers have been well documented in this and countless other studies and many solutions have been put forward. These recommended measures, including policy changes, increased staffing, safer building design, improved security, new programs to minimize patient agitation, and others need to be implemented by the healthcare institutions with the participation and control of those at risk. The healthcare staff and their unions or associations should be fully involved. Further research should then focus on evaluating the effectiveness of these new measures.
It would also be informative for the public to be given the opportunity to weigh in on the issue of healthcare violence prevention. Stakeholders, which include the general public, patients, frontline staff, and health professionals, should be widely and comprehensively consulted about their views and ideas. Open discussion might be prompted by such questions as: How can healthcare workers’ experiences be communicated and utilized to reshape the way our healthcare system functions? What can the public do to help reduce or eliminate violence in healthcare facilities? How can healthcare staff be protected from harmful societal attitudes, such as discrimination? How can patients’ rights be balanced with healthcare workers’ rights to a safe workplace? How much does the public value its universal healthcare system and how much are they willing to invest to make it work?
Footnotes
Acknowledgments
We gratefully acknowledge the courage of the participants who agreed to share their experiences, thoughts, and ideas for this study. We recognize that, for some, the issue of violence is emotionally difficult to talk about. We are grateful for the contribution to this study made by Linda Clayborne, who assisted in participant recruitment, organized interview groups, recorded the sessions, and generally supported the team. We wish to thank Sharon Richer who managed myriad logistics and administrative tasks and Doug Allan for providing important background information. We are also grateful to Mary McArthur and Jane McArthur who provided advice regarding methodical approaches and analysis. We thank the Ethics Committee at the University of Stirling for its thoughtful review of the study protocol and Professor Andrew Watterson who reviewed the proposed study and provided mentorship and encouragement.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This was a collaborative study between the Ontario Council of Hospital Unions/Canadian Union of Public Employees and academic researchers affiliated with the University of Stirling. As a descriptive qualitative study, the results will reflect the subjective experience of the participants, which will unavoidably be reflected in the results as reported by the authors. However, in reviewing and analyzing the data provided by the participants, the authors declare that they sought to accurately reflect the lived experiences and concerns as recounted to them without misrepresentation, omission, or elaboration of essential ideas. They further declare that there was no financial incentive to produce findings that did not accurately reflect the study data.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All study costs, including the authors’ time and expenses, were covered by Ontario Council of Hospital Unions/Canadian Union of Public Employees.